
Nasopharyngeal Swabs vs. Nasal Aspirates for Respiratory Virus Detection: A Systematic Review


1
School of Biomedical Sciences, Ulster University, Cromore Road, Coleraine BT52 1SA, UK
2
Altnagelvin Area Hospital, Glenshane Road, Londonderry BT47 6SB, UK
*
Author to whom correspondence should be addressed.
Pathogens 2021, 10(11), 1515; https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111515
Submission received: 16 October 2021
/
Revised: 10 November 2021
/
Accepted: 12 November 2021
/
Published: 20 November 2021
(This article belongs to the Special Issue Advances in Human Pathogens Infections)
Abstract
:Nasal pathogen detection sensitivities can be as low as 70% despite advances in molecular diagnostics. This may be linked to the choice of sampling method. A diagnostic test accuracy review for sensitivity was undertaken to compare sensitivity of swabbing to the nasopharynx and extracting nasal aspirates, using the PRISMA protocol, Cochrane rapid review methodology, and QUADAS-2 risk of bias tools, with meta-analysis of included studies. Sensitivities were calculated by a consensus standard of positivity by either method as the ‘gold standard.’ Insufficient sampling methodology, cross sectional study designs, and studies pooling samples across anatomical sites were excluded. Of 13 subsequently eligible studies, 8 had ‘high’ risk of bias, and 5 had ‘high’ applicability concerns. There were no statistical differences in overall sensitivities between collection methods for eight different viruses, and this did not differ with use of PCR, immunofluorescence, or culture. In one study alone, Influenza H1N1(2009) favored nasopharyngeal swabs, with aspirates having 93.3% of the sensitivity of swabs (p > 0.001). Similarly equivocal sensitivities were noted in reports detecting bacteria. The chain of sampling, from anatomical site to laboratory results, features different potential foci along which sensitivity may be lost. A fair body of evidence exists that use of a different sampling method will not yield more respiratory pathogens.
1. Introduction
Accurate laboratory-confirmed diagnoses aid both timely treatment and surveillance of respiratory infections and are facilitated by rapid detection methods [1,2]. The frustration of false negative results for specific pathogen carriage experienced by clinicians, thus escalating treatment upon clinical suspicion alone, predates SARS-CoV-2 and leads to reliance on repeat tests and imaging [3,4]. Pathogens may be lost at sampling, transport, or laboratory processing. Suboptimal sensitivity has persisted for viruses, despite the adoption of polymerase chain reaction (PCR) as the gold standard above viral culture and direct immunofluorescence (DIF). PCR may be perceived as less sensitive in head-to-head comparison with DIF. However, due to its increased accuracy and the elimination of false positives potentially found in DIF, PCR avoids the decreased sensitivities in patients over 5 years of age seen with DIF [5,6,7].
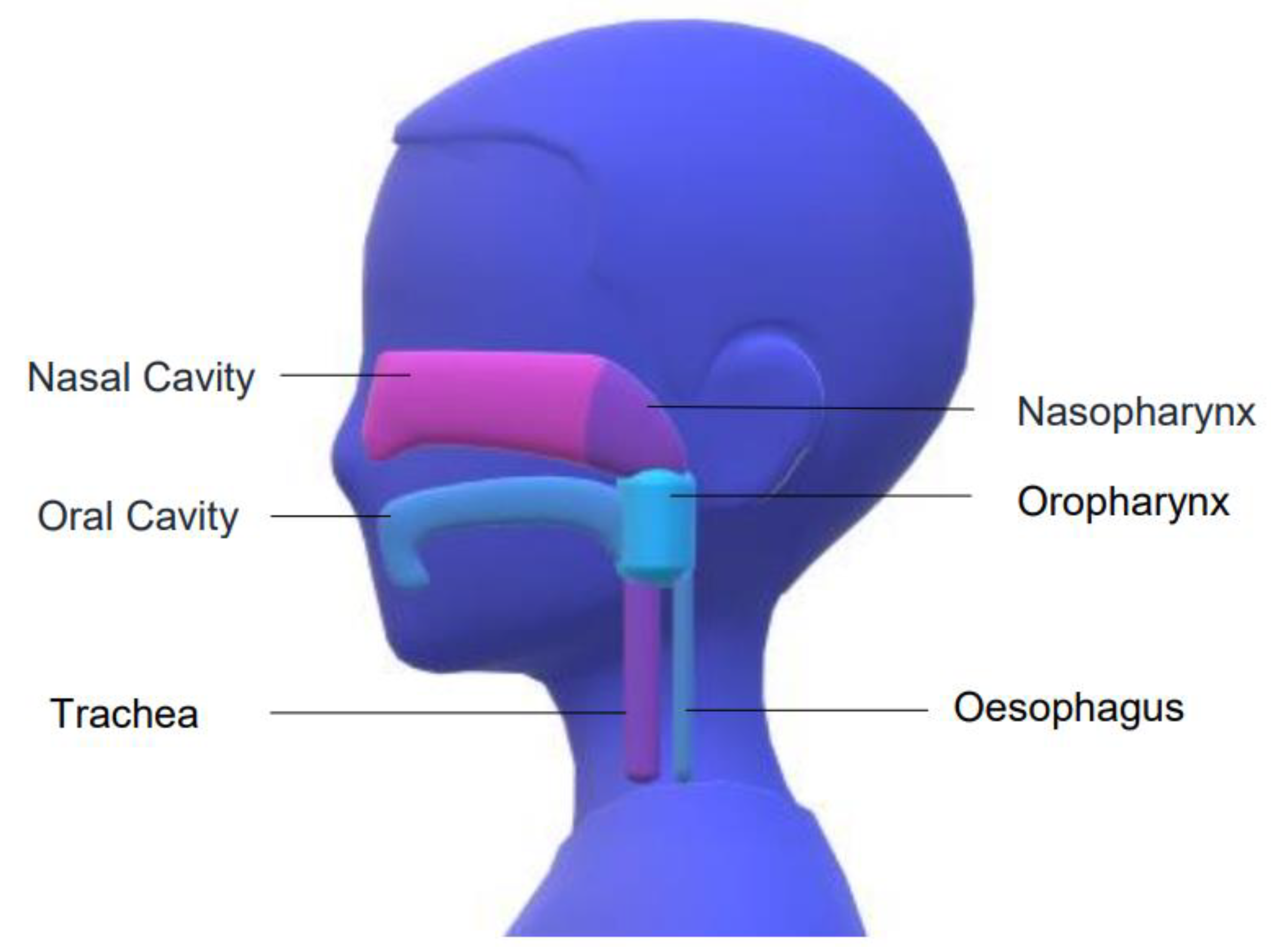
Higher viral loads present in the early course of a viral infection predominate more in the nose than in the throat, and slightly predominate in the nasopharynx than the anterior nasal cavity [8,9,10]. The nasopharynx is the uppermost portion of the throat lying at the back of the nasal cavity and accessible horizontally along the nasal floor, past occasionally obstructing turbinates and deviations of the septum (Figure 1).
