
Transfusion Transmissible Infections in Blood Donors in the Province of Bié, Angola, during a 15-Year Follow-Up, Imply the Need for Pathogen Reduction Technologies


 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Blood Donor Profile
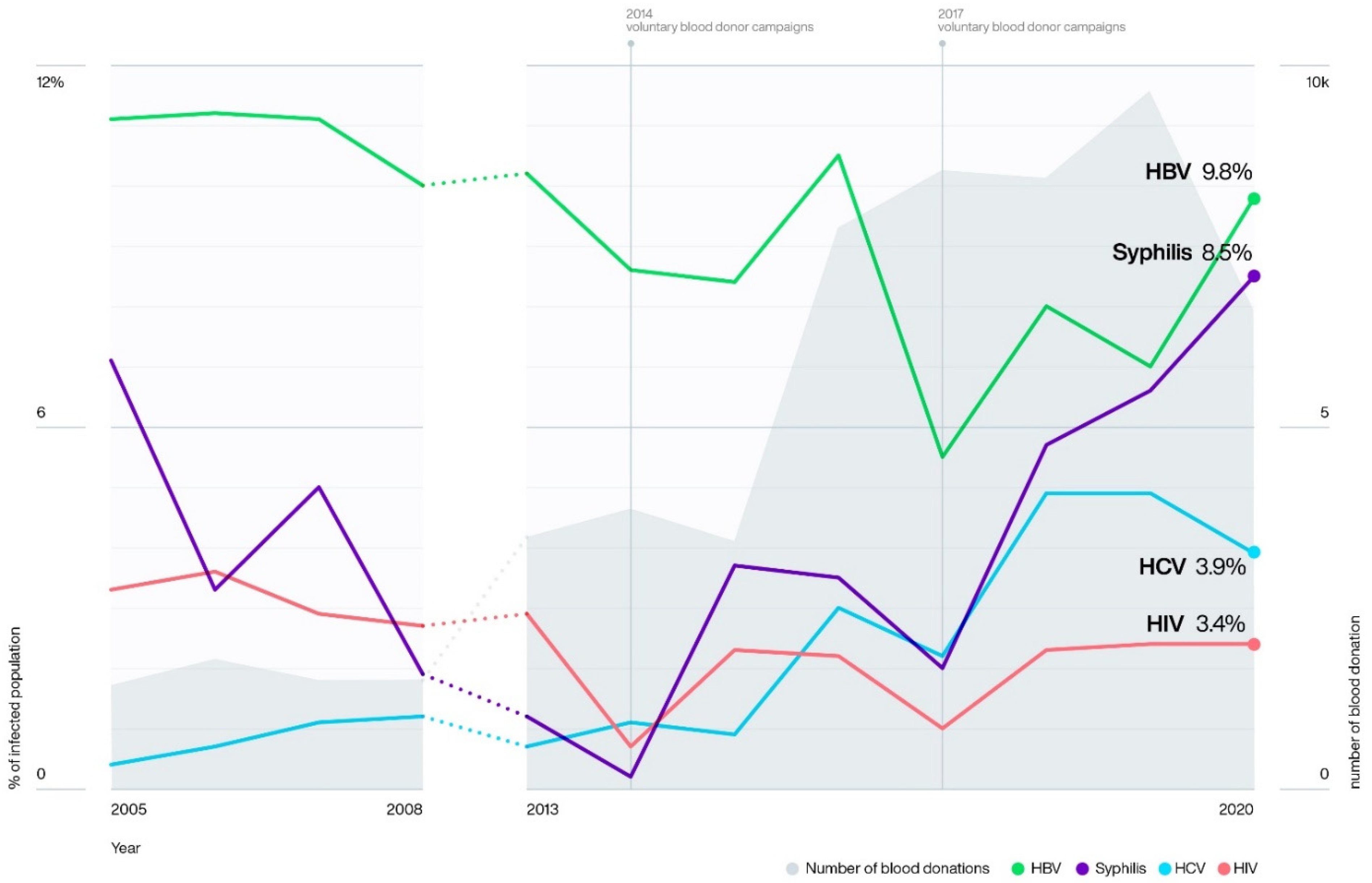
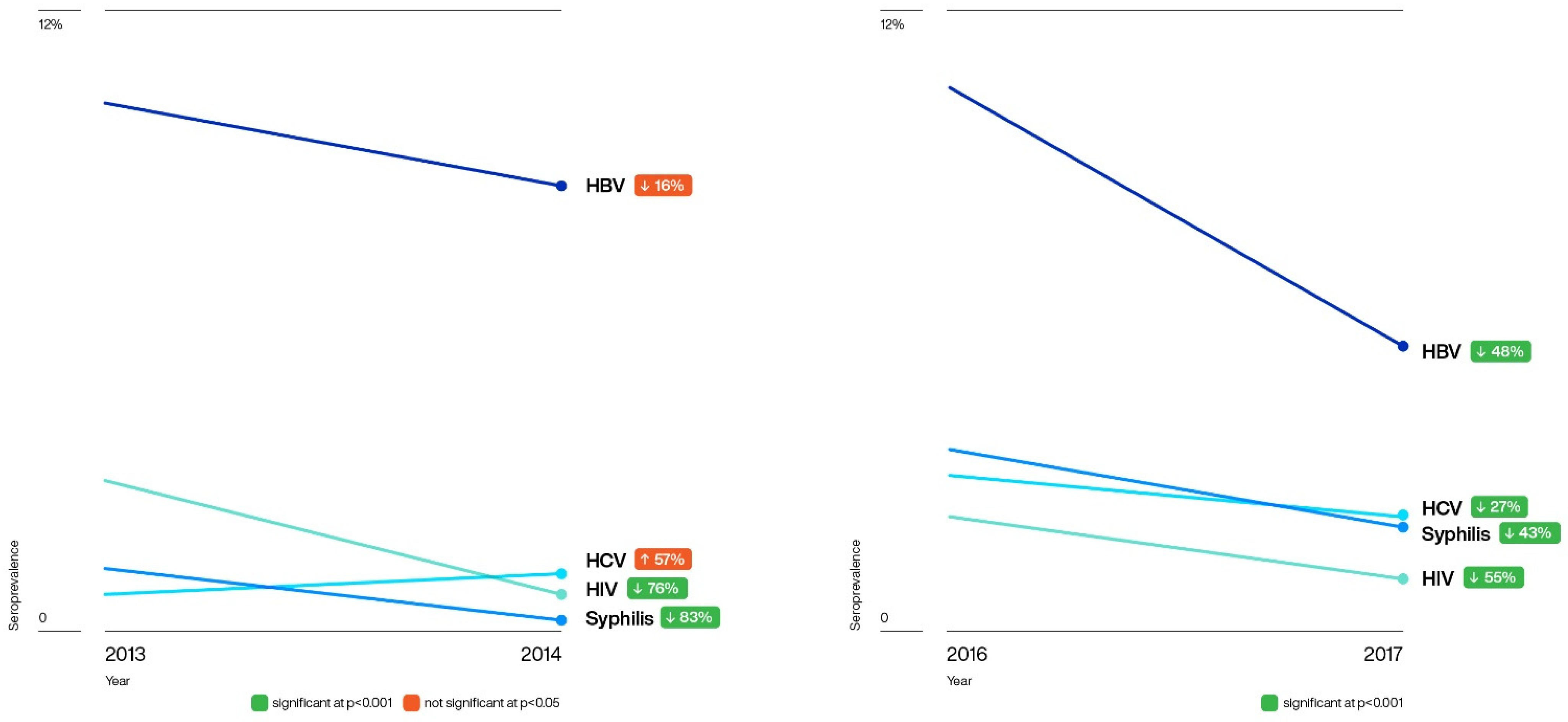
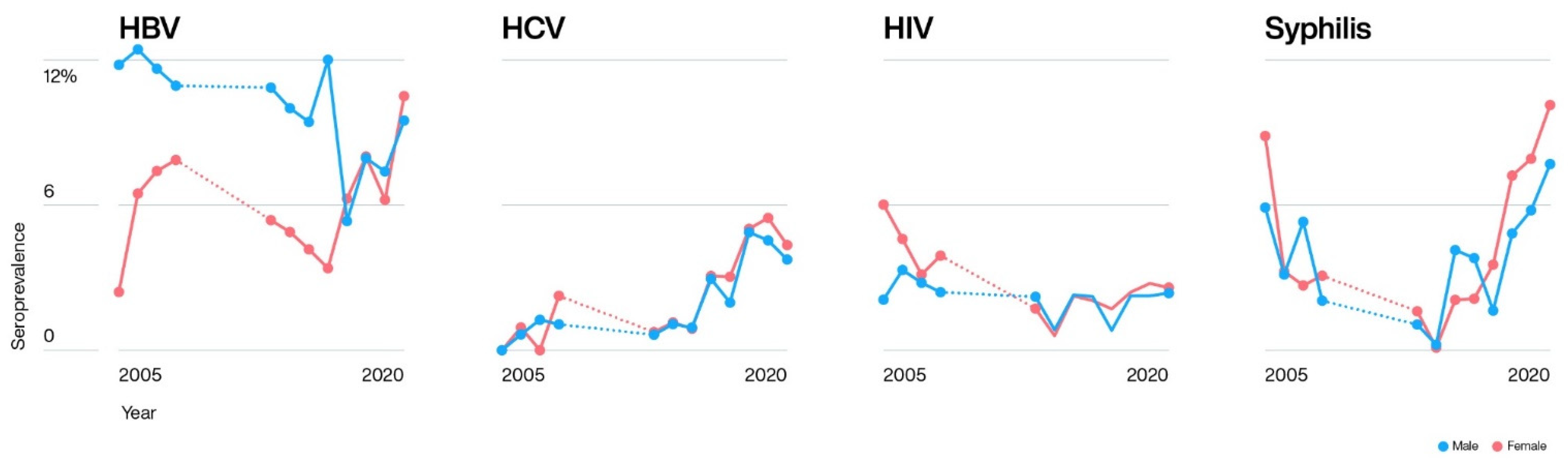
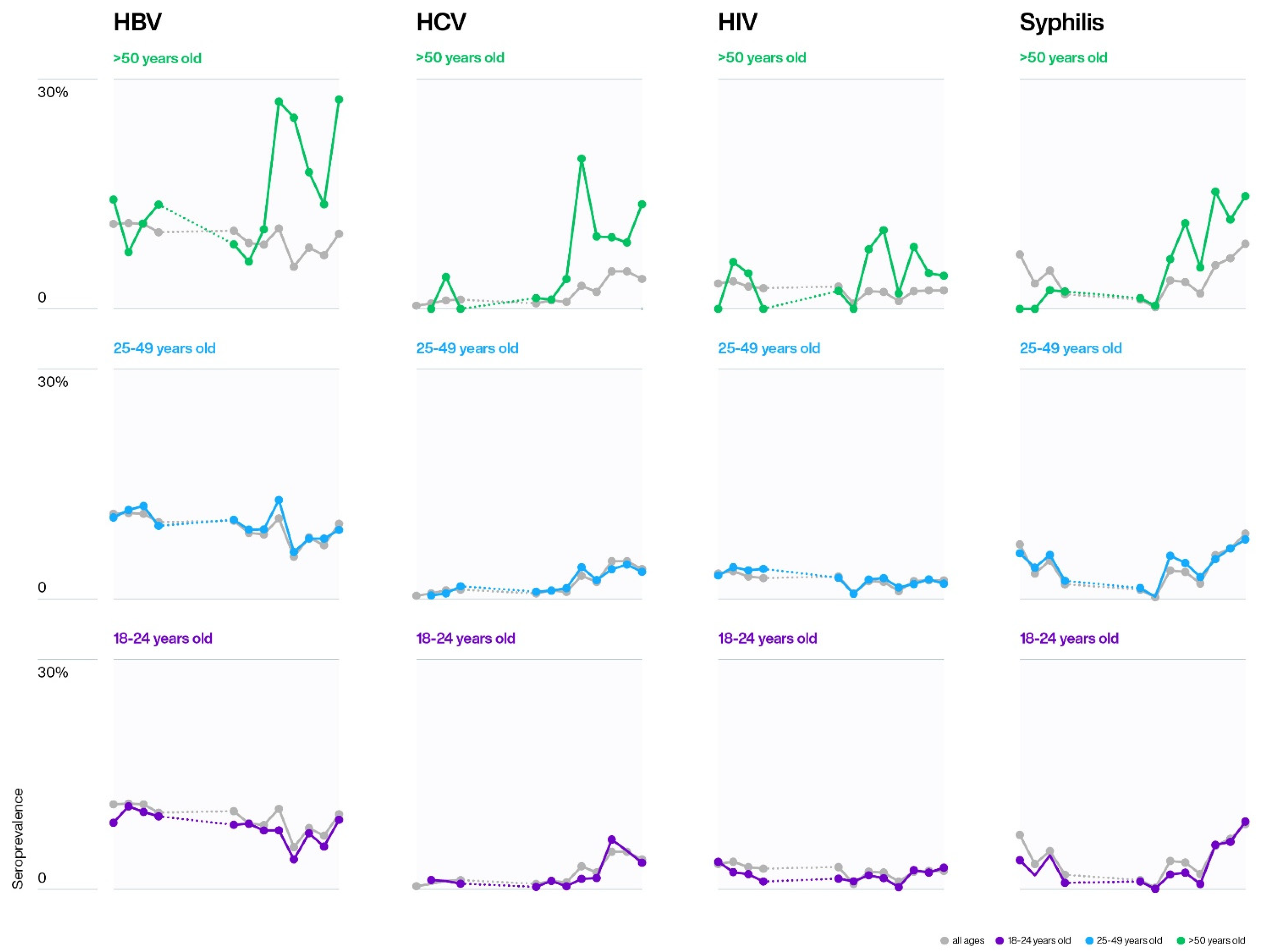
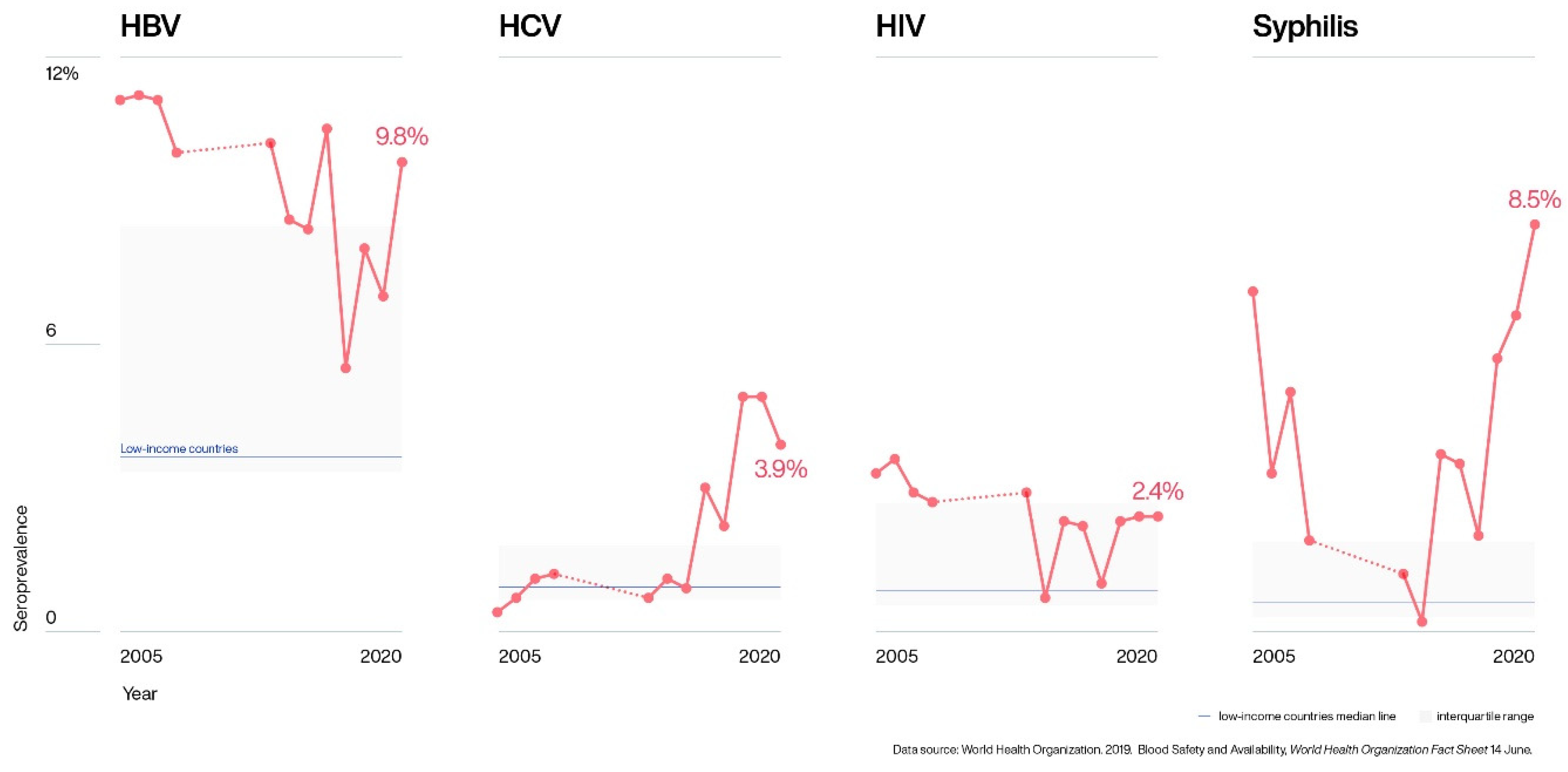
2.2. Trends over Time and Demographic Characteristics
2.3. Blood Donor Specimens
2.3.1. HCV
2.3.2. HBV-OBI
3. Discussion
3.1. Blood Donors
3.2. HBV
3.3. HCV
3.4. HIV
3.5. Syphilis
3.6. TTIs and Demographic Characteristics
3.7. Blood Donor Specimens
3.7.1. HCV: Blood Donor Specimens
3.7.2. HBV: Occult B Infection
4. Materials and Methods
4.1. Study Populations
4.1.1. Blood Donor Data
4.1.2. Blood Specimens
4.2. Serological Marker Detection Using Rapid Diagnostic Tests (RDT) at the HGB
4.3. Serological Markers and Molecular Testing for Hepatitis in Brazil
4.3.1. HCV Testing
4.3.2. Malaria Testing
4.3.3. HBV Testing
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact; Licence: CC BY-NC-SA 3.0 IGO ; World Health Organization: Geneva, Switzerland, 2021; (accessed on 12 October 2021). [Google Scholar]
- UNAIDS 2020. Available online: https://www.unaids.org/en/resources/documents/2020/unaids-data (accessed on 26 September 2021).
