
Intestinal Fatty Acid Binding Protein (I-FABP) as a Prognostic Marker in Critically Ill COVID-19 Patients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection
2.3. Biomarker Analysis
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Acute Gastointestinal Injury Score and Feeding Intolerance
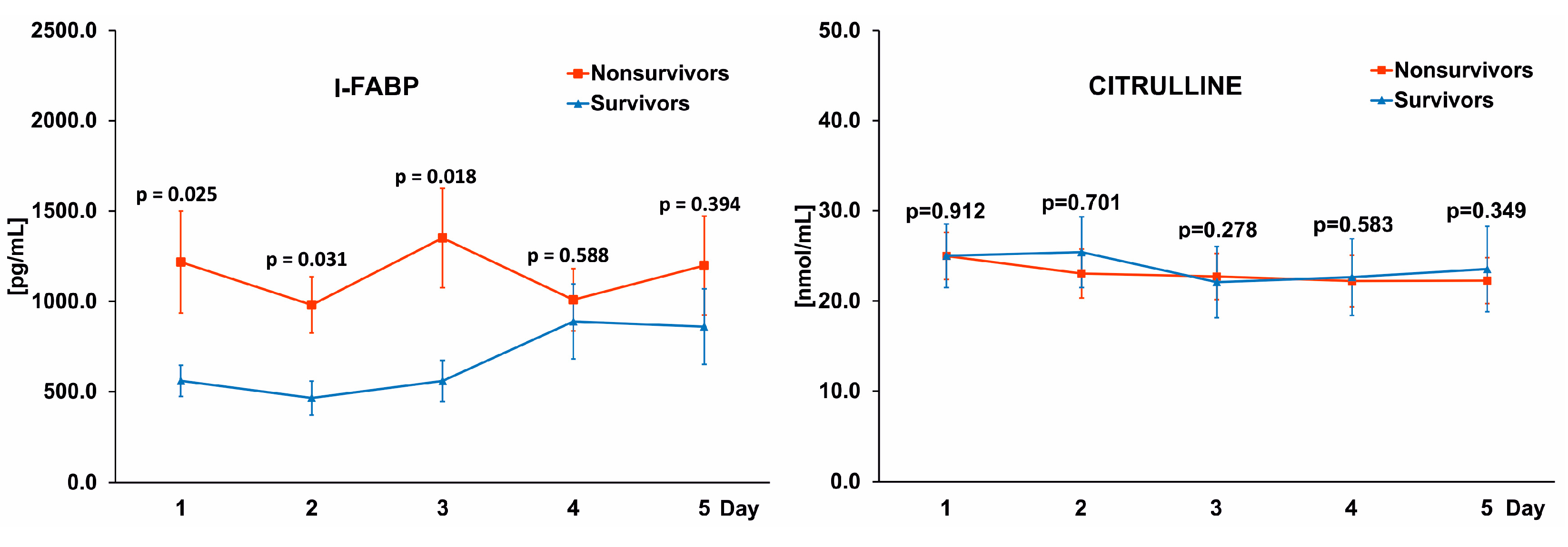
3.3. Differences in I-FABPand Citrulline Levels between Survivors and Nonsurvivors
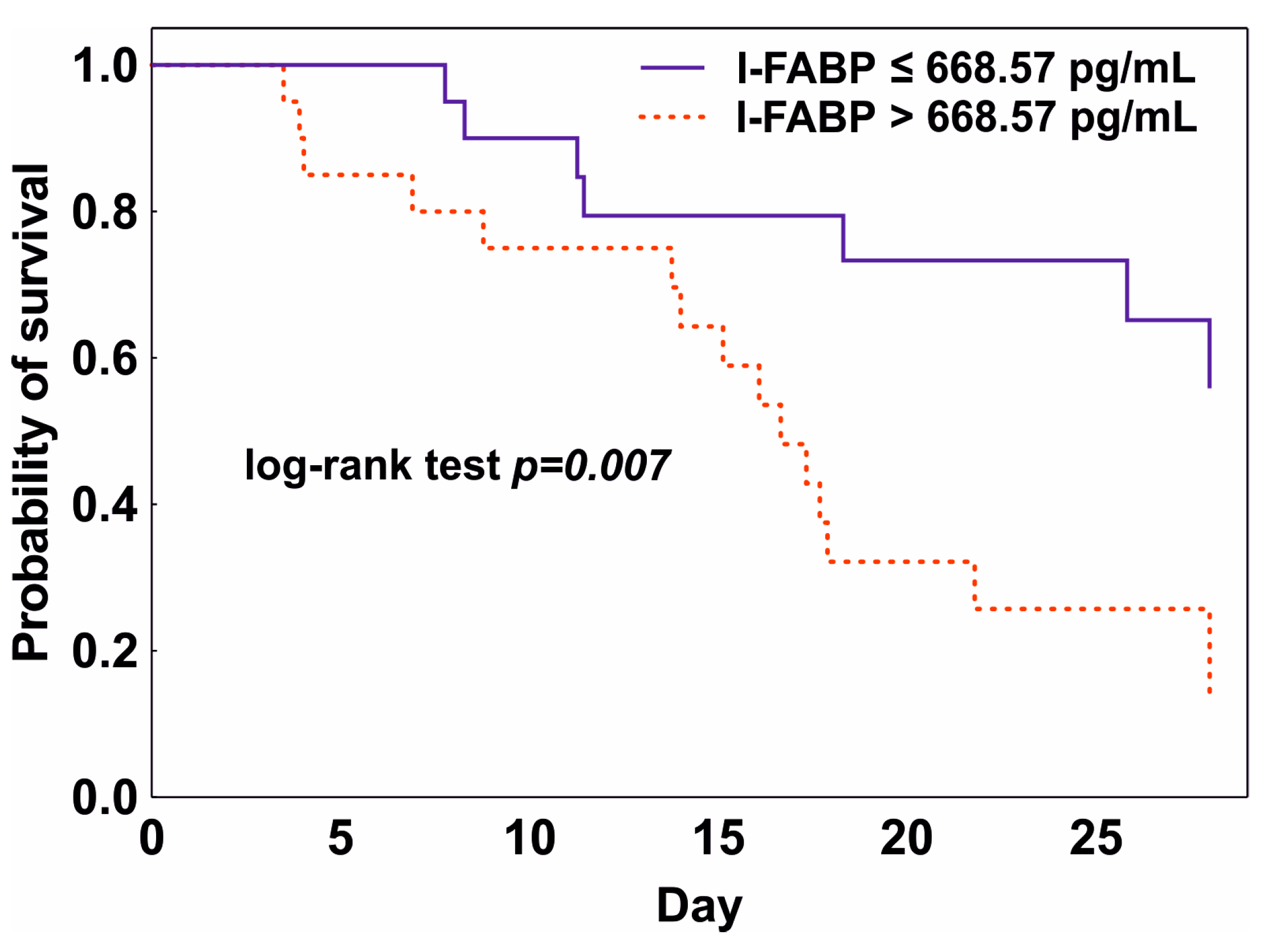
3.4. Prediction of Mortality
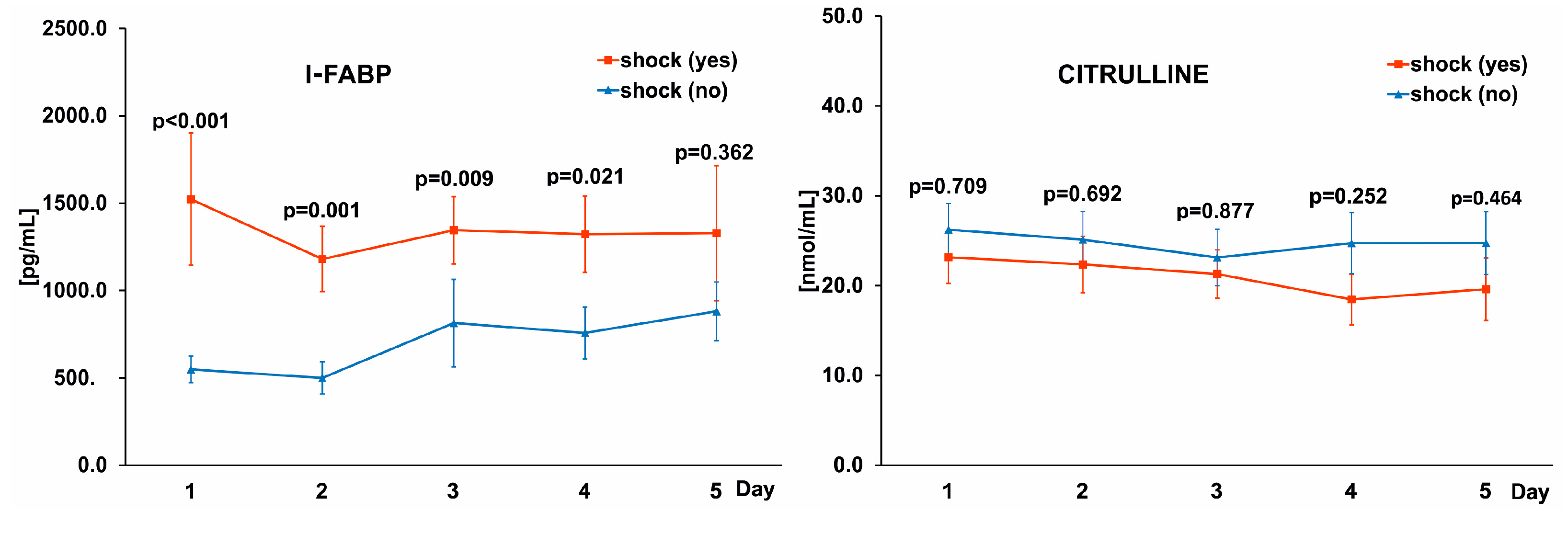
3.5. Differences in I-FABP Levels between Patients with Sepsis and Shock
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acosta, M.A.T.; Singer, B.D. Pathogenesis of COVID-19-induced ARDS: Implications for an ageing population. Eur. Respir. J. 2020, 56, 2002049. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA-J. Am. Med. Assoc. 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Improving the Prevention, Diagnosis and Clinical Management of Sepsis. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA70/A70_13-en.pdf (accessed on 24 November 2022).