There is a related but distinct microbiome between the anterior nares (AN) and nasopharynx [11]. A nasopharyngeal swab (NPS) is inserted to a depth equal to the distance from the nostril to the earlobe (nasotragal length, NTL), or until the nasopharynx is felt (a depth of up to 14 cm), with less deep swabs ≥ 5 cm sampling the middle turbinate or AN [12,13,14]. The NTL in children and infants is shorter but remains considerably longer than the 2cm depth occasionally cited in NPS studies, as described in pediatric intubation [15]. Combined oropharyngeal and anterior nasal swabs are shown to be comparable in sensitivity to a single sample of the nasopharynx, whilst benefiting from higher patient satisfaction [16,17]. These combined throat/nose swabs have become recommended practice for self-administration of the test. Paired oropharyngeal/NPSs convey increased sensitivity compared to NPS alone [18]. The swab type used is an important consideration, with greater yield of respiratory epithelial cells and greater patient satisfaction with a flocked swab (akin to a miniature toilet brush) than a rayon-tipped swab (resembling a long cotton “ear” bud), but pathogen detection rate is equivocal [19,20]. Other important pre-laboratory variables such as pre-impregnation of swabs with transport media, immediate placing in medium following collection, or refrigeration of the sample appear to add little to the diagnostic yield [21,22]. Nasal aspiration (NA) involves suction of mucous from the nasal cavity in a mucous trap subsequently rinsed with saline or transport medium. The similar but distinct nasal wash (NW), similarly described as the Naclerio method, is obtained by the drainage without suction of a small volume of saline flushed into the nose [23,24]. Samples obtained by nose blowing are not widely used, and the high prevalence of Staphylococcus aureus in these samples suggests microbial contamination from the AN, or external skin [25,26]. Unsurprisingly, a review of methods for Influenza detection found increased yield when pairing combinations of diverse methods [27].
In the absence of an unrelated gold standard, a composite reference standard combining these two imperfect tests can be used to create a “consensus standard” or “positive” rule against which to compare sensitivities [28,29]. In such cases without a true reference standard against which to expose false negatives, overall sensitivity will be overestimated. Nevertheless, head-to-head comparison of two such techniques with eyes open to this overall underestimation of total pathogen presence will still yield the best from two relatively “bad” options [30].
The current true sensitivity of nasopharyngeal swabbing for SARS-CoV-2 is estimated at 71–98% [31]. An increase in test sensitivity from 70–90% is enough to decrease by more than half the pre-test probability of infection at which one would still suspect an infection despite a negative test [32]. Thus, even a small increase in sensitivity by alteration of method could alter clinical practice. This systematic review was designed to compare the swabbing and aspirates per pathogen, laboratory method, and collection method using systematic methods.
2. Results
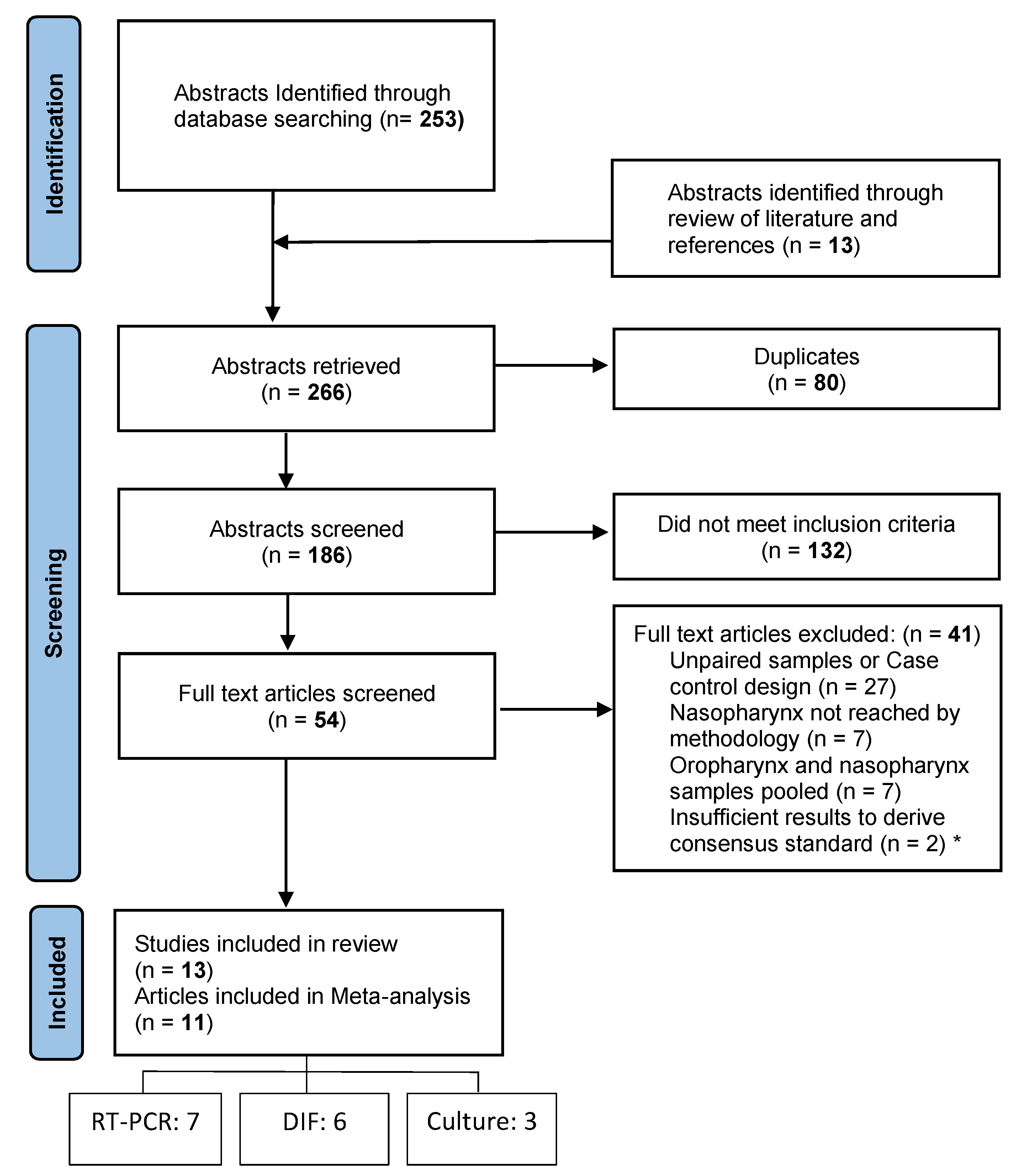
The initial search identified 253 articles (Figure 2). A further 13 were added from searching reference lists of key papers and reviews. After screening titles and abstracts, the abstracts of 186 publications were screened. Of the 54 abstracts that met the eligibility criteria, only 13 were eligible to be included in the final review after the full texts were reviewed. One study was an abstract published within a conference proceedings supplement.
2.1. Risk of Bias
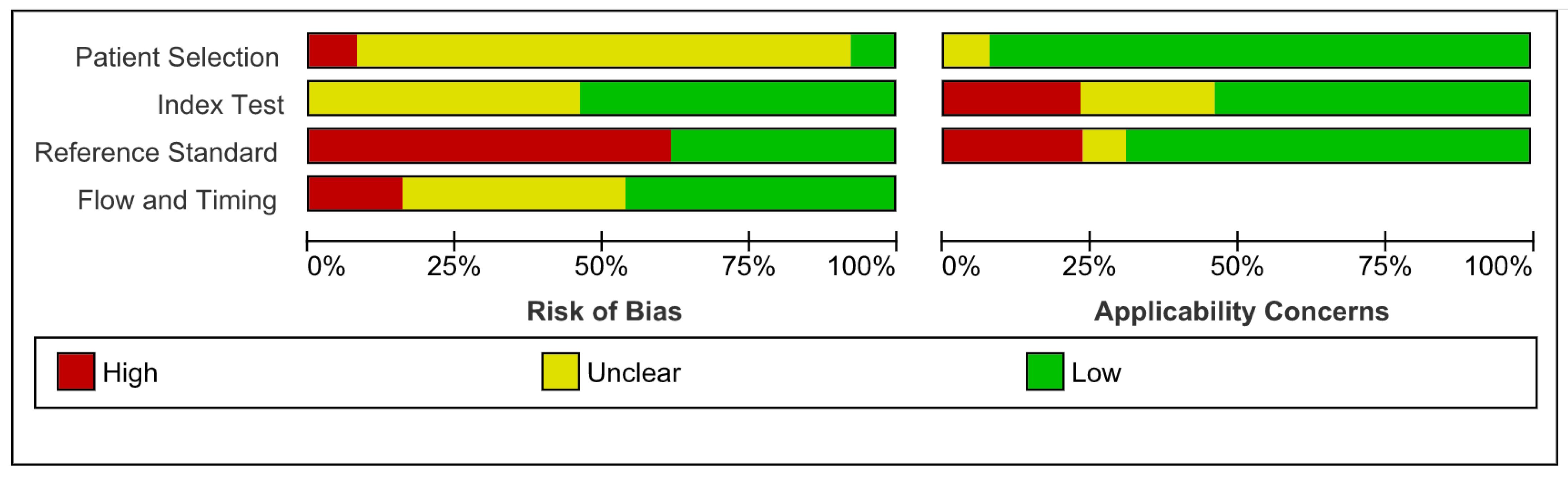
Using the QUADAS-2 tool, overall risk of bias was high: 8/13 studies displayed “high” risk of bias. Applicability concerns were “low” in 8/13 studies (Figure 3 and Figure 4). Lack of information on the patient selection process in 11/13 led to “unclear” risk of bias under patient selection. There were “low” applicability concerns due to patient selection, but this was a reflection of the review question including any and all populations; there was considerable homogeneity of age, ethnicity, or disease status. Three studies declared material support from companies manufacturing the testing kits.
