
Enduring Challenges despite Progress in Preventing Mother-to-Child Transmission of Hepatitis B Virus in Angola


Abstract
:1. Introduction
2. Results
2.1. Population Profile
2.2. Screening for HBV, Syphilis, and HIV
2.3. Risk Factor Assessment
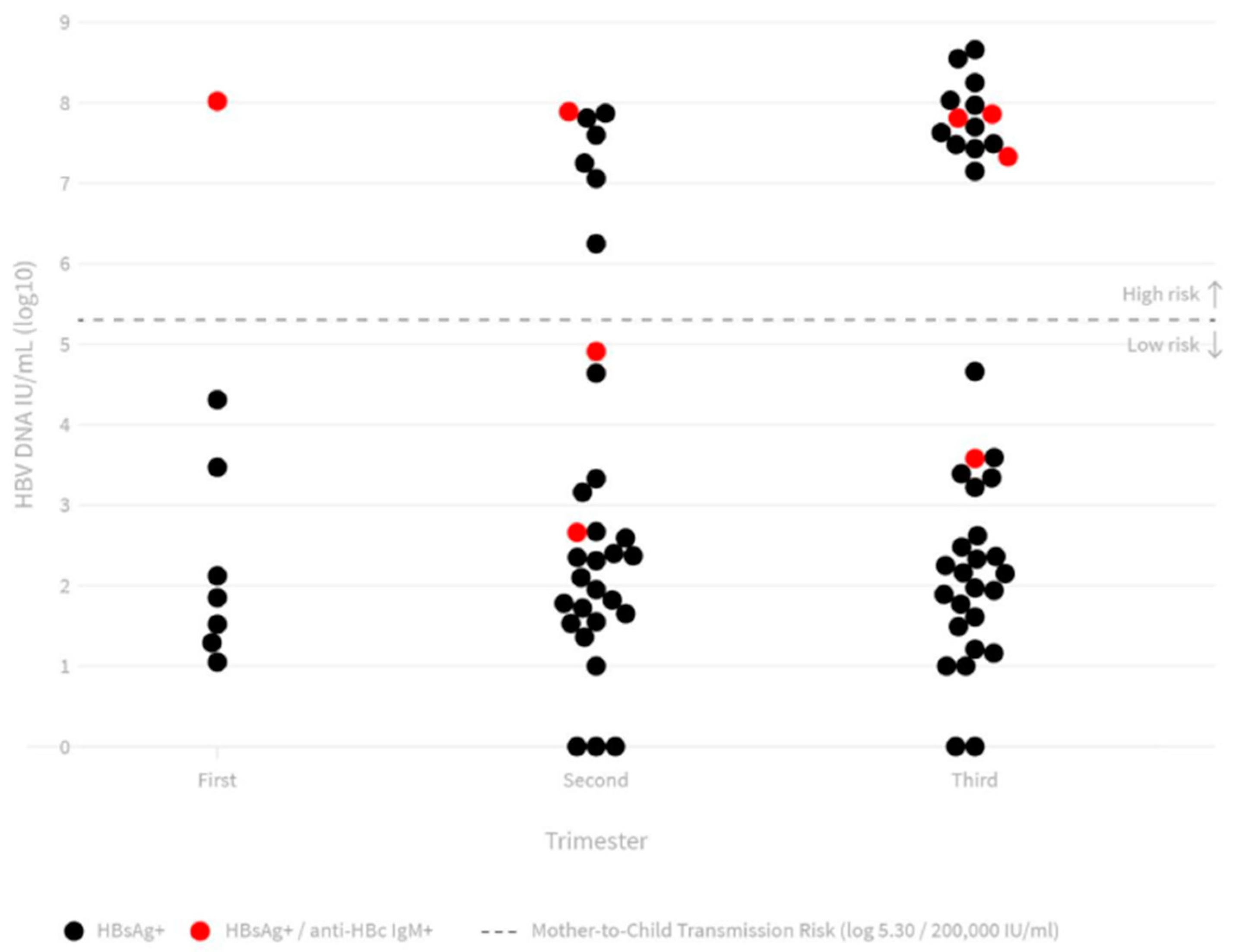
2.4. Serological and Molecular Testing for HBV
2.5. Offspring Tracking for HBV
3. Discussion
3.1. Mother-to Infant (Vertical) Transmission
3.1.1. Antenatal Care
3.1.2. Screening for Triple Infections (HBV, Syphilis and HIV)
3.1.3. Acute Hepatitis B Infection and Elevated Concentrations of HBV DNA
3.1.4. Timely Prophylaxis
3.1.5. Neonatal Challenge
3.2. Intrafamiliar Horizontal Transmission
3.3. Replicating Successful Programs to Eliminate MTCT
3.4. Study Limitations
4. Materials and Method
4.1. Study Population
4.2. Blood Specimens
4.2.1. Immediate Testing and Referral
4.2.2. Serological and Molecular Testing for HBV
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240027077 (accessed on 15 September 2021).
