
Epidemiological Data and Antimicrobial Resistance of Campylobacter spp. in Portugal from 13 Years of Surveillance
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analyses
3. Results
3.1. Data from the Surveillance Network
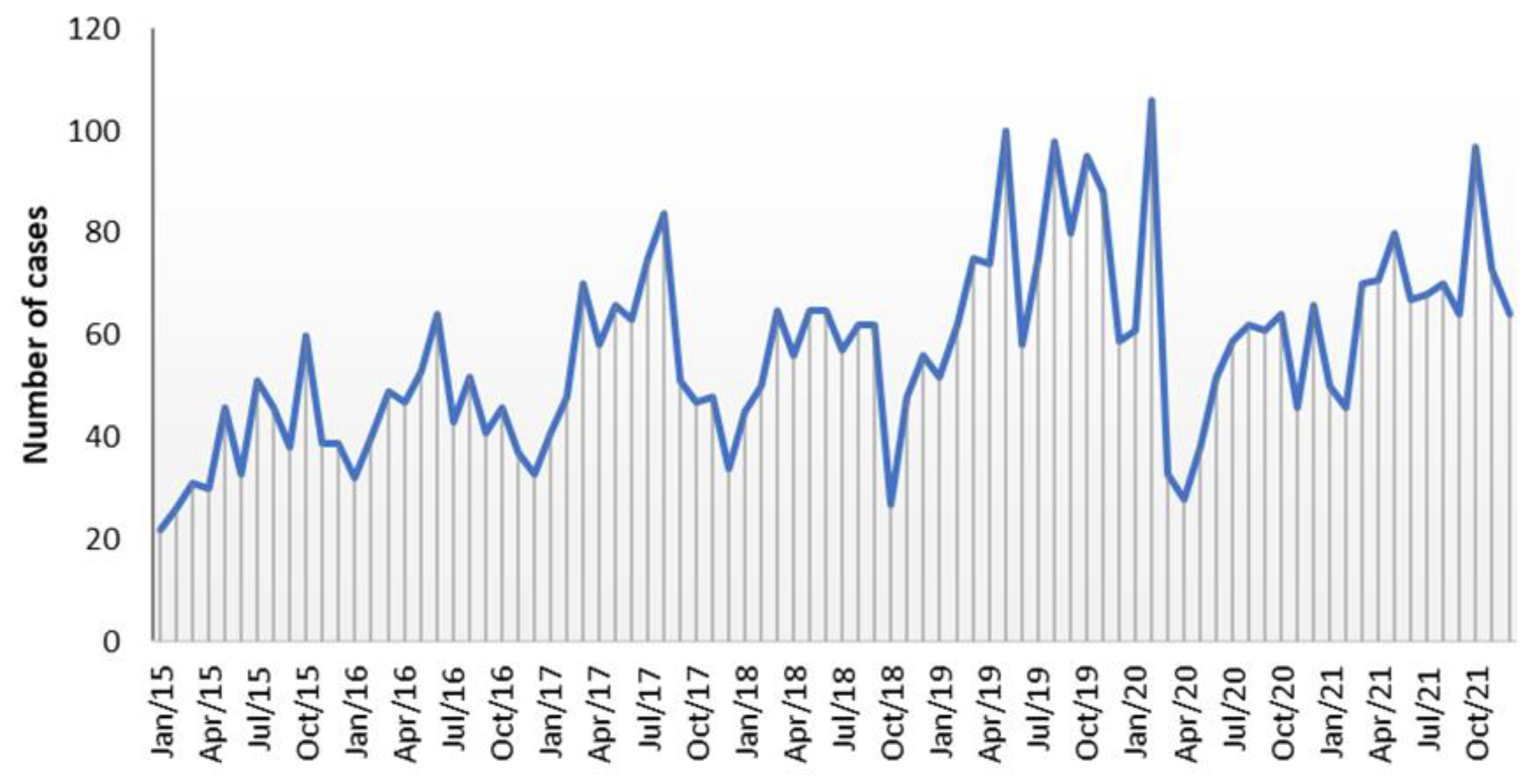
3.2. Temporal Distribution of Cases of Campylobacter Infection Received from 2009 to 2021
3.3. Seasonal Variation in the Number of Campylobacter Infection Cases
3.4. Demographic and Clinical Data
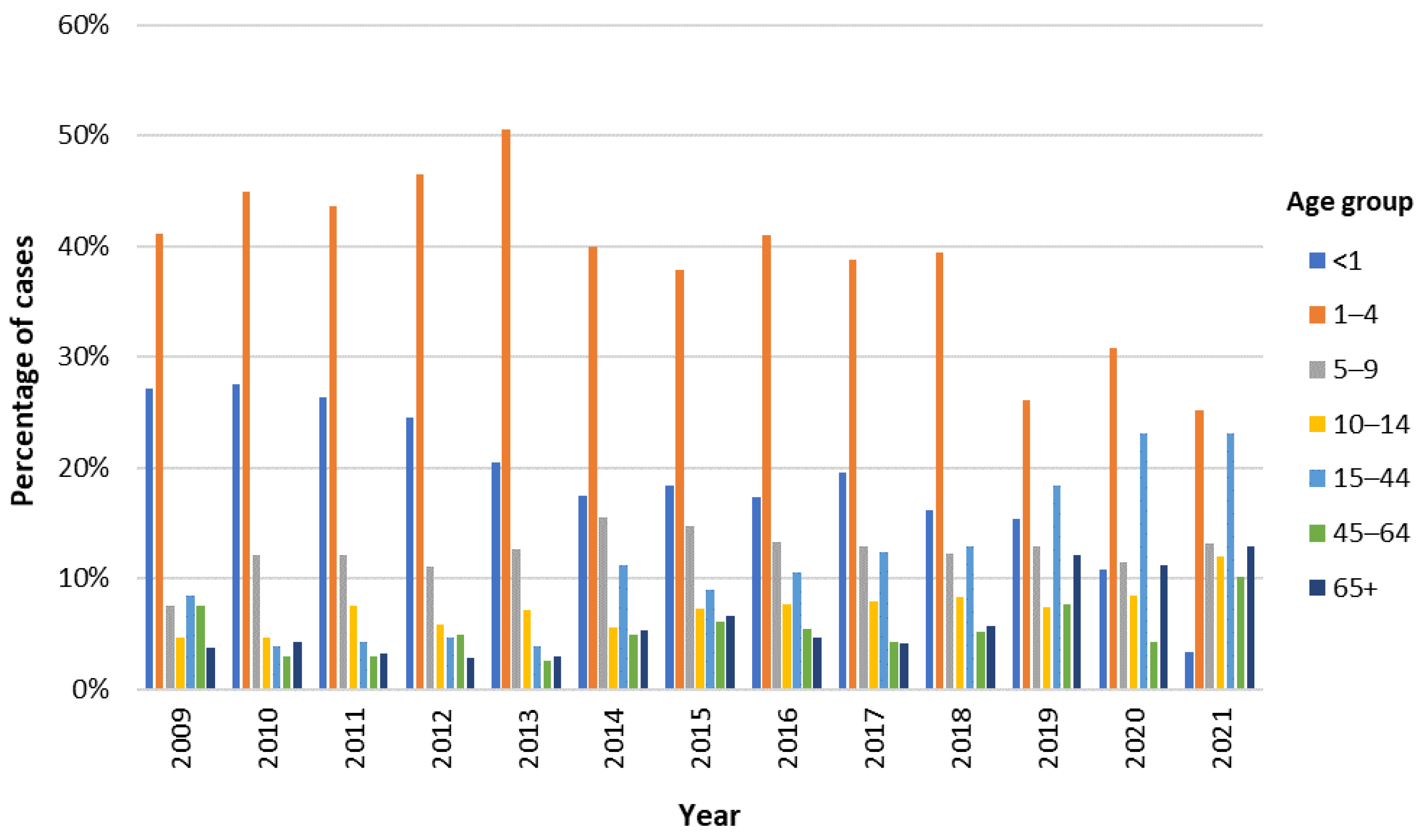
3.5. Distribution of Cases of Campylobacter Infection According to Age, Gender, and Geographic Region
3.6. Other Epidemiological Data
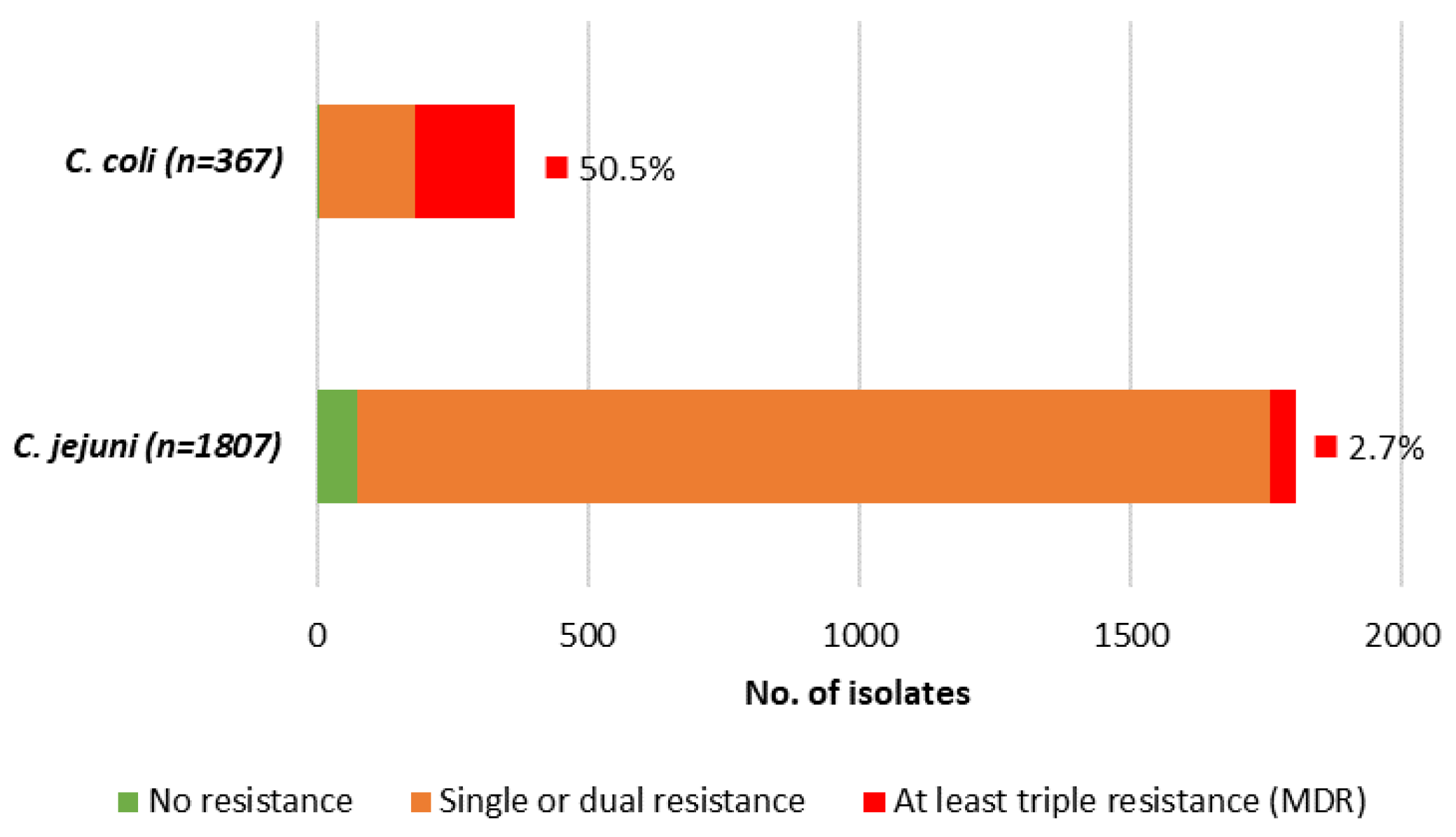
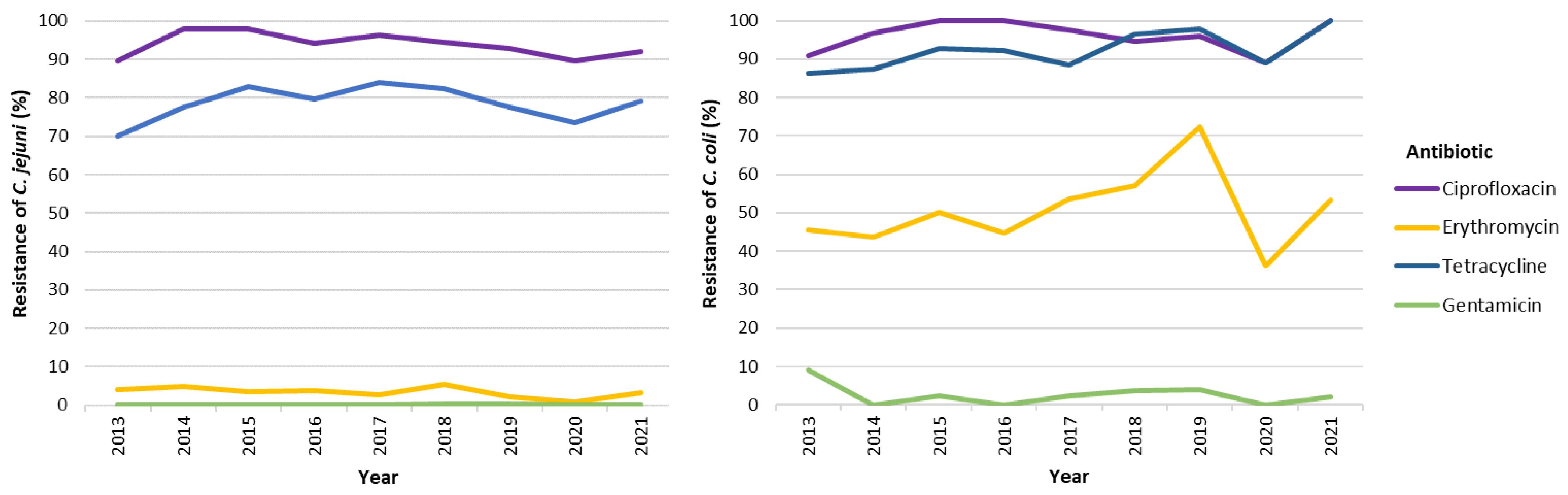
3.7. Antimicrobial Resistance of Campylobacter spp. Strains
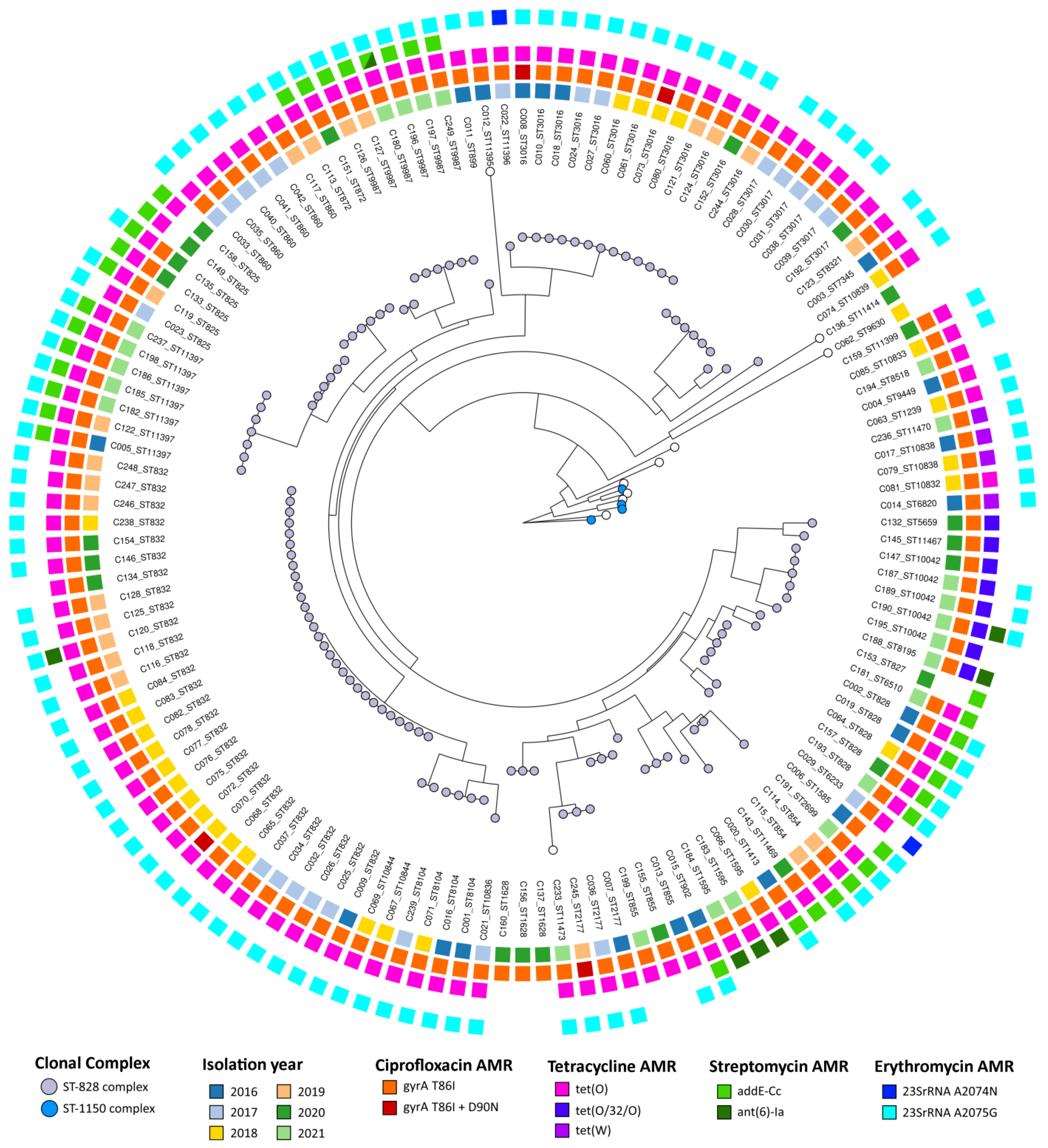
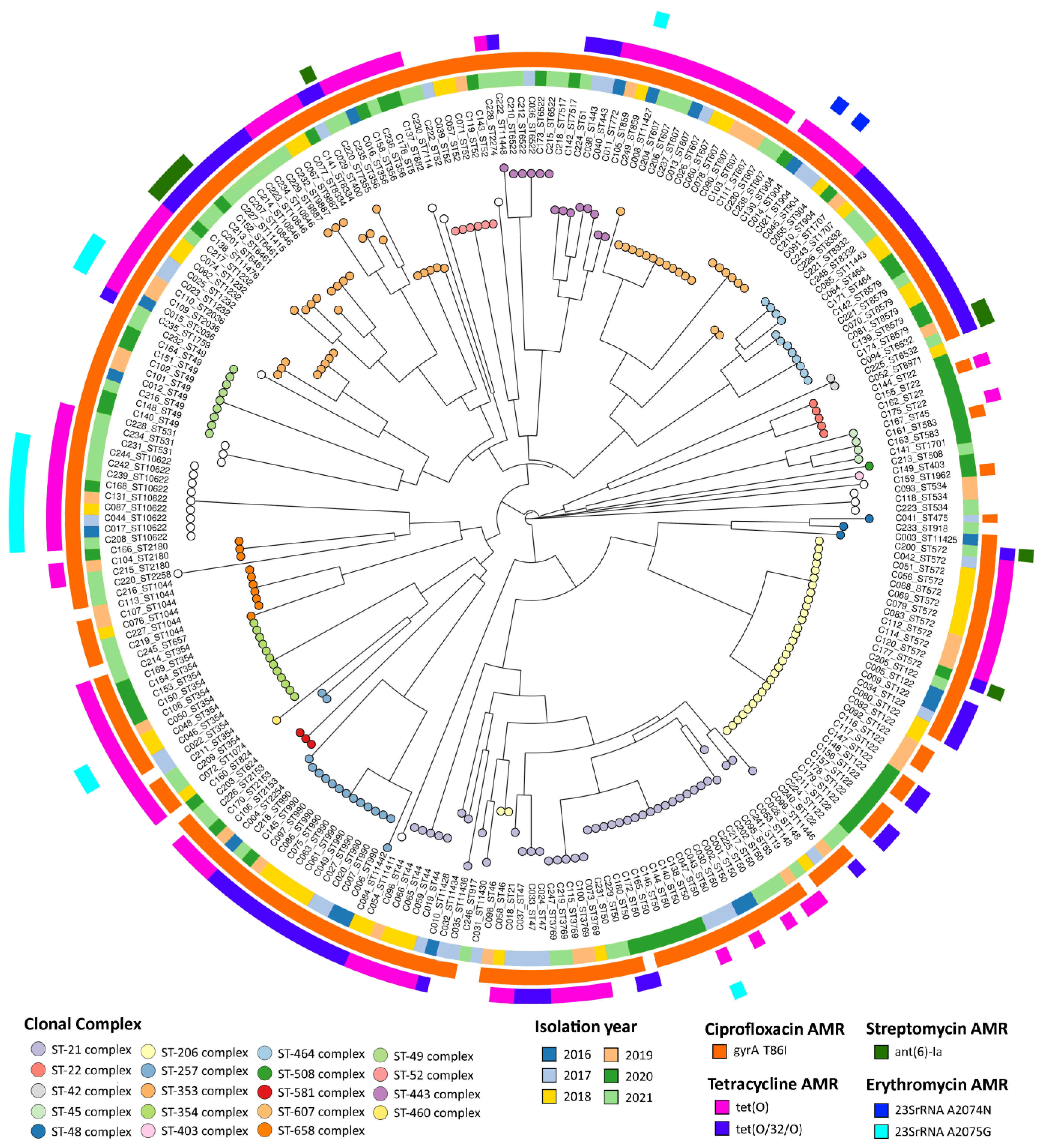
3.8. Campylobacter spp. Typing and AMR-Associated Genetic Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control (ECDC). Campylobacteriosis. In Annual Epidemiological Report for 2021; ECDC: Stockholm, Sweden, 2022. [Google Scholar]
- Rivera-Mendoza, D.; Martínez-Flores, I.; Santamaría, R.I.; Lozano, L.; Bustamante, V.H.; Pérez-Morales, D. Genomic Analysis Reveals the Genetic Determinants Associated With Antibiotic Resistance in the Zoonotic Pathogen Campylobacter spp. Distributed Globally. Front. Microbiol. 2020, 11, 513070. [Google Scholar] [CrossRef]
