
Pre-Vaccination Human Papillomavirus Genotypes and HPV16 Variants among Women Aged 25 Years or Less with Cervical Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
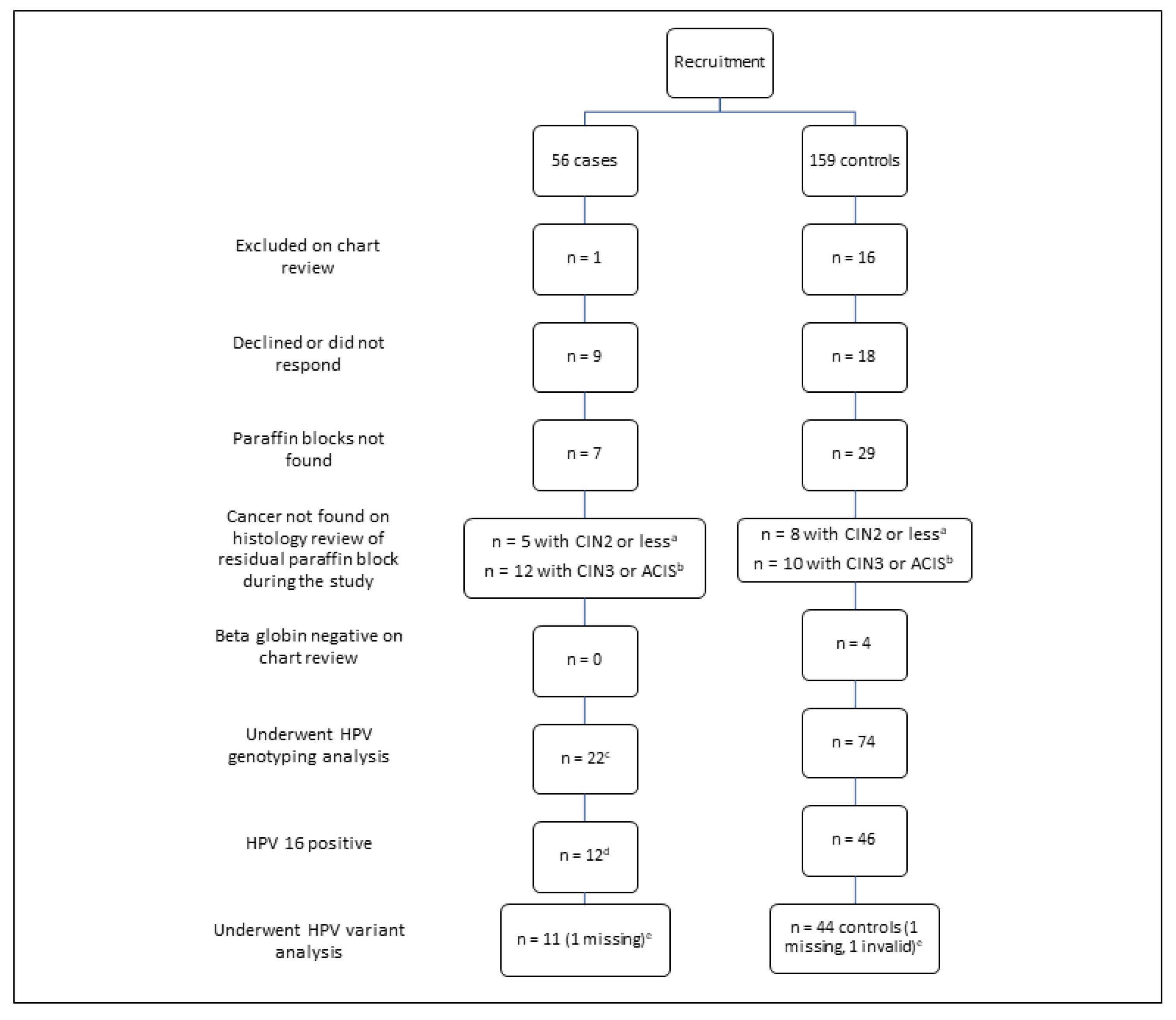
3.1. Recruitment and Demographic Information
3.2. HPV Genotyping Results
3.3. Multiple HPV Infections
3.4. HPV16 Variant Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Council Australia Cervical Cancer Screening Guidelines Working Party. National Cervical Screening Program: Guidelines for the Management of Screen-Detected Abnormalities, Screening in Specific Populations and Investigation of Abnormal Vaginal Bleeding; Cancer Council Australia Cervical Cancer Screening Guidelines Working Party: Sydney, Australia, 2016. [Google Scholar]
- Yap, D.; Liang, X.; Garland, S.M.; Hartley, S.; Gorelik, A.; Ogilvie, G.; Ogilvie, G.; Tan, J.; Wrede, C.D.H.; Jayasinghe, Y. Clinicians’ attitude towards changes in Australian National Cervical Screening Program. J. Clin. Virol. 2016, 76 (Suppl. 1), S81–S87. [Google Scholar] [CrossRef]
- Jayasinghe, Y.; Rangiah, C.; Gorelik, A.; Ogilvie, G.; Wark, J.D.; Hartley, S.; Garland, S.M. Primary HPV DNA based cervical cancer screening at 25 years: Views of young Australian women aged 16–28 years. J. Clin. Virol. 2016, 76 (Suppl. 1), S74–S80. [Google Scholar] [CrossRef] [PubMed]
- Denham, O.; Garland, S.M.; Gorelik AOgilvie, G.; Tan, J.; Mazza, D.; Wrede, D.; McBride, B.; Jayasinghe, Y. Attitudes to changes in cervical screening guidelines: Preliminary views of Australian general practitioners and nurse practitioners. J. Fam. Med. Dis. Prev. 2016, 2, 041. [Google Scholar] [CrossRef]
- Obermair, H.M.; Bennett, K.F.; Brotherton, J.M.L.; Smith, M.A.; McCaffery, K.J.; Dodd, R.H. Australian National Cervical Screening Program renewal: Attitudes and experiences of general practitioners, and obstetricians and gynaecologists. Aust. N. Z. J. Obstet. Gynaecol. 2021, 61, 416–423. [Google Scholar] [CrossRef] [PubMed]