- Pruett, C.R.; Vermeulen, M.; Zacharias, P.; Ingram, C.; Tagny, C.T.; Bloch, E.M. The Use of Rapid Diagnostic Tests for Transfusion Infectious Screening in Africa: A Literature Review. Transfus. Med. Rev. 2015, 29, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Roman, L.; Armstrong, B.; Smart, E. Donation testing and transfusion transmissible infections. ISBT Sci. Ser. 2020, 15, 192–206. [Google Scholar] [CrossRef]
- Loua, A.; Nikiema, J.B.; Sougou, A.; Kasilo, O.M.J. Transfusion in the WHO African Region. Transfus. Clin. Et Biol. 2019, 26, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Weimer, A.; Tagny, C.; Tapko, J.; Gouws, C.; Tobian, A.; Ness, P.; Bloch, E. Blood transfusion safety in sub-Saharan Africa: A literature review of changes and challenges in the 21st century. Transfusion 2018, 59, 412–427. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Regional office for África. Blood Safety. Fact Sheet June 2021. Available online: https://www.google.com.br/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwj6tfP7h_XzAhV6HbkGHYwlC7YQFnoECAsQAQ&url=https%3A%2F%2Fwww.afro.who.int%2Fhealth-topics%2Fblood-safety&usg=AOvVaw2Tl-PxO1NB3Az3nG2iZ97s (accessed on 9 September 2021).
- World Health Organization. Global Hepatitis Report 2017; License CC BY-NC-SA 3.0 IGO ; World Health Organization: Geneva, Switzerland, 2017; (accessed on 8 September 2021). [Google Scholar]
- World Health Organization. Report on Global Sexually Transmitted Infection Surveillance, 2018; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/reproductivehealth/publications/stis-surveillance-2018/en/ (accessed on 11 September 2021).
- Dwyer-Lindgren, L.; Cork, M.A.; Sligar, A.; Steuben, K.M.; Wilson, K.F.; Provost, N.R.; Mayala, B.K.; VanderHeide, J.D.; Collison, M.L.; Hall, J.B.; et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature 2019, 570, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Roth, W.K. History and Future of Nucleic Acid Amplification Technology Blood Donor Testing. Transfus. Med. Hemotherapy 2019, 46, 67–75. [Google Scholar] [CrossRef]
- Custer, B.; Agapova, M.; Martinez, R.H. The cost-effectiveness of pathogen reduction technology as assessed using a multiple risk reduction model. Transfusion 2010, 50, 2461–2473. [Google Scholar] [CrossRef]
- Marschner, S.; Dimberg, L.Y. Pathogen Reduction Technologies. In Transfusion Medicine and Hemostasis: Clinical and Laboratory Aspects, 3rd ed.; Beth, H., Shaz, B.H., Hillyer, C.D., Gil, M.R., Eds.; Elsevier Science: Cambridge, MA, USA, 2019; Chapter 48; pp. 289–293. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/book/9780128137260/transfusion-medicine-and-hemostasisISBN 978-0-12-813726-0.
- Bisseye, C.; Mombo, L.-E.; Bie, S.M.M.; Edou, A.; Eko-Mba, J.M.; Etho-Mengue, J.-C.; Mbacky, K.; Mongo-Delis, A.; M’Batchi, B.; Nagalo, B.M. Trends of blood-borne infectious diseases in a rural blood donation center of southeast Gabon (Koula-Moutou). Pan Afr. Med. J. 2018, 31, 81. [Google Scholar] [CrossRef]
- Drammeh, B.; Laperche, S.; Hilton, J.F.; Kaidarova, Z.; Ozeryansky, L.; De, A.; Kalou, M.; Benech, I.; Parekh, B.; Murphy, E.L.; et al. Proficiency Testing of Viral Marker Screening in African Blood Centers—Seven African Countries, 2017. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 947–952. [Google Scholar] [CrossRef] [Green Version]
- Yuen, M.-F.; Chen, D.-S.; Dusheiko, G.M.; Janssen, H.L.A.; Lau, D.T.Y.; Locarnini, S.A.; Peters, M.G.; Lai, C.-L. Hepatitis B virus infection. Nat. Rev. Dis. Prim. 2018, 4, 18035. [Google Scholar] [CrossRef]
- Machado, O. Director of the National Institute of Blood, Luanda, Angola. Personal Communication, 30 August 2021. [Google Scholar]
- Martins, J. National Coordinator of the Malaria Control and Combat Program, Luanda, Angola. Personal Comunication, 4 June 2021. [Google Scholar]
- Dondorp, A.; Nosten, F.; Stepniewska, K.; Day, N.; White, N. South East Asian Quinine Artesunate Malaria Trial (SEAQUAMAT) group Artesunate versus quinine for treatment of severe falciparum malaria: A randomised trial. Lancet 2005, 366, 717–725. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines for the Treatment of Malaria; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/162441 (accessed on 8 September 2021).
- Chicomo, J.A. A resistência de um povo, Editora Nzila, 2008. Available online: https://books.google.com/books/about/Kuito.html?id=HL2icQAACAAJ (accessed on 10 October 2021).
