Innovation in Assistive Technology: Voice of the User

1
Independent Internet Professional and Disability Advocate, Melbourne, Victoria 3000, Australia
2
Department of Health Professions, Swinburne University, Hawthorn, Victoria 3122, Australia
*
Author to whom correspondence should be addressed.
Societies 2019, 9(2), 48; https://0-doi-org.brum.beds.ac.uk/10.3390/soc9020048
Submission received: 31 March 2019
/
Revised: 16 June 2019
/
Accepted: 19 June 2019
/
Published: 24 June 2019
(This article belongs to the Special Issue Socio-technical Approaches for Assistive Technologies and People with Disabilities)
{kind=link}
{kind=link}
Abstract
:This article is an open letter to assistive technology stakeholders from an assistive technology user perspective. Contemporary systems thinking in assistive technology identifies the interlinking themes of people, products, personnel, policy and provision. We add to the current discourse on these five themes through the voice of an expert assistive technology user, who states that “As a disabled person and as a long-time expert assistive technology user, this is everything that I wish you knew and everything I wish you would do.” Our objective is to provide a user-centered commentary upon current trends and innovations in assistive technology, illuminating real impacts and outcomes from a social perspective and adding a rarely-heard voice to the literature.
1. Introduction
This is an exciting time to be an assistive technology (AT) user. Assistive technologies, defined as “especially produced or generally available devices, equipment instruments, or software” [1] are a demonstrated facilitator of functioning for people with disabilities and people ageing into disability. Assistive technologies have the potential to close the “capability gap” between a persons’ individual capacities and contextual barriers, and their goals. The historical lack of access to assistive technologies is changing with the confluence of technological development, human rights progress, and progressive public policy in many developed nations. Recent interest in the potential of assistive technology to meet the twin goals of universal health coverage and sustainable development [2] has uncovered a range of assistive technology system gaps [3]. Systems thinking enables the systematic evaluation of assistive technology and has identified at least five key perspectives, including people, products, personnel, policy, and provision [4]. Bodies of evidence regarding technology abandonment or non-use [5,6], consumer dissatisfaction [7], and supply chain complexities [8] suggest that the potential of assistive technology is not yet fully realized, and they point to the importance of matching person and technology [9] and the complexities of matching person, environment, and technology [10]. Throughout the discourse in this evidence base is the issue of the social embedding of technology.
Responding to the call by Nierling et al. (2018) for user involvement, this article presents an assistive technology user standpoint from Australia [11]. We draw on emancipatory theory [12] and contemporary views on the democratization of knowledge [13,14] to justify this rare example of a direct consumer voice within academic literature.
As authors, we firstly introduce ourselves and our standpoints. Then, author RB describes her perspectives according to the dimensions of people, products, personnel, policy. and provision. We conclude by summarizing “what good looks like” in assistive technology systems from an AT user perspective, considering the interlinking constellation of factors required to deliver on the promise of assistive technology.
2. Standpoints—A Statement of Position
Author RB is passionate about disability and chronic illness; she thinks and writes a lot about assistive technology and how it fits into people’s lives. RB has been disabled and usually homebound/bedridden1 for her entire adult life. Her primary interests include people whose disability is caused by chronic illness and those who are homebound and/or bedridden like her—two groups of people who are severely underserved by the current medical and disability systems. RB is connected to multiple user communities and has authored in the areas of user expertise [15], product design [16], and inclusive research [17]. She is also a systemic advocate [18]. RB contributed the content of this article.
Author NL is an occupational therapist, researcher, and university lecturer interested in the nexus between practice, research, and policy. NL utilizes inclusive research and co-design methodologies to set research priorities and guide methods in her work with individuals and communities. As president of Australia’s peak body for assistive technology, the Australian Rehabilitation and Assistive Technology Association (ARATA)2, NL brings an understanding of the collective voice of assistive technology stakeholders in Australia and internationally. NL contributed to the introduction, the conclusion, and the organizing of content of this article.
This is an open letter to assistive technology developers, assistive technology wholesalers, assistive technology retailers, and everybody else involved in the “producer” and “distributor” side of the equation. Author RB links the technical to the social across points three to seven below, stating: “As a disabled person and as a long-time expert assistive technology user, this is everything that I wish you knew and everything I wish you would do. I know that some of these things I have written about are difficult to implement due to external factors like cost, regulation (sometimes), and other barriers, but things are changing in AT, and these are the things I think we should all be working towards.”