- US Preventive Services Task, Force; Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; et al. Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement. J. Am. Med. Assoc. 2018, 320, 674–686. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, N.M.; Brennan, L.P.; Claure, L.; Balian, L.N.; Kasting, M.L.; Champion, V.L.; Forman, M.R. Clinician practices, knowledge, and attitudes regarding primary human papillomavirus testing for cervical cancer screening: A mixed-methods study in Indiana. Prev. Med. Rep. 2022, 31, 102070. [Google Scholar] [CrossRef]
- Lee, Y.W.; Morgan, J.R.; Fiascone, S.; Perkins, R.B. Underscreenng, overscreening, and guideline-adherent cervical cancer screening in a national cohort. Gynecol. Oncol. 2022, 167, 181–188. [Google Scholar] [CrossRef]
- de Villiers, E.M.; Fauquet, C.; Broker, T.R.; Bernard, H.U.; zur Hausen, H. Classification of papillomaviruses. Virology 2004, 324, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A review of human carcinogens—Part B: Biological agents. Lancet Oncol. 2009, 10, 321–322. [Google Scholar] [CrossRef]
- De Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Muñoz, N.; Bosch, F.X.; De Sanjosé, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.; Meijer, C.J. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, T.; Manos, M.M.; Peto, J.; Greer, C.E.; Munoz, N.; Bosch, F.X.; Wheeler, C.M. Human papillomavirus type 16 sequence variation in cervical cancers: A worldwide perspective. J. Virol. 1997, 71, 2463–2472. [Google Scholar] [CrossRef] [Green Version]
- Burke, R.; Harari, A.; Chen, Z. Human papillomavirus genome variants. Virology 2013, 445, 232–243. [Google Scholar] [CrossRef] [Green Version]
- Barbaro, B.; Brotherton, J.M. Assessing HPV vaccine coverage in Australia by geography and socioeconomic status: Are we protecting those most at risk? Aust. N. Z. J. Public Health 2014, 38, 419–423. [Google Scholar] [CrossRef]
- United Stated Food and Drug Administration. Gardasil 9 2018. Available online: https://www.fda.gov/biologicsbloodvaccines/vaccines/approvedproducts/ucm426445.htm (accessed on 1 September 2018).