2.2. Heterogeneity
The available literature was complicated by heterogeneity of participant age, participant health, laboratory methods, and collection methods, even within collection methods given the same name (Table 1).
2.3. Laboratory Methods
Methods used to detect pathogen carriage varied across studies. Eleven species-specific molecular methods were employed: seven using PCR and six using direct immunofluorescence, including one using both. Five different immunoassay kits were used for immunofluorescence. Three were cultured on inoculated Skim-milk-tryptone-glucose-glycerin for bacteria and one used the “R-mix” rapid culture method for viral growth. Where recorded, a negative cut-off was assigned to the Ct value > 40, with the exception of one, which was >35. Six used saline to transport the samples, six used viral transport medium, one used Guanidinium Thiocyanate Buffer, and one was unspecified.
2.4. Virology
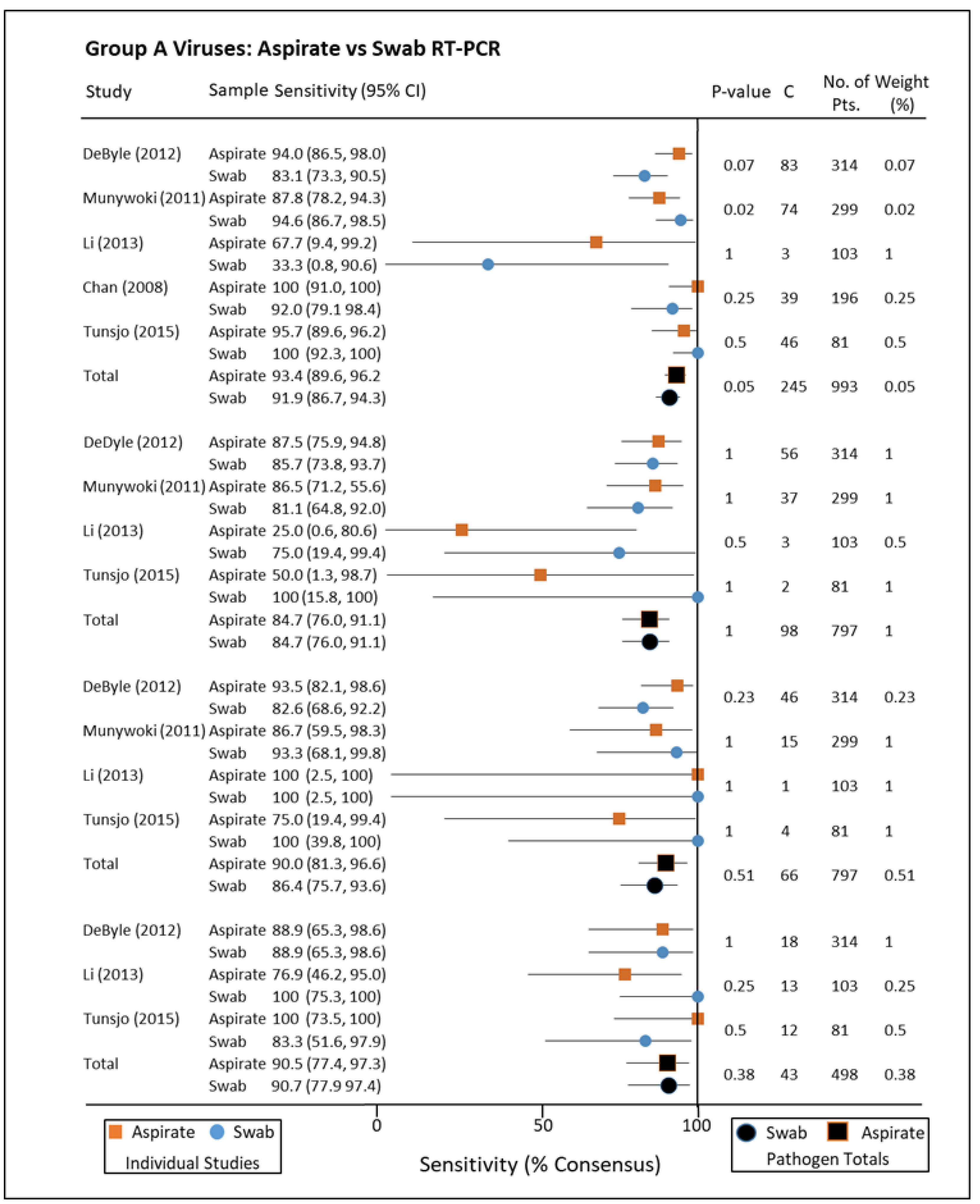
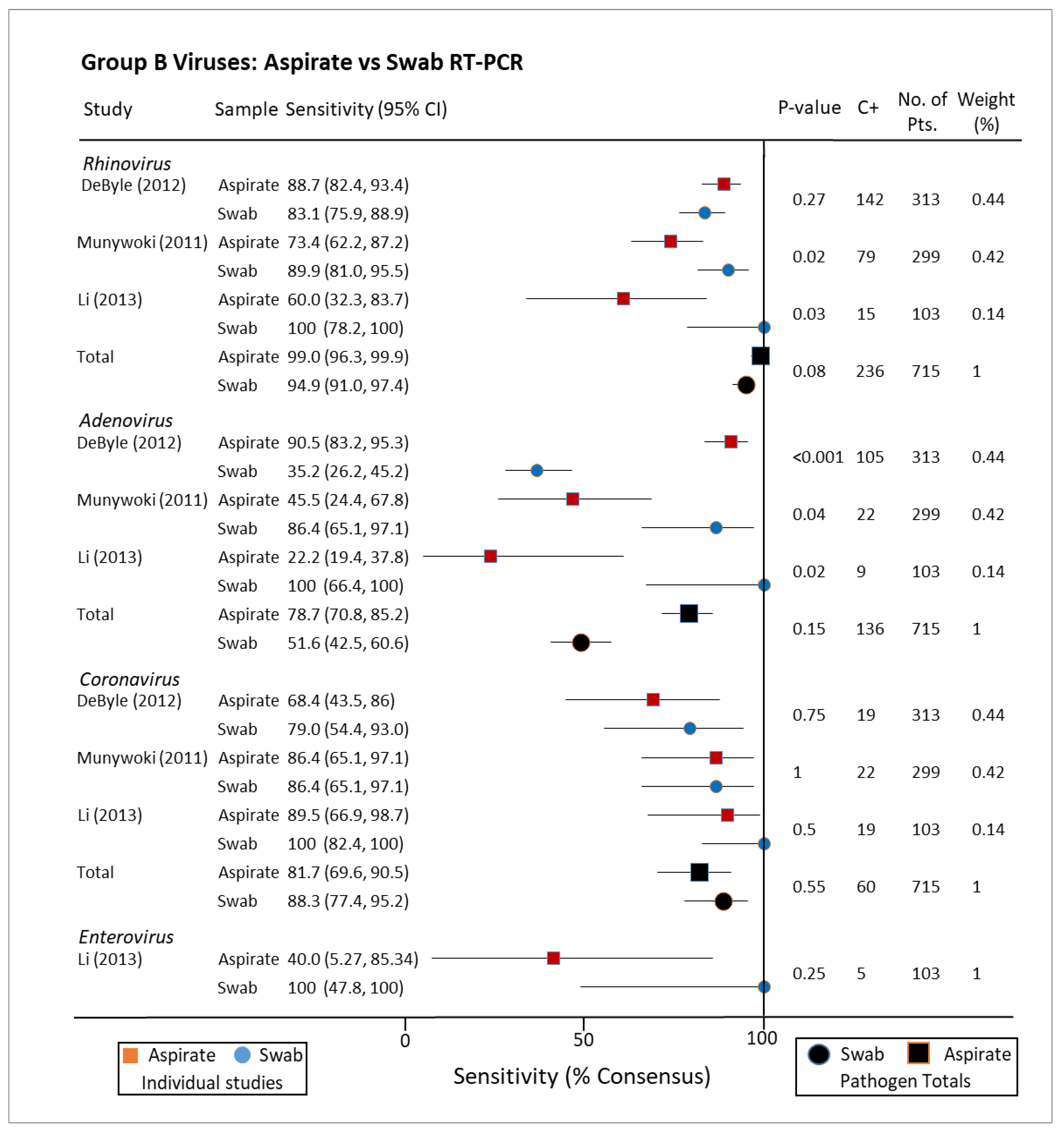
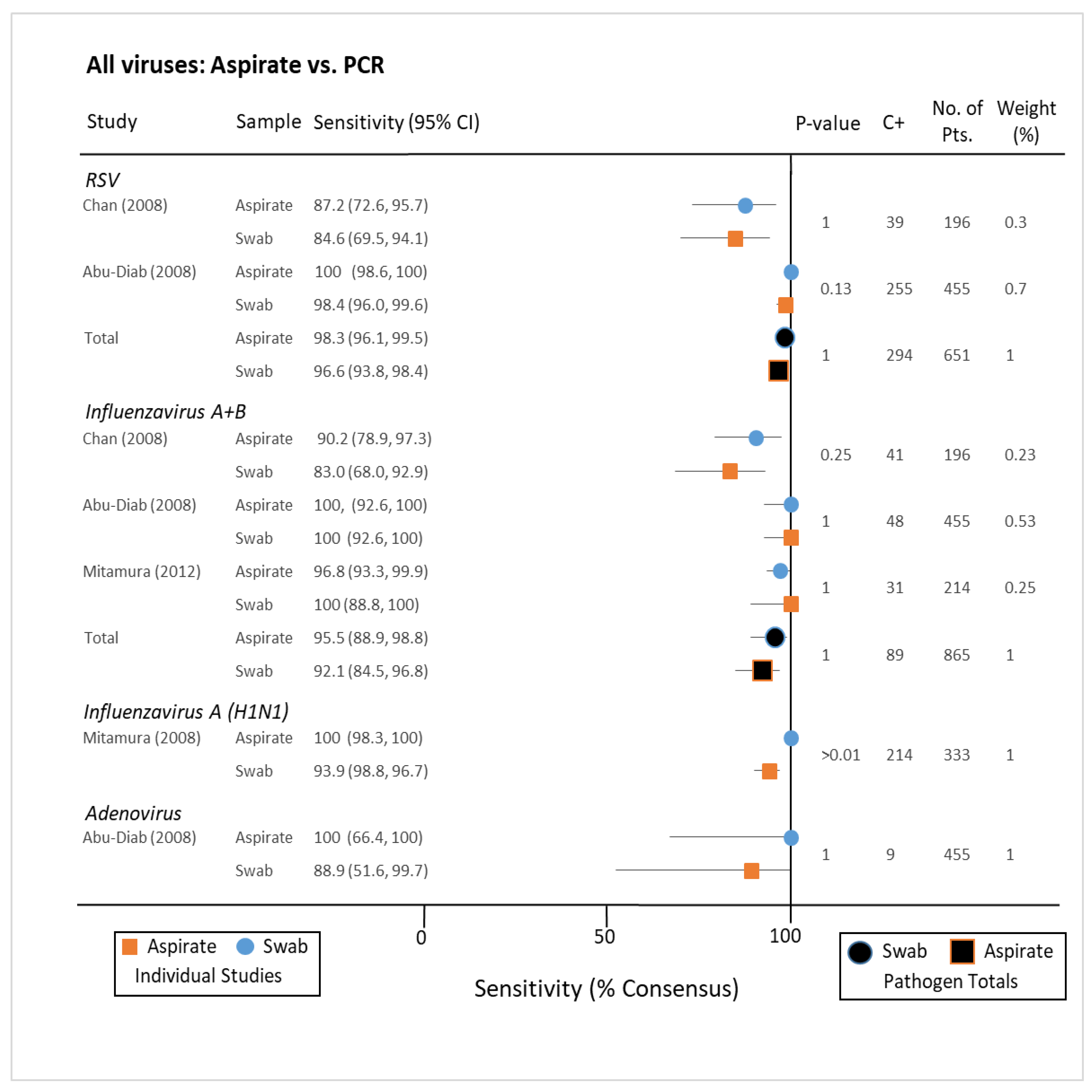
PCR analysis of NA and NPS for group A pathogens, i.e., those associated with hospitalising illness, included respiratory syncytial virus (RSV), parainfluenza virus, metapneumovirus, and influenza A+B (Figure 5). Sensitivities as a fraction of consensus standard (positive for either collection method) ranged between 84% and 96% for these pathogens by both collection methods. A similar lack of statistical dissimilarity was found when stratifying for group B viruses Rhinovirus, Adenovirus, Coronavirus, and Enterovirus (not normally associated with severe disease), but the range of sensitivities was greater (Figure 6) [33,34,35,36,37]. When immunofluorescence was utilized for diagnosis, there was little difference in sensitivity for either NA or NPS with the exception of one study exclusively testing for Influenza A H1N1(2009) (p < 0.001) [38,39]. When compared to nasal washes (similar to aspirates but without the use of suction), nasal swabs for influenza were similarly demonstrated to have greater sensitivity for detecting Influenza in one study of 122 participants (Figure 7) [40]. Another study of 89 paired samples, 25 nasopharyngeal washes compared to 26 swabs showed RSV carriage (p-value = 1) [41]. Many studies described findings seeming to advantage one collection method or other as a standalone, but this disappeared when pooled with others testing for the same pathogen by the same techniques. Indeed, when combined, the sensitivities of both collection methods for Parainfluenza virus were the same (84.7%/84.7%).
