
Cardiac Safety of mRNA-Based Vaccines in Patients with Systemic Lupus Erythematosus and Lupus-like Disorders with a History of Myocarditis
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Connective Tissue Disease Status
2.3. Clinical and Laboratory Markers of Myocarditis Activity
2.4. Statistical Analysis
3. Results
3.1. Patients and Disease Characteristics at Baseline
3.2. Clinical and Laboratory Feature Variations over Time
3.2.1. Disease Activity
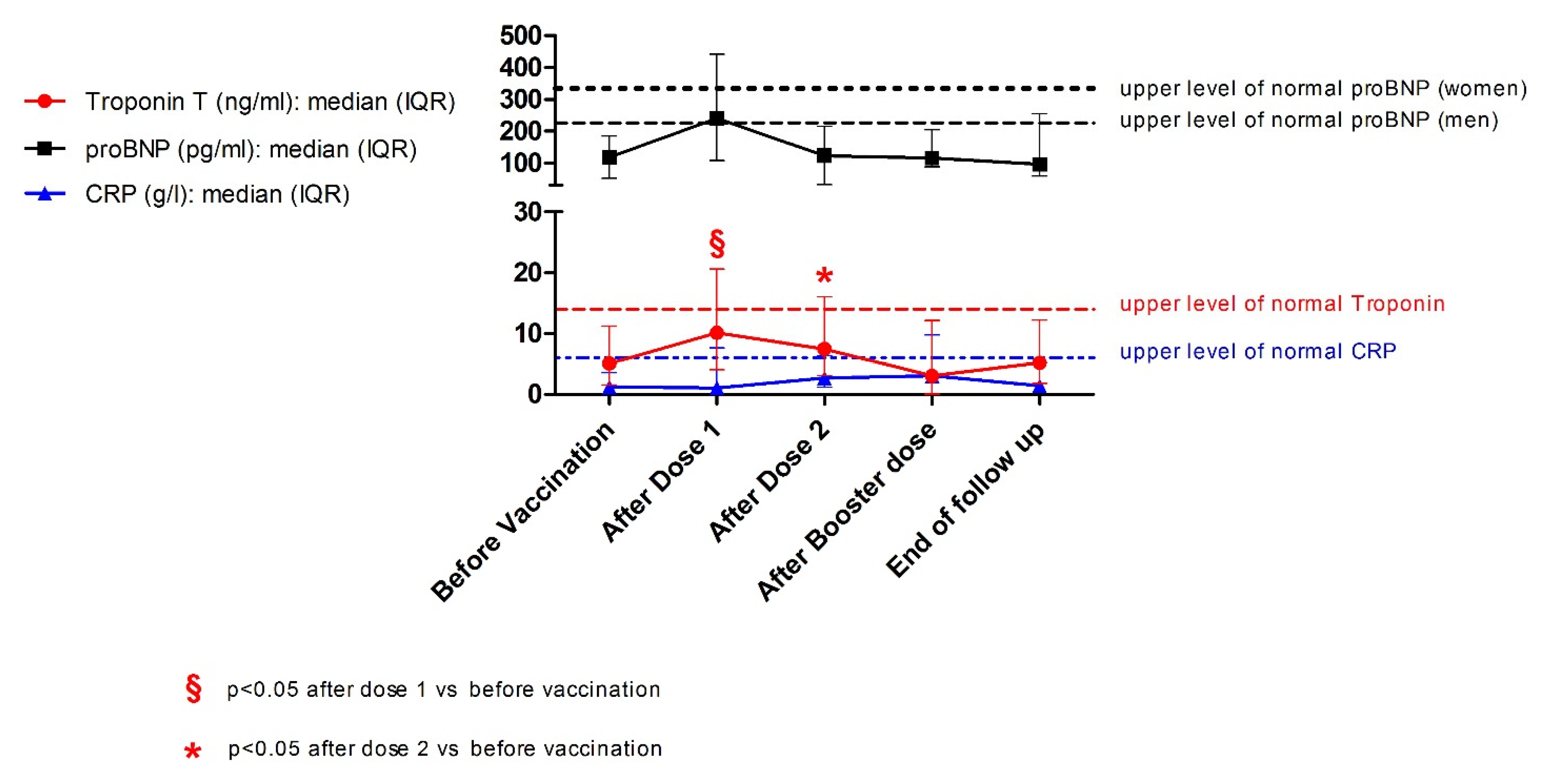
3.2.2. Markers of Myocardial Inflammation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joo, Y.B.; Kim, K.J.; Park, K.S.; Park, Y.J. Influenza infection as a trigger for systemic lupus erythematosus flares resulting in hospitalization. Sci. Rep. 2021, 11, 4630. [Google Scholar] [CrossRef] [PubMed]
- Strangfeld, A.; Schäfer, M.; Gianfrancesco, M.A.; Lawson-Tovey, S.; Liew, J.W.; Ljung, L.; Mateus, E.F.; Richez, C.; Santos, M.J.; Schmajuk, G.; et al. Factors associated with COVID-19-related death in people with rheumatic diseases: Results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2021, 80, 930–942. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, G.A.; Argolini, L.M.; Bellocchi, C.; Moroni, L.; Della-Torre, E.; Farina, N.; Caporali, R.F.; Beretta, L.; Gerosa, M.; Bozzolo, E.P.; et al. Impact of the COVID-19 pandemic in patients with systemic lupus erythematosus throughout one year. Clin. Immunol. 2021, 1, 108845. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [PubMed]
- Barbhaiya, M.; Levine, J.M.; Bykerk, V.P.; Jannat-Khah, D.; Mandl, L.A. Systemic rheumatic disease flares after SARS-CoV-2 vaccination among rheumatology outpatients in New York City. Ann. Rheum. Dis. 2021, 80, 1352–1354. [Google Scholar] [CrossRef]
- Felten, R.; Kawka, L.; Dubois, M.; Ugarte-Gil, M.F.; Fuentes-Silva, Y.; Piga, M.; Arnaud, L. Tolerance of COVID-19 vaccination in patients with systemic lupus erythematosus: The international VACOLUP study. Lancet Rheumatol. 2021, 3, e613–e615. [Google Scholar] [CrossRef]
- Chu, D.K.; Abrams, E.M.; Golden, D.B.; Blumenthal, K.G.; Wolfson, A.R.; Stone, C.A.; Krantz, M.S.; Shaker, M.; Greenhawt, M. Risk of Second Allergic Reaction to SARS-CoV-2 Vaccines: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2022, 182, 376–385. [Google Scholar] [CrossRef]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef]