- National HPV Vaccination Register. Australia Moves to Two Dose Nine Valent HPV Vaccine in 2018. Available online: http://www.hpvregister.org.au/health-professionals/announcements/Australia (accessed on 1 September 2019).
- National Cancer Control Indicators. HPV Vaccination Update. Available online: https://ncci.canceraustralia.gov.au/prevention/hpv-vaccination-uptake/hpv-vaccination-uptake (accessed on 20 December 2022).
- Zhai, L.; Tumban, E. Gardasil-9: A global survey of projected efficacy. Antivir. Res. 2016, 130, 101–109. [Google Scholar] [CrossRef]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 3.0) [Computer Software]. Social Psychology Network. 2011. Available online: http://www.randomizer.org/ (accessed on 1 October 2007).
- World Health Organization. WHO International Classification of Diseases 10 Online; WHO: Geneva, Switzerland, 2007; Available online: http://www.who.int/classifications/icd/en/ (accessed on 1 July 2009).
- SEIFA Postal Areas Data Cube. 2006 [Internet]. Australian Bureau of Statistics. 2006. Available online: http://www.abs.gov.au/ausstats/[email protected]/mf/2033.0.55.001/ (accessed on 1 November 2010).
- Garland, S.M.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Harper, D.M.; Leodolter, S.; Tang, G.W.; Ferris, D.G.; Steben, M.; Bryan, J.; et al. Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N. Engl. J. Med. 2007, 356, 1928–1943. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.E.; Garland, S.M.; Rumbold, A.R.; Tabrizi, S.N. Human papillomavirus genotyping using archival vulvaldysplastic or neoplastic biopsy tissues:comparison between the INNO-LiPA and lineararray assays. J. Clin. Microbiol. 2010, 48, 1458–1460. [Google Scholar] [CrossRef] [Green Version]
- Cornall, A.M.; Brotherton, J.M.L.; Callegari, E.T.; Tan, F.H.; Saville, M.; Pyman, J.; Phillips, S.; Malloy, M.J.; Tabrizi, S.N.; Garland, S.M.; et al. Assessment of attribution algorithms for resolving CIN3-related HPV genotype prevalence in mixed-genotype biopsy specimens using laser capture microdissection as the reference standard. Vaccine 2020, 38, 6312–6319. [Google Scholar] [CrossRef]
- Chan, S.Y.; Ho, L.I.S.A.; Ong, C.K.; Chow, V.I.N.C.E.N.T.; Drescher, B.E.R.N.D.; Dürst, M.; Ter Meulen, J.; Villa, L.; Luande, J.; Mgaya, H.N. Molecular variants of human papillomavirus type 16 from four continents suggest ancient pandemic spread of the virus and its coevolution with humankind. J. Virol. 1992, 66, 2057–2066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, L.; Chan, S.Y.; Burk, R.D.; Das, B.C.; Fujinaga, K.; Icenogle, J.P.; Kahn, T.; Kiviat, N.; Lancaster, W.; Mavromara-Nazos, P. The genetic drift of human papillomavirus type 16 is a means of reconstructing prehistoric viral spread and the movement of ancient human populations. J. Virol. 1993, 67, 6413–6423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, T.; Wheeler, C.M.; Halpern, A.L.; Stewart, A.C.; Hildesheim, A.; Jenison, S.A. Human papillomavirus type 16 variant lineages in United States populations characterized by nucleotide sequence analysis of the E6, L2, and L1 coding segments. J. Virol. 1995, 69, 7743–7753. [Google Scholar] [CrossRef] [Green Version]