- World Health Organization. Global Guidance on Criteria and Processes for Validation: Elimination of Mother-to-Child Transmission of HIV, Syphilis and Hepatitis B Virus; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-003936-0. Available online: https://www.who.int/publications/i/item/9789240039360 (accessed on 30 November 2021).
- Cohn, J.; Owiredu, M.N.; Taylor, M.M.; Easterbrook, P.; Lesi, O.; Francoise, B.; Broyles, L.N.; Mushavi, A.; Van Holten, J.; Ngugi, C.; et al. Eliminating mother-to-child transmission of human immunodeficiency virus, syphilis and hepatitis B in sub-Saharan Africa. Bull. World Health Organ. 2021, 99, 287–295. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommended Interventions for Improving Maternal and Newborn Health: Integrated Management of Pregnancy and Childbirth; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/handle/10665/69509 (accessed on 17 November 2021).
- World Health Organization. Guidelines on Hepatitis B and C Testing; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/251330 (accessed on 18 November 2021).
- Dionne-Odom, J.; Mbah, R.; Rembert, N.J.; Tancho, S.; Halle-Ekane, G.E.; Enah, C.; Welty, T.K.; Tih, P.M.; Tita, A.T. Hepatitis B, HIV, and Syphilis Seroprevalence in Pregnant Women and Blood Donors in Cameroon. Infect Dis. Obstet. Gynecol. 2016, 2016, 4359401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furtado, M.; Directora Nacional do Instituto de Luta Contra o Sida, Luanda, Angola. Personal communication, 10 December 2021.
- World Health Organization. Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications-detail-redirect/978-92-4-000270-8 (accessed on 8 September 2021).
- Instituto Nacional de Estatística (INE); Ministério da Saúde (MINSA); Ministério do Planeamento e do Desenvolvimento Territorial (MINPLAN); ICF. Inquérito de Indicadores Múltiplos e de Saúde em Angola 2015–2016; INE; MINSA; MINPLAN; ICF: Luanda, Angola, 2017; Available online: https://dhsprogram.com/pubs/pdf/fr327/fr327.pdf (accessed on 3 November 2021).
- Tekelab, T.; Chojenta, C.; Smith, R.; Loxton, D. The impact of antenatal care on neonatal mortality in sub-Saharan Africa: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0222566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Antenatal Care for A Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241549912. Available online: https://www.who.int/news/item/07-11-2016-new-guidelines-on-antenatal-care-for-a-positive-pregnancy-experience (accessed on 11 November 2021).