- Li, H.; Wang, Y.; Fu, Q.; Wang, Y.; Li, X.; Wu, C.; Shen, Z.; Zhang, Q.; Qin, P.; Shen, J.; et al. Integrated Genomic and Proteomic Analyses of High-Level Chloramphenicol Resistance in Campylobacter Jejuni. Sci. Rep. 2017, 7, 16973. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA); European Centre for Disease Prevention and Control (ECDC). The European Union One Health 2021 Zoonoses Report. EFSA J. 2022, 20, 7666. [Google Scholar] [CrossRef]
- Liu, F.; Lee, S.A.; Xue, J.; Riordan, S.M.; Zhang, L. Global Epidemiology of Campylobacteriosis and the Impact of COVID-19. Front. Cell. Infect. Microbiol. 2022, 12, 979055. [Google Scholar] [CrossRef] [PubMed]
- Cabrita, J.; Pires, I.; Vlaes, L.; Coignau, H.; Levy, J.; Goossens, H.; Goncalves, A.P.; de Mol, P.; Butzler, J.P. Campylobacter Enteritis in Portugal: Epidemiological Features and Biological Markers. Eur. J. Epidemiol. 1992, 8, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Carreira, A.C.; Clemente, L.; Rocha, T.; Tavares, A.; Geraldes, M.; Barahona, M.J.; Botelho, A.; Cunha, M.V. Comparative Genotypic and Antimicrobial Susceptibility Analysis of Zoonotic Campylobacter Species Isolated from Broilers in a Nationwide Survey, Portugal. J. Food Prot. 2012, 75, 2100–2109. [Google Scholar] [CrossRef] [PubMed]