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Ñamendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.-N.; Vincent, J.-L. Sepsis in Intensive Care Unit Patients: Worldwide Data from the ICON Audit. Open Forum Infect. Dis. 2018, 5, ofy313. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.-L.; McGinley, J.P.; Drysdale, S.B.; Pollard, A.J. Epidemiology and Immune Pathogenesis of Viral Sepsis. Front. Immunol. 2018, 9, 2147. [Google Scholar] [CrossRef] [PubMed]
- Smiechowicz, J.; Barteczko-Grajek, B.; Adamik, B.; Bojko, J.; Gozdzik, W.; Lipinska-Gediga, M. Influenza in patients with respiratory failure admitted to intensive care units in Poland and the use of extracorporeal respiratory support: A survey-based multicenter study. BMC Infect. Dis. 2021, 21, 954. [Google Scholar] [CrossRef] [PubMed]
- Karakike, E.; Giamarellos-Bourboulis, E.J.; Kyprianou, M.; Fleischmann-Struzek, C.; Pletz, M.W.; Netea, M.G.; Reinhart, K.; Kyriazopoulou, E. Coronavirus Disease 2019 as Cause of Viral Sepsis. Crit. Care Med. 2021, 49, 2042–2057. [Google Scholar] [CrossRef]
- Tarragon, B.; Valdenebro, M.; Serrano, M.L.; Maroto, A.; Llopez-Carratala, M.R.; Ramos, A.; Rubio, E.; Huerta, A.; Marques, M.; Portoles, J. Acute kidney failure in patients admitted due to COVID-19. Nefrologia 2021, 41, 34–40. [Google Scholar] [CrossRef]
- Italia, L.; Tomasoni, D.; Bisegna, S.; Pancaldi, E.; Stretti, L.; Adamo, M.; Metra, M. COVID-19 and Heart Failure: From Epidemiology during the Pandemic to Myocardial Injury, Myocarditis, and Heart Failure Sequelae. Front. Cardiovasc. Med. 2021, 8, 713560. [Google Scholar] [CrossRef]
- de Roquetaillade, C.; Bredin, S.; Lascarrou, J.-B.; Soumagne, T.; Cojocaru, M.; Chousterman, B.G.; Leclerc, M.; Gouhier, A.; Piton, G.; Pène, F.; et al. Timing and causes of death in severe COVID-19 patients. Crit. Care 2021, 25, 224. [Google Scholar] [CrossRef]
- Spearman, C.W.; Aghemo, A.; Valenti, L.; Sonderup, M.W. COVID-19 and the liver: A 2021 update. Liver Int. 2021, 41, 1988–1998. [Google Scholar] [CrossRef]
- Dumas, A.; Bernard, L.; Poquet, Y.; Lugo-Villarino, G.; Neyrolles, O. The role of the lung microbiota and the gut-lung axis in respiratory infectious diseases. Cell. Microbiol. 2018, 20, e12966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickson, R.P.; Singer, B.; Newstead, M.W.; Falkowski, N.R.; Erb-Downward, J.R.; Standiford, T.J.; Huffnagle, G.B. Enrichment of the lung microbiome with gut bacteria in sepsis and the acute respiratory distress syndrome. Nat. Microbiol. 2016, 1, 16113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaliszewski, K.; Diakowska, D.; Nowak, Ł.; Tokarczyk, U.; Sroczyński, M.; Sępek, M.; Dudek, A.; Sutkowska-Stępień, K.; Kiliś-Pstrusińska, K.; Matera-Witkiewicz, A.; et al. Assessment of Gastrointestinal Symptoms and Dyspnea in Patients Hospitalized due to COVID-19: Contribution to Clinical Course and Mortality. J. Clin. Med. 2022, 11, 1821. [Google Scholar] [CrossRef]