- Chotun, N.; Preiser, W.; van Rensburg, C.J.; Fernandez, P.; Theron, G.B.; Glebe, D.; Andersson, M.I. Point-of-care screening for hepatitis B virus infection in pregnant women at an antenatal clinic: A South African experience. PLoS ONE 2017, 12, e0181267. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.; Harmanci, H.; Hutin, Y.; Hess, S.; Bulterys, M.; Peck, R.; Rewari, B.; Mozalevskis, A.; Shibeshi, M.; Mumba, M.; et al. Global progress on the elimination of viral hepatitis as a major public health threat: An analysis of WHO Member State responses 2017. JHEP Rep. 2019, 1, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Sebastião, C.S.; Neto, Z.; Jandondo, D.; Mirandela, M.; Morais, J.; Brito, M. HIV, hepatitis B virus, hepatitis C virus, and syphilis among pregnant women attending antenatal care in Luanda, Angola: Seroprevalence and risk factors. J. Med. Virol. 2020, 92, 3265–3270. [Google Scholar] [CrossRef]
- Abesig, J.; Chen, Y.; Wang, H.; Sompo, F.M.; Wu, I.X.Y. Prevalence of viral hepatitis B in Ghana between 2015 and 2019: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0234348. [Google Scholar] [CrossRef]
- Eyong, E.M.; Yankam, B.M.; Seraphine, E.; Ngwa, C.H.; Nkfusai, N.C.; Anye, C.S.; Nfor, G.K.; Cumber, S.N. The prevalence of HBsAg, knowledge and practice of hepatitis B prevention among pregnant women in the Limbe and Muyuka Health Districts of the Southwest region of Cameroon: A three-year retrospective study. Pan. Afr. Med. J. 2019, 32, 122. [Google Scholar] [CrossRef]
- Atilola, G.; Tomisin, O.; Randle, M.; Isaac, K.O.; Odutolu, G.; Olomu, J.; Adenuga, L. Epidemiology of HBV in Pregnant Women, Southwest Nigeria. J Epidemiol Glob Health. 2018, 8, 115–123. [Google Scholar] [CrossRef]
- Amsalu, A.; Ferede, G.; Eshetie, S.; Tadewos, A.; Assegu, D. Prevalence, Infectivity, and Associated Risk Factors of Hepatitis B Virus among Pregnant Women in Yirgalem Hospital, Ethiopia: Implication of Screening to Control Mother-to-Child Transmission. J. Pregnancy 2018, 2018, 8435910. [Google Scholar] [CrossRef] [Green Version]
- Kayondo, S.P.; Byamugisha, J.K.; Ntuyo, P. Prevalence of hepatitis B virus infection and associated risk factors among pregnant women attending antenatal clinic in Mulago Hospital, Uganda: A cross-sectional study. BMJ Open 2020, 10, e033043. [Google Scholar] [CrossRef]
- Geffert, K.; Maponga, T.G.; Henerico, S.; Preiser, W.; Mongella, S.; Stich, A.; Kalluvya, S.; Mueller, A.; Kasang, C. Prevalence of chronic HBV infection in pregnant woman attending antenatal care in a tertiary hospital in Mwanza, Tanzania: A cross-sectional study. BMC Infect Dis. 2020, 20, 395. [Google Scholar] [CrossRef]
- Webster, G.J.; Reignat, S.; Maini, M.K.; Whalley, S.A.; Ogg, G.S.; King, A.; Brown, D.; Amlot, P.L.; Williams, R.; Vergani, D.; et al. Incubation phase of acute hepatitis B in man: Dynamic of cellular immune mechanisms. Hepatology 2000, 32, 1117–1124. [Google Scholar] [CrossRef]
- Gambarin-Gelwan, M. Hepatitis B in Pregnancy. Clin. Liver Dis. 2007, 11, 945–963. [Google Scholar] [CrossRef]
- Mavilia, M.G.; Wu, G.Y. Mechanisms and Prevention of Vertical Transmission in Chronic Viral Hepatitis. J. Clin. Transl. Hepatol. 2017, 5, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pondé, R.A.D.A. The serological markers of acute infection with hepatitis A, B, C, D, E and G viruses revisited. Arch. Virol. 2017, 162, 3587–3602. [Google Scholar] [CrossRef] [PubMed]
- Dunkelberg, J.; Berkley, E.M.F.; Thiel, K.W.; Leslie, K.K. Hepatitis B and C in pregnancy: A review and recommendations for care. J. Perinatol. 2014, 34, 882–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da Saúde; Secretaria de Vigilância em Saúde; Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Protocolo Clínico e Diretrizes Terapêuticas para Prevenção da Transmissão Vertical do HIV, Sífilis e Hepatites Virais; Ministério da Saúde: Brasília, Brazil, 2019; 248p, ISBN 978-85-334-2630-6.