3. People
Assistive technology is being located and chosen differently.
3.1. RB: “AT Users Have More Access to Peer Support.”
Peer support is not a new thing, but due to a growth in access to social media, the breadth and reach of peer support is only growing. In-person peer support is wonderful if it is available, if your disability allows you access to in person peer support, and if you live close enough to relevant peers. If, on the other hand, your disability is rare, if you are homebound or bedridden, if you live in a rural or remote area, or if your disability makes socialising in person difficult for any other reason … or even just if you do not happen to get on with someone in the local peer support group … then in the past you would have been out of luck. However, now with social media, as long as you have the skills to access the internet—either independently or with support—you can connect to others in similar situations to you either locally, nationally, or internationally. This means that a great many people are finding out about specific pieces of assistive technology by hearing peers post about it on social media, such as the Assistive Technology group on Facebook, or using hashtags such as #ATChat and #a11y on Twitter3. If you are an assistive technology developer or retailer, you need to work this into your marketing plans.”
3.2. RB: “AT Users May Need Additional Reliability and Consistency”
Some of us need more reliability and consistency than average users. Learning or adapting to new interfaces may be hard or impossible for some people. Dealing with failures might require that we organise external assistance. Even something as seemingly simple as rebooting a system of home automation devices might not be something we can do independently, especially if our support people are not comfortable with technology. If you are a retailer, offer consistency in software/hardware and easy-to-access support as your point of differentiation.
3.3. RB: “AT Users Need More Integration”
Funding mechanisms need to acknowledge the value of the integration of different pieces of assistive technology with the user’s current systems—including assistive technology systems and standard technology systems. For example, my living room curtains are automated and work fine with their specialised application but cannot interface with Siri, so I cannot use my voice to control them. For me, it is just annoying, but, for someone else, it could make the system completely unusable. Every different interface we need to use increases the cognitive complexity for the user. Not having integration opportunities also means users have much more trouble making things work together. It would be nice if a high temperature in my room automatically closed the lace curtains and turned on the air conditioner. As things are now, the air conditioner part works but because the curtains are on a separate system there is no way for me to make that happen. If both the curtain makers and the air conditioner makers used Apple’s HomeKit interface (or any other shared application programming interface API), this would be something I could easily set up for whatever temperature suited me. There is enormous value in integrating things, especially for those with cognitive or memory impairments. Make sure you have offered every opportunity for integration that you can, because you do not know which one suits your users.
