
Hepatitis E Virus (HEV) Infection in Hemodialysis Patients: A Multicenter Epidemiological Cohort Study in North-Eastern Greece

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Recruitment and Ethics
2.2. Samples’ Processing
2.3. Elisa Qualitative Anti-HEV IgG Detection
2.4. Quantitative RT-PCR for HEV RNA
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khuroo, M.S.; Khuroo, M.S. Hepatitis E: Discovery, global impact, control and cure. World J. Gastroenterol. 2016, 22, 7030–7045. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Casares, P.; Ramos-Romero, C.; Ramirez-Gonzalez, E.; Mas, A. Hepatitis E Virus in Industrialized Countries: The Silent Threat. BioMed Res. Int. 2016, 2016, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, S.; Teng, J.L.L.; Chiu, T.-H.; Lau, S.K.P.; Woo, P.C.Y. Hepatitis E Virus Genotypes and Evolution: Emergence of Camel Hepatitis E Variants. Int. J. Mol. Sci. 2017, 18, 869. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Simmonds, P. Classification and Genomic Diversity of Enterically Transmitted Hepatitis Viruses. Cold Spring Harb. Perspect. Med. 2018, 8, a031880. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Gracia, M.T.; García, M.; Suay, B.; Mateos-Lindemann, M.L. Current Knowledge on Hepatitis E. J. Clin. Transl. Hepatol. 2015, 3, 117–126. [Google Scholar] [PubMed]
- Wu, X.; Chen, P.; Lin, H.; Hao, X.; Liang, Z. Hepatitis E virus: Current epidemiology and vaccine. Hum. Vaccines Immunother. 2016, 12, 2603–2610. [Google Scholar] [CrossRef]
- Kamar, N.; Garrouste, C.; Haagsma, E.B.; Garrigue, V.; Pischke, S.; Chauvet, C.; Dumortier, J.; Cannesson, A.; Cassuto–Viguier, E.; Thervet, E.; et al. Factors Associated with Chronic Hepatitis in Patients With Hepatitis E Virus Infection Who Have Received Solid Organ Transplants. Gastroenterology 2011, 140, 1481–1489. [Google Scholar]
- Tavakoli, A.; Alavian, S.M.; Moghoofei, M.; Mostafaei, S.; Abbasi, S.; Farahmand, M. Seroepidemiology of hepatitis E virus infection in patients undergoing maintenance hemodialysis: Systematic review and meta-analysis. Ther. Apher. Dial. 2020, 25, 4–15. [Google Scholar] [CrossRef]
