
Epidemiologic Investigation of Two Welder’s Anthrax Cases Caused by Bacillus cereus Group Bacteria: Occupational Link Established by Environmental Detection

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Epidemiologic Investigations
2.1.1. Patient A
2.1.2. Patient B
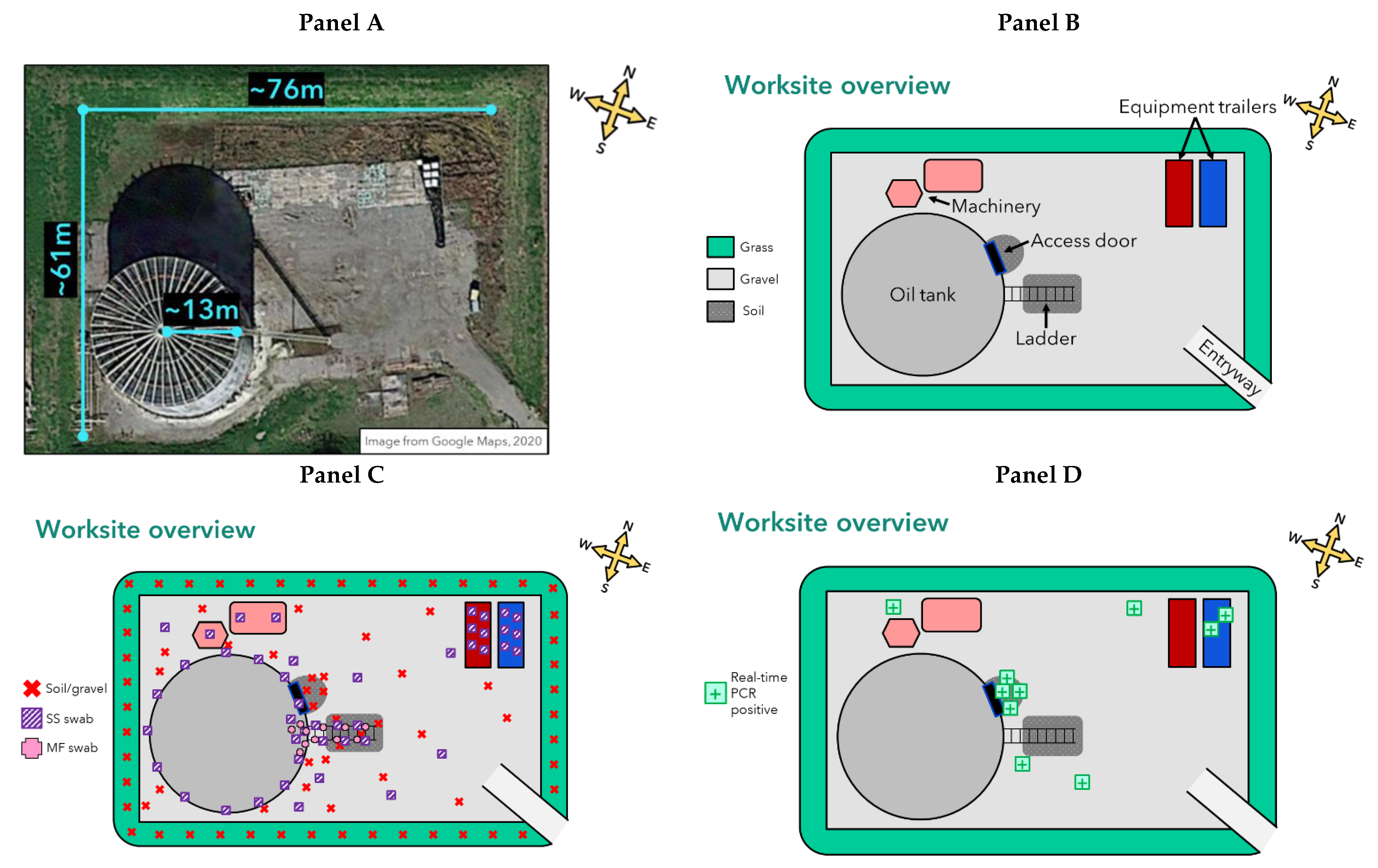
2.2. Environmental Sample Collection and Sampling Methodology
2.3. Laboratory Testing
2.4. Whole Genome Sequencing
3. Results
3.1. Epidemiologic Investigation—Patient A
3.2. Epidemiologic Investigation—Patient B
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
| Intended Recipients | Rationale | Recommendations |
| Worksite safety officer and welding employer | B. tropicus containing anthrax toxin genes was detected in a soil sample at patient A’s worksite, and it was a genetic match to the patient’s clinical isolate. Multiple other environmental samples tested real-time PCR-positive for the anthrax toxin genes. Therefore, the bacteria were still present at the worksite at the time of sampling and may pose a public health risk. |
|
| Family members sharing residence with patient A | Multiple environmental samples of work-related clothing and gear at patient A’s residence tested real-time PCR-positive for the anthrax toxin genes. Given that B. tropicus containing anthrax toxin genes was detected in a sample at the worksite and was a genetic match to the patient’s clinical isolate, it is possible these items were contaminated with the same bacteria that caused patient A’s illness and may pose a public health risk. | Family members may choose to keep or discard patient A’s work-related clothing and gear.
|
| * A 10% bleach solution was preferred over pH-adjusted bleach for safe use outside of a laboratory setting and was deemed adequate for disinfection of environmental surfaces. The resulting concentration of chlorine should be at least 5000 parts per million (ppm). | ||
References
- Brachman, P.S.; Kaufmann, A.F. Anthrax. In Bacterial Infections of Humans; Evans, A.S., Brachman, P.S., Eds.; Plenum Medical Book Company: New York, NY, USA, 1998; pp. 95–111. [Google Scholar]