3.4. RB: “AT Buyers Need More Information”
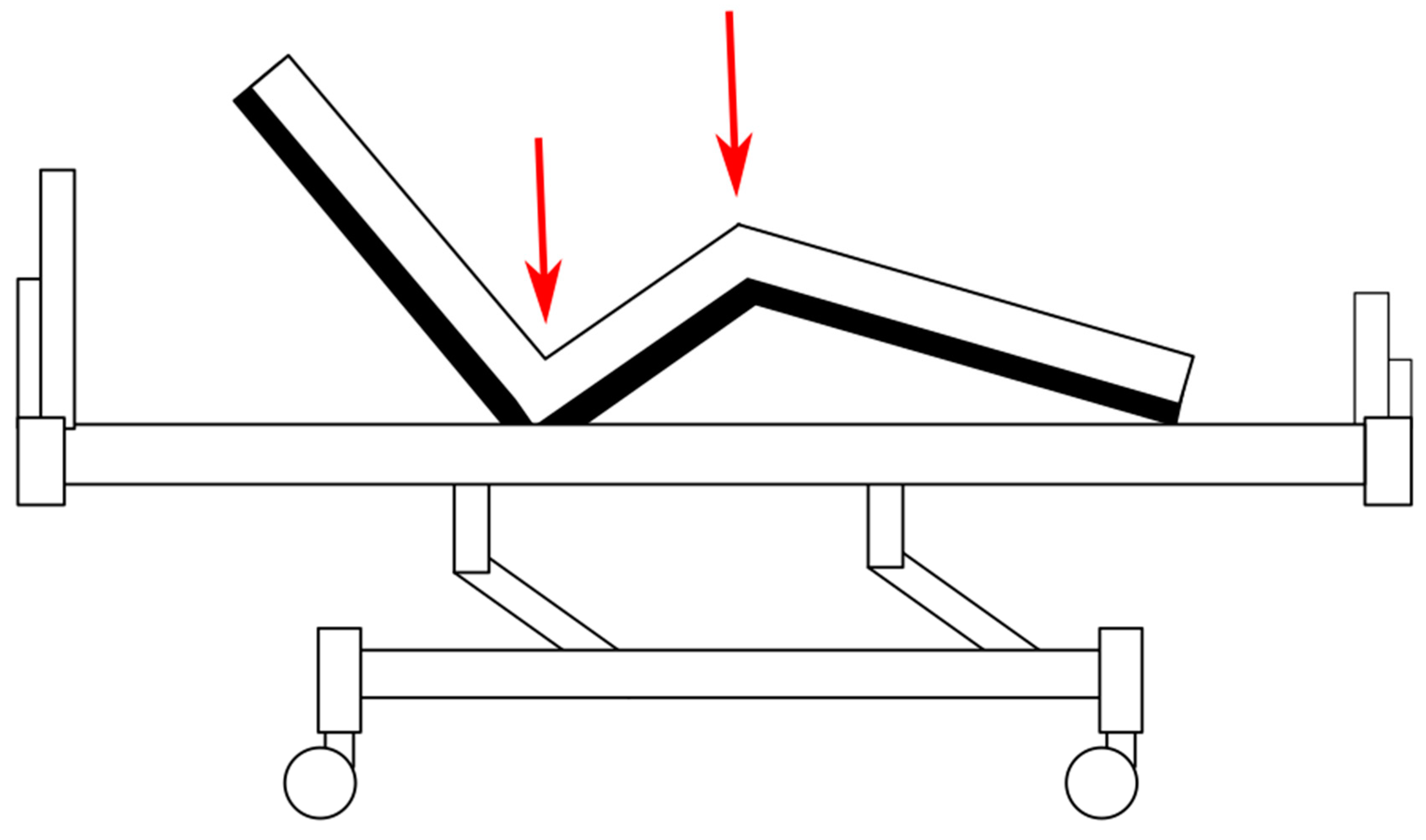
Make all the information about your equipment available, even information you think people do not usually care about. I bought a new hospital bed last year. This is where I spend all of my time, and I am very short, so having the bed’s hip and knee breaks (see Figure 1) fit me properly makes the difference between being comfortable and uncomfortable for the next ten years the bed lasts. There are many hospital bed retailers local to me, but not even one had this information on their website. I ended up having to make many phone calls and wait while sales folk ventured into their own showrooms and store rooms with literal tape measures to find this vital number, which is different, not just for each make of bed but often for each model. It was a huge waste of energy and time for me and for the retailers.
I told this story to another disabled friend of mine and she said that she had had almost the same experience, but the specific measurement that was vital to her was how high the back of the bed could be angled. If it was 65 degrees from horizontal, she needed help to get out of bed, but if the back went up to 70 degrees she could get up independently. She had the same frustrating waste of time and energy phoning all the companies involved to try to find an appropriate bed to buy.
When you are disabled, small details can be the difference between “I can do this easily” and “I cannot do this at all.” Having to phone up a dozen different retailers to beg for the information and then just crossing your fingers that you are given the correct information—that is just unhelpful. Please make as much information available on your website as you can. Exact measurements for everything that can be measured. Tell us how much force is needed to depress that switch and how much space there is around it. If there are engineering diagrams, put those up on your website too. With proper website design, you can arrange things so that casual viewers are not bombarded with unnecessary detail, but it is there for people who need it. This really matters.”
4. Products
4.1. RB: “Assistive Technology is More Mainstream”
Accessibility is going mainstream thanks to a number of factors, including the computerisation/convergence of everything and demographic changes as baby boomers age [11]. I have 43 pieces of equipment in my house that I would class as assistive technology—things that help me with something that I have trouble with specifically because of my disability. Of those 43 pieces, only 15 of them are technology that was developed specifically for people with disabilities. Things that are AT for me but not specifically aimed at folk with disabilities include: A variety of computer input devices (which I have mostly reprogrammed using commercial software which is also not disability-specific), a huge pile of off the shelf home automation devices like smart light globes and smart power switches, bedside trolleys to help me reach things, noise cancelling headphones, and microbead cushions which I use for positioning.