- Wang, M.; Wen, W.; Zhou, M.; Wang, C.; Feng, Z.H. Meta-Analysis of Risk of Myocarditis After Messenger RNA COVID-19 Vaccine. Am. J. Cardiol. 2022, 167, 155–157. [Google Scholar] [CrossRef]
- Cordero, A.; Cazorla, D.; Escribano, D.; Quintanilla, M.A.; López-Ayala, J.M.; Berbel, P.P.; Bertomeu-González, V. Myocarditis after RNA-based vaccines for coronavirus. Int. J. Cardiol. 2022, 353, 131–134. [Google Scholar] [CrossRef]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef]
- Husby, A.; Hansen, J.V.; Fosbøl, E.; Thiesson, E.M.; Madsen, M.; Thomsen, R.W.; Sørensen, H.T.; Andersen, M.; Wohlfahrt, J.; Gislason, G.; et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: Population based cohort study. BMJ 2021, 375, e068665. [Google Scholar] [CrossRef]
- Lai, F.T.; Li, X.; Peng, K.; Huang, L.; Ip, P.; Tong, X.; Chui, C.S.; Wan, E.Y.; Wong, C.K.; Chan, E.W.; et al. Carditis After COVID-19 Vaccination with a Messenger RNA Vaccine and an Inactivated Virus Vaccine: A Case-Control Study. Ann. Intern. Med. 2022, 175, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Floyd, A.; Lal, A.; Molina, K.; Puchalski, M.; Miller, D.; May, L. When Lightning Strikes Twice in Pediatrics: Case Report and Review of Recurrent Myocarditis. Pediatrics 2018, 141, e20164096. [Google Scholar] [CrossRef] [PubMed]
- Smatti, M.K.; Cyprian, F.S.; Nasrallah, G.K.; Al Thani, A.A.; Almishal, R.O.; Yassine, H.M. Viruses and Autoimmunity: A Review on the Potential Interaction and Molecular Mechanisms. Viruses 2019, 11, 762. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Nebro, A.; Rúa-Figueroa, Í.; López-Longo, F.J.; Galindo-Izquierdo, M.; Calvo-Alén, J.; Olivé-Marqués, A.; Ordóñez-Cañizares, C.; Martín-Martínez, M.A.; Blanco, R.; Melero-González, R.; et al. Cardiovascular Events in Systemic Lupus Erythematosus: A Nationwide Study in Spain From the RELESSER Registry. Medicine 2015, 94, e1183. [Google Scholar] [CrossRef]
- Liu, Y.; Kaplan, M.J. Cardiovascular disease in systemic lupus erythematosus: An update. Curr. Opin. Rheumatol. 2018, 30, 441–448. [Google Scholar] [CrossRef]
- Ramirez, G.A.; Efthymiou, M.; Isenberg, D.A.; Cohen, H. Under crossfire: Thromboembolic risk in systemic lupus erythematosus. Rheumatology 2019, 58, 940–952. [Google Scholar] [CrossRef]
- Doria, A.; Iaccarino, L.; Sarzi-Puttini, P.; Atzeni, F.; Turriel, M.; Petri, M. Cardiac involvement in systemic lupus erythematosus. Lupus 2005, 14, 683–686. [Google Scholar] [CrossRef]