- Duarte, A.; Santos, A.; Manageiro, V.; Martins, A.; Fraqueza, M.J.; Caniça, M.; Domingues, F.C.; Oleastro, M. Human, Food and Animal Campylobacter spp. Isolated in Portugal: High Genetic Diversity and Antibiotic Resistance Rates. Int. J. Antimicrob. Agents 2014, 44, 306–313. [Google Scholar] [CrossRef]
- Lemos, M.L.; Nunes, A.; Ancora, M.; Cammà, C.; da Costa, P.M.; Oleastro, M. Campylobacter jejuni in Different Canine Populations: Characteristics and Zoonotic Potential. Microorganisms 2021, 9, 2231. [Google Scholar] [CrossRef]
- Fraqueza, M.J.; Martins, A.; Borges, A.C.; Fernandes, M.H.; Fernandes, M.J.; Vaz, Y.; Bessa, R.J.B.; Barreto, A.S. Antimicrobial Resistance among Campylobacter Spp. Strains Isolated from Different Poultry Production Systems at Slaughterhouse Level. Poult. Sci. 2014, 93, 1578–1586. [Google Scholar] [CrossRef]
- Vicente, A.; Barros, R.; Florinda, A.; Silva, A.; Hanscheid, T. High Rates of Fluoroquinolone-Resistant Campylobacter in Portugal—Need for Surveillance. EuroSurveillance 2008, 13, 8031. [Google Scholar] [CrossRef]
- Barata, A.R.; Nunes, B.; Oliveira, R.; Guedes, H.; Almeida, C.; Saavedra, M.J.; da Silva, G.J.; Almeida, G. Occurrence and Seasonality of Campylobacter spp. in Portuguese Dairy Farms. Int. J. Food Microbiol. 2022, 383, 109961. [Google Scholar] [CrossRef]
