
Achromobacter spp. in a Cohort of Non-Selected Pre- and Post-Lung Transplant Recipients

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Achromobacter spp. Pre-Transplantation
2.3. Achromobacter spp. in Relation to Transplantation
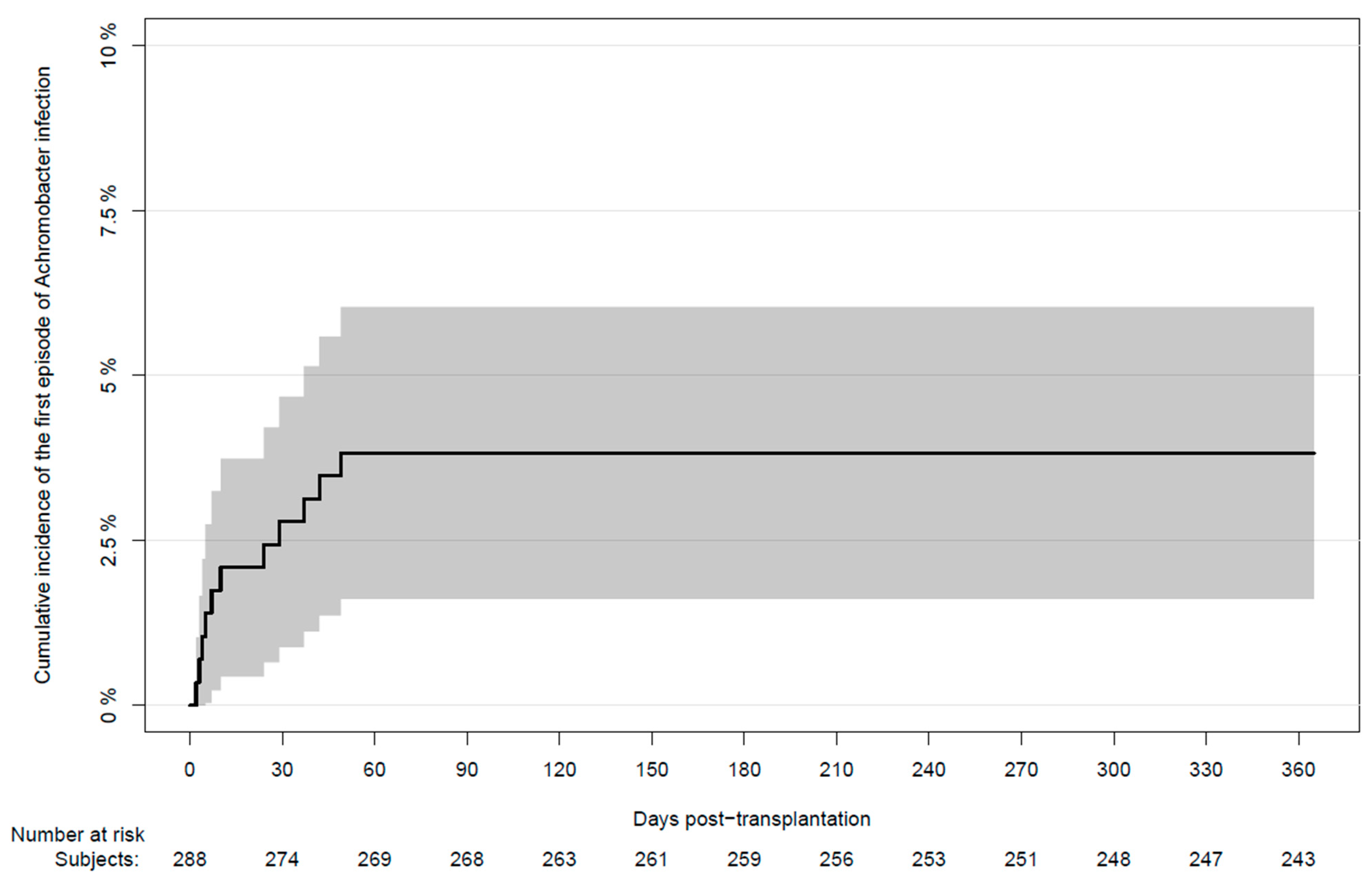
2.4. Achromobacter spp. after Transplantation
2.5. Characteristics of Infected Non-CF Patients
2.6. Characteristics of Infected CF Patients
2.7. Mortality
3. Discussions
4. Materials and Methods
4.1. Data Sources
4.2. Definitions
4.2.1. Achromobacter spp. Infections
4.2.2. Cultures
4.2.3. Immunosuppression and Antimicrobial Prophylaxis
4.2.4. Microbiological Surveillance
4.2.5. Incidence of Achromobacter spp. Infections after Transplantation
4.2.6. Cause of Death
4.3. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Cystic Fibrosis Patient without Infection Prior to Lung Transplantation
Appendix A.2. Patient with Achromobacter spp. Clearance after Lung Transplantation
Appendix B
Patients Included in Previous Publications
References
- Isler, B.; Kidd, T.J.; Stewart, A.G.; Harris, P.; Paterson, D.L. Achromobacter Infections and Treatment Options. Antimicrob. Agents Chemother. 2020, 64, e01025-20. [Google Scholar] [CrossRef] [PubMed]
- Spilker, T.; Vandamme, P.; Lipuma, J.J. Identification and Distribution of Achromobacter Species in Cystic Fibrosis. J. Cyst. Fibros. 2013, 12, 298–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swenson, C.E.; Sadikot, R.T. Achromobacter Respiratory Infections. Ann. Am. Thorac. Soc. 2015, 12, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Pan, F.; Guo, J.; Yan, W.; Jin, Y.; Liu, C.; Qin, L.; Fang, X. Hospital Acquired Pneumonia Due to Achromobacter Spp. in a Geriatric Ward in China: Clinical Characteristic, Genome Variability, Biofilm Production, Antibiotic Resistance and Integron in Isolated Strains. Front. Microbiol. 2016, 7, 621. [Google Scholar] [CrossRef] [PubMed]
- Pérez Barragán, E.; Sandino Pérez, J.; Corbella, L.; Orellana, M.A.; Fernández-Ruiz, M. Achromobacter Xylosoxidans Bacteremia: Clinical and Microbiological Features in a 10-Year Case Series. Rev. Esp. Quimioter. 2018, 31, 268–273. [Google Scholar] [PubMed]