- Brotherton, J.M.L.; Tabrizi, S.N.; Phillips, S.; Pyman, J.; Cornall, A.M.; Lambie, N.; Anderson, L.; Cummings, M.; Payton, D.; Scurry, J.P.; et al. Looking beyond human papillomavirus (HPV) genotype 16 and 18: Defining HPV genotype distribution in cervical cancers in Australia prior to vaccination. Int. J. Cancer 2017, 141, 1576–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagström, S.; van der Weele, P.; Rounge, T.B.; Christiansen, I.K.; King, A.J.; Ambur, O.H. HPV16 whole genome minority variants in persistent infections from young Dutch women. J. Clin. Virol. 2019, 119, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Totaro, M.E.; Gili, J.A.; Liotta, D.J.; Schurr, T.G.; Picconi, M.A.; Badano, I. Genetic variation in the E6 and E7 genes of human papillomavirus type 16 in northeastern Argentina. J. Med. Virol. 2022, 94, 745–751. [Google Scholar] [CrossRef]
- Jayasinghe, Y.; Sasongko, S.; Lim, W.; Grover, S.R.; Tabrizi, S.N.; Moore, E.E.; Donath Garland, S.M.; for the Early-onset Cervical Cancer (EOCC) Study Group. The association between unwanted sexual experiences and early-onset cervical cancer and precancer by age 25 years or less: A case control study. J. Women’s Health 2017, 26, 774–787. [Google Scholar] [CrossRef] [PubMed]
- Quint, W.; Jenkins, D.; Molijn, A.; Struijk, L.; van de Sandt, M.; Doorbar, J.; Mols, J.; Van Hoof, C.; Hardt, K.; Struyf, F.; et al. One virus, one lesion--individual components of CIN lesions contain a specific HPV type. J. Pathol. 2012, 227, 62–71. [Google Scholar] [CrossRef]
- Kalantari, M.; Garcia-Carranca, A.; Morales-Vazquez, C.D.; Zuna, R.; Montiel, D.P.; Calleja-Macias, I.E.; Johansson, B.; Andersson, S.; Bernard, H.U. Laser capture microdissection of cervical human papillomavirus infections: Copy number of the virus in cancerous and normal tissue and heterogeneous DNA methylation. Virology 2009, 390, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Stevens, M.P.; Tabrizi, S.N.; Quinn, M.A.; Garland, S.M. Human papillomavirus genotype prevalence in cervical biopsies from women diagnosed with cervical intraepithelial neoplasia or cervical cancer in Melbourne, Australia. Int. J. Gynecol. Cancer 2006, 16, 1017–1024. [Google Scholar] [CrossRef]
- Ong, C.K.; Chan, S.Y.; Campo, M.S.; Fujinaga, K.; Mavromara-Nazos, P.; Labropoulou, V.; Pfister, H.; Tay, S.K.; Ter Meulen, J.; Villa, L.L. Evolution of human papillomavirus type 18: An ancient phylogenetic root in Africa intratype diversity reflect coevolution with human ethnic groups. J. Virol. 1993, 67, 6424–6431. [Google Scholar] [CrossRef] [Green Version]
- Pastrana, D.V.; Vass, W.C.; Lowy, D.R.; Schiller, J.T. NHPV16 VLP vaccine induces human antibodies that neutralize divergent variants of HPV16. Virology 2001, 279, 361–369. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Year | General Diagnosis Code | Specific Diagnosis Code |
|---|---|---|
| 1983–June 1998 | 180 Malignant Neoplasm of Cervix Uteri | 180.0 Endo Cervix |
| 180.1 Exocervix | ||
| 180.8 Other specified sites of cervix | ||