- Ménard, A.; Dachet, F.; Prouzet-Mauleon, V.; Oleastro, M.; Mégraud, F. Development of a Real-Time Fluorescence Resonance Energy Transfer PCR to Identify the Main Pathogenic Campylobacter spp. Clin. Microbiol. Infect. 2005, 11, 281–287. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 12.0, 2022. Available online: http://www.eucast.org (accessed on 4 September 2023).
- European Centre for Disease Prevention and Control (ECDC). EU Protocol for Harmonised Monitoring of Antimicrobial Resistance in Human Salmonella and Campylobacter Isolates—Stockholm: ECDC; 2016; Annex 2. EUCAST Clinical Breakpoints and Epidemiological Cut-Off Values for the Priority List of Antimicrobials to Be Tested for Campylobacter jejuni and C. coli as of 31 August 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/eu-protocol-harmonised-monitoring-antimicrobial-resistance-human-salmonella-and-0 (accessed on 4 September 2023).
- Jehl, F.; Caron, F.; Cattoen, C.; Cattoir, V.; Dubreuil, L.; Lina, G.; Merens, A.; Plesiat, P.; Ploy, M.-C.; Soussy, C.-J.; et al. Comité de l’ Antibiogramme de La Société Française de Microbiologie Recommandations 2020. Com. L’Antibiogramme La Société Française Microbiol. 2020, 86, 1–181. [Google Scholar]