4.2. RB: “Assistive Technology is Being Used Differently”
People are going to do things that you never ever anticipated with your technology no matter what you do. It is vastly to your advantage to lean in and enjoy this rather than futilely trying to make it stop. Make your technology open, hackable, interoperable, expandable, compatible—all as much as you can! Make everything maker friendly and repairable. Make it upgradable for users and design your tech and your apps with modularity so one can upgrade pieces as soon as new technology becomes available—because you know it always will even if right now you cannot imagine what that will look like. Publish your application programming interfaces and make sure your apps are URL-addressable and will interact properly with web-based services such as ‘If This, Then That’ (IFTTT)4, Zapir5, and others.
Here are examples of some assistive technology mash-ups and uses that I am sure the original tech inventors never imagined:
- Eye controlled wheelchair—plans are available for a 3D printed open sourced system which converts a standard power chair to be able to be driven by an eye gaze system6 AAC (assistive and alternative communication) being used to control voice activated assistants such as Alexa, Google Home, and Siri7.
The impact of disruptive use is ”a whole tapestry of possibilities instead of a linear progression,” and I would like to acknowledge this quote as a personal communication from Helen Peake, who is part of my circle of support.
4.3. RB: “What AT Users Want from Their AT”
Assistive technology is often built with the assumption that someone must help you with it. People have wildly varying combinations of abilities and impairments, as well as very different degrees of access to support, so this is a broken assumption. In the last few years of my own life, I have struggled to find resting leg and ankle splints that do not prevent me from getting out of bed and walking to the toilet at night, as well as resting arm splints that I can put on and take off myself. My bedside commode also has a seat cushion which is so heavy I can barely lift it off the commode; this is surely a situation that others also find problematic. Sometime soon I will also need a dynamic air mattress, and I was dismayed to find that none of the ones available in Australia can be controlled by remote control of any sort, let alone an app on my phone. One Australian distributor (who I assume never heard of phone banking, passwords, or biometric security) told me it would be “too dangerous” to be able to alter mattress controls via app but apparently had no issues with the control box sitting at the end of the bed to be fiddled with by anybody who walked into the room. Please build all of the opportunities for independence that you can into your assistive technology. In most cases, you can incorporate security for users that need to not have access to some settings and independence for users that need that into the same unit without much trouble, especially if you think about it up front.
Leveraging the unique insights that the AT user has on utility, functionality, and adaptability, we suggest the addition of disabled people in a supply chain would address the fact that non-disabled people do not always understand what is required. Beyond “market research,” the inclusion of disabled persons as innovators and advisors throughout is critical to good outcomes. [7]
4.4. RB: “Internationalisation”
With internet access widely available, it is now much easier to find out about and access overseas equipment. Additionally, much local equipment comes without local support because it is mainstream technology purchased from a mainstream shop. As such, there is less of a disadvantage of buying equipment direct from overseas. This means that your assistive technology website needs to assume that international purchasers will read it to find information and place orders—make sure to not assume all readers have local knowledge. In addition, make international shipping available wherever necessary. Many funding policies do not support this type of purchasing, however, and arranging for repair or replacement in case of faults can be slow and difficult. We need to overcome these difficulties so that AT users in all locations, including those without local suppliers, can take advantage of innovations.
5. Personnel
5.1. RB: “Disintermediation is Increasing”
In this context, we use disintermediation to mean accessing assistive technology without a professional involved in situations where a professional used to be mandatory. Some examples include:
- Accessing assistive and alternative communication (AAC) apps without a speech and language pathologist (SLP)
- Buying a wheelchair without an allied health professional being involved
- Buying hearing aids without an audiologist being involved
People might be buying things online without any professional involved at all, or they may purchase somewhere like a pharmacy where there might be a pharmacist technically involved but who has little or no relevant training.