| 180.9 Cervix Uteri, unspecified | ||
| July 1998–2007 | C53 Malignant Neoplasm of Cervix Uteri | C53.0 Endo Cervix |
| C53.1 Exocervix | ||
| C53.8 Overlapping lesion of cervix uteri | ||
| C53.9 Cervix Uteri, unspecified |
| Gene | Primer Pair | Nucleotide Position Change | Amplicon Length (Base Pairs) |
|---|---|---|---|
| L1 | 5′-GTTGATACTACACGCAGTAC-3′ | 6695:6721:6803 | 169 |
| 5′-ATGTCATAACGTCTGCAGTT-3′ | |||
| E2 | 5′-GCAGTTTGATGGAGACATATGC-3′ | 3159:3161:3181:3182 | 110 |
| 5′-CATAATAGTCAACTTGACCCTCT-3′ | |||
| E6 | 5′-TGCAATGTTTCAGGACCCACA-3′ | 131:132:143:145:178 | 118 |
| 5′-AGTAACTGTTGCTTGCAGTAC-3′ | |||
| E6 T350G | 5′-GAATCCATATGCTGTATGTGAT-3′ | 350 | 102 |
| Case (≤25 Years) n = 22 | Controls (>25 Years) n = 78 | p Value, (χ2) OR [95%CI] | |
|---|---|---|---|
| Deceased status n (%) | 6 (27.3) | 52 (66.7) | <0.001. 0.2 [0.1–0.6] |
| Median age at diagnosis (years) | 24.0 | 50.5 | <0.001(rank-sum) |
| Interquartile range (IQR) | 22–25 | 40–64 | |
| Total range | 18–25 | 26–92 | |
| Ethnicity n% | 20 (90.1) | 67 (85.9) | 0.83 |
| Caucasian | 1 (4.5) | 6 (7.7) | |
| Aboriginal, Torres Strait Islander | 1 (4.6) | 3 (3.9) | |
| Asian | 0 (0.0) | 2 (2.6) | |
| Other | |||
| Median SEIFA decile a | 7.5 | 6.5 | |
| IQR | 5–9 | 4–8 | |
| range | 1–10 | 1–10 | |
| Total | 22 (100) | 78 (100) |
| HPV Type | Cases n (%) | SCC a | AC b | Other c | NE d | Controls n (%) | SCC a | AC b | Other c | UD e | Total n (%) | p Value, OR [95%CI] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 16 | 12 (54.5) | 9 (75.0) | 2 (40.0) | 0 | 1 (25.0) | 46 (66.7) | 37 (72.6) | 6 (54.6) | 2 (40.0) | 1 (50.0) | 58 (63.7) | 0.30, 0.6, [0.2–1.8] f |
| 18 | 8 (36.3) | 1 (8.3) | 3 (60.0) | 1 (100.0) | 3 (75.0) | 12 (17.3) | 6 (11.8) | 3 (27.3) | 2 (40.0) | 1 (40.0) | 20 (22.0) | 0.06, 2.7, [0.8–8.9] g |
| 31 | 0 (0.0) | 0 | 0 | 0 | 0 | 1 (1.4) | 1 (32.0) | 0 | 0 | 0 | 1 (1.1) | |
| 33 | 1 (4.5) | 1 (8.3) | 0 | 0 | 0 | 3 (4.3) | 2 (3.9) | 0 | 1 (20.0) | 0 | 4 (4.4) | |
| 39 | 0 (0.0) | 0 | 0 | 0 | 0 | 2 (2.9) | 2 (3.9) | 0 | 0 | 0 | 2 (2.2) | |
| 45 | 1 (4.5) | 1 (8.3) | 0 | 0 | 0 | 2 (2.9) | 1 (2.0) | 1 (9.1) | 0 | 0 | 3 (3.3) | |
| 51 | 0 (0.0) | 0 | 0 | 0 | 0 | 1 (1.4) | 1 (2.0 | 0 | 0 | 0 | 1 (1.1) | |
| 52 | 0 (0.0) | 0 | 0 | 0 | 0 | 1 (1.4) | 1 (2.0) | 0 | 0 | 0 | 1 (1.1) | |
| 58 | 0 (0.0) | 0 | 0 | 0 | 0 | 1 (1.4) | 0 | 1 (9.1) | 0 | 0 | 1 (1.1) | |
| Total | 22 (100.0) | 12 (54.6) | 5 (22.7) | 1 (4.6) | 4 (18.2) | 69 (100.0) | 51 (84.1) | 11 (15.9) | 5 (7.2) | 2 (2.0) | 91 (100.0) |
| Subject | Histological Diagnosis | Stage | Specimen | Histology in Block Tested | Year of Diagnosis | HPV Type | HPV Type |
|---|---|---|---|---|---|---|---|
| Case | mucoepidermoid | IB NOS a | HPV DNA bank | Not applicable | 1984 | 18 b | 51 |
| Control | SCC | IB NOS a | Paraffin | cancer | 2000 | 16 c | 52 |
| Control | adenosquamous | IIA | Paraffin | cancer | 1988 | 16 c | 52 |
| Control | SCC | IBI | Paraffin | cancer | 2003 | 51 d | 82 |
| Control | SCC | IIB | Paraffin | cancer | 1994 | 16 c | 45 |
| Control | SCC | IAI | Paraffin | cancer | 2001 | 16 c | 45 |