- Llarena, A.; Ribeiro-Gonçalves, B.F.; Nuno Silva, D.; Halkilahti, J.; Machado, M.P.; Da Silva, M.S.; Jaakkonen, A.; Isidro, J.; Hämäläinen, C.; Joenperä, J.; et al. INNUENDO: A Cross-sectoral Platform for the Integration of Genomics in the Surveillance of Food-borne Pathogens. EFSA Support. Publ. 2018, 15, 1498E. [Google Scholar] [CrossRef]
- Jolley, K.A.; Bray, J.E.; Maiden, M.C.J. Open-Access Bacterial Population Genomics: BIGSdb Software, the PubMLST.Org Website and Their Applications. Wellcome Open Res. 2018, 3, 124. [Google Scholar] [CrossRef]
- Bortolaia, V.; Kaas, R.S.; Ruppe, E.; Roberts, M.C.; Schwarz, S.; Cattoir, V.; Philippon, A.; Allesoe, R.L.; Rebelo, A.R.; Florensa, A.F.; et al. ResFinder 4.0 for Predictions of Phenotypes from Genotypes. J. Antimicrob. Chemother. 2020, 75, 3491–3500. [Google Scholar] [CrossRef]
- Zhou, Z.; Alikhan, N.-F.; Sergeant, M.J.; Luhmann, N.; Vaz, C.; Francisco, A.P.; Carriço, J.A.; Achtman, M. GrapeTree: Visualization of Core Genomic Relationships among 100,000 Bacterial Pathogens. Genome Res. 2018, 28, 1395–1404. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Surveillance Atlas of Infectious Disease. Available online: www.ecdc.europa.eu/en/surveillance-atlas-infectious-diseases (accessed on 5 September 2023).