2.5. Bacteriology
Neither aspirate-wash versus swab for Bordetella pertussis PCR nor non-typable Haemophilus influenzae in culture yielded a significant advantage [42,43]. Collated sensitivities of the Naclerio method vs. NPS for a variety of species in 24 healthy British adults favored NPS for Neisseria (60.2%/100%), Diptherioids (66.7%/100%), and Alpha-haemolytic streptococci (18.8%/100%, p < 0.001), the Naclerio method for Staphylococcus aureus (100%/66.7%), and equivocal for Moraxella catarrhallis [33]. A similar number of Kenyan infants presenting to hospital with mild illness not requiring hospitalization, and having a suction catheter passed to the nasopharynx grew Streptococcus pneumoniae in 55 samples. In comparison, 47 (85.0%) of these grew the pathogen on their NPS (p = 0.005) [44]. These high yields may reflect the later adoption of the pneumococcal vaccine in Kenya in 2011 [45].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of included studies.
| Author | Year | Patients | Wash/Aspirate | Population | Lab Technique | Swab |
|---|---|---|---|---|---|---|
| DeByle [33] | 2012 | 314 | aspirate-wash | infants | RT-PCR | flocked |
| Chan [35] | 2008 | 196 | aspirate | Infants, children | DIF and RT-PCR | unknown |
| Suave [41] | 2012 | 89 | wash | Infants, children | DIF | flocked |
| Munywoki [34] | 2011 | 299 | aspirate-wash | Infants, children | RT-PCR | flocked |
| Abu-Diab [39] | 2008 | 455 | aspirate | Infants, children | DIF | flocked |
| Agoritsas [40] | 2006 | 122 | wash | Infants, children | DIF and viral culture | foam |
| Tunsjo [37] | 2015 | 81 | aspirate | infants | RT-PCR | flocked |
| Nunes [42] | 2016 | 484 | aspirate-wash | infants | RT-PCR | flocked |
| Li [35] | 2013 | 103 | aspirate-wash | adults | RT-PCR | flocked |
| Abdullahi [44] | 2007 | 62 | aspirate-wash | infants | culture | rayon tipped |
| Winokur [43] | 2013 | 15 | wash | adults | DIF | flocked |
| Gritzfeld [24] | 2011 | 24 | wash | adults | culture and RT-PCR | rayon tipped |
| Mitamura [38] | 2012 | 330 | aspirate | children, adults | DIF | unknown |
RT-PCR: reverse-transcriptase polymerase chain reaction; DIF: direct immunoflourescencel; aspirate-wash: studies that tested instilled saline removed by a suction catheter; aspirate: suctioning of nasal secretions without flushed water; wash: free drainage of instilled water.
3. Discussion
This systematic review found a moderate body of evidence comparing nasopharyngeal swabs with aspirates and washes with no significant difference in sensitivity. These are sufficient to recommend either method for optimal bacterial and viral coverage. Findings were predominantly from PCR-based diagnostics, comparing swabs with suction-using aspirates, and comparing viruses. Beyond these strata, data were sparse, particularly for purely wash-based methods, and for detection of bacteria. Statistical significance of higher NP swab sensitivity was high for H1N1(2009), but this same study found no clear advantage to this method for Influenza A or B. Some of the studies included were from an era of DIF and culture, which will have less relevance in future with the predominance of genomic diagnostics. Furthermore, the mechanics of removing pathogens from their in vivo habitat are poorly understood—swabbing and brushing are more abrasive and likely to access deeper layers of the mucosal barrier. Differences in adhesive properties of bacteria and viruses, as extra- and intracellular agents, respectively, remain, and the adhesive properties of biofilm also require further characterization [46].
3.1. Limitations of the Study
The abundance of confounding variables can only be accounted for in part by risk of bias assessments. Variations in transport, time in storage, and laboratory staff have not been considered. In the absence of a reference standard, the approximation of similar sensitivity rates for multiple different method comparisons implies saturation of this diagnostic chain; only on the smaller studies were large differences in sensitivities seen, and these not only disappeared when pooling studies but when comparing with better powered studies. This implies a limiting common denominator to all. Along the diagnostic chain from mucosa to laboratory bench, the step least likely to be controlled is the specific anatomical sampling technique. Single operator sampling under direct vision and controlled conditions, as described elsewhere, would be required for complete confidence in sampling [47]. This methodological heterogeneity can be controlled for in part by case matched control studies, where such variations were likely to affect both groups equally.
The Cochrane rapid review protocol proved a portable and efficient mode of prompt evidence synthesis for this timely clinical question with the use of open access freeware. Rapid reviews maintain a moderate degree of quality assessment while removing full search saturation and streamlining study selection and data extraction. As rapid reviews are an evolving methodology, it is unclear the extent to which methodological omissions compromise the quality of these results [48].
3.2. Limitations of Current Literature
Most published works to date focus on viral detection only. The clinical application of viral detection is not straightforward. Such techniques indicate only pathogen carriage and not severity of respiratory disease. Variations in viral shedding in the upper respiratory tract include: a shorter time to peak viral concentrations in saliva in SARS-CoV-2 compared to severe acute respiratory syndrome (SARS) (5 days vs. 7–10 days) and completed viral shedding of Influenza virus in adults is only completed around 5-7 days compared to infectivity persisting beyond 10 days in infants [49,50]. The attributable fraction, namely the percentage of times a disease is caused by a detected virus, ranges from 12% for Rhinovirus to 93% for RSV [51]. Thus, even truly reliable results do not confirm disease. Ergonomics also merit consideration: the washing method has been described as more comfortable for adults than a nasopharyngeal swab, and in children, anterior nasal swabbing results in lower infant distress score than an aspirate [23,31]. The Naclerio method requires a degree of coordination; however, that restricts its use to adults. The perceived and achieved discomfort may also be presumed to affect the thoroughness and accuracy in a linear fashion. A need for better understanding of anatomy of the nose in the literature is also called for. As the NP cannot be reached except via contact with the turbinates and septum, nasopharyngeal swabs may be more appropriately named a “pan-nasal” swab.
3.3. Future Directions
How else to augment sensitivity? Moist swabs appear to add little advantage over dry swabs; repeated titres in severe cases may give a retrospective estimate of the sensitivity of initial samples [52,53]. This study looked at viral and bacterial carriage. This still leaves the issue of the best method for sampling wider nasal ecology in the era of next generation sequencing. Increased diversity of microbiota can be removed from brushing the inferior turbinate compared with nasal washing [54]. Given this niche-specific diversity, it is difficult to assess if such variations denote a different topographical area being sampled or a different constellation of organisms being easier to remove from the nasal lining. Gradual mapping of the nasopharyngeal microbiome over lifespan is a prerequisite to the future application of such technologies to diagnostics and therapy [55]. Emerging point-of-care diagnostics are in readiness to accelerate all accurate and reliable respiratory pathogen sampling to guide timely treatment and surveillance on a global level but will rely on the most sensitive sampling methods available [56].
4. Materials and Methods
4.1. Protocol
The protocol followed guidance from the Cochrane Rapid Reviews Methods Group. Rapid reviews streamline evidence synthesis methods such as one-person title screening and elimination of grey literature, while maintaining a high degree of rigor [57]. The preferred reporting items for systematic reviews and meta-analyses (PRISMA) and the Cochrane handbook for diagnostic test accuracy reviews were used [58,59]. The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) prior to formal screening of search results against eligibility criteria. Consultation with stakeholders in medicine and a public focus group aided the study design.
4.2. Inclusion Criteria
All studies comparing sensitivity in microbiological sampling for the upper respiratory tract were sought. Variations in viruses, bacteria and fungi detected and differing laboratory techniques were included and stratified by these categories in the reported results. Studies were limited to those in humans, and those since the first publication of WHO guidelines on swab and aspirate collection in 2006 [32]. Pooled samples between different anatomical sites were excluded, such as swabbing of the nose and throat by the same swab or where samples were not paired from the same patient. Where a consensus standard was not included or this information could not be calculated, these studies were also excluded.
4.3. Nasopharynx Definition
Nasopharyngeal swabs were defined as swabbing to a depth of >5 cm in adults and >3 cm in children or with relevant reference to surface anatomy, by citing WHO guidelines for swab collection, or following the same methodology as other studies to the same effect. Where these data were lacking, the authors were contacted for clarification, and/or judgments made on appropriate anatomical nomenclature and documented staff training. Broad interpretation of the term “nasopharynx” elsewhere in the literature to include the middle turbinate and AN led to the inclusion of ‘nasopharyngeal’ studies without further methodological detail but graded ‘high’ for applicability concerns.
4.4. Search Strategy
Cochrane CENTRAL, MEDLINE, and Embase were searched on 09/06/2020, followed by supplemental exploration of reference lists of review articles. Help of a specialist health librarian was sought to ensure that wording variations and the correct Boolean operators optimized search saturation. Full details of search terms are accessible online via the protocol (PROSPERO registration no. CRD42020189577).