- Sylvan, S.P.E.; Jacobson, S.H.; Christenson, B. Prevalence of antibodies to hepatitis E virus among hemodialysis patients in Sweden. J. Med. Virol. 1998, 54, 38–43. [Google Scholar] [CrossRef]
- Shrestha, A.C.; Flower, R.L. A Comparative Study of Assay Performance of Commercial Hepatitis E Virus Enzyme-Linked Im-munosorbent Assay Kits in Australian Blood Donor Samples. J. Blood Transfus. 2016, 2016, 9647675. [Google Scholar] [CrossRef]
- Psichogiou, M.; Vaindirli, E.; Tzala, E.; Voudiclari, S.; Boletis, J.; Vosnidis, G.; Moutafis, S.; Skoutelis, G.; Hadjiconstantinou, V.; Troonen, H.; et al. Hepatitis E virus (HEV) infection in haemodialysis patients. The Multicentre Haemodialysis Cohort Study on Viral Hepatitis. Nephrol. Dial. Transplant. 1996, 11, 1093–1095. [Google Scholar] [CrossRef] [PubMed]
- Dalekos, G.N.; Zervou, E. Antibodies to hepatitis E virus among several populations in Greece: Increased prevalence in an he-modialysis unit. Transfusion 1998, 38, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Stefanidis, I.; Zervou, E.; Rizos, C.; Syrganis, C.; Patsidis, E.; Kyriakopoulos, G.; Sdrakas, L.; Tsianas, N.; Rigopoulou, E.; Liakopoulos, V.; et al. Hepatitis E Virus Antibodies in Hemodialysis Patients: An Epidemiological Survey in Central Greece. Int. J. Artif. Organs 2004, 27, 842–847. [Google Scholar] [CrossRef]
- Bendall, R.; Ellis, V. A comparison of two commercially available anti-HEV IgG kits and a re-evaluation of anti-HEV IgG sero-prevalence data in developed countries. J. Med. Virol. 2010, 82, 799–805. [Google Scholar] [CrossRef]
- Park, H.K.; Jeong, S.-H.; Kim, J.-W.; Woo, B.-H.; Lee, D.H.; Kim, H.Y.; Ahn, S. Seroprevalence of anti-hepatitis E virus (HEV) in a Korean population: Comparison of two commercial anti-HEV assays. BMC Infect. Dis. 2012, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, T.; Diekmann, J.; Eberhardt, M.; Knabbe, C.; Dreier, J. Monitoring of Anti-Hepatitis E Virus Antibody Seroconversion in Asymptomatically Infected Blood Donors: Systematic Comparison of Nine Commercial Anti-HEV IgM and IgG Assays. Viruses 2016, 8, 232. [Google Scholar] [PubMed]