- Louis, V.R.; Gillespie, I.A.; O’Brien, S.J.; Russek-Cohen, E.; Pearson, A.D.; Colwell, R.R. Temperature-Driven Campylobacter Seasonality in England and Wales. Appl. Environ. Microbiol. 2005, 71, 85–92. [Google Scholar] [CrossRef]
- Lake, I.R.; Colón-González, F.J.; Takkinen, J.; Rossi, M.; Sudre, B.; Gomes Dias, J.; Tavoschi, L.; Joshi, A.; Semenza, J.C.; Nichols, G. Exploring Campylobacter Seasonality across Europe Using the European Surveillance System (TESSy), 2008 to 2016. Eurosurveillance 2019, 24, 1800028. [Google Scholar] [CrossRef]
- Luber, P.; Brynestad, S.; Topsch, D.; Scherer, K.; Bartelt, E. Quantification of Campylobacter Species Cross-Contamination during Handling of Contaminated Fresh Chicken Parts in Kitchens. Appl. Environ. Microbiol. 2006, 72, 66–70. [Google Scholar] [CrossRef]
- Cardoso, M.J.; Ferreira, V.; Truninger, M.; Maia, R.; Teixeira, P. Cross-Contamination Events of Campylobacter Spp. in Domestic Kitchens Associated with Consumer Handling Practices of Raw Poultry. Int. J. Food Microbiol. 2021, 338, 108984. [Google Scholar] [CrossRef]
- Mylius, S.D.; Nauta, M.J.; Havelaar, A.H. Cross-Contamination during Food Preparation: A Mechanistic Model Applied to Chicken-Borne Campylobacter. Risk Anal. 2007, 27, 803–813. [Google Scholar] [CrossRef]
- Levesque, S.; Fournier, E.; Carrier, N.; Frost, E.; Arbeit, R.D.; Michaud, S. Campylobacteriosis in Urban versus Rural Areas: A Case-Case Study Integrated with Molecular Typing to Validate Risk Factors and to Attribute Sources of Infection. PLoS ONE 2013, 8, 17–20. [Google Scholar] [CrossRef]
- Murray, R.T.; Cruz-Cano, R.; Nasko, D.; Blythe, D.; Ryan, P.; Boyle, M.M.; Wilson, S.M.; Sapkota, A.R. Association between Private Drinking Water Wells and the Incidence of Campylobacteriosis in Maryland: An Ecological Analysis Using Foodborne Diseases Active Surveillance Network (FoodNet) Data (2007–2016). Environ. Res. 2020, 188, 109773. [Google Scholar] [CrossRef]
- Sheppard, S.K.; Maiden, M.C.J. The Evolution of Campylobacter jejuni and Campylobacter coli. Cold Spring Harb. Perspect. Biol. 2015, 7, a018119. [Google Scholar] [CrossRef]
- Quino, W.; Caro-Castro, J.; Hurtado, V.; Flores-León, D.; Gonzalez-Escalona, N.; Gavilan, R.G. Genomic Analysis and Antimicrobial Resistance of Campylobacter jejuni and Campylobacter coli in Peru. Front. Microbiol. 2022, 12, 802404. [Google Scholar] [CrossRef]
- Ge, B.; Wang, F.; Sjölund-Karlsson, M.; McDermott, P.F. Antimicrobial Resistance in Campylobacter: Susceptibility Testing Methods and Resistance Trends. J. Microbiol. Methods 2013, 95, 57–67. [Google Scholar] [CrossRef]
- Bolinger, H.; Kathariou, S. The Current State of Macrolide Resistance in Campylobacter Spp.: Trends and Impacts of Resistance Mechanisms. Appl. Environ. Microbiol. 2017, 83, e00416-17. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA); European Centre for Disease Prevention and Control (ECDC). The European Union Summary Report on Antimicrobial Resistance in Zoonotic and Indicator Bacteria from Humans, Animals and Food in 2020/2021. EFSA J. 2023, 21, 7867. [Google Scholar] [CrossRef]
- Tang, Y.; Fang, L.; Xu, C.; Zhang, Q. Antibiotic Resistance Trends and Mechanisms in the Foodborne Pathogen, Campylobacter. Anim. Health Res. Rev. 2017, 18, 87–98. [Google Scholar] [CrossRef]
- Hendriksen, R.S.; Bortolaia, V.; Tate, H.; Tyson, G.H.; Aarestrup, F.M.; McDermott, P.F. Using Genomics to Track Global Antimicrobial Resistance. Front. Public Health 2019, 7, 242. [Google Scholar] [CrossRef]
- Dahl, L.G.; Joensen, K.G.; Østerlund, M.T.; Kiil, K.; Nielsen, E.M. Prediction of Antimicrobial Resistance in Clinical Campylobacter jejuni Isolates from Whole-Genome Sequencing Data. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 673–682. [Google Scholar] [CrossRef]
- Sifré, E.; Salha, B.A.; Ducournau, A.; Floch, P.; Chardon, H.; Mégraud, F.; Lehours, P. EUCAST Recommendations for Antimicrobial Susceptibility Testing Applied to the Three Main Campylobacter Species Isolated in Humans. J. Microbiol. Methods 2015, 119, 206–213. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA); Aerts, M.; Battisti, A.; Hendriksen, R.; Kempf, I.; Teale, C.; Tenhagen, B.A.; Veldman, K.; Wasyl, D.; Guerra, B.; et al. Technical Specifications on Harmonised Monitoring of Antimicrobial Resistance in Zoonotic and Indicator Bacteria from Food-Producing Animals and Food. EFSA J. 2019, 17, 5709. [Google Scholar] [CrossRef]