- Marion-Sanchez, K.; Pailla, K.; Olive, C.; Le Coutour, X.; Derancourt, C. Achromobacter Spp. Healthcare Associated Infections in the French West Indies: A Longitudinal Study from 2006 to 2016. BMC Infect. Dis. 2019, 19, 795. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, J.P.; Lutgring, J.D.; Burd, E.M. Other Gram-Negative and Gram-Variable Bacilli. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier Health Sciences: Amsterdam, The Netherlands, 2020; pp. 2847–2864.e5. [Google Scholar]
- Wang, M.; Ridderberg, W.; Hansen, C.R.; Høiby, N.; Jensen-Fangel, S.; Olesen, H.V.; Skov, M.; Lemming, L.E.; Pressler, T.; Johansen, H.K.; et al. Early Treatment with Inhaled Antibiotics Postpones next Occurrence of Achromobacter in Cystic Fibrosis. J. Cyst. Fibros. 2013, 12, 638–643. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, S.M.; Penstoft, L.N.; Nørskov-Lauritsen, N. Motility, Biofilm Formation and Antimicrobial Efflux of Sessile and Planktonic Cells of Achromobacter Xylosoxidans. Pathogens 2019, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Somayaji, R.; Stanojevic, S.; Tullis, D.E.; Stephenson, A.L.; Ratjen, F.; Waters, V. Clinical Outcomes Associated with Achromobacter Species Infection in Patients with Cystic Fibrosis. Ann. Am. Thorac. Soc. 2017, 14, 1412–1418. [Google Scholar] [CrossRef]
- Hansen, C.R.; Pressler, T.; Nielsen, K.G.; Jensen, P.Ø.; Bjarnsholt, T.; Høiby, N. Inflammation in Achromobacter Xylosoxidans Infected Cystic Fibrosis Patients. J. Cyst. Fibros. 2010, 9, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Qvist, T.; Taylor-Robinson, D.; Waldmann, E.; Olesen, H.V.; Hansen, C.R.; Mathiesen, I.H.; Høiby, N.; Katzenstein, T.L.; Smyth, R.L.; Diggle, P.J.; et al. Comparing the Harmful Effects of Nontuberculous Mycobacteria and Gram Negative Bacteria on Lung Function in Patients with Cystic Fibrosis. J. Cyst. Fibros. 2016, 15, 380–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoch, P.E.; Cunha, B.A. Nosocomial Achromobacter Xylosoxidans Infections. Infect. Control Hosp. Epidemiol. 1988, 9, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Marion-Sanchez, K.; Olive, C.; Platon, M.-G.; Cesarine, M.; Derancourt, C.; Pailla, K. Achromobacter Xylosoxidans in Hospital Environments: Still Waters Run Deep. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Benvenuto, L.J.; Sonett, J.R. Long-Term Outcomes and Management of Lung Transplant Recipients. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 285–297. [Google Scholar] [CrossRef]