- Kang, M.K.; Kim, K.O.; Kim, M.C.; Cho, J.H.; Kim, S.B.; Gil Park, J.; Kim, K.H.; Lee, S.H.; Jang, B.I.; Kim, T.N. Clinical characteristics of coronavirus disease 2019 patients with diarrhea in Daegu. Korean J. Intern. Med. 2020, 35, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Paz, M.; Siraj, L.; Boyd, T.; Salamone, S.; Lite, T.-L.V.; Leung, K.M.; Chirinos, J.D.; Shang, H.H.; Townsend, M.J.; et al. Feeding Intolerance in Critically Ill Patients with COVID-19. Clin. Nutr. 2022, 41, 3069–3076. [Google Scholar] [CrossRef]
- Lamers, M.M.; Beumer, J.; van der Vaart, J.; Knoops, K.; Puschhof, J.; Breugem, T.I.; Ravelli, R.B.G.; van Schayck, J.P.; Mykytyn, A.Z.; Duimel, H.Q.; et al. SARS-CoV-2 productively infects human gut enterocytes. Science 2020, 369, 50–54. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Harmer, D.; Gilbert, M.; Borman, R.; Clark, K.L. Quantitative mRNA expression profiling of ACE 2, a novel homologue of angiotensin converting enzyme. FEBS Lett. 2002, 532, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Blaser, A.R.; Preiser, J.-C.; Fruhwald, S.; Wilmer, A.; Wernerman, J.; Benstoem, C.; Casaer, M.P.; Starkopf, J.; van Zanten, A.; Rooyackers, O.; et al. Gastrointestinal dysfunction in the critically ill: A systematic scoping review and research agenda proposed by the Section of Metabolism, Endocrinology and Nutrition of the European Society of Intensive Care Medicine. Crit. Care 2020, 24, 224. [Google Scholar] [CrossRef] [PubMed]
- Blaser, A.R.; Padar, M.; Mändul, M.; Elke, G.; Engel, C.; Fischer, K.; Giabicani, M.; Gold, T.; Hess, B.; Hiesmayr, M.; et al. Development of the Gastrointestinal Dysfunction Score (GIDS) for critically ill patients—A prospective multicenter observational study (iSOFA study). Clin. Nutr. 2021, 40, 4932–4940. [Google Scholar] [CrossRef] [PubMed]
- Blaser, A.R.; Malbrain, M.L.N.G.; Starkopf, J.; Fruhwald, S.; Jakob, S.M.; De Waele, J.; Braun, J.-P.; Poeze, M.; Spies, C. Gastrointestinal function in intensive care patients: Terminology, definitions and management. Recommendations of the ESICM Working Group on Abdominal Problems. Intensiv. Care Med. 2012, 38, 384–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelsers, M.M.; Hermens, W.T.; Glatz, J.F. Fatty acid-binding proteins as plasma markers of tissue injury. Clin. Chim. Acta 2005, 352, 15–35. [Google Scholar] [CrossRef] [PubMed]
- Voth, M.; Duchene, M.; Auner, B.; Lustenberger, T.; Relja, B.; Marzi, I. I-FABP is a Novel Marker for the Detection of Intestinal Injury in Severely Injured Trauma Patients. World J. Surg. 2017, 41, 3120–3127. [Google Scholar] [CrossRef]
- Sun, D.-L.; Cen, Y.-Y.; Li, S.-M.; Li, W.-M.; Lu, Q.-P.; Xu, P.-Y. Accuracy of the serum intestinal fatty-acid-binding protein for diagnosis of acute intestinal ischemia: A meta-analysis. Sci. Rep. 2016, 6, srep34371. [Google Scholar] [CrossRef] [Green Version]