- Jernigan, J.A.; Stephens, D.S.; Ashford, D.A.; Omenaca, C.; Topiel, M.S.; Galbraith, M.; Tapper, M.; Fisk, T.L.; Zaki, S.; Popovic, T.; et al. Bioterrorism-related inhalational anthrax: The first 10 cases reported in the United States. Emerg. Infect. Dis. 2001, 7, 933–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bales, M.E.; Dannenberg, A.L.; Brachman, P.S.; Kaufmann, A.F.; Klatsky, P.C.; Ashford, D.A. Epidemiologic response to anthrax outbreaks: Field investigations, 1950–2001. Emerg. Infect. Dis. 2002, 8, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. The prophylaxis and treatment of anthrax. Int. J. Antimicrob. Agents 2002, 20, 320–325. [Google Scholar] [CrossRef]
- Avashia, S.B.; Riggins, W.S.; Lindley, C.; Hoffmaster, A.; Drumgoole, R.; Nekomoto, T.; Jackson, P.J.; Hill, K.K.; Williams, K.; Lehman, L.; et al. Fatal Pneumonia among metalworkers due to inhalation exposure to Bacillus cereus containing Bacillus anthracis toxin genes. Clin. Infect. Dis. 2007, 44, 414–416. [Google Scholar] [CrossRef] [PubMed]
- Dawson, P.; Schrodt, C.A.; Feldmann, K.; Traxler, R.M.; Gee, J.E.; Kolton, C.B.; Marston, C.K.; Gulvik, C.A.; Antonini, J.M.; Negrón, M.E.; et al. Notes from the Field: Fatal Anthrax Pneumonia in Welders and Other Metalworkers Caused by Bacillus cereus Group Bacteria Containing Anthrax Toxin Genes—U.S. Gulf Coast States, 1994–2020. Morb. Mortal. Wkly. Rep. 2021, 70, 1453–1454. [Google Scholar] [CrossRef] [PubMed]
- Hoffmaster, A.R.; Ravel, J.; Rasko, D.A.; Chapman, G.D.; Chute, M.D.; Marston, C.K.; De, B.K.; Sacchi, C.T.; Fitzgerald, C.; Mayer, L.W.; et al. Identification of anthrax toxin genes in a Bacillus cereus associated with an illness resembling inhalation anthrax. Proc. Natl. Acad. Sci. USA 2004, 101, 8449–8454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marston, C.K.; Ibrahim, H.; Lee, P.; Churchwell, G.; Gumke, M.; Stanek, D.; Gee, J.E.; Boyer, A.E.; Gallegos-Candela, M.; Barr, J.R.; et al. Anthrax toxin-expressing Bacillus cereus isolated from an anthrax-like eschar. PLoS ONE 2016, 11, e0156987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pena-Gonzalez, A.; Marston, C.K.; Rodriguez-R, L.M.; Kolton, C.B.; Garcia-Diaz, J.; Theppote, A.; Frace, M.; Konstantinidis, K.T.; Hoffmaster, A.R. Draft genome sequence of Bacillus cereus LA2007, a human-pathogenic isolate harboring anthrax-like plasmids. Genome Announc. 2017, 5, e00181-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, A.M.; Beres, S.B.; Consamus, E.N.; Long, S.W.; Flores, A.R.; Barrios, R.; Richter, G.S.; Oh, S.-Y.; Garufi, G.; Maier, H.; et al. Rapidly progressive, fatal, inhalation anthrax-like infection in a human: Case report, pathogen genome sequencing, pathology, and coordinated response. Arch. Pathol. Lab. Med. 2011, 135, 1447–1459. [Google Scholar] [CrossRef]