- Holm, A.E.; Schultz, H.H.L.; Johansen, H.K.; Pressler, T.; Lund, T.K.; Iversen, M.; Perch, M. Bacterial Re-Colonization Occurs Early after Lung Transplantation in Cystic Fibrosis Patients. J. Clin. Med. 2021, 10, 1275. [Google Scholar] [CrossRef]
- Lobo, L.J.; Tulu, Z.; Aris, R.M.; Noone, P.G. Pan-Resistant Achromobacter Xylosoxidans and Stenotrophomonas Maltophilia Infection in Cystic Fibrosis Does Not Reduce Survival After Lung Transplantation. Transplantation 2015, 99, 2196–2202. [Google Scholar] [CrossRef]
- Nolley, E.; Robinson, K.; Pilewski, J.; Sanchez, P.; D’Cunha, J.; Morrell, M. Lung Transplantation for Patients with Cystic Fibrosis and Achromobacter Xylosoxidans in the Lung Allocation Score Era. J. Heart Lung Transpl. 2019, 38, S315–S316. [Google Scholar] [CrossRef]
- Pouch, S.M.; Patel, G. Practice, the A.I.D.C. of Multidrug-Resistant Gram-Negative Bacterial Infections in Solid Organ Transplant Recipients—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transpl. 2019, 33, e13594. [Google Scholar] [CrossRef]
- Gabrielaite, M.; Bartell, J.A.; Nørskov-Lauritsen, N.; Pressler, T.; Nielsen, F.C.; Johansen, H.K.; Marvig, R.L. Transmission and Antibiotic Resistance of Achromobacter in Cystic Fibrosis. J. Clin. Microbiol. 2021, 59, e02911-20. [Google Scholar] [CrossRef]
- Ridderberg, W.; Bendstrup, K.E.M.; Olesen, H.V.; Jensen-Fangel, S.; Nørskov-Lauritsen, N. Marked Increase in Incidence of Achromobacter Xylosoxidans Infections Caused by Sporadic Acquisition from the Environment. J. Cyst. Fibros. 2011, 10, 466–469. [Google Scholar] [CrossRef] [Green Version]
- Ridderberg, W.; Wang, M.; Nørskov-Lauritsen, N. Multilocus Sequence Analysis of Isolates of Achromobacter from Patients with Cystic Fibrosis Reveals Infecting Species Other than Achromobacter Xylosoxidans. J. Clin. Microbiol. 2012, 50, 2688–2694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heldman, M.R.; Guo, K.; Nelson, B.; Babu, T.; Ison, M.G. Treatment of Multidrug-Resistant Gram-Negative Bacilli after Solid Organ Transplant: Outcomes and Complications. Transpl. Infect. Dis. 2021, 23, e13474. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.J.; Cheng, T.Z.; Honeybrook, A.L.; Gray, A.L.; Snyder, L.D.; Palmer, S.M.; Abi Hachem, R.; Jang, D.W. Correlation between Sinus and Lung Cultures in Lung Transplant Patients with Cystic Fibrosis. Int. Forum. Allergy Rhinol. 2018, 8, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Johansen, H.K.; Aanaes, K.; Pressler, T.; Nielsen, K.G.; Fisker, J.; Skov, M.; Høiby, N.; von Buchwald, C. Colonisation and Infection of the Paranasal Sinuses in Cystic Fibrosis Patients Is Accompanied by a Reduced PMN Response. J. Cyst. Fibros. 2012, 11, 525–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, M.-K.; Rachakonda, L.; Weill, D.; Hwang, P.H. Effects of Sinus Surgery on Lung Transplantation Outcomes in Cystic Fibrosis. Am. J. Rhinol. 2008, 22, 192–196. [Google Scholar] [CrossRef]
- Holzmann, D.; Speich, R.; Kaufmann, T.; Laube, I.; Russi, E.W.; Simmen, D.; Weder, W.; Boehler, A. Effects of Sinus Surgery in Patients with Cystic Fibrosis after Lung Transplantation: A 10-Year Experience. Transplantation 2004, 77, 134–136. [Google Scholar] [CrossRef]
- Aanaes, K.; von Buchwald, C.; Hjuler, T.; Skov, M.; Alanin, M.; Johansen, H.K. The Effect of Sinus Surgery with Intensive Follow-up on Pathogenic Sinus Bacteria in Patients with Cystic Fibrosis. Am. J. Rhinol. Allergy 2013, 27, e1–e4. [Google Scholar] [CrossRef]
- Aanaes, K.; Johansen, H.K.; Skov, M.; Buchvald, F.F.; Hjuler, T.; Pressler, T.; Hoiby, N.; Nielsen, K.G.; von Buchwald, C. Clinical Effects of Sinus Surgery and Adjuvant Therapy in Cystic Fibrosis Patients—Can Chronic Lung Infections Be Postponed? Rhinology 2013, 51, 222–230. [Google Scholar] [CrossRef]
- Verleden, G.M.; Glanville, A.R.; Lease, E.D.; Fisher, A.J.; Calabrese, F.; Corris, P.A.; Ensor, C.R.; Gottlieb, J.; Hachem, R.R.; Lama, V.; et al. Chronic Lung Allograft Dysfunction: Definition, Diagnostic Criteria, and Approaches to Treatment-A Consensus Report from the Pulmonary Council of the ISHLT. J. Heart Lung Transpl. 2019, 38, 493–503. [Google Scholar] [CrossRef] [Green Version]
- Centre of Excellence for Personalized Medicine of Infectious Complications in Immune Deficiency (PERSIMUNE). Available online: http://www.Persimune.Dk/ (accessed on 1 September 2020).