4.5. Screening
A title and abstract screening form was piloted using 30 abstracts and adopted without modification to dual screen 20% of abstracts with conflict resolution. Remaining abstracts were screened by one reviewer, and a second reviewer screened all excluded abstracts. A full text screening form was piloted using 5 full text articles with the same process. Rayyan QCRI was used to streamline the selection process.
4.6. Data Extraction
Results were stratified by virus, bacteria, and differing laboratory techniques. Aspirates are defined as extraction of fluids by suction catheter and washes as free drainage of instilled saline into a dish. A third hybrid method, where flushed water was then aspirated, has been incorporated under Aspirates [32]. Where studies included multiple sampling methods, only relevant data were used. Where the consensus standard was equal to the sensitivity of one of the sampling methods, i.e., there were no false negatives for one of the two collection methods, these data were acknowledged as having a ‘high’ risk of bias.
4.7. Data Analysis
Meta-analysis was summarized for studies with similar methodologies; for more sparse and/or heterogeneous evidence, a narrative summary is offered. Sensitivity analysis and McNemars’ test for paired samples were derived using Medcalc and Scistat online statistical software, respectively.
4.8. Risk of Bias Assessment
The QUADAS-2 risk of bias tool for diagnostic test accuracy reviews was used to grade risk of bias and applicability concerns by one reviewer (MF) with verification by second viewer (JD). Due to risks unique to this study, the questions “Were false negatives two-sided?” under reference standard, and “Were separate nostrils used?” were added under flow and timing. Risk of bias tables were generated in Review Manager 5.
Author Contributions
Conceptualization, M.F.F.; methodology, M.F.F., M.K. and J.S.G.D.; software, M.F.F.; validation, J.S.G.D.; formal analysis, M.F.F. and J.S.G.D.; writing—original draft preparation, M.F.F.; writing—review and editing, M.F.F., M.K. and J.S.G.D.; supervision, M.K. and J.S.G.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Full protocol data, including inclusion and exclusion criteria and search terms can be accessed on the PROSPERO register registration no. CRD42020189577 https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020189577 (accessed on 10 October 2021); Web and mobile application Rayyan QCRI can be accessed for free at https://www.rayyan.ai/ (accessed on 10 October 2021); Diagnostic test evaluation calculator (MedCalc) can be accessed at https://www.medcalc.org/calc/diagnostic_test.php (accessed on 10 October 2021); McNemar’s test on paired proportions (SciStat) can be accessed at https://www.scistat.com/statisticaltests/mcnemar.php (accessed on 10 October 2021); Review Manager 5 (The Cochrane Collaboration) can be accessed at revman.cochrane.org (accessed on 10 October 2021); QUADAS-2 Risk of Bias tool (University of Bristol) can be accessed at https://www.bristol.ac.uk/population-health-sciences/projects/quadas/quadas-2/ (accessed on 10 October 2021).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyse |
| QUADAS-2 | Quality Assessment of Diagnostic Accuracy Studies-2 |
| (RT-)(q-)PCR | (Reverse Transcriptase) (quantitative)Polymerase Chain Reaction |
| SARS(-CoV-19) | Severe Acute Respiratory Syndrome (Coronavirus-2019) |
| DIF | Direct Immunofluorescence |
| NPS | Nasopharyngeal Swab |
| NTL | Naso-tragal Length |
| NA | Nasal Aspiration |
| NW | Nasal Wash |
| PROSPERO | International prospective register of systematic reviews |
| WHO | World Health Organisation |
| Rayyan QCRI | Rayyan Qatar Computing Research Institute |
| RevMan | Review Manager |
| 16S-rRNA | 16S-Ribosomal Ribonucleic Acid |
References
- Centers for Disease Control and Prevention. Information on Rapid Molecular Assays, RT-PCR, and Other Molecular Assays for Diagnosis of Influenza Virus Infection. 2019. Available online: https://www.cdc.gov/flu/professionals/diagnosis/molecular-assays.htm (accessed on 10 November 2021).
- World Health Organization. Surveillance Strategies for COVID-19 Human Infection: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. WHO Recommendations on the Use of Rapid Testing for Influenza Diagnosis; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Chartrand, C.; Tremblay, N.; Renaud, C.; Papenburg, J. Diagnostic Accuracy of Rapid Antigen Detection Tests for Respiratory Syncytial Virus Infection: Systematic Review and Meta-analysis. J. Clin. Microbiol. 2015, 53, 3738–3749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steininger, C.; Kundi, M.; Aberle, S.W.; Aberle, J.H.; Popow-Kraupp, T. Effectiveness of reverse transcription-PCR, virus isolation, and enzyme-linked immunosorbent assay for diagnosis of influenza A virus infection in different age groups. J. Clin. Microbiol. 2002, 40, 2051–2056. [Google Scholar] [CrossRef] [Green Version]
- Kuypers, J.; Wright, N.; Ferrenberg, J.; Huang, M.L.; Cent, A.; Corey, L.; Morrow, R. Comparison of real-time PCR assays with fluorescent-antibody assays for diagnosis of respiratory virus infections in children. J. Clin. Microbiol. 2006, 44, 2382–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Mawaddah, A.; Gendeh, H.S.; Lum, S.G.; Marina, M.B. Upper respiratory tract sampling in COVID-19. Malays. J. Pathol. 2020, 42, 23–35. [Google Scholar]
- Callahan, C.; Lee, R.; Lee, G.; Zulauf, K.E.; Kirby, J.E.; Arnaout, R. Nasal-Swab Testing Misses Patients with Low SARS-CoV-2 Viral Loads. medRxiv 2020. [Google Scholar] [CrossRef]
- Luna, P.N.; Hasegawa, K.; Ajami, N.J.; Espinola, J.A.; Henke, D.M.; Petrosino, J.F.; Piedra, P.A.; Sullivan, A.F.; Camargo, C.A., Jr.; Shaw, C.A.; et al. The association between anterior nares and nasopharyngeal microbiota in infants hospitalized for bronchiolitis. Microbiome 2018, 6, 2. [Google Scholar] [CrossRef]
- Satzke, C.; Turner, P.; Virolainen-Julkunen, A.; Adrian, P.V.; Antonio, M.; Hare, K.M.; Henao-Restrepo, A.M.; Leach, A.J.; Klugman, K.P.; Porter, B.D.; et al. WHO Pneumococcal Carriage Working Group. Standard method for detecting upper respiratory carriage of Streptococcus pneumoniae: Updated recommendations from the World Health Organization Pneumococcal Carriage Working Group. Vaccine 2013, 32, 165–179. [Google Scholar] [CrossRef]
- Gizurarson, S. Anatomical and histological factors affecting intranasal drug and vaccine delivery. Curr. Drug Deliv. 2012, 9, 566–582. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Li, N.; Dong, N. How to Obtain a Nasopharyngeal Swab Specimen. N. Engl. J. Med. 2020, 383, e14. [Google Scholar] [PubMed]
- Gray, M.M.; Delaney, H.; Umoren, R.; Strandjord, T.P.; Sawyer, T. Accuracy of the nasal-tragus length measurement for correct endotracheal tube placement in a cohort of neonatal resuscitation simulators. J. Perinatol. 2017, 37, 975–978. [Google Scholar] [CrossRef]
- LeBlanc, J.J.; Heinstein, C.; MacDonald, J.; Pettipas, J.; Hatchette, T.F.; Patriquin, G. A combined oropharyngeal/nares swab is a suitable alternative to nasopharyngeal swabs for the detection of SARS-CoV-2. J. Clin. Virol. 2020, 128, 104442. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, P.; Denham, J.; Assous, J.; Hughes, C. RSV testing in bronchiolitis: Which nasal sampling method is best? Arch. Dis. Child. 2005, 90, 634–635. [Google Scholar] [CrossRef] [PubMed]
- Ek, P.; Böttiger, B.; Dahlman, D.; Hansen, K.B.; Nyman, M.; Nilsson, A.C. A combination of naso- and oropharyngeal swabs improves the diagnostic yield of respiratory viruses in adult emergency department patients. Infect. Dis. 2019, 51, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Daley, P.; Castriciano, S.; Chernesky, M.; Smieja, M. Comparison of flocked and rayon swabs for collection of respiratory epithelial cells from uninfected volunteers and symptomatic patients. J. Clin. Microbiol. 2006, 44, 2265–2267. [Google Scholar] [CrossRef] [Green Version]
- Bruijns, B.B.; Tiggelaar, R.M.; Gardeniers, H. The Extraction and Recovery Efficiency of Pure DNA for Different Types of Swabs. J. Forensic Sci. 2018, 63, 1492–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, S.; Molteni, C.G.; Daleno, C.; Valzano, A.; Cesati, L.; Gualtieri, L.; Tagliabue, C.; Bosis, S.; Principi, N. Comparison of nasopharyngeal nylon flocked swabs with universal transport medium and rayon-bud swabs with a sponge reservoir of viral transport medium in the diagnosis of paediatric influenza. J. Med. Microbiol. 2010, 59 Pt 1, 96–99. [Google Scholar] [CrossRef]
- Moore, C.; Corden, S.; Sinha, J.; Jones, R. Dry cotton or flocked respiratory swabs as a simple collection technique for the molecular detection of respiratory viruses using real-time NASBA. J. Virol. Methods 2008, 153, 84–89. [Google Scholar] [CrossRef]
- World Health Organization. Collecting, Preserving and Shipping Specimens for the Diagnosis of Avian Influenza A(H5N1) Virus Infection Guide for Field Operations. 2006. Available online: https://www.who.int/ihr/publications/CDS_EPR_ARO_2006_1.pdf. (accessed on 10 November 2021).