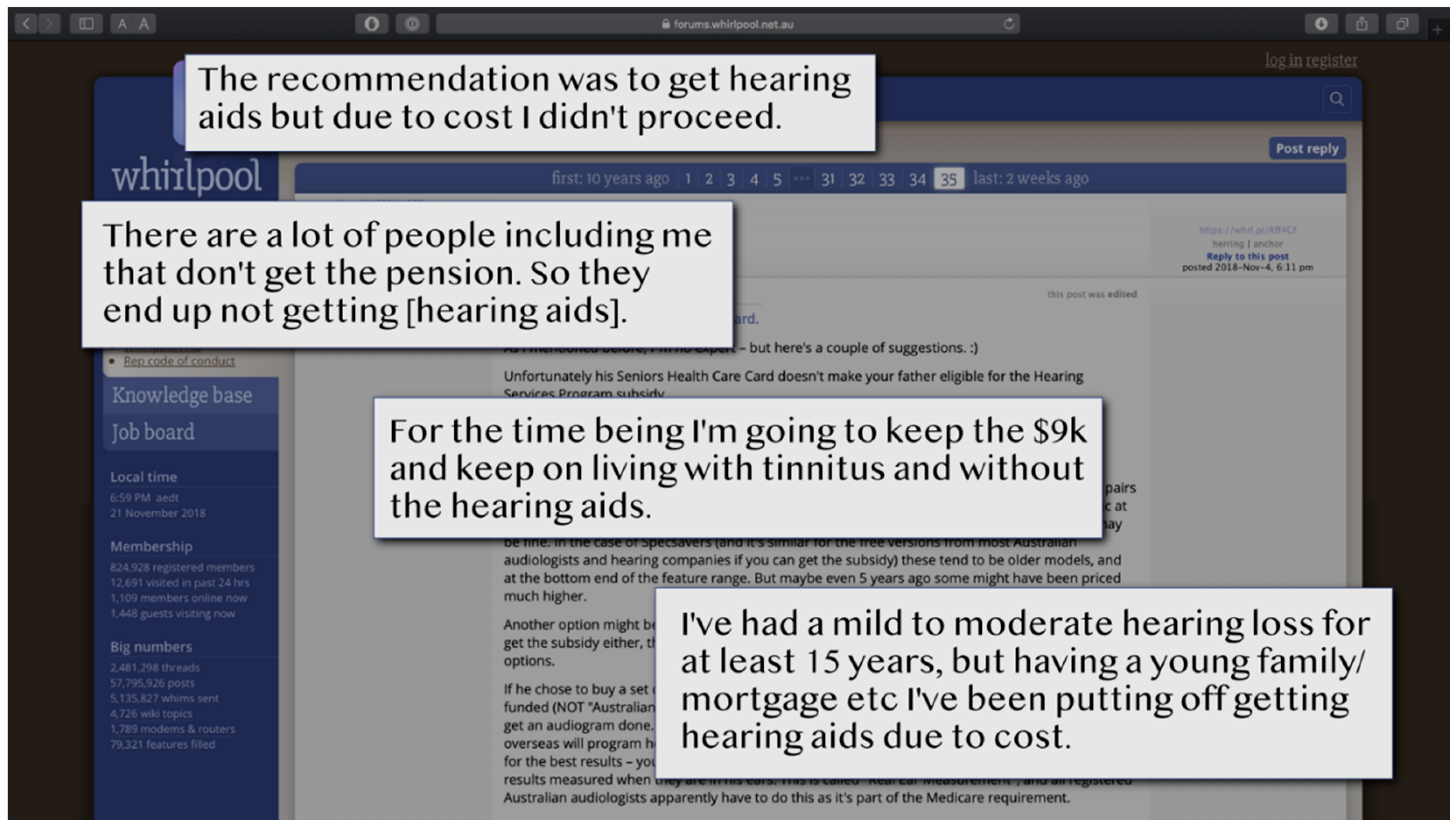
I have seen that disintermediation worries professionals very much—they realise that clients will be without professional support or guidance and may make sub-optimal choices. In some cases, making a bad choice can mean that you do not get the most optimal outcomes, but, in other cases, it can actually be dangerous. Those things are true, but there is another danger that I have not seen assistive technology professionals acknowledge very much—the danger of going without assistive technology altogether because the cost is prohibitive. The following image (Figure 2) is from a single Australian internet forum thread I found. Just one thread in just one place.
In the disability communities that I am familiar with, there are a lot of people going without desperately needed equipment for lack of funding. This includes people whose disability is just outside funding guidelines, people who are incorrectly advised by medical professionals not to seek disability funding, and people who would be eligible for funding but cannot jump through all the required hoops to satisfy bureaucracy. In all cases, it usually means there is just no money for professionals to be involved. Remember that of the 3 million Australians living in poverty, nearly 40% have a disability [19].