- Kabinda, J.M.; Michèle, D.-W.; Donnen, P.; Miyanga, S.A.; Ende, J.V.D. Factors for viral infection in blood donors of South Kivu in the Democratic Republic of Congo. Pan Afr. Med. J. 2014, 19, 385. [Google Scholar] [CrossRef]
- Nagalo, M.B. Seroprevalence of human immunodeficiency virus, hepatitis B and C viruses and syphilis among blood donors in Koudougou (Burkina Faso) in 2009. Blood Transfus. 2011, 9, 419–424. [Google Scholar] [CrossRef]
- Xie, D.-D.; Li, J.; Chen, J.-T.; Eyi, U.M.; Matesa, R.A.; Obono, M.M.O.; Ehapo, C.S.; Yang, L.-Y.; Yang, H.-T.; Lin, M. Seroprevalence of Human Immunodeficiency Virus, Hepatitis B Virus, Hepatitis C Virus, and Treponema pallidum Infections among Blood Donors on Bioko Island, Equatorial Guinea. PLoS ONE 2015, 10, e0139947. [Google Scholar] [CrossRef] [Green Version]
- Moukoko, C.E.E.; Sack, F.N.; Same, E.G.E.; Mbangue, M.; Lehman, L.G. HIV, HBV, HCV and T. pallidum infections among blood donors and Transfusion-related complications among recipients at the Laquintinie hospital in Douala, Cameroon. BMC Hematol. 2014, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- M’Baya, B. Seroprevalence and trends in transfusion transmissible infections among voluntary non-remunerated blood donors at the Malawi Blood Transfusion Service-a time trend study. Malawi Med. J. 2019, 31, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Yambasu, E.E.; Reid, A.; Owiti, P.; Manzi, M.; Murray, M.J.S.; Edwin, A.K. Hidden dangers-prevalence of blood borne pathogens, hepatitis B, C, HIV and syphilis, among blood donors in Sierra Leone in 2016: Opportunities for improvement: A retrospective, cross-sectional study. Pan Afr. Med. J. 2018, 30, 44. [Google Scholar] [CrossRef]
- Mremi, A.; Yahaya, J.J.; Nyindo, M.; Mollel, E. Transfusion-Transmitted Infections and associated risk factors at the Northern Zone Blood Transfusion Center in Tanzania: A study of blood donors between 2017 and 2019. PLoS ONE 2021, 16, e0249061. [Google Scholar] [CrossRef]
- Jary, A.; Dienta, S.; Leducq, V.; Le Hingrat, Q.; Cisse, M.; Diarra, A.B.; Fofana, D.B.; Ba, A.; Baby, M.; Achenbach, C.J.; et al. Seroprevalence and risk factors for HIV, HCV, HBV and syphilis among blood donors in Mali. BMC Infect. Dis. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Nkrumah, B.; Owusu, M.; Averu, P. Hepatitis B and C viral infections among blood donors. A retrospective study from a rural community of Ghana. BMC Res. Notes 2011, 4, 529. [Google Scholar] [CrossRef] [Green Version]
- Boushab, B.M.; Limame, O.C.M.M.; Zahra, F.-M.F.; Mamoudou, S.; Darnycka, B.M.R.; Saliou, S.M. Estimation of seroprevalence of HIV, hepatitis B and C virus and syphilis among blood donors in the hospital of Aïoun, Mauritania. Pan Afr. Med. J. 2017, 28. [Google Scholar] [CrossRef]
- Okoroiwu, H.U.; Okafor, I.M.; Asemota, E.A.; Okpokam, D.C. Seroprevalence of transfusion-transmissible infections (HBV, HCV, syphilis and HIV) among prospective blood donors in a tertiary health care facility in Calabar, Nigeria; an eleven years evaluation. BMC Public Health 2018, 18, 645. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Blood Safety and Availability, World Health Organization Fact Sheet 14 June 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/blood-safety-and-availability (accessed on 11 February 2020).
- World Health Organization. WHO Guidelines on Hepatitis B and C Testing; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2017; Available online: http://apps.who.int/iris/bitstream/handle/10665/254621/9789241549981-eng.pdf (accessed on 23 July 2021).
- Apata, I.W.; Averhoff, F.; Pitman, J.; Bjork, A.; Yu, J.; Amin, N.A.; Dhingra, N.; Kolwaite, A.; Marfin, A. Centers for Disease Control and Prevention (CDC). Progress toward prevention of transfusion-transmitted hepatitis B and hepatitis C infection—sub-Saharan Africa, 2000–2011. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 613–619. [Google Scholar]
- Abate, M.; Wolde, T. Seroprevalence of Human Immunodeficiency Virus, Hepatitis B Virus, Hepatitis C Virus, and Syphilis among Blood Donors at Jigjiga Blood Bank, Eastern Ethiopia. Ethiop. J. Health Sci. 2016, 26, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirisu, J.O.; Alli, T.O.; Adegoke, A.O.; Osazuwa, F. A Survey of prevalence of serum antibodies to human immunodeficiency deficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV) among blood donors. North Am. J. Med. Sci. 2011, 3, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Mavenyengwa, R.T.; Mukesi, M.; Chipare, I.; Shoombe, E. Prevalence of human immunodeficiency virus, syphilis, hepatitis B and C in blood donations in Namibia. BMC Public Health 2014, 14, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fong, I.W. Blood Transfusion-Associated Infections in the Twenty-First Century: New Challenges. In Current Trends and Concerns in Infectious Diseases. Emerging Infectious Diseases of the 21st Century; Springer: Cham, Switzerland, 2020; Chapter 8; pp. 191–215. [Google Scholar] [CrossRef]
- Abdella, S.; Berheto, T.M.; Tolera, G.; Belete, W.; Deressa, T.; Feleke, A.; H/silassie, A.; Gezahegn, N.; Tadesse, D.; Tefera, M.; et al. Sero-prevalence of transfusion transmittable infections: HIV, Hepatitis B, C and Treponema pallidum and associated factors among blood donors in Ethiopia: A retrospective study. PLoS ONE 2020, 15, e0241086. [Google Scholar] [CrossRef]
- Comunidade dos Países de Lingua Oficial portuguesa. Relatório Final, Angola 2017. Available online: https://www.google.com.br/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwikzq69tPDzAhXFqpUCHak4D3kQFnoECAgQAQ&url=https%3A%2F%2Fsaude.cplp.org%2Fmedia%2F1922%2Fcplp_angola_2018-1.pdf&usg=AOvVaw2jI2VD54_q16l80ccc3Bh (accessed on 4 August 2021).