- Pan, C.Q.; Duan, Z.; Dai, E.; Zhang, S.; Han, G.; Wang, Y.; Zhang, H.; Zou, H.; Zhu, B.; Zhao, W.; et al. Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load. N. Engl. J. Med. 2016, 374, 2324–2334. [Google Scholar] [CrossRef] [PubMed]
- Keane, E.; Funk, A.L.; Shimakawa, Y. Systematic review with meta-analysis: The risk of mother-to-child transmission of hepatitis B virus infection in sub-Saharan Africa. Aliment. Pharmacol. Ther. 2016, 44, 1005–1017. [Google Scholar] [CrossRef] [Green Version]
- Veronese, P.; Dodi, I.; Esposito, S.; Indolfi, G. Prevention of vertical transmission of hepatitis B virus infection. World J. Gastroenterol. 2021, 27, 4182–4193. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S.B., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.K.; Kumar, M.P.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.-S.; Chen, H.L.; Chien, R.N.; Dokmeci, A.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Adelino, G.; Ministry of Health of Guinea-Bissau, WHO consultant, Rio, Brazil. Personal Communication, 17 November 2021.
- Seck, A.; Maylin, S.; Akbar, S.M.F.; Funk, A.L.; Bercion, R.; Mishiro, S.; Ndiaye, B.; Fontanet, A.; Vray, M.; Simon, F.; et al. Poor Sensitivity of Commercial Rapid Diagnostic Tests for Hepatitis B e Antigen in Senegal, West Africa. Am. J. Trop. Med. Hyg. 2018, 99, 428–434. [Google Scholar] [CrossRef]
- Stockdale, A.J.; Silungwe, N.M.; Shawa, I.T.; Kreuels, B.; Gordon, M.A.; Geretti, A.M. Diagnostic performance evaluation of hepatitis B e antigen rapid diagnostic tests in Malawi. BMC Infect. Dis. 2021, 21, 487. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde Secretaria de Ciência, Tecnologia, Inovação e Insumos Estratégicos em Saúde; Departamento de Gestão e Incorporação de Tecnologias e Inovação em Saúde; Coordenação-Geral de Gestão de Tecnologias em Saúde; Coordenação de Gestão de Protocolos Clínicos e Diretrizes Terapêuticas. Protocolo Clínico e Diretrizes Terapêuticas para Prevenção da Transmissão Vertical do HIV, Sífilis e Hepatites Virais. CONITEC, Brasília—DF 2020. Available online: http://conitec.gov.br/images/Consultas/Relatorios/2020/PCDT_PTV_HIV_CP_42_2020.pdf (accessed on 27 November 2021).
- Bodo, B.; Malande, O. Delayed introduction of the birth dose of Hepatitis B vaccine in EPI programs in East Africa: A missed opportunity for combating vertical transmission of Hepatitis B. Pan. Afr. Med. J. 2017, 27, 19. [Google Scholar] [CrossRef]
- Lesi, O.A.; Ward, J.W. Paving the way towards hepatitis B virus-free generations in Africa. Lancet Glob. Health 2021, 9, e1491–e1492. [Google Scholar] [CrossRef]
- Morais, A.; Coordenadora do Programa Nacional de Vacinação, Luanda, Angola. Personal communication, 1 August 2021.
- Nelson, C.M.; Wibisono, H.; Purwanto, H.; Mansyur, I.; Moniaga, V.; Widjaya, A. Hepatitis B vaccine freezing in the Indonesian cold chain: Evidence and solutions. Bull. World Health Organ. 2004, 82, 99–105. [Google Scholar]
- Wang, L.; Li, J.; Chen, H.; Li, F.; Armstrong, G.L.; Nelson, C.; Ze, W.; Shapiro, C.N. Hepatitis B vaccination of newborn infants in rural China: Evaluation of a village-based, out-of-cold-chain delivery strategy. Bull. World Health Organ. 2007, 85, 688–694. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hepatitis B vaccines: WHO Position Paper—July 2017. Wkly. Epidemiol. Rec. 2017, 92, 369–392. Available online: https://apps.who.int/iris/handle/10665/255873 (accessed on 10 November 2021).