- Du Toit, R.; Reuter, H.; Walzl, G.; Snyders, C.; Chegou, N.N.; Herbst, P.G.; Doubell, A.F. Serum cytokine levels associated with myocardial injury in systemic lupus erythematosus. Rheumatology 2021, 60, 2010–2021. [Google Scholar] [CrossRef]
- Panchal, L.; Divate, S.; Vaideeswar, P.; Pandit, S.P. Cardiovascular involvement in systemic lupus erythematosus: An autopsy study of 27 patients in India. J. Postgrad. Med. 2006, 52, 5–10. [Google Scholar]
- Cheng, C.Y.; Baritussio, A.; Giordani, A.S.; Iliceto, S.; Marcolongo, R.; Caforio, A.L.P. Myocarditis in systemic immune-mediated diseases: Prevalence, characteristics and prognosis. A systematic review. Autoimmun. Rev. 2022, 21, 103037. [Google Scholar] [CrossRef]
- Du Toit, R.; Herbst, P.G.; van Rensburg, A.; du Plessis, L.M.; Reuter, H.; Doubell, A.F. Clinical features and outcome of lupus myocarditis in the Western Cape, South Africa. Lupus 2017, 26, 38–47. [Google Scholar] [CrossRef]
- Thomas, G.; Aubart, F.C.; Chiche, L.; Haroche, J.; Hié, M.; Hervier, B.; Costedoat-Chalumeau, N.; Mazodier, K.; Ebbo, M.; Cluzel, P.; et al. Lupus Myocarditis: Initial Presentation and Longterm Outcomes in a Multicentric Series of 29 Patients. J. Rheumatol. 2016, 44, 24–32. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef]
- Mosca, M.; Neri, R.; Bombardieri, S. Undifferentiated connective tissue diseases (UCTD): A review of the literature and a proposal for preliminary classification criteria. Clin. Exp. Rheumatol. 1999, 17, 615–620. [Google Scholar]
- Tanaka, Y.; Kuwana, M.; Fujii, T.; Kameda, H.; Muro, Y.; Fujio, K.; Itoh, Y.; Yasuoka, H.; Fukaya, S.; Ashihara, K.; et al. 2019 Diagnostic criteria for mixed connective tissue disease (MCTD): From the Japan research committee of the ministry of health, labor, and welfare for systemic autoimmune diseases. Mod. Rheumatol. 2020, 31, 29–33. [Google Scholar] [CrossRef]
- Zawadowski, G.M.; Klarich, K.W.; Moder, K.G.; Edwards, W.D.; Cooper, L. A contemporary case series of lupus myocarditis. Lupus 2012, 21, 1378–1384. [Google Scholar] [CrossRef]
- Ministero-Della-Salute-(Italian-Ministry-of-Health). Archivio Normativa Vaccinazioni [Archive of the Regulations on Vaccination]. 2021. Available online: https://www.salute.gov.it/portale/vaccinazioni/archivioNormativaVaccinazioni.jsp (accessed on 8 March 2022).