- Coufal, S.; Kokesova, A.; Tlaskalova-Hogenova, H.; Frybova, B.; Snajdauf, J.; Rygl, M.; Kverka, M. Urinary I-FABP, L-FABP, TFF-3, and SAA Can Diagnose and Predict the Disease Course in Necrotizing Enterocolitis at the Early Stage of Disease. J. Immunol. Res. 2020, 2020, 3074313. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.H.W.; Li, D.Y.; Hazen, S.L. Dietary metabolism, the gut microbiome, and heart failure. Nat. Rev. Cardiol. 2019, 16, 137–154. [Google Scholar] [CrossRef]
- Kitai, T.; Kim, Y.-H.; Kiefer, K.; Morales, R.; Borowski, A.G.; Grodin, J.L.; Tang, W.W. Circulating intestinal fatty acid-binding protein (I-FABP) levels in acute decompensated heart failure. Clin. Biochem. 2017, 50, 491–495. [Google Scholar] [CrossRef]
- Adamik, B.; Kübler, A.; Gozdzik, A.; Gozdzik, W. Prolonged Cardiopulmonary Bypass is a Risk Factor for Intestinal Ischaemic Damage and Endotoxaemia. Heart Lung Circ. 2017, 26, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Windmueller, H.G.; Spaeth, A.E. Source and fate of circulating citrulline. Am. J. Physiol. Metab. 1981, 241, E473–E480. [Google Scholar] [CrossRef] [PubMed]
- Dossin, O.; Rupassara, S.; Weng, H.-Y.; Williams, D.; Garlick, P.; Schoeman, J. Effect of Parvoviral Enteritis on Plasma Citrulline Concentration in Dogs. J. Vet. Intern. Med. 2011, 25, 215–221. [Google Scholar] [CrossRef]
- Herbers, A.H.; Feuth, T.; Donnelly, J.P.; Blijlevens, N.M. Citrulline-based assessment score: First choice for measuring and monitoring intestinal failure after high-dose chemotherapy. Ann. Oncol. 2010, 21, 1706–1711. [Google Scholar] [CrossRef]
- Shen, L.-J.; Guan, Y.-Y.; Wu, X.-P.; Wang, Q.; Wang, L.; Xiao, T.; Wu, H.-R.; Wang, J.-G. Serum citrulline as a diagnostic marker of sepsis-induced intestinal dysfunction. Clin. Res. Hepatol. Gastroenterol. 2015, 39, 230–236. [Google Scholar] [CrossRef]
- Giron, L.B.; Dweep, H.; Yin, X.; Wang, H.; Damra, M.; Goldman, A.R.; Gorman, N.; Palmer, C.S.; Tang, H.-Y.; Shaikh, M.W.; et al. Plasma Markers of Disrupted Gut Permeability in Severe COVID-19 Patients. Front. Immunol. 2021, 12, 686240. [Google Scholar] [CrossRef] [PubMed]
- Piton, G.; Belon, F.; Cypriani, B.; Regnard, J.; Puyraveau, M.; Manzon, C.; Navellou, J.-C.; Capellier, G. Enterocyte Damage in Critically Ill Patients Is Associated With Shock Condition and 28-Day Mortality. Crit. Care Med. 2013, 41, 2169–2176. [Google Scholar] [CrossRef] [PubMed]
- Guedj, K.; Uzzan, M.; Soudan, D.; Trichet, C.; Nicoletti, A.; Weiss, E.; Manceau, H.; Nuzzo, A.; Corcos, O.; Treton, X.; et al. I-FABP is decreased in COVID-19 patients, independently of the prognosis. PLoS ONE 2021, 16, e0249799. [Google Scholar] [CrossRef]
- Piton, G.; Manzon, C.; Monnet, E.; Cypriani, B.; Barbot, O.; Navellou, J.-C.; Carbonnel, F.; Capellier, G. Plasma citrulline kinetics and prognostic value in critically ill patients. Intensiv. Care Med. 2010, 36, 702–706. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease is Suspected: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020.