- United Nations Children’s Fund & World Health Organization. Angola: WHO and UNICEF Estimates of Immunization Coverage: 2015 Revision, 5 July 2016. Available online: https://data.unicef.org/wp-content/uploads/country_profiles/Angola/Immunization_ago.pdf (accessed on 4 February 2022).
- World Health Organization. Worldwide Implementation of Hepatitis B Vaccination of Newborns, 2006. Wkly. Epidemiol. Rec. 2006, 83, 429–434. Available online: https://apps.who.int/iris/handle/10665/241243 (accessed on 10 December 2021).
- Whittle, H.; Mclauchlan, K.; Bradley, A.; Ajdukiewicz, A.; Howard, C.; Zuckerman, A.; Mcgregor, I. Hepatitis B Virus Infection in Two Gambian Villages. Lancet 1983, 321, 1203–1206. [Google Scholar] [CrossRef]
- Edmunds, W.J.; Medley, G.F.; Nokes, D.J.; O’Callaghan, C.J.; Whittle, H.C.; Hall, A.J. Epidemiological patterns of hepatitis B virus (HBV) in highly endemic areasr. Epidemiology Infect. 1996, 117, 313–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, S.; Boughton, C.R.; Dore, G.J. Blood-borne viruses and their survival in the environment: Is public concern about community needlestick exposures justified? Aust. New Zealand J. Public Health 2003, 27, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Schillie, S.; Vellozzi, C.; Reingold, A.; Harris, A.; Haber, P.; Ward, J.W.; Nelson, N.P. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm. Rep. 2018, 67, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.P.; Easterbrook, P.J.; McMahon, B.J. Epidemiology of Hepatitis B Virus Infection and Impact of Vaccination on Disease. Clin. Liver Dis. 2016, 20, 607–628. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection; World Health Organization: Geneva, Switzerland, 2015; Available online: https://www.who.int/publications-detail-redirect/9789241549059 (accessed on 11 October 2021).
- Pondé, R.A. Acute hepatitis B virus infection or acute exacerbation of chronic hepatitis B infection: The differential serological diagnosis. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 29–40. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | N | (%) | HBsAg Prevalence | OR | 95% CI | p Value |
|---|---|---|---|---|---|---|
| Total | 1012 | (100) | 8.7 | - | - | - |
| Age category (years) | ||||||
| 13–19 | 273 | (27.0) | 9.5 | 1.01 | 0.35–2.86 | 0.981 |
| 20–29 | 462 | (45.6) | 9.3 | 1.05 | 0.12–8.55 | 0.962 |
| 30–39 | 250 | (24.7) | 6.8 | 0.72 | 0.08–6.04 | 0.770 |
| ≥40 | 11 | (1.0) | 9.1 | 1.0- | ||
| Not known | 16 | (1.5) | 6.2 | 0.66 | 0.08–11.93 | 0.783 |
| Gestational age (weeks) | ||||||
| 1–12 | 84 | (8.3) | 10.7 | 1.32 | 0.61–2.82 | 0.471 |
| 13–24 | 412 | (41.1) | 8.9 | 1.04 | 0.82–1.31 | 0.722 |