- World Health Organization. WHO Guidelines for the Treatment of Treponema Pallidum (Syphilis); World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int›rtis›syphilis (accessed on 11 September 2021).
- Abebe, M.; Marga, N. Human Immunodeficiency Virus and Syphilis Among Blood Donors at Western Oromia, Ethiopia. J. Blood Med. 2021, ume 12, 671–677. [Google Scholar] [CrossRef]
- Vermeulen, M.; Swanevelder, R.; Chowdhury, D.; Ingram, C.; Reddy, R.; Bloch, E.M.; Custer, B.S.; Murphy, E.L. For the NHLBI Recipient Epidemiology and Donor evaluation Study-III (REDS-III) International Component Use of Blood Donor Screening to Monitor Prevalence of HIV and Hepatitis B and C Viruses, South Africa. Emerg. Infect. Dis. 2017, 23, 1560–1563. [Google Scholar] [CrossRef] [Green Version]
- Sherlock, S. Hepatitis B: The disease. Vaccine 1990, 8, S6–S9. [Google Scholar] [CrossRef]
- Li, Z.; Hou, X.; Cao, G. Is mother-to-infant transmission the most important factor for persistent HBV infection? Emerg. Microbes Infect. 2015, 4, e30. [Google Scholar] [CrossRef]
- Siraj, N.; Achila, O.O.; Issac, J.; Menghisteab, E.; Hailemariam, M.; Hagos, S.; Gebremeskel, Y.; Tesfamichael, D. Seroprevalence of transfusion-transmissible infections among blood donors at National Blood Transfusion Service, Eritrea: A seven-year retrospective study. BMC Infect. Dis. 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Onyango, C.G.; Ogonda, L.; Guyah, B.; Okoth, P.; Shiluli, C.; Humwa, F.; Opollo, V. Seroprevalence and determinants of transfusion transmissible infections among voluntary blood donors in Homabay, Kisumu and Siaya counties in western Kenya. BMC Res. Notes 2018, 11, 171. [Google Scholar] [CrossRef]
- World Health Organization. Training Modules on Hepatitis B and C Screening, Diagnosis and Treatment; Licence: CC BY-NC-SA 3.0 IGO ; World Health Organization: Geneva, Switzerland, 2020; (accessed on 20 August 2021). [Google Scholar]
- Mullis, C.E.; Laeyendecker, O.; Reynolds, S.; Ocama, P.; Quinn, J.; Boaz, I.; Gray, R.H.; Kirk, G.D.; Thomas, D.L.; Quinn, T.C.; et al. High Frequency of False-Positive Hepatitis C Virus Enzyme-Linked Immunosorbent Assay in Rakai, Uganda. Clin. Infect. Dis. 2013, 57, 1747–1750. [Google Scholar] [CrossRef] [Green Version]
- Oluyinka, O.O.; Tong, H.; Tien, S.B.; Fagbami, A.H.; Adekanle, O.; Ojurongbe, O.; Bock, C.-T.; Kremsner, P.G.; Velavan, T.P. Occult Hepatitis B Virus Infection in Nigerian Blood Donors and Hepatitis B Virus Transmission Risks. PLoS ONE 2015, 10, e0131912. [Google Scholar] [CrossRef]
- Mahmoud, O.A.E.K.; Ghazal, A.A.E.R.; Metwally, D.E.S.; Elnour, A.M.; Yousif, G.E.A. Detection of occult hepatitis B virus infection among blood donors in Sudan. J. Egypt. Public Health Assoc. 2013, 88, 14–18. [Google Scholar] [CrossRef]
- Busch, M.P.; Bloch, E.M.; Kleinman, S.H. Prevention of transfusion-transmitted infections. Blood 2019, 133, 1854–1864. [Google Scholar] [CrossRef] [Green Version]
- Velati, C.; Romanò, L.; Piccinini, V.; Marano, G.; Catalano, L.; Pupella, S.; Facco, G.; Pati, I.; Tosti, M.E.; Vaglio, S.; et al. Prevalence, incidence and residual risk of transfusion-transmitted hepatitis C virus and human immunodeficiency virus after the implementation of nucleic acid testing in Italy: A 7-year (2009–2015) survey. Blood Transfus. Trasfus. Del Sangue 2018, 16, 1–12. [Google Scholar] [CrossRef]
- Cicchetti, A.; Berrino, A.; Casini, M.; Codella, P.; Coretti, S.; Facco, G.; Fiore, A.; Marano, G.; Marchetti, M.; Midolo, E.; et al. Health Technology Assessment of pathogen reduction technologies applied to plasma for clinical use. Blood Transfus. 2016, 14, 287–386. [Google Scholar] [CrossRef]
- El Dusouqui, S.A.; Lanteri, M.C.; Schwabe, R.; Grzesiczek, A.; North, A.; Mufti, N.; Sekongo, Y.M.; Pitman, J.; Tagny, C.T. Progress towards an appropriate pathogen reduction technology for whole blood in Africa. ISBT Sci. Ser. 2019, 15, 151–163. [Google Scholar] [CrossRef]