- Logan, M.; MacKinder, M.; Clark, C.M.; Kountouri, A.; Jere, M.; Ijaz, U.Z.; Hansen, R.; McGrogan, P.; Russell, R.K.; Gerasimidis, K. Intestinal fatty acid binding protein is a disease biomarker in paediatric coeliac disease and Crohn’s disease. BMC Gastroenterol. 2022, 22, 260. [Google Scholar] [CrossRef]
- Elkhatib, I.; Buchman, A.L. Plasma Citrulline Concentration as a Marker for Disease Activity in Patients With Crohn’s Disease. J. Clin. Gastroenterol. 2012, 46, 308–310. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki World Medical Association Declaration of Helsinki. Bull. World Health Organ. 2013, 79, 373–374. [Google Scholar]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parasa, S.; Desai, M.; Chandrasekar, V.T.; Patel, H.K.; Kennedy, K.F.; Roesch, T.; Spadaccini, M.; Colombo, M.; Gabbiadini, R.; Artifon, E.L.A.; et al. Prevalence of Gastrointestinal Symptoms and Fecal Viral Shedding in Patients with Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2020, 3, e2011335. [Google Scholar] [CrossRef]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal–Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef] [PubMed]
- Boraschi, P.; Giugliano, L.; Mercogliano, G.; Donati, F.; Romano, S.; Neri, E. Abdominal and gastrointestinal manifestations in COVID-19 patients: Is imaging useful? World J. Gastroenterol. 2021, 27, 4143–4159. [Google Scholar] [CrossRef]
- Camilleri, M. Leaky gut: Mechanisms, measurement and clinical implications in humans. Gut 2019, 68, 1516–1526. [Google Scholar] [CrossRef]
- Sarikaya, M.; Ergul, B.; Dogan, Z.; Filik, L.; Can, M.; Arslan, L. Intestinal Fatty Acid Binding Protein (I-FABP) as a Promising Test for Crohn’s Disease: A Preliminary Study. Clin. Lab. 2015, 61, 87–91. [Google Scholar] [CrossRef]
- Adriaanse, M.P.M.; Tack, G.J.; Passos, V.L.; Damoiseaux, J.G.M.C.; Schreurs, M.W.J.; Van Wijck, K.; Riedl, R.G.; Masclee, A.A.M.; Buurman, W.A.; Mulder, C.J.J.; et al. Serum I-FABP as marker for enterocyte damage in coeliac disease and its relation to villous atrophy and circulating autoantibodies. Aliment. Pharmacol. Ther. 2013, 37, 482–490. [Google Scholar] [CrossRef]
- Crenn, P.; Coudray–Lucas, C.; Thuillier, F.; Cynober, L.; Messing, B. Postabsorptive plasma citrulline concentration is a marker of absorptive enterocyte mass and intestinal failure in humans. Gastroenterology 2000, 119, 1496–1505. [Google Scholar] [CrossRef]
- Fragkos, K.C.; Forbes, A. Citrulline as a marker of intestinal function and absorption in clinical settings: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2018, 6, 181–191. [Google Scholar] [CrossRef]
- van Vliet, M.J.; Tissing, W.J.; Rings, E.H.; Koetse, H.A.; Stellaard, F.; Kamps, W.A.; de Bont, E.S. Citrulline as a marker for chemotherapy induced mucosal barrier injury in pediatric patients. Pediatr. Blood Cancer 2009, 53, 1188–1194. [Google Scholar] [CrossRef]
- Ware, L.B.; Magarik, J.A.; Wickersham, N.; Cunningham, G.; Rice, T.W.; Christman, B.W.; Wheeler, A.P.; Bernard, G.R.; Summar, M.L. Low plasma citrulline levels are associated with acute respiratory distress syndrome in patients with severe sepsis. Crit. Care 2013, 17, R10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansone, L.; Briviba, M.; Silamikelis, I.; Terentjeva, A.; Perkons, I.; Birzniece, L.; Rovite, V.; Rozentale, B.; Viksna, L.; Kolesova, O.; et al. Amino Acid Metabolism is Significantly Altered at the Time of Admission in Hospital for Severe COVID-19 Patients: Findings from Longitudinal Targeted Metabolomics Analysis. Microbiol. Spectr. 2021, 9, e00338-21. [Google Scholar] [CrossRef]
- Obayan, A.O.E. Overview of the Rationale for L-Glutamine Treatment in Moderate-Severe COVID-19 Infection. J. Infect. Dis. Epidemiol. 2021, 7, 187. [Google Scholar] [CrossRef]