- Mansuy, J.M.; Gallian, P.; Dimeglio, C.; Saune, K.; Arnaud, C.; Pelletier, B.; Morel, P.; Legrand, D.; Tiberghien, P.; Izopet, J. A nationwide survey of hepatitis E viral infection in French blood donors. Hepatology 2016, 63, 1145–1154. [Google Scholar] [CrossRef]
- Mrzljak, A.; Dinjar-Kujundzic, P.; Knotek, M.; Kudumija, B.; Ilic, M.; Gulin, M.; Zibar, L.; Hrstic, I.; Jurekovic, Z.; Kolaric, B.; et al. Seroepidemiology of hepatitis E in patients on haemodialysis in Croatia. Int. Urol. Nephrol. 2020, 52, 371–378. [Google Scholar] [CrossRef]
- Uçar, E.; Cetin, M. Hatay’da hemodiyaliz tedavisi alan hastalarda hepatit e virus seropozitifliği [Hepatitis E virus seropositivity in hemodialysis patients in Hatay province, Turkey]. Mikrobiyol. Bul. 2009, 43, 299–302. [Google Scholar]
- Faber, M.; Askar, M.; Stark, K. Case-control study on risk factors for acute hepatitis E in Germany, 2012 to 2014. Eurosurveillance 2018, 23, 17–00469. [Google Scholar] [CrossRef]
- Baumann-Popczyk, A.; Popczyk, B.; Gołąb, E.; Rożej-Bielicka, W.; Sadkowska-Todys, M. A cross-sectional study among Polish hunters: Seroprevalence of hepatitis E and the analysis of factors contributing to HEV infections. Med Microbiol. Immunol. 2017, 206, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Monini, M.; Ostanello, F.; Dominicis, A.; Tagliapietra, V.; Vaccari, G.; Rizzoli, A.; Trombetta, C.M.; Montomoli, E.; Di Bartolo, I. Seroprevalence of Hepatitis E Virus in Forestry Workers from Trentino-Alto Adige Region (Northern Italy). Pathogens 2020, 9, 568. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, A.; Chaussade, H.; Rigaud, E.; Rodriguez, J.; Berthault, C.; Boué, F.; Tognon, M.; Touzé, A.; Garcia-Bonnet, N.; Choutet, P.; et al. High Hepatitis E Virus Seroprevalence in Forestry Workers and in Wild Boars in France. J. Clin. Microbiol. 2012, 50, 2888–2893. [Google Scholar] [CrossRef] [PubMed]