- Gritzfeld, J.F.; Roberts, P.; Roche, L.; El Batrawy, S.; Gordon, S.B. Comparison between nasopharyngeal swab and nasal wash, using culture and PCR, in the detection of potential respiratory pathogens. BMC Res. Notes 2011, 4, 122. [Google Scholar] [CrossRef] [Green Version]
- Leach, A.J.; Stubbs, E.; Hare, K.; Beissbarth, J.; Morris, P.S. Comparison of nasal swabs with nose blowing for community-based pneumococcal surveillance of healthy children. J. Clin. Microbiol. 2008, 46, 2081–2082. [Google Scholar] [CrossRef] [Green Version]
- Van den Bergh, M.R.; Bogaert, D.; Dun, L.; Vons, J.; Chu, M.L.; Trzciński, K.; Veenhoven, R.H.; Sanders, E.A.; Schilder, A.M. Alternative sampling methods for detecting bacterial pathogens in children with upper respiratory tract infections. J. Clin. Microbiol. 2012, 50, 4134–4137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, S.; Thompson, M.G.; Flannery, B.; Fry, A. Comparison of Respiratory Specimen Collection Methods for Detection of Influenza Virus Infection by Reverse Transcription-PCR: A Literature Review. J. Clin. Microbiol. 2019, 57, e00027-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, S.; Hemyari, P.; Canchola, J.A.; Duncan, J. Dual composite reference standards (dCRS) in molecular diagnostic research: A new approach to reduce bias in the presence of Imperfect reference. J. Biopharm. Stat. 2018, 28, 951–965. [Google Scholar] [CrossRef]
- Umemneku Chikere, C.M.; Wilson, K.; Graziadio, S.; Vale, L.; Allen, A.J. Diagnostic test evaluation methodology: A systematic review of methods employed to evaluate diagnostic tests in the absence of gold standard-An update. PLoS ONE 2019, 14, e0223832. [Google Scholar] [CrossRef]
- Worster, A.; Carpenter, C. Incorporation bias in studies of diagnostic tests: How to avoid being biased about bias. CJEM 2008, 10, 174–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arevalo-Rodriguez, I.; Buitrago-Garcia, D.; Simancas-Racines, D.; Zambrano-Achig, P.; Del Campo, R.; Ciapponi, A.; Sued, O.; Martinez-García, L.; Rutjes, A.; Low, N.; et al. False-negative results of initial RT-PCR assays for COVID-19: A systematic review. PLoS ONE 2020, 15, e0242958. [Google Scholar] [CrossRef] [PubMed]
- Woloshin, S.; Patel, N.; Kesselheim, A.S. False Negative Tests for SARS-CoV-2 Infection-Challenges and Implications. N. Engl. J. Med. 2020, 383, e38. [Google Scholar] [CrossRef]
- Debyle, C.; Bulkow, L.; Miernyk, K.; Chikoyak, L.; Hummel, K.B.; Hennessy, T.; Singleton, R. Comparison of nasopharyngeal flocked swabs and nasopharyngeal wash collection methods for respiratory virus detection in hospitalized children using real-time polymerase chain reaction. J. Virol. Methods 2012, 185, 89–93. [Google Scholar] [CrossRef]
- Munywoki, P.K.; Hamid, F.; Mutunga, M.; Welch, S.; Cane, P.; Nokes, D.J. Improved detection of respiratory viruses in pediatric outpatients with acute respiratory illness by real-time PCR using nasopharyngeal flocked swabs. J. Clin. Microbiol. 2011, 49, 3365–3367. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Chen, Q.Y.; Li, Y.Y.; Wang, Y.F.; Yang, Z.F.; Zhong, N.S. Comparison among nasopharyngeal swab, nasal wash, and oropharyngeal swab for respiratory virus detection in adults with acute pharyngitis. BMC Infect. Dis. 2013, 13, 281. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.H.; Peiris, J.S.; Lim, W.; Nicholls, J.M.; Chiu, S.S. Comparison of nasopharyngeal flocked swabs and aspirates for rapid diagnosis of respiratory viruses in children. J. Clin. Virol. 2008, 42, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Tunsjø, H.S.; Berg, A.S.; Inchley, C.S.; Røberg, I.K.; Leegaard, T.M. Comparison of nasopharyngeal aspirate with flocked swab for PCR-detection of respiratory viruses in children. APMIS 2015, 123, 473–477. [Google Scholar] [CrossRef]
- Mitamura, K.; Kawakami, C.; Shimizu, H.; Abe, T.; Konomi, Y.; Yasumi, Y.; Yamazaki, M.; Ichikawa, M.; Sugaya, N. Evaluation of a new immunochromatographic assay for rapid identification of influenza A, B, and A(H1N1)2009 viruses. J. Infect. Chemother. 2013, 19, 633–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu-Diab, A.; Azzeh, M.; Ghneim, R.; Ghneim, R.; Zoughbi, M.; Turkuman, S.; Rishmawi, N.; Issa, A.E.; Siriani, I.; Dauodi, R.; et al. Comparison between pernasal flocked swabs and nasopharyngeal aspirates for detection of common respiratory viruses in samples from children. J. Clin. Microbiol. 2008, 46, 2414–2417. [Google Scholar] [CrossRef] [Green Version]
- Agoritsas, K.; Mack, K.; Bonsu, B.K.; Goodman, D.; Salamon, D.; Marcon, M.J. Evaluation of the Quidel QuickVue test for detection of influenza A and B viruses in the pediatric emergency medicine setting by use of three specimen collection methods. J. Clin. Microbiol. 2006, 44, 2638–2641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suave, L.; Doan, Q.; Steer, Q.; Book, L.; Tilley, P. Flocked nasopharyngeal swabs vs nasopharyngeal wash for the diagnosis of respiratory viruses in children. Can. J. Infect. Dis. Med. Microbiol. 2012, 23 (Suppl. 1), 53b. [Google Scholar]
- Nunes, M.C.; Soofie, N.; Downs, S.; Tebeila, N.; Mudau, A.; de Gouveia, L.; Madhi, S.A. Comparing the Yield of Nasopharyngeal Swabs, Nasal Aspirates, and Induced Sputum for Detection of Bordetella pertussis in Hospitalized Infants. Clin. Infect. Dis. 2016, 63 (Suppl. 4), S181–S186. [Google Scholar] [CrossRef]
- Winokur, P.L.; Chaloner, K.; Doern, G.V.; Ferreira, J.; Apicella, M.A. Safety and immunological outcomes following human inoculation with nontypeable Haemophilus influenzae. J. Infect. Dis. 2013, 208, 728–738. [Google Scholar] [CrossRef] [Green Version]
- Abdullahi, O.; Wanjiru, E.; Musyimi, R.; Glass, N.; Scott, J.A. Validation of nasopharyngeal sampling and culture techniques for detection of Streptococcus pneumoniae in children in Kenya. J. Clin. Microbiol. 2007, 45, 3408–3410. [Google Scholar] [CrossRef] [Green Version]
- Hammitt, L.L.; Etyang, A.O.; Morpeth, S.C.; Ojal, J.; Mutuku, A.; Mturi, N.; Moisi, J.C.; Adetifa, I.M.; Karani, A.; Akech, D.O.; et al. Effect of ten-valent pneumococcal conjugate vaccine on invasive pneumococcal disease and nasopharyngeal carriage in Kenya: A longitudinal surveillance study. Lancet 2019, 393, 2146–2154. [Google Scholar] [CrossRef] [Green Version]