- Mehandru, S.; Poles, M.; Tenner-Racz, K.; Horowitz, A.; Hurley, A.; Hogan, C.; Boden, D.; Racz, P.; Markowitz, M. Primary HIV-1 Infection Is Associated with Preferential Depletion of CD4+ T Lymphocytes from Effector Sites in the Gastrointestinal Tract. J. Exp. Med. 2004, 200, 761–770. [Google Scholar] [CrossRef] [Green Version]
- Brenchley, J.M.; Price, D.A.; Douek, D.C. HIV disease: Fallout from a mucosal catastrophe? Nat. Immunol. 2006, 7, 235–239. [Google Scholar] [CrossRef]
- Skowyra, A.; Mikula, T.; Suchacz, M.; Skowyra, A.; Wiercińska-Drapało, A. The role of serum I-FABP concentration in assessment of small intestine mucosa among HIV-infected patients. Eur. J. Inflamm. 2015, 13, 75–81. [Google Scholar] [CrossRef]
- El Kamari, V.; Sattar, A.; Mccomsey, G.A. Brief Report: Gut Structural Damage: An Ongoing Process in Chronically Untreated HIV Infection. JAIDS J. Acquir. Immune Defic. Syndr. 2019, 80, 242–245. [Google Scholar] [CrossRef]
- Saia, R.S.; Giusti, H.; Luis-Silva, F.; Pedroso, K.J.B.; Auxiliadora-Martins, M.; Morejón, K.M.L.; Degiovani, A.M.; Cadelca, M.R.; Basile-Filho, A. Clinical investigation of intestinal fatty acid-binding protein (I-FABP) as a biomarker of SARS-CoV-2 infection. Int. J. Infect. Dis. 2021, 113, 82–86. [Google Scholar] [CrossRef]
- van Haren, F.M.P. Prognostic Value of Enterocyte Injury in Critically Ill Patients: No Gut, No Glory? Crit. Care Med. 2013, 41, 2238–2239. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.-X.; Chen, S.; Ma, L.-P.; Jiang, L.-Y.; Chen, J.-W.; Chang, R.-M.; Wen, L.-Q.; Wu, W.; Jiang, Z.-P.; Huang, Z.-T.; et al. Functional and Morphological Changes of the Gut Barrier during the Restitution Process after Hemorrhagic Shock. World J. Gastroenterol. 2005, 11, 35. [Google Scholar] [CrossRef] [PubMed]
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA-J. Am. Med. Assoc. 2020, 323, 1612–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, L.C.; Parodi, S.M.; Escobar, G.J.; Liu, V.X. Characteristics of Hospitalized Adults With COVID-19 in an Integrated Health Care System in California. JAMA-J. Am. Med. Assoc. 2020, 323, 2195–2198. [Google Scholar] [CrossRef]
- Sharma, S.; Badami, V.; Rojas, E.; Mittal, A.; Stansbury, R.; Rana, B.; Wilson, A.; Wen, S. ICU Mortality in Patients With Coronavirus Disease 2019 Infection: Highlighting Healthcare Disparities in Rural Appalachia. Crit. Care Explor. 2021, 3, e547. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. COVID-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef]
- Auld, S.C.; Caridi-Scheible, M.; Blum, J.M.; Robichaux, C.; Kraft, C.; Jacob, J.T.; Jabaley, C.S.; Carpenter, D.; Kaplow, R.; Hernandez-Romieu, A.C.; et al. ICU and Ventilator Mortality Among Critically Ill Adults with Coronavirus Disease 2019. Crit. Care Med. 2020, 48, e799–e804. [Google Scholar] [CrossRef]
- Carbonell, R.; Urgelés, S.; Rodríguez, A.; Bodí, M.; Martín-Loeches, I.; Solé-Violán, J.; Díaz, E.; Gómez, J.; Trefler, S.; Vallverdú, M.; et al. Mortality comparison between the first and second/third waves among 3,795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study. Lancet Reg. Health-Eur. 2021, 11, 100243. [Google Scholar] [CrossRef]
- Chen, T.-H.; Hsu, M.-T.; Lee, M.-Y.; Chou, C.-K. Gastrointestinal Involvement in SARS-CoV-2 Infection. Viruses 2022, 14, 1188. [Google Scholar] [CrossRef]
- Sekino, M.; Funaoka, H.; Sato, S.; Okada, K.; Inoue, H.; Yano, R.; Matsumoto, S.; Ichinomiya, T.; Higashijima, U.; Matsumoto, S.; et al. Intestinal fatty acid-binding protein level as a predictor of 28-day mortality and bowel ischemia in patients with septic shock: A preliminary study. J. Crit. Care 2017, 42, 92–100. [Google Scholar] [CrossRef]