- Markakis, G.E.; Papatheodoridis, G.V.; Cholongitas, E. Epidemiology and treatment of hepatitis E in the liver transplantation setting: A literature review. J. Viral Hepat. 2022, 29, 698–718. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Naik, S. Epidemiology of hepatitis E: Current status. J. Gastroenterol. Hepatol. 2009, 24, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- Mrzljak, A.; Jemersic, L.; Savic, V.; Balen, I.; Ilic, M.; Jurekovic, Z.; Pavicic-Saric, J.; Mikulic, D.; Vilibic-Cavlek, T. Hepatitis E Virus in Croatia in the “One-Health” Context. Pathogens 2021, 10, 699. [Google Scholar] [CrossRef]
- Behzadifar, M.; Lankarani, K.B. Seroprevalence of Hepatitis E Virus in Iran: A Systematic Review and Meta-analysis. Middle East J. Dig. Dis. 2016, 8, 189–200. [Google Scholar] [CrossRef]
- Jelicic, P.; Ferenc, T.; Mrzljak, A.; Jemersic, L.; Janev-Holcer, N.; Milosevic, M.; Bogdanic, M.; Barbic, L.; Kolaric, B.; Stevanovic, V.; et al. Insights into hepatitis E virus epidemiology in Croatia. World J. Gastroenterol. 2022, 28, 5494–5505. [Google Scholar] [CrossRef]
- Ouji, M.; Taherkhani, R.; Farshadpour, F. High prevalence of hepatitis E among regular hemodialysis patients in South of Iran. Int. J. Artif. Organs 2021, 44, 658–663. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Mean (SD) †, N (%) ‡ | Anti-HEV IgG (+); n = 42 (%) | Anti-HEV IgG (−); n = 363 (%) | Univariate Analysis p-Value | Multivariate Analysis OR; ±95%CI ⁋ | Multivariate Analysis p-Value ⁋ |
|---|---|---|---|---|---|---|
| Age | ||||||
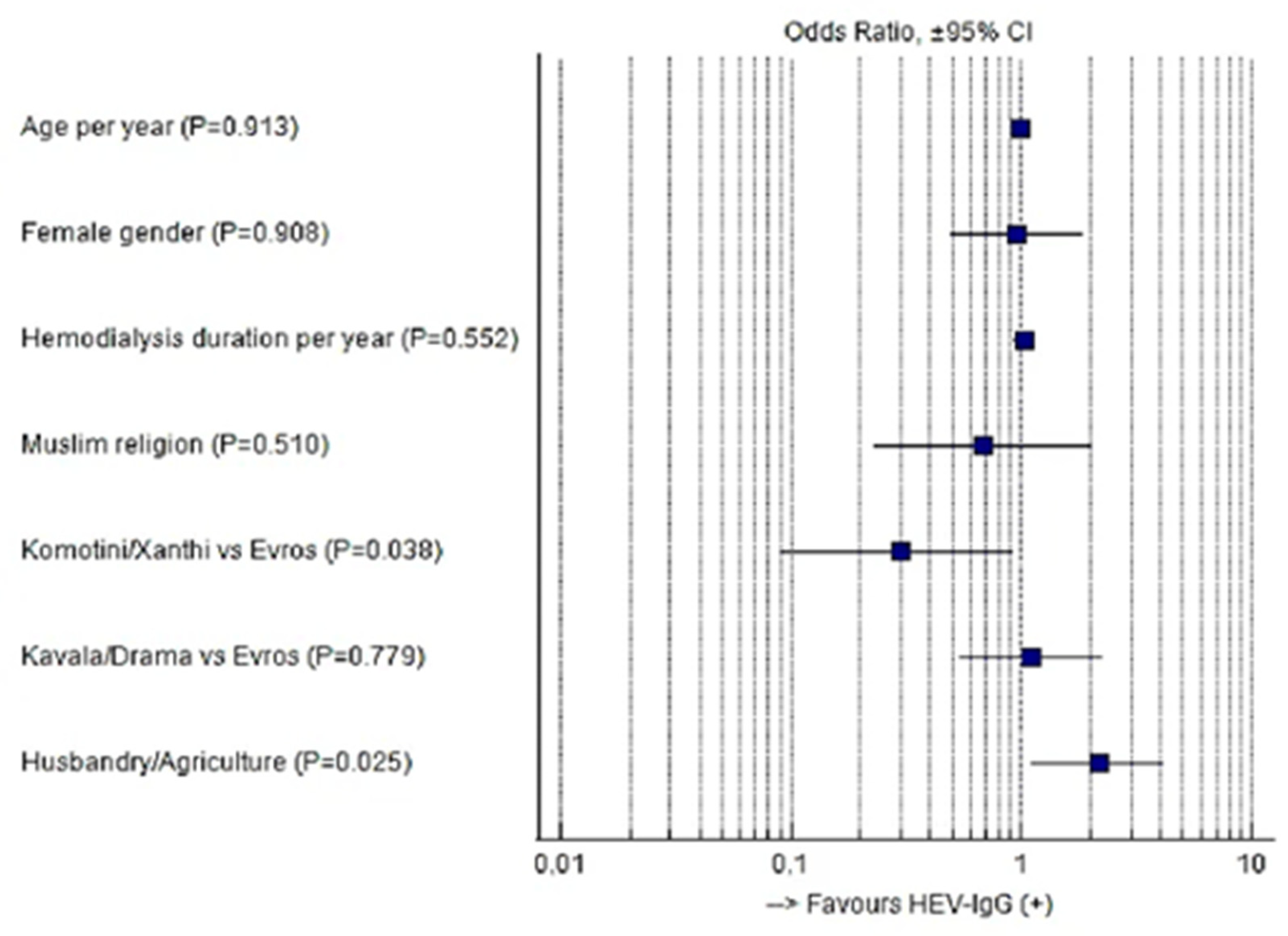
| Mean (SD) | 67.1 ± 13.6 | 66.1 ± 11.9 | 67.2 ± 13.8 | 0.641 | 0.999 (0.974–1.023) | 0.913 |
| Gender | ||||||
| Males | 250 (62.7) | 26 (61.9) | 224 (61.7) | 0.980 | 1.000 | |
| Females | 155 (37.3) | 16 (38.1) | 139 (38.3) | 0.961 (0.490–1.883) | 0.908 | |