| 25–42 | 505 | (49.9) | 8.3 | 1.0- | ||
| Unknown | 11 | (1.0) | 0.0 | - | - | - |
| Risk Factors | ||||||
| Antenatal care | ||||||
| Yes | 908 | (89.7) | 8.7 | 1.0- | ||
| No | 104 | (10.3) | 8.6 | 0.99 | 0.48–2.04 | 0.987 |
| Alcohol intake | ||||||
| Drinker | 113 | (11.4) | 8.8 | 1.01 | 0.50–2.06 | 0.963 |
| Non-drinker | 883 | (88.6) | 8.7 | 1.0- | ||
| Blood transfusion | ||||||
| Yes | 29 | (2.9) | 13.7 | 1.69 | 0.57–4.97 | 0.955 |
| No | 972 | (97.1) | 8.6 | 1.0- | ||
| Surgery | ||||||
| Yes | 55 | (5.5) | 5.4 | 0.58 | 0.17–1.90 | 0.373 |
| No | 945 | (94.5) | 9.9 | 1.0- | ||
| Tattoo | ||||||
| Yes | 30 | (3.0) | 16.6 | 2.14 | 0.79-5.74 | 0.130 |
| No | 972 | (97.0) | 8.5 | 1.0- | ||
| Body piercing | ||||||
| Yes | 883 | (88.1) | 9.0 | 1.61 | 0.72–3.58 | 0.238 |
| No | 119 | (11.9) | 5.8 | 1.0- | ||
| Scarification | ||||||
| Yes | 183 | (18.3) | 8.7 | 0.99 | 0.56–1.75 | 0.983 |
| No | 819 | (81.7) | 8.7 | 1.0- | ||
| Female genital circumcision | ||||||
| Yes | 11 | (1.1) | 9.1 | 1.03 | 0.13–8.21 | 0.971 |
| No | 991 | (99.9) | 8.7 | 1.0- | ||
| Razor sharing | ||||||
| Yes | 75 | (7.5) | 9.3 | 1.07 | 0.47–2.41 | 0.861 |
| No | 927 | (92.5) | 8.7 | 1.0- | ||
| Sharing of nail grooming appliances | ||||||
| Yes | 458 | (45.9) | 8.0 | 0.84 | 0.54–1.31 | 0.449 |
| No | 540 | 54.1) | 9.4 | 1.0- | ||
| Sharing of toothbrush | ||||||
| Yes | 62 | (6.2) | 9.6 | 1.12 | 0.46–2.68 | 0.797 |
| No | 940 | (93.8) | 8.7 | 1.0- | ||
| Use of intravaginal astringent substances | ||||||
| Yes | 500 | (50.0) | 8.0 | 0.81 | 0.52–1.27 | 0.372 |
| No | 500 | (50.0) | 9.6 | 1.0- | ||
| Anal sex | ||||||
| Yes | 191 | (19.1) | 7.3 | 0.78 | 0.43–1.42 | 0.429 |
| No | 810 | (80.9) | 9.1 | 1.0- | ||
| Oral sex | ||||||
| Yes | 147 | (14.7) | 8.1 | 0.90 | 0.48–1.71 | 0.771 |
| No | 854 | (85.3) | 8.8 | 1.0- | ||
| More than one sexual partner in the past 6 months | ||||||
| Yes | 14 | (1.4) | 14.2 | 1.74 | 0.38–7.92 | 0.470 |
| No | 987 | (98.6) | 8.7 | 1.0- | ||
| Polygamous sexual partner | ||||||
| Yes | 413 | (54.0) | 8.9 | 1.03 | 0.62–1.70 | 0.893 |
| No | 357 | (46.0) | 12.6 | 1.0- | ||
| No or infrequent use of condoms | ||||||
| Yes | 977 | (97.7) | 8.9 | 2.15 | 0.28–16.14 | 0.457 |
| No | 23 | (2.3) | 4.35 | 1.0- | ||
| Past history of STD | ||||||
| Yes | 99 | (9.9) | 12.1 | 1.49 | 0.78–2.85 | 0.223 |
| No | 900 | (90.1) | 8.4 | |||
| Syphilis | ||||||
| Yes | 69 | (7.1) | 8.7 | 1.01 | 0.42–2.42 | 0.972 |
| No | 910 | (92.9) | 8.5 | 1.0- | ||
| HIV | ||||||
| Yes | 10 | (1.1) | 10.0 | 1.16 | 0.14 -9.29 | 0.887 |
| No | 906 | (98.9) | 8.7 | 1.0- |