- Leoni, M.L.G.; Lombardelli, L.; Colombi, D.; Bignami, E.G.; Pergolotti, B.; Repetti, F.; Villani, M.; Bellini, V.; Rossi, T.; Halasz, G.; et al. Prediction of 28-day mortality in critically ill patients with COVID-19: Development and internal validation of a clinical prediction model. PLoS ONE 2021, 16, e0254550. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Nonsurvivors, N = 23 | Survivors, N = 17 | p |
|---|---|---|---|
| Age (years) | 65 ± 3 (39–90) | 53 ± 3 (28–75) | 0.025 |
| Sex, male N(%) | 16 (69) | 9 (53) | 0.283 |
| APACHE II score | 19 ± 1 (9–33) | 14 ± 1 (6–24) | 0.018 |
| SOFA score | 9 ± 1 (3–13) | 7 ± 1 (4–12) | 0.126 |
| Comorbidities n (%) | |||
| Hypertension | 3 (13) | 6 (35) | 0.100 |
| Coronary heart disease | 6 (26) | 2 (12) | 0.239 |
| Chronic kidney disease | 6 (26) | 0 | 0.026 |
| Diabetes | 3 (13) | 2 (12) | 0.645 |
| Obesity | 1 (4) | 3 (17) | 0.197 |
| COPD | 1 (4) | 0 | 0.575 |
| BMI | 31 ± 2 (20–42) | 29 ± 1 (25–37) | 0.395 |
| Length of stay, ICU (day) | 13 ± 2 (3–44) | 27 ± 6 (2–106) | 0.049 |
| Length of stay, hospital (day) | 16 ± 2 (3–47) | 29 ± 4 (10–61) | 0.004 |
| Parameter | Nonsurvivors, N = 23 | Survivors, N = 17 | p |
|---|---|---|---|
| PCT (ng/mL) | 1.05 ± 0.24 (0.03–3.89) | 0.43 ± 0.11 (0.05–1.58) | 0.156 |
| CRP (mg/L) | 159 ± 24 (17–412) | 174 ± 23 (11–342) | 0.603 |
| WBC (103/uL) | 13.2 ± 1.0 (7.1–24.0) | 14.6 ± 1.8 (5.7–34.5) | 0.681 |
| Platelets (103/uL) | 237 ± 21 (60–505) | 293 ± 35 (111–553) | 0.373 |
| D-dimer (mg/L) | 15.27 ± 4.97 (0.54–87.15) | 14.33 ± 6.7 (0.47–98.12) | 0.198 |
| Fibrinogen (g/L) | 5.46 ± 0.46 (2.23–9.04) | 6.03 ± 0.5 (2.54–10) | 0.493 |
| Creatinine (mg/dL) | 1.29 ± 0.13 (0.47–2.66) | 0.86 ± 0.10 (0.46–1.87) | 0.015 |
| PaO2/FiO2 | 150 ± 12 (52–282) | 145 ± 14 (61–252) | 0.902 |
| Bilirubin (mg/dL) | 0.9 ± 0.1 (0.2–3.9) | 1.0 ± 0.2 (0.4–2.8) | 0.758 |
| Ferritine (ng/mL) | 1368 ± 392 (443–3474) | 714 ± 237 (71–1725) | 0.201 |
| Lactate (mmol/L) | 2.21 ± 0.21 (0.70–5.20) | 1.51 ± 0.15 (0.70–0.15) | 0.024 |
| Parameter | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 |
|---|---|---|---|---|---|
| AGI score (%) | |||||
| grade I/II | 100 | 93 | 90 | 97 | 92 |
| grade III/IV | 0 | 7 | 10 | 3 | 8 |
| Feeding intolerance (%) | 8 | 10 | 10 | 19 | 9 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Odds Ratio | p | Odds Ratio | p | |
| APACHE II | 1.165730 × 100 | 0.018 | 1.583274 × 100 | 0.018 |
| shock | 1.166667 × 101 | 0.004 | 8.958130 × 101 | 0.020 |
| I-FABP | 7.428571 × 100 | 0.005 | 5.114207 × 101 | 0.030 |
| age | 1.062695 × 100 | 0.018 | ||
| sex | 4.921875 × 10−1 | 0.286 | ||
| BMI | 1.066471 × 100 | 0.422 | ||
| SOFA | 1.234788 × 100 | 0.125 | ||
| PCT | 2.708447 × 100 | 0.006 | 3.078094 × 101 | 0.187 |
| CRP | 9.986929 × 10−1 | 0.669 | ||
| WBC | 1.002122 × 100 | 0.971 | ||
| Creatinine | 5.259518 × 100 | 0.024 | 2.216123 × 102 | 0.685 |
| Citrulline | 9.998672 × 10−1 | 0.995 | ||
| Lactate | 2.901363 × 100 | 0.057 | ||
| PaO2/FiO2 | 1.001565 × 100 | 0.078 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyszko, M.; Lipińska-Gediga, M.; Lemańska-Perek, A.; Kobylińska, K.; Gozdzik, W.; Adamik, B. Intestinal Fatty Acid Binding Protein (I-FABP) as a Prognostic Marker in Critically Ill COVID-19 Patients. Pathogens 2022, 11, 1526. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11121526
Tyszko M, Lipińska-Gediga M, Lemańska-Perek A, Kobylińska K, Gozdzik W, Adamik B. Intestinal Fatty Acid Binding Protein (I-FABP) as a Prognostic Marker in Critically Ill COVID-19 Patients. Pathogens. 2022; 11(12):1526. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11121526
Chicago/Turabian StyleTyszko, Maciej, Małgorzata Lipińska-Gediga, Anna Lemańska-Perek, Katarzyna Kobylińska, Waldemar Gozdzik, and Barbara Adamik. 2022. "Intestinal Fatty Acid Binding Protein (I-FABP) as a Prognostic Marker in Critically Ill COVID-19 Patients" Pathogens 11, no. 12: 1526. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11121526