- Hoffmaster, A.R.; Hill, K.K.; Gee, J.E.; Marston, C.K.; De, B.K.; Popovic, T.; Sue, D.; Wilkins, P.P.; Avashia, S.B.; Drumgoole, R.; et al. Characterization of Bacillus cereus Isolates Associated with Fatal Pneumonias: Strains Are Closely Related to Bacillus anthracis and Harbor B. anthracis Virulence Genes. J. Clin. Microbiol. 2006, 44, 3352–3360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Du, J.; Lai, Q.; Zeng, R.; Ye, D.; Xu, J.; Shao, Z. Proposal of nine novel species of the Bacillus cereus group. Int. J. Syst. Evol. Microbiol. 2017, 67, 2499–2508. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, P. Bacillus. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996. [Google Scholar]
- Wergeland, E.; Iversen, B. Deaths from pneumonia after welding. Scand. J. Work Environ. Health 2001, 27, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonini, J. Health effects of welding. Crit. Rev. Toxicol. 2003, 33, 61–103. [Google Scholar] [CrossRef] [PubMed]
- De Perio, M.A.; Hendricks, K.A.; Dowell, C.H.; Bower, W.A.; Burton, N.C.; Dawson, P.; Schrodt, C.A.; Salzer, J.S.; Marston, C.K.; Feldmann, K.; et al. Welder’s Anthrax: A Review of an Occupational Disease. Pathogens 2022, 11, 402. [Google Scholar] [CrossRef] [PubMed]
- CDC. The Laboratory Response Network Partners in Preparedness. Available online: https://emergency.cdc.gov/lrn/ (accessed on 1 March 2022).
- Hoffmaster, A.R.; Meyer, R.F.; Bowen, M.P.; Marston, C.K.; Weyant, R.S.; Thurman, K.; Messenger, S.L.; Minor, E.E.; Winchell, J.M.; Rasmussen, M.V.; et al. Evaluation and Validation of a Real-Time Polymerase Chain Reaction Assay for Rapid Identification of Bacillus anthracis. Emerg. Infect. Dis. 2002, 8, 1178–1182. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, K.; Martines, R.B.; Bielamowicz, H.; Boyer, A.E.; Long, S.; Byers, P.; Stoddard, R.A.; Taylor, K.; Kolton, C.B.; Gallegos-Candela, M.; et al. Welder’s Anthrax: A Tale of Two Cases. Clin. Infect. Dis. 2022; in press. [Google Scholar]
- CDC. Surface Sampling Procedures for Bacillus anthracis Spores from Smooth, Non-Porous Surfaces. Available online: https://www.cdc.gov/niosh/topics/emres/surface-sampling-bacillus-anthracis.html (accessed on 30 May 2020).