| Characteristics | HBsAg | Anti-HBc IgM | HBeAg | HBV DNA | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Positive | (%) | N | Positive | (%) | N | Positive | (%) | Median | Log10 IU/mL (Average ± sd) | N | >200,000 IU/mL | (%) | |
| Age category (years) | ||||||||||||||
| 13–19 | 273 | 26 | (9.5) | 17 | 3 | (17.6) | 17 | 7 | (41.2) | 2479 | 4.0 ± 2.9 | 23 | 8 | (34.8) |
| 2–29 | 462 | 43 | (9.3) | 36 | 3 | (8.3) | 36 | 10 | (27.8) | 228 | 3.4 ± 2.4 | 39 | 9 | (23.1) |
| 30–39 | 250 | 17 | (6.8) | 15 | 2 | (13.3) | 13 | 3 | (23.1) | 242 | 3.5 ± 2.9 | 14 | 4 | (28.6) |
| ≥40 | 11 | 1 | (9.1) | 1 | 0 | (0) | 1 | 0 | (0) | 36 | 1.5 * | 1 | 0 | (0) |
| Gestational age | ||||||||||||||
| 1st trimester | 84 | 9 | (10.7) | 6 | 1 | (16.7) | 6 | 1 | (16.7) | 102 | 2.9 ± 2.3 | 8 | 1 | (12.5) |
| 2nd trimester | 412 | 37 | (9.0) | 32 | 4 | (12.5) | 30 | 6 | (20.0) | 235 | 3.2 ± 2.5 | 31 | 7 | (22.6) |
| 3rd trimester | 505 | 42 | (8.3) | 32 | 4 | (12.5) | 32 | 14 | (43.7) | 1666 | 4.1 ± 2.9 | 39 | 14 | (35.9) |
| Coinfection | ||||||||||||||
| Syphilis positive | 69 | 6 | (8.7) | 5 | 1 | (20.0) | 5 | 3 | (60.0) | 3.59 × 107 | 5.2 ± 3.2 | 6 | 3 | (50.0) |
| negative | 910 | 78 | (8.6) | 62 | 7 | (11.3) | 60 | 18 | (30.0) | 235 | 3.5 ± 2.6 | 71 | 19 | (26.8) |
| HIV positive | 10 | 1 | (8.7) | 0 | - | - | 0 | - | - | 133 | 2.1 * | 1 | 0 | (0) |
| negative | 906 | 79 | (10.0) | 66 | 8 | (12.1) | 64 | 20 | (31.2) | 235 | 3.5 ± 2.7 | 73 | 20 | (27.4) |
| FAMILY | Profile | Age | Gender | HBsAg | HBeAg | Anti-HBc IgM | HBV DNA (10 log) | Vacine HBV |
|---|---|---|---|---|---|---|---|---|
| 1 | Mother | 27 | F | Positive | Positive | Neg | 1.21 | No |
| Child 1 | 9 | F | Neg | - | - | - | No | |
| Child 2 | 7 | F | Positive | Positive | Neg | - | No | |
| Child 3 | 5 | F | Positive | Neg | Neg | - | No | |
| Child 4 | 1 | M | Neg | Neg | Neg | - | Yes | |
| 2 | Mother | 34 | F | Positive | Neg | Neg | - | No |
| Child1 | 16 | F | Neg | - | - | - | No | |
| Child 2 | 9 | F | Positive | Positive | Neg | - | No | |
| Child 3 | 4 | M | Neg | - | - | - | No | |
| Child 4 | 1 | F | Neg | - | - | - | Yes | |
| 6 | Mother * | 42 | F | Positive | Neg | Neg | 1.55 | No |
| Child 1 | 21 | F | Neg | - | - | - | No | |
| Child 2 | 20 | F | Neg | - | - | - | No | |
| Child 3 | 14 | F | Neg | - | - | - | No | |
| Child 4 | 13 | F | Neg | - | - | - | No | |
| Child 5 | 10 | F | Positive | Neg | Neg | - | No | |
| Child 6 | 8 | F | Neg | - | - | - | No | |
| 7 | Mother | 27 | F | Neg | Neg | Neg | 3.16 | No |
| Child 1 | 10 | M | Neg | - | - | - | No | |
| Child 2 | 8 | F | Neg | - | - | - | No | |
| Child 3 | 7 | F | Neg | - | - | - | No | |
| Child 4 | 4 | F | Neg | - | - | - | No | |
| Child 5 | 1 | F | Neg | - | - | - | Yes | |