A cheap and non-adjustable wheelchair will almost certainly not be as appropriate as a wheelchair that your occupational therapist helped you pick out. However, any wheelchair may be infinitely superior to going without a wheelchair at all when you need one. Off-the-shelf hearing aids, which are configured via an app probably will not give you as good a result as audiologist-tuned hearing aids, but they are still significantly better than nothing at all.
Internationally, of course, there are even more people who will never have access to trained professionals and top of the line equipment or government funding, so the benefit of disintermediated equipment is even stronger in those places. Make sure your literature is accessible to consumers as well as professionals, because consumers are going to read it either way. The more you directly help people who are purchasing your assistive technology without the aid of a professional, the better their outcomes will be.
5.2. RB “The Dangers of Assistive Technology Jargon”
I always like to tell people I define assistive technology as “stuff that helps people do stuff.” This is an intentional over-simplification of the definition, but it does rather highlight how much jargon is frequently used around assistive technology.
This was fine when assistive technology was almost always accessed via a professional, such as an occupational therapist, speech and language pathologist, or rehabilitation professional, because those people could explain what things meant and guide consumers through. However, it is a lot more unhelpful when a good portion of your customer base is either purchasing things directly or doing their own product research so they can take the results back to their professionals.
Some few examples of the extensive collection of assistive technology related jargon:
- Augmentative and Alternative Communication
- Environmental Control Unit
- Ability switch
- Auslan
- Dwell control
- Transfers
- Video Modelling
- Even phrases such as “activities of daily living” which sound self-explanatory have a specialised meaning in this context
We must also remember that the internet is international. Even if your product is only aimed at people in one country, it will certainly be browsed and almost certainly also be purchased be people from across the globe. A phrase like “durable medical equipment” may be well known by most disabled Americans, for example, but outside America it is not used at all.
6. Policy RB “Assistive Technology is Being Funded Differently”
A lot of assistive technology pricing is done with the assumption that assistive technology is usually or always going to be government-funded or paid for out of similar funds such as compensation payments. Some funding schemes offer personalised budgets, like Australia’s National Disability Insurance Scheme (NDIS). These approaches are becoming more common, and this means that we are going to have more disabled folk with government funding. However, this will by no means be all of your customers. People fund assistive technology privately, using health insurance, using crowdfunding, using their superannuation, using charity or grants, and using a huge range of other methods. Consider offering alternative funding styles like AfterPay, lay-by, rent-to-buy, and reselling your own second-hand refurbished equipment where appropriate.
7. Provision
7.1. RB: “Assistive Technology is Being Purchased by Different People”
Lots of people who use assistive technology do not identify as disabled. We need to make sure our assistive technology marketing and documentation reflects the needs of those people, or they simply will not see what is available or perceive it as being for “people like them.” People who use assistive technology may identify as any or several of:
- Disabled/person with a disability
- chronically ill
- mentally ill
- autistic
- neurodiverse
- elderly/aged
- senior citizens
- baby boomers
- injured
They may also identify with none of those labels. Make sure you are not just marketing your assistive technology in traditional disability-specific forums or using disability-specific language. If you do, you will miss much of your audience. For some assistive technology products, some or even most of your audience will be people who are not in fact disabled at all but are just looking for convenience, ease of use, and automation potential (e.g., home automation enthusiasts). Other people may be looking to plan for their own future ageing.
Keep intersectionality in mind! Both in terms of people with multiple different disabilities and in terms of gender, race, sexuality, socioeconomics, and so on. This is not a new issue, of course, but it is pretty much been ignored in the past for disability. Go look at your websites and your literature—how many of those people are white and appear in heterosexual relationships or with someone who appears to be a nurse as a carer? We need to update things to be inclusive in many ways. Some companies—especially newer and more agile ones—are doing great with this, but many are not.
7.2. AT Buyers Cannot Always Do Trials
We need a funding model that does not assume you can always trial stuff—if most AT is mainstream stuff, it does not necessarily come from anywhere it can be trialled. In other cases, you can get it for significantly less money if you buy it from somewhere which does not allow trials. In still other cases, equipment needs to come from overseas because it is just not available in Australia. I have a friend who ended up having to crowdfund her wheelchair because the most appropriate wheelchair for her had no Australian distributor and therefore could not be trialled; Australia’s National Disability Insurance Scheme (NDIS)10 refused to fund it without a trial. We all understand that trialling things is optimal, but reality is messy and does not always work the way the bureaucracy wishes it would.