- Dai, L.; Sahin, O.; Grover, M.; Zhang, Q. New and Alternative Strategies for the Prevention, Control, and Treatment of Antibiotic-Resistant Campylobacter. Transl. Res. 2020, 223, 76–88. [Google Scholar] [CrossRef]
- Nunes, A.; Oleastro, M.; Alves, F.; Liassine, N.; Lowe, D.M.; Benejat, L.; Ducounau, A.; Jehanne, Q.; Borges, V.; Gomes, J.P.; et al. Recurrent Campylobacter jejuni Infections with In Vivo Selection of Resistance to Macrolides and Carbapenems: Molecular Characterization of Resistance Determinants. Microbiol. Spectr. 2023, 11, e0107023. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Overall | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | ||
| Total cases received in the NRL | 129 | 248 | 347 | 328 | 426 | 437 | 461 | 537 | 685 | 658 | 916 | 676 | 820 | 6668 |
| Isolates processed by the NRL | 129 | 248 | 347 | 328 | 426 | 437 | 461 | 537 | 685 | 658 | 364 | 260 | 325 | 5205 |
| Isolates with antibiotic susceptibility data | 0 | 0 | 0 | 0 | 119 | 135 | 182 | 191 | 289 | 336 | 349 | 248 | 325 | 2174 |
| Isolates with typing data * | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 20/17 | 23/30 | 27/42 | 21/32 | 22/53 | 23/70 | 380 |
| Year | Overall | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | ||
| C. jejuni n (%) | 112 (86.8) | 208 (83.9) | 300 (86.5) | 294 (89.6) | 393 (92.3) | 388 (88.8) | 394 (85.5) | 474 (88.3) | 626 (91.4) | 591 (89.8) | 311 (85.4) | 221 (85.0) | 278 (85.5) | 4590 (88.2) |
| C. coli n (%) | 17 (13.2) | 40 (16.1) | 47 (13.5) | 34 (10.4) | 33 (7.7) | 49 (11.2) | 67 (14.5) | 63 (11.7) | 59 (8.6) | 67 (10.2) | 53 (14.6) | 39 (15.0) | 47 (14.5) | 615 (11.8) |
| Total | 129 | 248 | 347 | 328 | 426 | 437 | 461 | 537 | 685 | 658 | 364 | 260 | 325 | 5205 |
| Reported Symptoms | With Diarrhea (Including Bloody Diarrhea) n = 3405 n (% within Group) | Without Diarrhea n = 268 n (% within Group) |
|---|---|---|
| Abdominal pain | 299 (8.8) | 65 (24.3) |
| Fever | 316 (9.3) | 58 (21.6) |
| Vomiting | 102 (3.0) | 12 (4.5) |
| Abdominal pain + fever | 61 (1.8) | 14 (5.2) |
| Abdominal pain + vomiting | 27 (0.8) | 7 (2.6) |
| Abdominal pain + fever + vomiting | 12 (0.4) | 2 (0.7) |
| Fever + vomiting | 68 (2.0) | 2 (0.7) |
| No other reported symptoms | 2520 (74.0) | -- |
| Main Symptom | Pediatric Population (n = 2982) n (% within Group) | Adult Population (n = 677) n (% within Group) | Total (n = 3659) n (% of Total) | OR (95%CI) | p |
|---|---|---|---|---|---|
| Bloody Diarrhea | 1353 (45.4) | 101 (14.9) | 1454 (39.7) | 4.7367 (3.788–5.922) | <0.001 |
| Non-bloody diarrhea | 1492 (48.4) | 449 (66.3) | 1941 (53.0) | 0.5085 (0.427–0.606) | <0.001 |
| Abdominal pain | 345 (11.6) | 140 (20.7) | 485 (13.3) | 0.5018 (0.404–0.624) | <0.001 |
| Fever | 404 (13.5) | 128 (18.9) | 592 (16.2) | 0.6721 (0.540–0.837) | <0.001 |
| Vomiting | 180 (7.3) | 52 (7.7) | 232 (6.3) | 0.7721 (0.560–1.064) | 0.114 |
| No. Positive Samples (% within Group) (% of Total) | Total | ||
|---|---|---|---|
| Campylobacter jejuni | Campylobacter coli | ||
| Gender (n = 5144) | |||
| Female | 1791 (39.5 a) (34.8) | 257 (42.3 a) (5.0) | 2048 (39.8) |
| Male | 2745 (60.5 a) (53.4) | 351 (57.7 a) (6.8) | 3096 (60.2) |
| Total | 4536 (88.2) | 608 (11.8) | 5144 (100) |
| Age group (n = 5120) | |||
| <1 | 831 (18.4 a) (16.2) | 103 (17.0 a) (2.0) | 934 (18.2) |
| 1–4 | 1807 (40.0 a) (35.3) | 194 (32.1 b) (3.8) | 2001 (39.1) |
| 5–9 | 589 (13.0 a) (11.5) | 68 (11.2 a) (1.3) | 657 (12.8) |
| 10–14 | 348 (7.7 a) (6.8) | 36 (6.0 b) (0.7) | 384 (7.5) |
| 15–44 | 482 (10.7 a) (9.4) | 95 (15.7 b) (1.9) | 577 (11.3) |
| 45–64 | 212 (4.7 a) (4.1) | 52 (8.6 b) (1.0) | 264 (5.2) |
| + 65 | 246(5.4 a) (4.8) | 57 (9.4 b) (1.1) | 303 (5.9) |
| Total | 4515 (88.2 a) | 605 (11.8 b) | 5120 (100) |
| Region (n = 5203) | |||
| North | 2317 (50.5 a) (45.0) | 271(44.1 b) (5.2) | 2588 (44.7) |
| Center | 711 (15.5 a) (13.9) | 78 (12.7 a) (1.5) | 789 (15.2) |
| Metropolitan Lisbon Area | 1560 (34.0 a) (29.5) | 241 (43.3 b) (5.1) | 1826 (35.1) |
| Total | 4588 (88.2) | 615 (11.8) | 5203 (100) |
| Antimicrobial Category | Antimicrobial Agent | Mean Inhibition Diameter Zone (in mm) (SD) | p | % Resistance (n/n Total) | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Total | C. jejuni | C. coli | Total (n = 2174) | C. jejuni (n = 1807) | C. coli (n = 367) | ||||