| 8 | Mother | 17 | F | Neg | Neg | Neg | 2.10 | No |
| Child 1 | 1 | F | Neg | - | - | - | Yes | |
| 9 | Mother * | 28 | F | Positive | Neg | Neg | - | No |
| Child 1 | 10 | M | Neg | - | - | - | No | |
| Child 2 | 6 | F | Neg | - | - | - | No | |
| Child 3 | 5 | M | Neg | - | - | - | No | |
| Child 4 | 3 | F | Neg | - | - | - | No | |
| Child 5 | 3m | F | Neg | - | - | - | incomplete | |
| 10 | Mother | 21 | F | Positive | Positive | Positive | 7.86 | No |
| Child 1 | 1 | M | Positive | Positive | Neg | - | Yes | |
| 11 | Mother * | 20 | F | Positive | Neg | Neg | 2.62 | No |
| Child 1 | 5 | M | Positive | Positive | Neg | - | No | |
| Child 2 | 4 | F | Positive | Positive | Positive | - | No | |
| Child 3 | 8m | F | Neg | - | - | - | Yes | |
| 15 | Mother | 29 | F | Positive | Neg | Neg | 1.0 | No |
| Child 1 | 1 | F | Neg | - | - | - | Yes | |
| 16 | Mother | 17 | F | Positive | Neg | Neg | - | No |
| Child 1 | 1 | M | Neg | - | - | - | Yes | |
| 17 | Mother * | 23 | F | Positive | Neg | Neg | 1.29 | No |
| Child 1 | 5 | F | Neg | - | - | - | No | |
| Child 2 | 3 | M | Neg | - | - | - | unknown | |
| 28 | Mother | 28 | F | Positive | Neg | Neg | - | No |
| Child 1 | 12 | M | Positive | Neg | Neg | - | No | |
| Child 2 | 7 | F | Positive | Neg | Positive | - | No | |
| Child 3 | 5 | F | Positive | Positive | Positive | - | No | |
| Child 4 | 2 | F | Neg | - | - | - | unknown | |
| 31 | Mother | 37 | F | Positive | Neg | Neg | - | No |
| Child 1 | 14 | F | Neg | - | - | - | No | |
| Child2 | 10 | F | Neg | - | - | - | No | |
| Child3 | 8 | M | Neg | - | - | - | No | |
| Child 4 | 4 | F | Neg | - | - | - | No | |
| Child 5 | 2 | M | Neg | - | - | - | Yes | |
| 107 | Mother | 23 | F | Positive | Neg | Neg | 3.33 | No |
| Child 1 | 2 | M | Neg | - | - | - | unknown | |
| Child 2 | 3m | F | Neg | - | - | - | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peliganga, L.B.; Horta, M.A.P.; Lewis-Ximenez, L.L. Enduring Challenges despite Progress in Preventing Mother-to-Child Transmission of Hepatitis B Virus in Angola. Pathogens 2022, 11, 225. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11020225
Peliganga LB, Horta MAP, Lewis-Ximenez LL. Enduring Challenges despite Progress in Preventing Mother-to-Child Transmission of Hepatitis B Virus in Angola. Pathogens. 2022; 11(2):225. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11020225
Chicago/Turabian StylePeliganga, Luis Baião, Marco Aurélio Pereira Horta, and Lia Laura Lewis-Ximenez. 2022. "Enduring Challenges despite Progress in Preventing Mother-to-Child Transmission of Hepatitis B Virus in Angola" Pathogens 11, no. 2: 225. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11020225