- Ramirez, G.A.; Della-Torre, E.; Moroni, L.; Yacoub, M.R.; Dagna, L.; OSR-COVAX Group. Correspondence on Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann. Rheum. Dis. 2021. In press. [Google Scholar] [CrossRef]
- Franklyn, K.; Lau, W.C.S.; Navarra, S.V.; Louthrenoo, W.; Lateef, A.; Hamijoyo, L.; Wahono, C.S.; Le Chen, S.; Jin, O.; Morton, S.; et al. Definition and initial validation of a Lupus Low Disease Activity State (LLDAS). Ann. Rheum. Dis. 2015, 75, 1615–1621. [Google Scholar] [CrossRef] [PubMed]
- Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar] [PubMed]
- Isenberg, D.A.; Rahman, A.; Allen, E.B.; Farewell, V.; Akil, M.; Bruce, I.N.; D’cruz, D.; Griffiths, B.; Khamashta, M.; Maddison, P.; et al. BILAG 2004. Development and initial validation of an updated version of the British Isles Lupus Assessment Group’s disease activity index for patients with systemic lupus erythematosus. Rheumatology 2005, 44, 902–906. [Google Scholar] [CrossRef] [PubMed]
- Isenberg, D.A.; Rahman, A.; Allen, E.B.; Farewell, V.; Akil, M.; Bruce, I.N.; D’cruz, D.; Griffiths, B.; Khamashta, M.; Maddison, P. The Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index for Systemic Lupus Erythematosus International Comparison. J. Rheumatol. 2000, 27, 373–376. [Google Scholar]
- Ramirez, G.A.; Canti, V.; Moiola, L.; Magnoni, M.; Rovere-Querini, P.; Coletto, L.A.; Dagna, L.; Manfredi, A.A.; Bozzolo, E.P. Performance of SLE responder index and lupus low disease activity state in real life: A prospective cohort study. Int. J. Rheum. Dis. 2019, 22, 1752–1761. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US from December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Update: Cardiac-related events during the civilian smallpox vaccination program—United States, 2003. MMWR Morb. Mortal. Wkly. Rep. 2003, 52, 492–496. [Google Scholar]
- Machado, P.M.; Lawson-Tovey, S.; Strangfeld, A.; Mateus, E.F.; Hyrich, K.L.; Gossec, L.; Carmona, L.; Rodrigues, A.; Raffeiner, B.; Duarte, C.; et al. Safety of vaccination against SARS-CoV-2 in people with rheumatic and musculoskeletal diseases: Results from the EULAR Coronavirus Vaccine (COVAX) physician-reported registry. Ann. Rheum. Dis. 2022, 81, 695–709. [Google Scholar] [CrossRef]
- Su, J.R.; McNeil, M.M.; Welsh, K.J.; Marquez, P.L.; Ng, C.; Yan, M.; Cano, M.V. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990–2018. Vaccine 2021, 39, 839–845. [Google Scholar] [CrossRef]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: Clinical observations and potential mechanisms. Nat. Rev. Cardiol. 2022, 19, 75–77. [Google Scholar] [CrossRef]
- Baumeier, C.; Aleshcheva, G.; Harms, D.; Gross, U.; Hamm, C.; Assmus, B.; Westenfeld, R.; Kelm, M.; Rammos, S.; Wenzel, P.; et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. Int. J. Mol. Sci. 2022, 23, 6940. [Google Scholar] [CrossRef]
- Huang, X.; Huang, B.; He, Y.; Feng, L.; Shi, J.; Wang, L.; Peng, J.; Chen, Y. Sars-Cov-2 Spike Protein-Induced Damage of hiPSC-Derived Cardiomyocytes. Adv. Biol. 2022, 6, e2101327. [Google Scholar] [CrossRef]