- Grobbelaar, A.A.; Weyer, J.; Moolla, N.; Van Vuren, P.J.; Moises, F.; Paweska, J.T. Resurgence of Yellow Fever in Angola, 2015–2016. Emerg. Infect. Dis. 2016, 22, 1854–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Blood Donors a (%) | Age Groups b | Gender c | Number of Blood Donors Tested d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18–24 (%) | 25–49 (%) | >50 (%) | Unknown | Male (%) | Female (%) | Unknown | HBsAg (%) | Anti-HCV (%) | Anti-HIV (%) | Anti-Treponema (%) | ||
| 2005 | 1430 (2.5) | 115 (34.8) | 208 (63.0) | 7 (2.1) | 1100 | 306 (78.7) | 83 (21.3) | 1041 | 1429 (99.9) | 1135 (79.4) | 1371 (95.8) | 1232 (86.2) |
| 2006 | 1792 (3.1) | 647 (36.8) | 1058 (60.1) | 54 (3.1) | 33 | 1417 (79.8) | 359 (20.2) | 16 | 1780 (99.3) | 1554 (86.7) | 1737 (96.9) | 1630 (91) |
| 2007 | 1500 (2.6) | 616 (44) | 747 (53) | 44 (3.1) | 93 | 1254 (88.6) | 162 (11.4) | 84 | 1490 (99.3) | 848 (56.5) | 1463 (97.5) | 1372 (91.5) |
| 2008 | 1508 (2.6) | 601 (42.4) | 772 (54.5) | 44 (3.1) | 91 | 1138 (89.7) | 130 (10.3) | 240 | 1498 (99.3) | 1054 (69.9) | 1487 (98.6) | 1486 (98.5) |
| 2013 | 3476 (6) | 1670 (48) | 1581 (45.5) | 225 (6.5) | 0 | 2490 (71.6) | 986 (28.4) | 0 | 3307 (95.13) | 3279 (94.33) | 3278 (94.30) | 3279 (94.33) |
| 2014 | 3869 (6.6) | 1622 (43.5) | 1847 (49.5) | 259 (7) | 141 | 2726 (73.1) | 1002 (26.9) | 141 | 3750 (96.9) | 3679 (95) | 3869 (100) | 3652 (94.4) |
| 2015 | 3420 (5.9) | 1790 (52.3) | 1551 (45.3) | 79 (2.3) | 0 | 2730 (79.8) | 690 (20.2) | 0 | 3331 (97.4) | 3331 (97.4) | 3330 (97.36) | 3331(97.4) |
| 2016 | 7751 (13.4) | 3926 (50.6) | 3709 (47.8) | 116 (1.5) | 0 | 6379 (82.3) | 1372 (17.7) | 0 | 7171 (92.5) | 7169 (92.4) | 7171 (92.5) | 7171 (92.5) |
| 2017 | 8544 (14.7) | 3585 (41.9) | 4811 (56.3) | 148 (1.7) | 0 | 6964 (81.5) | 1580 (18.5) | 0 | 8544 (100) | 8544 (100) | 8544 (100) | 8544 (100) |
| 2018 | 8436 (14.6) | 2904 (34.4) | 5297 (62.8) | 235 (2.8) | 0 | 5388 (63.9) | 3048 (36.1) | 0 | 8436 (100) | 8436 (100) | 8436 (100) | 8436 (100) |
| 2019 | 9640 (16.6) | 4568 (47.4) | 4772 (49.5) | 300 (3.1) | 0 | 6168 (64) | 3472 (36) | 0 | 9640 (100) | 9640 (100) | 9640 (100) | 9640 (100) |
| 2020 | 6613 (11.4) | 2641 (39.9) | 3687 (55.8) | 285 (4.3) | 0 | 4454 (67.4) | 2159 (32.6) | 0 | 6613 (100) | 6613 (100) | 6613 (100) | 6613 (100) |
| Total | 57,979 (100) | 24,685 (43.7) | 30,040 (53.1) | 1796 (3.2) | 1459 | 41,414 (73.4) | 15,043 (26.6) | 1523 | 56,961 (98.2) | 55,282 (95.3) | 56,939 (98.2) | 56,386 (97.2) |
| HBV+ | HCV+ | HIV+ | Syphilis+ | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | Total | n | % | CI | Total | n | % | CI | Total | n | % | CI | Total | n | % | CI |
| 2005 | 1429 | 159 | 11.1 | 9.5–12.8 | 1135 | 4 | 0.4 | 0.1–0.8 | 1370 | 45 | 3.3 | 2.4–4.3 | 1232 | 88 | 7.1 | 5.7–8.7 |
| 2006 | 1780 | 200 | 11.2 | 9.8–12.7 | 1554 | 11 | 0.7 | 0.3–1.2 | 1712 | 61 | 3.6 | 2.7–4.5 | 1630 | 54 | 3.3 | 2.4–4.3 |
| 2007 | 1490 | 166 | 11.1 | 9.5–12.8 | 848 | 9 | 1.1 | 0.4–2.0 | 1458 | 42 | 2.9 | 2.0–3.8 | 1372 | 69 | 5 | 3.9–6.3 |
| 2008 | 1498 | 150 | 10 | 8.5–11.6 | 1054 | 13 | 1.2 | 0.6–2.0 | 1489 | 40 | 2.7 | 1.9–3.6 | 1486 | 28 | 1.9 | 1.2–2.7 |
| 2013 | 3279 | 305 | 9.3 | 8.3–10.4 | 3279 | 22 | 0.7 | 0.4–1.0 | 3278 | 68 | 2.1 | 1.6–2.6 | 3279 | 40 | 1.2 | 0.8–1.6 |
| 2014 | 3750 | 322 | 8.6 | 7.7–9.5 | 3679 | 39 | 1.1 | 0.7–1.4 | 3869 | 29 | 0.7 | 0.5–1.0 | 3652 | 7 | 0.2 | 0.1–0.3 |
| 2015 | 3331 | 279 | 8.4 | 7.4–9.3 | 3331 | 31 | 0.9 | 0.6–1.3 | 3330 | 76 | 2.3 | 1.8–2.8 | 3331 | 124 | 3.7 | 3.1–4.4 |
| 2016 | 7171 | 752 | 10.5 | 9.7–11.2 | 7169 | 215 | 3 | 2.6–3.4 | 7171 | 157 | 2.2 | 1.8–2.5 | 7171 | 252 | 3.5 | 3.0–3.9 |
| 2017 | 8544 | 471 | 5.5 | 5.0–6.0 | 8544 | 185 | 2.2 | 1.8–2.4 | 8544 | 84 | 1.0 | 0.8–1.2 | 8544 | 170 | 2 | 1.7–2.3 |
| 2018 | 8436 | 672 | 8 | 7.5–8.7 | 8436 | 416 | 4.9 | 4.4–5.4 | 8436 | 194 | 2.3 | 2.0–2.7 | 8436 | 480 | 5.7 | 5.3–6.3 |
| 2019 | 9640 | 672 | 7 | 6.4–7.4 | 9640 | 470 | 4.9 | 4.4–5.3 | 9640 | 235 | 2.4 | 2.1–2.7 | 9640 | 632 | 6.6 | 6.0–7.0 |