| Control | SCC | IIIB | 2 Paraffin blocks | cancer | 1987 | 16 c | 52 |
| Control | SCC | IIIB | Paraffin | cancer | 2005 | 16 c | 18 |
| HPV Gene | SNPs | Case | Control | Amino Acid Change |
|---|---|---|---|---|
| L1 | n = 6 | n = 23 | ||
| AAc-C6695 | 1 | 3 | Thr to Pro (T 353P) | |
| AAc-A6721 | 1 | 3 | No base change | |
| subtotal | 2 | 6 | ||
| E2 | n = 10 | n = 38 | ||
| AA-G3159 | 2 | Thr to Arg (T 135 R) | ||
| AA-A3159 | 1 | 2 | Thr to Lys (T 135 K) | |
| AA-T3161 | 1 | 2 | His to Tyr (H 136 Y) | |
| AA-C3181 | 2 | Glu to Asp (E 142D) | ||
| AA-A3182 | 1 | 4 | Ala to Thr (A 143 T) | |
| subtotal | 3 | 12 | ||
| E6 | n = 10 | n = 41 | ||
| E-G131 | 3 | Arg to Gly (R 10 G) | ||
| AA-T145 | 1 | 5 | Gln to His (Q 14 H) | |
| E-C154 | 1 | No base change | ||
| E-G162 | 1 | Gln to Arg (Q 20R) | ||
| E-A176 | 1 | Asp to Asn (D 25 N) | ||
| As-G178 | 1 | Asp to Glu (D 25 E) | ||
| AA-G183 | 1 | Ile to Arg (L 27 R) | ||
| subtotal | 4 | 10 | ||
| E6 350 region | n = 9 | n = 38 | ||
| AA-T335 | 2 | His to Tyr (H 78 Y) | ||
| E-G350 | 3 | 14 | Leu to Val (L 83V) | |
| As-G350 | 1 | Leu to Val (L 83V) | ||
| AA-G350 | 4 | Leu to Val (L 83V) | ||
| subtotal | 3 | 21 | ||
| Total SNPs | Total SNPs | 12 | 49 |
| Variant Class | Case n (%) | Control n (%) | Total n (%) | p Value, OR [95%CI] |
|---|---|---|---|---|
| European | 10 (91.9) | 38 (86.3) | 48 (87.3) | 0.7(χ2), 1.6, [0.6–79.8] |
| Asian American | 1 (9.1) | 5 (11.4) | 6 (10.9) | 0.8 (χ2), 0.8, [0.0–8.3] |
| Asian | 0 (0.0) | 1 (2.3) | 1 (1.8) | |
| Total | 11 (100.0) | 44 (100.0) | 55 (100.0) |
| Morphology | European Variant n (%) | Asian American Variant n (%) | Asian Variant n (%) | Total |
|---|---|---|---|---|
| SCC a | 40 (90.9) | 3 (6.8) | 1 (2.3) | 44 |
| AC b | 6 (75.0) | 2 (25.0) | 0 (0.0) | 8 |
| Other epithelial c | 1(50.0) | 1 (50.0) | 0 (0.0) | 2 |
| NE d | 1(100.0) | 0 (0.0) | 0 (0.0) | 1 |
| Total | 48 (87.3) | 6 (10.9) | 1 (1.8) | 55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jayasinghe, Y.L.; Tabrizi, S.N.; Stevens, M.; Leong, T.Y.-M.; Pyman, J.; Grover, S.R.; Garland, S.M.; the Early-Onset Cervical Cancer (EOCC) Study Group. Pre-Vaccination Human Papillomavirus Genotypes and HPV16 Variants among Women Aged 25 Years or Less with Cervical Cancer. Pathogens 2023, 12, 451. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030451
Jayasinghe YL, Tabrizi SN, Stevens M, Leong TY-M, Pyman J, Grover SR, Garland SM, the Early-Onset Cervical Cancer (EOCC) Study Group. Pre-Vaccination Human Papillomavirus Genotypes and HPV16 Variants among Women Aged 25 Years or Less with Cervical Cancer. Pathogens. 2023; 12(3):451. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030451
Chicago/Turabian StyleJayasinghe, Yasmin L., Sepehr N. Tabrizi, Matthew Stevens, Trishe Y-M. Leong, Jan Pyman, Sonia R. Grover, Suzanne M. Garland, and the Early-Onset Cervical Cancer (EOCC) Study Group. 2023. "Pre-Vaccination Human Papillomavirus Genotypes and HPV16 Variants among Women Aged 25 Years or Less with Cervical Cancer" Pathogens 12, no. 3: 451. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030451