- Marrama, D.; Mahita, J.; Sette, A.; Peters, B. Lack of evidence of significant homology of SARS-CoV-2 spike sequences to myocarditis-associated antigens. EBioMedicine 2022, 75, 103807. [Google Scholar] [CrossRef]
- Dursun, A.D.; Saricam, E.; Sariyildiz, G.T.; Iscanli, M.D.; Cantekin, O.F. The Evaluation of Oxidative Stress in the Young Adults with COVID-19 mRNA Vaccines Induced Acute Pericarditis-Myopericarditis. Int. J. Gen. Med. 2022, 15, 161–167. [Google Scholar] [CrossRef]
- Tower, J.; Pomatto, L.C.D.; Davies, K.J.A. Sex differences in the response to oxidative and proteolytic stress. Redox Biol. 2020, 31, 101488. [Google Scholar] [CrossRef]
- Perl, A. Oxidative stress in the pathology and treatment of systemic lupus erythematosus. Nat. Rev. Rheumatol. 2013, 9, 674–686. [Google Scholar] [CrossRef]
- Ene, C.D.; Georgescu, S.R.; Tampa, M.; Matei, C.; Mitran, C.I.; Mitran, M.I.; Penescu, M.N.; Nicolae, I. Cellular Response against Oxidative Stress, a Novel Insight into Lupus Nephritis Pathogenesis. J. Pers. Med. 2021, 11, 693. [Google Scholar] [CrossRef]
- Ramirez, G.A.; Asperti, C.; Cucca, V.; Yacoub, M.R. Challenges to Vaccination against SARS-CoV-2 in Patients with Immune-Mediated Diseases. Vaccines 2021, 9, 1147. [Google Scholar] [CrossRef]
- Kroon, F.P.; Najm, A.; Alunno, A.; Schoones, J.W.; Landewé, R.B.; Machado, P.M.; Navarro-Compán, V. Risk and prognosis of SARS-CoV-2 infection and vaccination against SARS-CoV-2 in rheumatic and musculoskeletal diseases: A systematic literature review to inform EULAR recommendations. Ann. Rheum. Dis. 2022, 81, 422–432. [Google Scholar] [CrossRef]


{kind=link}
| Feature | Value |
|---|---|
| SLE | UCTD | MCTD: n (%) | 11 (85) | 1(8) | 1(8) |
| Females: n (%) | 7 (54) |
| Age at UCTD/MCTD/SLE onset (years): median (IQR) | 30 (25–34) |
| Age at myocarditis onset (years): median (IQR) | 37 (30–40) |
| Disease duration (years): median (IQR) | 17 (4–22) |
| General clinical features: n (%) | |
| Joint manifestations | 9 (82) |
| Mucocutaneous manifestations | 8 (64) |
| Haematological manifestations | 8 (64) |
| Lupus nephritis | 5 (36) |
| Neuropsychiatric SLE | 3 (18) |
| Serositis | 6 (45) |
| Constitutional symptoms | 4 (27) |
| Positive ADNA | 8 (64) |
| Positive antiphospholipid antibodies | 6 (45) |
| Treatment features | |
| Prednisone (any dose): n (%) | 2 (15) |
| Immunosuppressants: n (%) | 7 (54) |
| Mycophenolate mofetil | 6 (46) |
| Azathioprine | 1 (8) |
| Immunomodulants: n (%) | 8 (62) |
| Hydroxychloroquine | 7 (54) |
| Belimumab | 3 (23) |
| Before Vaccination | After Vaccination | End of Follow-Up | |
|---|---|---|---|
| Disease status | |||
| Patients in LLDAS: n (%) | 9 (82) | 8 (80) | 8 (80) |
| SLEDAI-2K: median (IQR) | 2 (0–3) | 2 (0–4) | 1 (0–2) |
| BILAG constitutional: median (IQR) | 0 (0–0) | 0 (0–1) * | 0 (0–0) |
| BILAG mucocutaneous: median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–0) |
| BILAG musculoskeletal: median (IQR) | 0 (0–0) | 0 (0–1) | 0 (0–0) |
| BILAG haematological: median (IQR) | 0 (0–1) | 1 (0–1) | 1 (0–1) |