- Rose, L.J.; Hodges, L.; O’Connell, H.; Noble-Wang, J. National Validation Study of a Cellulose Sponge Wipe-Processing Method for Use after Sampling Bacillus anthracis Spores from Surfaces. Appl. Environ. Microbiol. 2011, 77, 8355–8359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marston, C.K.; Gee, J.E.; Popovic, T.; Hoffmaster, A.R. Molecular approaches to identify and differentiate Bacillus anthracis from phenotypically similar Bacillus species isolates. BMC Microbiol. 2006, 6, 22. [Google Scholar] [CrossRef] [Green Version]
- Treangen, T.J.; Ondov, B.D.; Koren, S.; Phillippy, A.M. The Harvest suite for rapid core-genome alignment and visualization of thousands of intraspecific microbial genomes. Genome Biol. 2014, 15, 524. [Google Scholar] [CrossRef] [Green Version]
- Gold, H. Anthrax: A Review of Sixty Cases, With a Report on the Therapeutic Use of Sulfonamide Compounds. Arch. Intern. Med. 1942, 70, 785–821. [Google Scholar] [CrossRef]
- Fergusson, W.M. A Case of Anthrax Treated by Sclavo’s Serum. Br. Med. J. 1911, 2, 103–104. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, A.E. Anthrax in a 15 Months Old Baby. Br. Med. J. 1929, 2, 667. [Google Scholar] [CrossRef] [PubMed]
- Herley, R. Eight Cases of External Anthrax. Lancet 1909, 174, 1662–1665. [Google Scholar] [CrossRef] [Green Version]
- CDC. Hierarchy of Controls. Available online: https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed on 25 April 2022).
- CDC. Health Hazard Evaluations (HHEs). Available online: https://www.cdc.gov/niosh/hhe/default.html (accessed on 25 April 2022).
- CDC. The Respiratory Protection Information Trusted Source. Available online: https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/respsource.html (accessed on 25 April 2022).
- Bower, W.A.; Hendricks, K.; Pillai, S.; Guarnizo, J.; Meaney-Delman, D. Clinical Framework and Medical Countermeasure Use During an Anthrax Mass-Casualty Incident. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2015, 64, 1–22. [Google Scholar]
- Weber, D.J.; Sickbert-Bennett, E.; Gergen, M.F.; Rutala, W.A. Efficacy of Selected Hand Hygiene Agents Used to Remove Bacillus atrophaeus (a Surrogate of Bacillus anthracis) From Contaminated Hands. JAMA 2003, 289, 1274–1277. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number of Samples | Sampling Site * | Sampling Location | Sample Type † | Real-Time PCR Result § | Culture Result | WGS Result |
|---|---|---|---|---|---|---|
| 1 | Worksite | Front of oil tank access door | Soil | Positive | Positive | B. tropicus¶ |
| 3 | Worksite | Front of oil tank access door | Soil | Positive | Negative | N/A |
| 4 | Worksite | Worksite grounds | Gravel | Positive | Negative | N/A |
| 2 | Worksite | Grinder tools and cabinets | SS swab in NB | Positive | Negative | N/A |
| Total 10 real-time PCR-positive samples from worksite (8%) | ||||||
| 3 | Residence | Work boots | MF swab in PBS | Positive | Negative | N/A |
| 1 | Residence | Work lunch cooler | SS swab in NB | Positive | Negative | N/A |
| Total 4 real-time PCR-positive samples from work-related clothing and gear at residence (22%) | ||||||