8. Conclusions
Discourse within the global assistive technology community has moved from a focus on assistive products to embrace assistive technology systems, coupled with “the need for user involvement in all aspects of research, policy development, system design and service provision… [and] the need to work from an environmental approach to functioning, in contrast to the medical model that has historically been dominant” [20] (p. 435). Through this article, we have responded to the call for user involvement in authorship. We outlined some of the shifts underway in the complex systems surrounding assistive technology, and we took a deep dive into the details of living with disability and living with technology. Examples of the impacts of design, marketing, provision, terminology, professionalization, and procurement systems were presented.
As such, what innovations are required in the assistive technology system from the perspective of AT users? All elements of assistive technology systems are intricately related, and multiple concurrent actions are required to improve the system from the perspective of AT users. Expertise will be recognised in a diverse range of AT people, including peers. AT products include the potential of mainstream and innovative product solutions, while specifications and adaptability will be fit for purpose as defined by AT users. Regardless of funding source, provision systems have the flexibility to enable important service steps, such as trials, and embrace the opportunities of international supply. Personnel systems actively co-construct “disintermediated” solutions. AT policy is geared around “what AT users want.” AT stakeholders, such as suppliers, avoid labels and embrace intersectionality.
Readers will, it is hoped, see the political through this exploration of the personal. Small system elements such as the details of design, product adjustment, or of language are critically important from a user perspective, and their impact reverberates through the assistive technology system as a whole. These illustrations amplify the perspective that “… future research should focus not only on the technical development as such, but rather on a sound implementation, social embedding and evaluation of technological solutions which already exist” [11] (p. 3).
Overall, we concur with Nierling et al. (2018) in their findings that “… people with disabilities have an open and optimistic attitude towards new and emerging technologies” [11] (p. 3). As RB states: “Really good assistive technology is life changing. Assistive technology systems where each piece of technology is appropriate and all the pieces work together effectively can be profoundly enabling. I hope that, if the assistive technology production chain is able to take on board some of the things I have written about, we can increase the chances of more people being able to obtain an optimal outcome from their assistive technology system.”
Author Contributions
R.B. conceptualization and writing—original draft preparation, review, and editing; N.L. writing—introduction, review, conclusion, referencing, and editing.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- ISO. ISO/AS 9999 Assistive Products for Persons with Disability—Classification and Terminology; International Organization for Standardization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Assembly. Improving Access to Assistive Technology; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- MacLachlan, M.; Banes, D.; Bell, D.; Borg, J.; Donnelly, B.; Fembek, M.; Ghosh, R.; Gowran, R.; Hannay, E.; Hiscock, D.; et al. Assistive technology policy: A position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 454–466. [Google Scholar] [CrossRef] [PubMed]
- MacLachlan, M.; Scherer, M. Systems thinking for assistive technology: A commentary on the GREAT summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.O.; Scherer, M.; Cooper, R.; Bell, D.; Hobbs, D.A.; Pettersson, C.; Seymour, N.; Borg, J.; Johnson, M.J.; Lane, J.P.; et al. Assistive technology products: A position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.J. Technology adoption, acceptance, satisfaction and benefit: Integrating various assistive technology outcomes. Disabil. Rehabil. Assist. Technol. 2017, 12, 1–2. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, D.; Layton, N.; Vicary, F.; Steel, E. Motivations and incentives: Exploring assistive technology service delivery from the perspectives of multiple stakeholders. In Proceedings of the RESNA 2015: New Frontiers in Assistive Technology, Denver, CO, USA, 10–14 June 2015. [Google Scholar]