| 2020 | 6613 | 650 | 9.8 | 9.1–10.5 | 6613 | 261 | 3.9 | 3.4–4.4 | 6613 | 161 | 2.4 | 2.0–2.8 | 6613 | 562 | 8.5 | 7.8–9.1 |
| Total | 56,961 | 4798 | 8.4 | 8.2–8.7 | 55,282 | 1676 | 3 | 2.8–3.1 | 56,910 | 1219 | 2.1 | 2.0–2.2 | 56,386 | 2506 | 4.4 | 4.2–4.6 |
| Demographics | Number | HBV | HCV | HIV | Syphilis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | n | % | OR 95% CI | Total | n | % | OR 95% CI | Total | n | % | OR 95% CI | Total | n | % | OR 95% CI | ||
| Age | |||||||||||||||||
| 18–24 | 24,684 | 24,242 | 1734 | 7.2 | 1 | 23,631 | 657 | 2.8 | 1 | 24,194 | 418 | 1.7 | 1 | 24,034 | 886 | 3.7 | 1 |
| 25–49 | 30,040 | 29,615 | 2626 | 8.9 | 1.26 (1.18–1.34) | 28,796 | 881 | 3.1 | 1.10 (0.99–1.22) a | 29,547 | 656 | 2.2 | 1.29 (1.14–1.46) | 29,331 | 1391 | 4.7 | 1.30 (1.19–1.42) |
| >50 | 1796 | 1773 | 285 | 16.1 | 2.48 (2.17–2.85) | 1725 | 132 | 7.7 | 2.89 (2.39–3.52) | 1765 | 76 | 4.3 | 2.56 (1.99–3.28) | 1746 | 144 | 8.3 | 2.35 (1.96–2.82) |
| Gender | |||||||||||||||||
| Male | 41,414 | 40,709 | 3648 | 9.0 | 1.35 (1.26–1.46) | 39,399 | 1114 | 2.8 | 0.73 (0.67–0.82) | 40,592 | 801 | 2.0 | 0.84 (0.74–0.96) | 40,276 | 1580 | 3.9 | 0.66 (0.61–0.73) |
| Female | 15,043 | 14,859 | 1003 | 6.8 | 1 | 14,646 | 555 | 3.8 | 1 | 14,850 | 346 | 2.3 | 1 | 14,772 | 853 | 5.8 | 1 |
| Gender/Age | |||||||||||||||||
| Male | |||||||||||||||||
| 18–24 | 18,376 | 18,011 | 1369 | 7.6 | 1 | 17,492 | 457 | 2.6 | 1 | 17,967 | 299 | 1.7 | 1 | 17,841 | 547 | 3.1 | 1 |
| 25–49 | 21,709 | 21,385 | 2040 | 9.5 | 1.28 (1.19–1.38) | 20,715 | 567 | 2.7 | 1.04 (0.93–1.19) a | 21,322 | 450 | 2.1 | 1.27 (1.10–1.48) | 21,150 | 932 | 4.4 | 1.46 (1.31–1.62) |
| >50 | 1124 | 1111 | 211 | 19.0 | 2.85 (2.43–3.34) | 1069 | 88 | 8.2 | 3.34 (2.64–4.21) | 1103 | 45 | 4.1 | 2.51 (1.83–3.46) | 1089 | 90 | 8.3 | 2.84 (2.26–3.59) |
| Female | |||||||||||||||||
| 18–24 | 6179 | 6102 | 358 | 5.9 | 1 | 6029 | 200 | 3.3 | 1 | 6099 | 118 | 1.9 | 1 | 6066 | 338 | 5.6 | 1 |
| 25–49 | 8170 | 8073 | 571 | 7.1 | 1.22 (1.07–1.40) | 7950 | 311 | 3.9 | 1.18 (0.99–1.42) a | 8067 | 196 | 2.4 | 1.26 (1.0–1.59) | 8028 | 456 | 5.7 | 1.02 (0.88–1.18) a |
| >50 | 662 | 652 | 73 | 11.2 | 2.02 (1.55–2.64) | 646 | 44 | 6.8 | 2.13 (1.52–2.98) | 652 | 31 | 4.8 | 2.53 (1.69–3.79) | 647 | 54 | 8.4 | 1.54 (1.14–2.08) |
| Number | ID | 1st RDT | 2nd RDT | qHBsAg | qHBsAg | Anti-HBc | Anti-HBc | HBV DNA |
|---|---|---|---|---|---|---|---|---|
| Determine® | Vikia® | Liason® | IU/mL | IgG | IgM | IU/mL | ||
| 1 | 241 | n | n | n | 0.036 | n | n | 272 |
| 2 | 249 | n | n | n | <0.030 | n | - | 18 |
| 3 | 284 | n | n | n | <0.030 | n | n | <10 |
| 4 | 349 | n | n | n | <0.030 | p | - | 13 |
| 5 | 389 | n | n | n | <0.030 | p | - | 38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peliganga, L.B.; Mello, V.M.; de Sousa, P.S.F.; Horta, M.A.P.; Soares, Á.D.; Nunes, J.P.d.S.; Nobrega, M.; Lewis-Ximenez, L.L. Transfusion Transmissible Infections in Blood Donors in the Province of Bié, Angola, during a 15-Year Follow-Up, Imply the Need for Pathogen Reduction Technologies. Pathogens 2021, 10, 1633. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10121633
Peliganga LB, Mello VM, de Sousa PSF, Horta MAP, Soares ÁD, Nunes JPdS, Nobrega M, Lewis-Ximenez LL. Transfusion Transmissible Infections in Blood Donors in the Province of Bié, Angola, during a 15-Year Follow-Up, Imply the Need for Pathogen Reduction Technologies. Pathogens. 2021; 10(12):1633. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10121633
Chicago/Turabian StylePeliganga, Luis Baião, Vinicius Motta Mello, Paulo Sergio Fonseca de Sousa, Marco Aurelio Pereira Horta, Álvaro Domingos Soares, João Pedro da Silva Nunes, Miguel Nobrega, and Lia Laura Lewis-Ximenez. 2021. "Transfusion Transmissible Infections in Blood Donors in the Province of Bié, Angola, during a 15-Year Follow-Up, Imply the Need for Pathogen Reduction Technologies" Pathogens 10, no. 12: 1633. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10121633