| 1 | Worksite | Beneath oil tank ladder | Soil | Inconclusive | Negative | N/A |
| 1 | Worksite | Worksite grounds | Gravel | Inconclusive | Negative | N/A |
| 1 | Worksite | Rubber mats and wood pallets | SS swab in NB | Inconclusive | Negative | N/A |
| 1 | Worksite | Welding rods and container | SS swab in NB | Inconclusive | Negative | N/A |
| Total 4 real-time PCR-inconclusive samples from worksite (3%) | ||||||
| 55 | Worksite | Various locations | Soil | Negative | Not done | N/A |
| 11 | Worksite | Various locations | Gravel | Negative | Not done | N/A |
| 41 | Worksite | Various locations | SS swab in NB | Negative | Not done | N/A |
| 11 | Worksite | Various locations | MF swab in PBS | Negative | Not done | N/A |
| Total 118 real-time PCR-negative samples from worksite (89%) | ||||||
| 2 | Residence | Work-related clothing/gear | Filter cartridge | Negative | Not done | N/A |
| 4 | Residence | Work-related clothing/gear | SS swab in NB | Negative | Not done | N/A |
| 8 | Residence | Work-related clothing/gear | MF swab in PBS | Negative | Not done | N/A |
| Total 14 real-time PCR-negative samples from work-related clothing and gear at residence (78%) | ||||||
| 18 | Residence | Yard—various locations | Soil | Negative | Not done | N/A |
| 5 | Residence | Yard—various locations | Gravel | Negative | Not done | N/A |
| 12 | Residence | Yard—various locations | SS swab in NB | Negative | Not done | N/A |
| Total 35 real-time PCR-negative samples from yard at residence (100%) | ||||||
| LA2020 Clinical | LA2020b Environmental | G9241 1 | 03BB87 2 | LA2007 3 | BcFL2013 4 | BC-AK 5 | |
|---|---|---|---|---|---|---|---|
| LA2020 Clinical | 0 | ||||||
| LA2020b Environmental | 2 | 0 | |||||
| G9241 | 39 | 39 | 0 | ||||
| 03BB87 | 120 | 120 | 147 | 0 | |||
| LA2007 | 216 | 218 | 213 | 319 | 0 | ||
| BcFL2013 | 244 | 246 | 241 | 347 | 62 | 0 | |
| BC-AK | 1005 | 1005 | 1000 | 1113 | 1139 | 1165 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dawson, P.; Salzer, J.S.; Schrodt, C.A.; Feldmann, K.; Kolton, C.B.; Gee, J.E.; Marston, C.K.; Gulvik, C.A.; Elrod, M.G.; Villarma, A.; et al. Epidemiologic Investigation of Two Welder’s Anthrax Cases Caused by Bacillus cereus Group Bacteria: Occupational Link Established by Environmental Detection. Pathogens 2022, 11, 825. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11080825
Dawson P, Salzer JS, Schrodt CA, Feldmann K, Kolton CB, Gee JE, Marston CK, Gulvik CA, Elrod MG, Villarma A, et al. Epidemiologic Investigation of Two Welder’s Anthrax Cases Caused by Bacillus cereus Group Bacteria: Occupational Link Established by Environmental Detection. Pathogens. 2022; 11(8):825. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11080825
Chicago/Turabian StyleDawson, Patrick, Johanna S. Salzer, Caroline A. Schrodt, Karl Feldmann, Cari B. Kolton, Jay E. Gee, Chung K. Marston, Christopher A. Gulvik, Mindy G. Elrod, Aaron Villarma, and et al. 2022. "Epidemiologic Investigation of Two Welder’s Anthrax Cases Caused by Bacillus cereus Group Bacteria: Occupational Link Established by Environmental Detection" Pathogens 11, no. 8: 825. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11080825