- MacLachlan, M. Access to assistive technology, systems thinking, and market shaping: A response to durocher et al. Ethics Behav. 2018, 29, 196–200. [Google Scholar] [CrossRef]
- Scherer, M.J. Living in the State of Stuck: How Assistive Technology Impacts the Lives of People with Disabilities, 4th ed.; Brookline Books: Cambridge, MA, USA, 2000. [Google Scholar]
- Law, M.; Cooper, B.; Stewart, D.; Rigby, P.; Letts, L. The person-environment—Occupation model: A transactive approach to occupational performance. Can. J. Occup. Ther. 1996, 63, 9–23. [Google Scholar] [CrossRef]
- Nierling, L.; Maia, M.J.F.; Hennen, L.; Wolbring, G.; Bratan, T.; Kukk, P.; Cas, J.; Capari, L.; Krieger-Lamina, J.; Mordini, E. Assistive Technologies for People with Disabilities. Part. III: Perspectives on Assistive Technologies; EPRS European Parliamentary Research Service: Brussels, Belgium, 2018. [Google Scholar]
- Hekman, S. Truth and method. In The Feminist Standpoint Theory Reader; Harding, S., Ed.; Routledge: New York, NY, USA, 2004. [Google Scholar]
- Löfgren, H.; de Leeuw, E.; Leahy, M. (Eds.) Democratizing Health: Consumer Groups in the Policy Process; Deakin University: Melbourne, VIC, Australia, 2011. [Google Scholar]
- Jasanoff, S. States of Knowledge: The Co-Production of Science and the Social Order; Routledge: Abingdon, UK, 2004. [Google Scholar]
- Steel, E.; Buchanan, R.; Layton, N.; Wilson, E. Currency and competence of occupational therapists and consumers with rapidly changing technology. Occup. Ther. Int. 2016, 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, R.; Layton, N. Expert users involved in AT design: The example of the bed spaTM. Indep. Living J. 2010, 26, 6–7. [Google Scholar]
- Layton, N.; Foreman, L.; Buchanan, R.; O’Brien, P. Researching the things that matter: A model of inclusive research for consumers and their allied health practitioners. In Proceedings of the Victorian Allied Health Research Conference, Melbourne, Australia, 28 March 2014. [Google Scholar]
- Buchanan, R. Becoming Visible: A Chat with Ricky Buchanan. Every Australian Counts, Ed.; Available online: https://www.everyaustraliancounts.com.au/becoming-visible-a-chat-with-ricky-buchanan/ (accessed on 21 May 2019).
- Productivity Commission. Rising Inequality? A Stocktake of the Evidence; Productivity Commission Research Paper: Canberra, Australia, 2018; Available online: https://www.pc.gov.au/research/completed/rising-inequality/rising-inequality.pdf (accessed on 1 March 2018).
- Scherer, M.J.; MacLachlan, M.; Khasnabis, C. Introduction to the special issue on the first global research, innovation, and education on assistive technology (GREAT) Summit and invitation to contribute to and continue the discussions. Disabil. Rehabil. Assist. Technol. 2018, 13, 435–436. [Google Scholar] [CrossRef] [PubMed]
| 1 | RB uses identity-first language here, preferring “disabled person” to “person with a disability”. She also uses the words “homebound” and “bedridden,” which are the words most commonly used by those populations to describe themselves. |
| 2 | ARATA. www.arata.org.au (accessed on 1 March 2018). |
| 3 | Example: Assistive Technology Facebook Group. Available online: https://www.facebook.com/groups/assistive.technology.group/ (accessed on 1 March 2018). |
| 4 | https://en.wikipedia.org/wiki/IFTTT (accessed on 1 March 2018). |
| 5 | |
| 6 | https://www.instructables.com/id/Eye-controlled-wheelchair/ (accessed on 1 March 2018). |
| 7 | https://www.youtube.com/watch?v=fql8YZCPquw and https://smarthomesmadesimple.org/2018/07/06/will-alexa-understand-him/ (accessed on 1 March 2018). |
| 8 | https://sugru.com/blog/13-sugru-designs-that-make-things-easier-for-people-to-use.html (accessed on 1 March 2018). |
| 9 | https://www.plastimake.com (accessed on 1 March 2018). |
| 10 | NDIA https://www.ndis.gov.au/ (accessed on 1 March 2018). |
Figure 1.
Adjustable Bed dimensions.

Figure 2.
Internet forum thread regarding access to hearing aids.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Buchanan, R.; Layton, N. Innovation in Assistive Technology: Voice of the User. Societies 2019, 9, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/soc9020048
AMA Style
Buchanan R, Layton N. Innovation in Assistive Technology: Voice of the User. Societies. 2019; 9(2):48. https://0-doi-org.brum.beds.ac.uk/10.3390/soc9020048
Chicago/Turabian StyleBuchanan, Ricky, and Natasha Layton. 2019. "Innovation in Assistive Technology: Voice of the User" Societies 9, no. 2: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/soc9020048
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.