- Suh, J.D.; Ramakrishnan, V.; Palmer, J.N. Biofilms. Otolaryngol. Clin. N. Am. 2010, 43, 521–530. [Google Scholar] [CrossRef]
- Lu, Y.T.; Wang, S.H.; Liou, M.L.; Shen, T.A.; Lu, Y.C.; Hsin, C.H.; Yang, S.F.; Chen, Y.Y.; Chang, T.H. Microbiota Dysbiosis in Fungal Rhinosinusitis. J. Clin. Med. 2019, 8, 1973. [Google Scholar] [CrossRef] [Green Version]
- Gartlehner, G.; Affengruber, L.; Titscher, V.; Noel-Storr, A.; Dooley, G.; Ballarini, N.; König, F. Single-reviewer abstract screening missed 13 percent of relevant studies: A crowd-based, randomized controlled trial. J. Clin. Epidemiol. 2020, 121, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Lau, L.L.; Cowling, B.J.; Fang, V.J.; Chan, K.H.; Lau, E.H.; Lipsitch, M.; Cheng, C.K.; Houck, P.M.; Uyeki, T.M.; Peiris, J.S.; et al. Viral shedding and clinical illness in naturally acquired influenza virus infections. J. Infect. Dis. 2010, 201, 1509–1516. [Google Scholar] [CrossRef] [Green Version]
- Self, W.H.; Williams, D.J.; Zhu, Y.; Ampofo, K.; Pavia, A.T.; Chappell, J.D.; Hymas, W.C.; Stockmann, C.; Bramley, A.M.; Schneider, E.; et al. Respiratory Viral Detection in Children and Adults: Comparing Asymptomatic Controls and Patients with Community-Acquired Pneumonia. J. Infect. Dis. 2016, 213, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Warnke, P.; Devide, A.; Weise, M.; Frickmann, H.; Schwarz, N.G.; Schäffler, H.; Ottl, P.; Podbielski, A. Utilizing Moist or Dry Swabs for the Sampling of Nasal MRSA Carriers? An In Vivo and In Vitro Study. PLoS ONE 2016, 11, e0163073. [Google Scholar] [CrossRef] [Green Version]
- Hagiya, H.; Mio, M.; Murase, T.; Egawa, K.; Kokumai, Y.; Uchida, T.; Morimoto, N.; Otsuka, F.; Shiota, S. Is wet swab superior to dry swab as an intranasal screening test? J. Intensiv. Care 2013, 1, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Losada, M.; Crandall, K.A.; Freishtat, R.J. Two sampling methods yield distinct microbial signatures in the nasopharynges of asthmatic children. Microbiome 2016, 4, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, M.; Dooley, J. The microbiome of the nasopharynx. J. Med. Microbiol. 2021, 70, 001368. [Google Scholar] [CrossRef] [PubMed]
- Chartrand, C.; Leeflang, M.M.; Minion, J.; Brewer, T.; Pai, M. Accuracy of rapid influenza diagnostic tests: A meta-analysis. Ann. Intern. Med. 2012, 156, 500–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garritty, C.; Gartlehner, G.; Kamel, C.; King, V.; Nussbaumer-Streit, B.; Stevens, A. Cochrane Rapid Reviews. Interim Guidance from the Cochrane Rapid Reviews Methods Group. J. Clin. Epidemiol. 2020, 130, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.J.; Wisniewski, S.; Davenport, C. Chapter 4: Guide to the contents of a Cochrane Diagnostic Test Accuracy Protocol. In Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy Version 1.0.0; Deeks, J.J., Bossuyt, P.M., Gatsonis, C., Eds.; The Cochrane Collaboration: London, UK, 2013; Available online: http://srdta.cochrane.org/ (accessed on 16 October 2021).
Figure 1.
Anatomy of the Upper Respiratory Tract.

Figure 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Flow chart. RT PCR: Reverse Transcriptase Polymerase Chain Reaction; DIF: Immunoflourescence; * Several studies met more than one exclusion criteria and/or used multiple laboratory methods.
Figure 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Flow chart. RT PCR: Reverse Transcriptase Polymerase Chain Reaction; DIF: Immunoflourescence; * Several studies met more than one exclusion criteria and/or used multiple laboratory methods.

Figure 3.
Methodological Quality Summary Chart.

Figure 4.
Methodological Quality Summary Table.

Figure 5.
Group A viruses: aspirates vs. swab, reverse transcriptase polymerase chain reaction. RSV: respiratory syncytial virus; CI: confidence interval; C+: total consensus positive; No. of Pts.: number of patients; RT-PCR: reverse transcriptase polymerase chain reaction.
Figure 5.
Group A viruses: aspirates vs. swab, reverse transcriptase polymerase chain reaction. RSV: respiratory syncytial virus; CI: confidence interval; C+: total consensus positive; No. of Pts.: number of patients; RT-PCR: reverse transcriptase polymerase chain reaction.

Figure 6.
Group B viruses: aspirates vs. swab, reverse transcriptase polymerase chain reaction. CI: confidence interval; C+: total consensus positive; No. of Pts.: number of patients; RT-PCR: reverse transcriptase polymerase chain reaction.
Figure 6.
Group B viruses: aspirates vs. swab, reverse transcriptase polymerase chain reaction. CI: confidence interval; C+: total consensus positive; No. of Pts.: number of patients; RT-PCR: reverse transcriptase polymerase chain reaction.

Figure 7.
All viruses: aspirates vs. swab, direct immunoflourescence. RSV: respiratory syncytial virus; CI: confidence interval; C+: total consensus positive; No. of Pts.: number of patients; DIF: direct immunofluorescence.
Figure 7.
All viruses: aspirates vs. swab, direct immunoflourescence. RSV: respiratory syncytial virus; CI: confidence interval; C+: total consensus positive; No. of Pts.: number of patients; DIF: direct immunofluorescence.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Flynn, M.F.; Kelly, M.; Dooley, J.S.G. Nasopharyngeal Swabs vs. Nasal Aspirates for Respiratory Virus Detection: A Systematic Review. Pathogens 2021, 10, 1515. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111515
AMA Style
Flynn MF, Kelly M, Dooley JSG. Nasopharyngeal Swabs vs. Nasal Aspirates for Respiratory Virus Detection: A Systematic Review. Pathogens. 2021; 10(11):1515. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111515
Chicago/Turabian StyleFlynn, Matthew F., Martin Kelly, and James S. G. Dooley. 2021. "Nasopharyngeal Swabs vs. Nasal Aspirates for Respiratory Virus Detection: A Systematic Review" Pathogens 10, no. 11: 1515. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10111515
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.