| Fluoroquinolones | Ciprofloxacin (CIP) | 9.35 (7.07) | 10.54 (8.70) | 8.66 (579) | 0.002 | 94.2 (2048) | 93.7 (1694) | 96.5 (354) | 0.043 |
| Macrolides | Erythromycin (ERY) | 26.31 (8.02) | 28.12 (5.44) | 15.85 (11.06) | <0.001 | 11.8 (252) | 3.3 (60) | 52.3 (192) | <0.001 |
| Tetracyclines | Tetracycline (TCY) | 14.36 (11.53) | 16.66 (12.78) | 10.02 (7.97) | <0.001 | 81.6 (1773) | 79.2 (1431) | 93.2 (342) | <0.001 |
| Aminoglycosides | Gentamicin (GEN) | 28.40 (3.95) | 28.47 (3.78) | 26.69 (4.21) | <0.001 | 0.5 (11) | 0.1 (2) | 2.5 (9) | <0.001 |
| Penicillins + β-lactamase inhibitors | Amoxicillin–clavulanic acid (AMC) * | 28.66 (4.71) | 28.76 (4.34) | 23.95 (5.79) | <0.001 | 0.8 (12/1547) | 0.2 (3/1314) | 3.9 (9/233) | <0.001 |
| Carbapenems | Ertapenem (ETP) ** | 0.125 (0.019) | 0.19 (0.034) | 0.5 (0.075) | <0.001 | 1.6 (24/1543) | 0.7 (9/1311) | 6.5 (15/232) | <0.001 |
| Penicillins | Ampicillin (AMP) | 10.42 (7.22) | 11.56 (7.64) | 10.69 (7.47) | 0.348 | 76.3 (944/1238) | 75.5 (794/1051) | 80.2 (150/187) | 0.192 |
| Amoxicillin | Ampicillin | Ciprofloxacin | Erythromycin | Ertapenem | Gentamicin | Tetracycline | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R | S | p Value OR (95%CI) | R | S | p Value OR (95%CI) | R | S | p Value OR (95%CI) | R | S | p Value OR (95%CI) | R | S | p Value OR (95%CI) | R | S | p Value OR (95%CI) | R | S | p Value OR (95%CI) | |
| Gender Female Male | 6 6 | 614 916 | 0.697 Ref 0.793 (0.247–2.547) | 372 568 | 127 167 | 0.279 Ref 1.160 (0.887–1.515) | 810 1225 | 48 78 | 0.734 Ref 0.937 (0.645–1.363) | 112 138 | 1185 746 | 0.959 Ref 0.991 (0.714–1.377) | 11 13 | 605 909 | 0.662 Ref 0.831 (0.362–1.907) | 6 5 | 852 1298 | 0.470 Ref 0.640 (0.190–2.150) | 708 1055 | 150 248 | 0.509 Ref 0.926 (0.736–1.164) |
| Age <15 15–44 45+ | 8 2 2 | 960 302 267 | 0.825 Ref 0.658 (0.134–3.234) 0.700 (0.143–3.425) | 589 184 168 | 160 67 67 | 0.022 Ref 0.714 (0.510–1.000) 0.660 (0.472–0.923) | 1344 355 337 | 63 30 33 | 0.001 Ref. 0.531 (0.335–0.841) 0.456 (0.293–0.709) | 148 44 57 | 1259 341 313 | 0.183 Ref. 1.002 (0.646–1.553) 1.458 (0.965–2.202) | 16 5 3 | 948 299 267 | 0.564 Ref. 0822 (0.291–2.322) 0.506 (0.143–1.790) | 7 2 2 | 1400 383 368 | 0.949 Ref. 0.850 (0.171–4.230) 0.787 (0.158–3.916) | 1178 308 278 | 229 77 92 | <0.001 Ref. 0.778 (0.579–1.046) 0.571 (0.431–0.756) |
| Species C. jejuni C. coli | 3 9 | 1311 224 | <0.001 Ref. 17.987 (4.765–67.90) | 794 150 | 257 37 | 0.123 Ref. 1.360 (0.920–2.010) | 1694 354 | 113 13 | 0.041 Ref. 1.850 (1.026–3.336) | 60 192 | 1747 175 | <0.001 Ref. 31.088 (22.27–43.40) | 9 15 | 1302 217 | <0.001 Ref. 9.775 (4.193–22.79) | 2 9 | 1805 358 | <0.001 Ref. 20.989 (4.48–98.33) | 1431 342 | 376 25 | <0.001 Ref. 3.705 (2.423–5.666) |
| Region North Center Metropolitan Lisbon Area | 5 3 4 | 690 176 668 | 0.390 Ref. 1.994 (0.447–8.901) 0.680 (0.177–2.614) | 403 112 428 | 136 32 126 | 0.421 Ref. 1.206 (0.773–1.882) 1.195 (0.901–1.585) | 940 227 880 | 59 20 47 | 0.166 Ref. 0.767 (0.449–1.310) 1.276 (0.854–1.908) | 98 35 119 | 901 212 808 | 0.698 Ref. 1.205 (0.714–2.034) 0.966 (0.680–1.373) | 6 2 16 | 686 177 655 | 0.135 Ref. 1.081 (0.21–5.556) 2.480 (0.945–6.513) | 3 1 7 | 996 246 920 | 0.574 Ref. 1.151 (0.116–11.47) 2.023 (0.507–8.066) | 828 203 741 | 171 44 186 | 0.215 Ref. 1.077 (0.741–1.564) 1.236 (0.974–1.568) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, A.; Pereira, L.; Lemos, M.-L.; Pinto, M.; Rodrigues, J.C.; Matias, R.; Santos, A.; PTCampyNet; Oleastro, M. Epidemiological Data and Antimicrobial Resistance of Campylobacter spp. in Portugal from 13 Years of Surveillance. Pathogens 2024, 13, 147. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens13020147
Duarte A, Pereira L, Lemos M-L, Pinto M, Rodrigues JC, Matias R, Santos A, PTCampyNet, Oleastro M. Epidemiological Data and Antimicrobial Resistance of Campylobacter spp. in Portugal from 13 Years of Surveillance. Pathogens. 2024; 13(2):147. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens13020147
Chicago/Turabian StyleDuarte, Andreia, Luísa Pereira, Maria-Leonor Lemos, Miguel Pinto, João Carlos Rodrigues, Rui Matias, Andrea Santos, PTCampyNet, and Mónica Oleastro. 2024. "Epidemiological Data and Antimicrobial Resistance of Campylobacter spp. in Portugal from 13 Years of Surveillance" Pathogens 13, no. 2: 147. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens13020147