| Hemodialysis duration * | ||||||
| Mean (SD) | 5.75 ± 3.56 | 6.14 ± 3.66 | 5.71 ± 3.56 | 0.452 | 1.027 (0.941–1.121) | 0.552 |
| Religion | ||||||
| Christians | 327 (80.7) | 36 (85.7) | 291 (80.2) | 0.388 | 1.000 | |
| Muslims | 78 (19.3) | 6 (14.3) | 72 (19.8) | 0.694 (0.234–2.059) | 0.510 | |
| Residence | ||||||
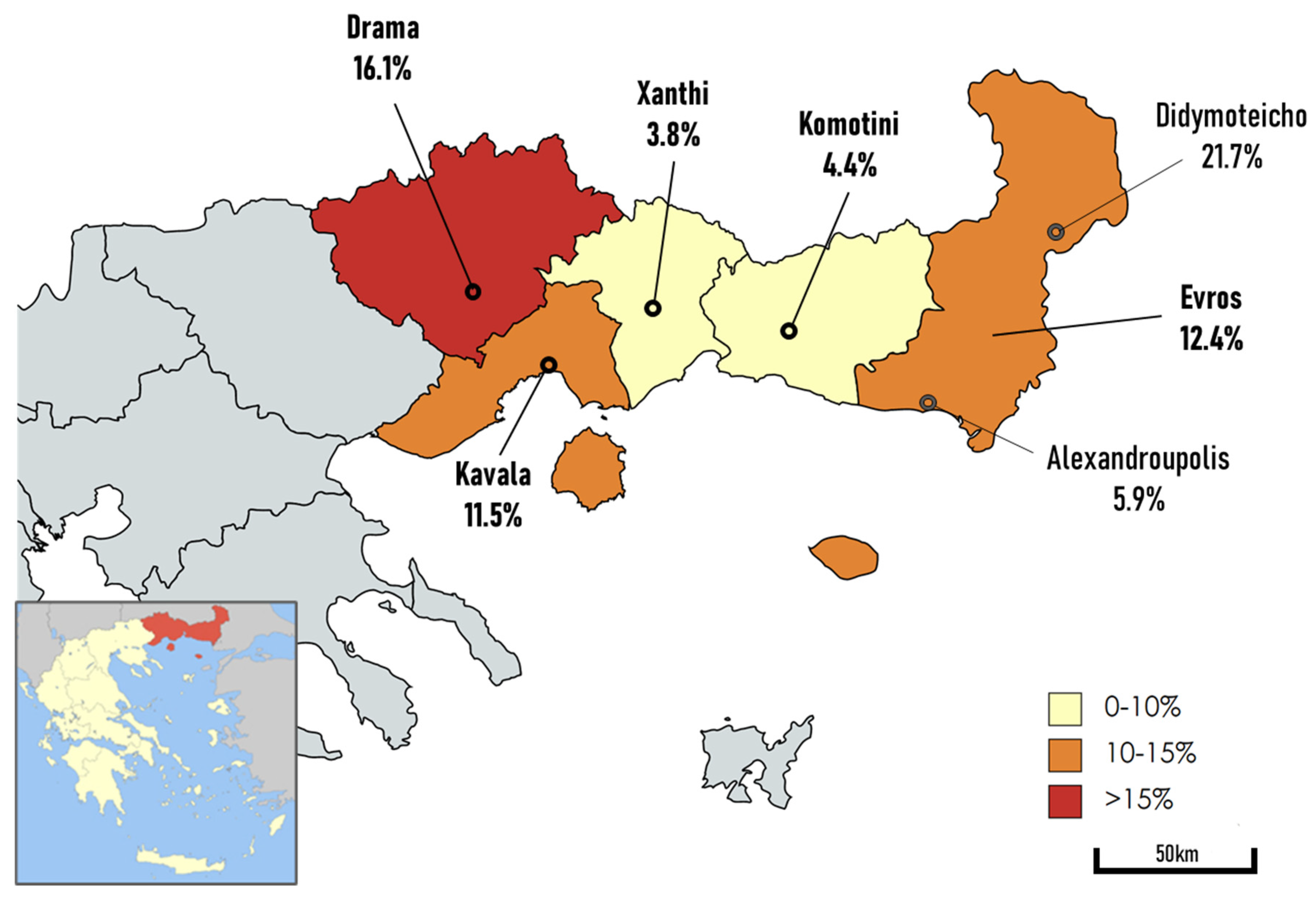
| Evros (Alexandroupolis/Didymoteicho) | 145 (35.8) | 18 (42.9) | 127 (35.0) | 0.028 | 1.000 | |
| Komotini/Xanthi | 120 (29.6) | 5 (11.9) | 115 (31.7) | 0.296 (0.094–0.936) | 0.038 | |
| Kavala/Drama | 140 (34.6) | 19 (45.2) | 121 (33.3) | 1.107 (0.543–2.260) | 0.779 | |
| Husbandry/Agriculture | ||||||
| No | 302 (74.6) | 24 (57.1) | 278 (76.6) | 0.006 | 1.000 | |
| Yes | 103 (25.4) | 18 (42.9) | 85 (23.4) | 2.155 (1.102–4.214) | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kogias, D.; Skeva, A.; Smyrlis, A.; Mourvati, E.; Kantartzi, K.; Romanidou, G.; Kalientzidou, M.; Rekari, V.; Konstantinidou, E.; Kiorteve, P.; et al. Hepatitis E Virus (HEV) Infection in Hemodialysis Patients: A Multicenter Epidemiological Cohort Study in North-Eastern Greece. Pathogens 2023, 12, 667. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12050667
Kogias D, Skeva A, Smyrlis A, Mourvati E, Kantartzi K, Romanidou G, Kalientzidou M, Rekari V, Konstantinidou E, Kiorteve P, et al. Hepatitis E Virus (HEV) Infection in Hemodialysis Patients: A Multicenter Epidemiological Cohort Study in North-Eastern Greece. Pathogens. 2023; 12(5):667. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12050667
Chicago/Turabian StyleKogias, Dionysios, Aikaterini Skeva, Andreas Smyrlis, Efthymia Mourvati, Konstantinia Kantartzi, Gioulia Romanidou, Maria Kalientzidou, Vasiliki Rekari, Eleni Konstantinidou, Parthena Kiorteve, and et al. 2023. "Hepatitis E Virus (HEV) Infection in Hemodialysis Patients: A Multicenter Epidemiological Cohort Study in North-Eastern Greece" Pathogens 12, no. 5: 667. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12050667