| BILAG neuropsychiatric: median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| BILAG cardiorespiratory: median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| BILAG gastrointestinal: median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| BILAG ophthalmic: median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| BILAG renal: median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| SLICC/ACR damage index: median (IQR) | 1 (1–3) | 2 (1–3) | 2 (1–3) |
| PDN dose (mg/day): median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Laboratory Tests | Reference Range | Before Vaccination | After Dose 1 | After Dose 2 | After Vaccination | After Booster Dose |
|---|---|---|---|---|---|---|
| Timing with respect to each timepoint (days) | NA | 13 (6–20) | 17 (4–29) | NA | 7 (2–15) | |
| Laboratory test results | ||||||
| Haemoglobin (g/dL): median (IQR) | F: 12–16 M: 14–18 | 14.2 (13.3–15.1) | 13.7 (13.2–14.5) | 13.8 (13.4–14.6) ^ | 13.9 (12.9–14.4) § | 14.6 (12.2–14.9) |
| WBC/microlitre: median (IQR) | 4800–10,800 | 5100 (4400–6200) | 5350 (4175–5925) | 4450 (3593–5470) | 5145 (4150–7325) | 3690 (3300–5270) |
| Neutrophils (%): median (IQR) | 40–75 | 54 (51–60) | 61 (51–66) | 51 (47–64) | 60 (56–66) | 51 (50–54) |
| Lymphocytes (%): median (IQR) | 20–50 | 30 (28–34) | 27 (25–33) | 29 (23–37) | 22 (20–30) | 36 (33–37) |
| Monocytes (%): median (IQR) | 2–15 | 10 (7–10) | 9 (9–11) | 10 (7–10) | 10 (7–10) | 10 (10–10) |
| Eosinophils (%): median (IQR) | 1–6 | 3 (1–3) | 2 (2–3) * | 3 (1–5) * | 3 (1–5) | 2 (2–3) |
| Basophils (%): median (IQR) | 0–2 | 1 (0–1) | 0 (0–1) | 1 (0–1) | 1 (0–1) | 0 (0–1) |
| Platelets × 106/microlitre: median (IQR) | 130–400 | 237 (202–260) | 204 (139–222) | 195 (179–200) | 219 (190–258) | 229 (223–254) |
| Positive ADNA: n (%) | Negative | 5 (45) | ND | ND | 6 (60) | ND |
| Complement C3 (g/L): median (IQR) | 0.90–1.80 | 1.04 (0.95–1.09) | ND | ND | 1.02 (0.89–1.07) | ND |
| Complement C4 (g/L): median (IQR) | 0.10–0.40 | 0.18 (0.14–0.20) | ND | ND | 0.23 (0.15–0.29) | ND |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramirez, G.A.; Batani, V.; Moroni, L.; De Luca, G.; Pizzetti, G.; Sala, S.; Peretto, G.; Campochiaro, C.; Della-Torre, E.; Bozzolo, E.P.; et al. Cardiac Safety of mRNA-Based Vaccines in Patients with Systemic Lupus Erythematosus and Lupus-like Disorders with a History of Myocarditis. Pathogens 2022, 11, 1001. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11091001
Ramirez GA, Batani V, Moroni L, De Luca G, Pizzetti G, Sala S, Peretto G, Campochiaro C, Della-Torre E, Bozzolo EP, et al. Cardiac Safety of mRNA-Based Vaccines in Patients with Systemic Lupus Erythematosus and Lupus-like Disorders with a History of Myocarditis. Pathogens. 2022; 11(9):1001. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11091001
Chicago/Turabian StyleRamirez, Giuseppe A., Veronica Batani, Luca Moroni, Giacomo De Luca, Giuseppe Pizzetti, Simone Sala, Giovanni Peretto, Corrado Campochiaro, Emanuel Della-Torre, Enrica P. Bozzolo, and et al. 2022. "Cardiac Safety of mRNA-Based Vaccines in Patients with Systemic Lupus Erythematosus and Lupus-like Disorders with a History of Myocarditis" Pathogens 11, no. 9: 1001. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11091001