- Voldstedlund, M.; Haarh, M.; Mølbak, K. The Danish Microbiology Database (MIBA) 2010 to 2013. Eurosurveillance 2014, 19, 20667. [Google Scholar] [CrossRef] [Green Version]
- Proesmans, M.; Balinska-Miskiewicz, W.; Dupont, L.; Bossuyt, X.; Verhaegen, J.; Høiby, N.; de Boeck, K. Evaluating the “Leeds Criteria” for Pseudomonas Aeruginosa Infection in a Cystic Fibrosis Centre. Eur. Respir. J. 2006, 27, 937–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, B.D.; Greysson-Wong, J.; Somayaji, R.; Waddell, B.; Whelan, F.J.; Storey, D.G.; Rabin, H.R.; Surette, M.G.; Parkins, M.D. Prevalence and Outcomes of Achromobacter Species Infections in Adults with Cystic Fibrosis: A North American Cohort Study. J. Clin. Microbiol. 2017, 55, 2074–2085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wareham, N.E.; Da Cunha-Bang, C.; Borges, Á.H.; Ekenberg, C.; Gerstoft, J.; Gustafsson, F.; Hansen, D.; Heilmann, C.; Helleberg, M.; Hillingsø, J.; et al. Classification of Death Causes after Transplantation (CLASS): Evaluation of Methodology and Initial Results. Medicine 2018, 97, e11564. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Non-Achromobacter (n = 277) | Achromobacter spp. (n = 11) | Total (n = 288) | p-Value | |
|---|---|---|---|---|
| Age at transplantation, median (IQR) | 53 (46–59) | 33 (29–45) | 53 (44–58) | 0.006 |
| Male gender, n (%) | 144 (52) | 6 (55) | 150 (52) | 1.0 |
| Double lung transplantation, n (%) | 249 (90) | 11 (100) | 260 (90) | 0.540 |
| Underlying disease, n (%) | ||||
| Cystic fibrosis | 32 (12) | 9 (82) | 41 (14) | |
| Emphysema | 136 (49) | 1 (9.1) | 137 (48) | |
| Pulmonary fibrosis | 100 (36) | 1 (9.1) | 101 (35) | |
| Pulmonary hypertension | 9 (3.2) | 0 (0.0) | 9 (3.1) | <0.001 |
| Patient No | Underlying Disease | Achromobacter spp. Pre-LTX | Persistent Infection Pre-LTX | Achromobacter spp. in Relation to LTX | Days to Positive Culture | Species | Persistent Infection | Dead | Days to Death | Cause of Death |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | CF | Yes | Yes | Yes | 2 | A.X 1,2 | No | Yes | 1560 | Rejection 3 |
| 2 | CF | Yes | Yes | Yes | 7 | A.R 2 | No | Yes | 3284 | Rejection 3 |
| 3 | CF | Yes | No | No | 49 | A.X 1,2 | No | Yes | 1950 | Bacterial infection |
| 4 | CF | No | No | No | 5 | A.R 2 | No | Yes | 12 | Primary graft failure 4 |
| 5 | CF | Yes | No | No | 24 | A.S 1, A.X 2 | Yes | No | ||
| 6 | CF | Yes | Yes | Yes | 4 | A.X 1, A.R 2 | Yes | Yes | 2096 | Rejection 3 |
| 7 | CF | Yes | Yes | No | 3 | A.X 1,2 | Yes | Yes | 179 | Infection |
| 8 | CF | Yes | Yes | Yes | 10 | A.X 1,2 | Yes | Yes | 349 | Cardiac or vascular failure 5 |
| 9 | CF | Yes | No | No | 29 | A.X 1,2 | No | No | ||
| 10 | Emphysema | No | No | No | 37 | A.X | No | No | ||
| 11 | Fibrosis | No | No | No | 42 | A.S | No | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crone, C.G.; Rezahosseini, O.; Schultz, H.H.L.; Qvist, T.; Johansen, H.K.; Nielsen, S.D.; Perch, M. Achromobacter spp. in a Cohort of Non-Selected Pre- and Post-Lung Transplant Recipients. Pathogens 2022, 11, 181. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11020181
Crone CG, Rezahosseini O, Schultz HHL, Qvist T, Johansen HK, Nielsen SD, Perch M. Achromobacter spp. in a Cohort of Non-Selected Pre- and Post-Lung Transplant Recipients. Pathogens. 2022; 11(2):181. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11020181
Chicago/Turabian StyleCrone, Cornelia Geisler, Omid Rezahosseini, Hans Henrik Lawaetz Schultz, Tavs Qvist, Helle Krogh Johansen, Susanne Dam Nielsen, and Michael Perch. 2022. "Achromobacter spp. in a Cohort of Non-Selected Pre- and Post-Lung Transplant Recipients" Pathogens 11, no. 2: 181. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11020181