High Prevalence of Strongyloidiasis in Spain: A Hospital-Based Study

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Seroprevalence
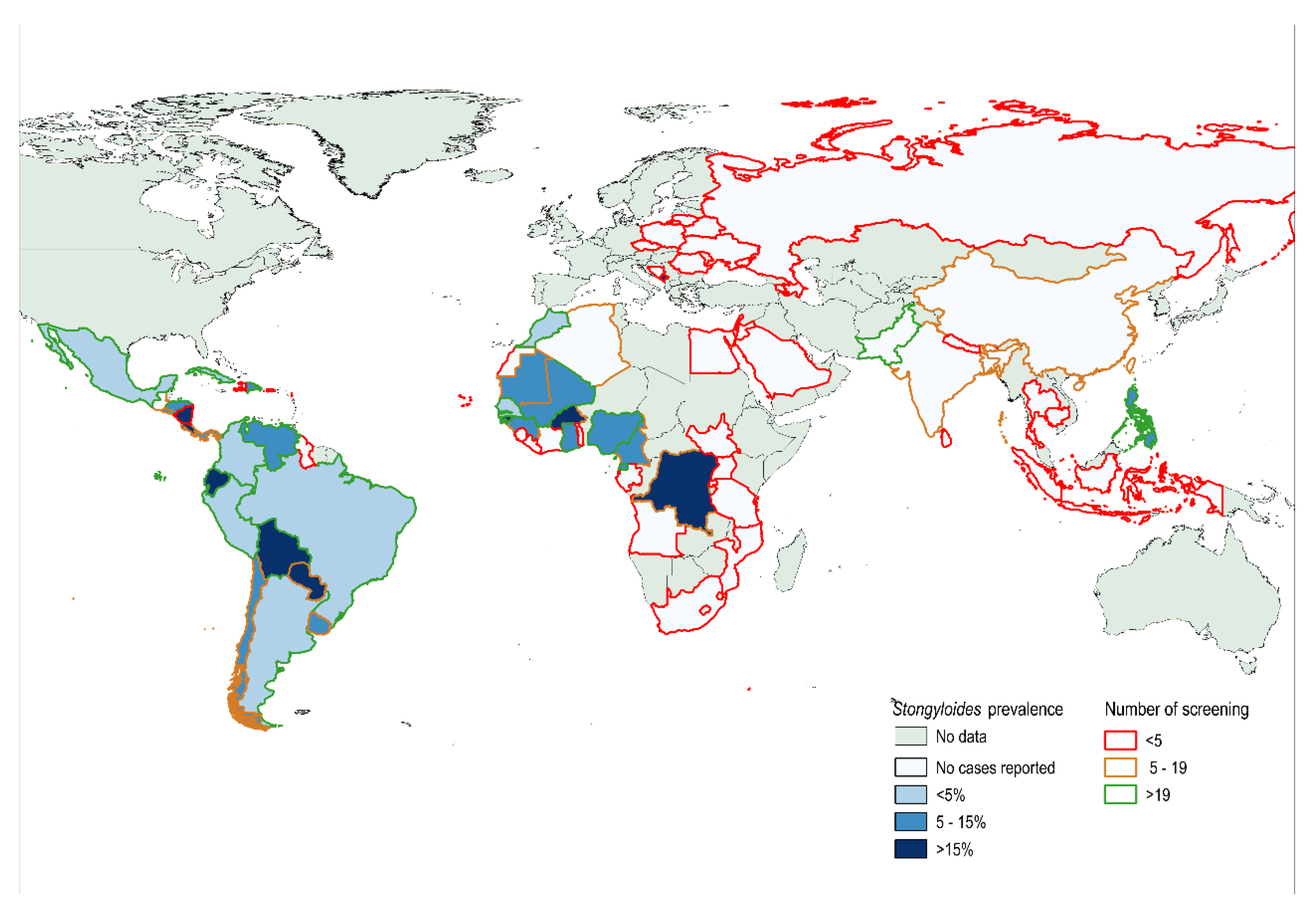
2.1.1. Seroprevalence by Geographic Distribution
2.1.2. Seroprevalence by Screening Department
3. Discussion
4. Materials and Methods
4.1. Study Population, Data Collection and Patient Management
4.2. Microbiological Procedures Serology of S. stercoralis
4.3. Sample Size Estimation
4.4. Statistical Analysis
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix

{kind=link}
| Prevalence | CI-95% | n | |
|---|---|---|---|
| LATIN AMERICA | |||
| ARGENTINA | 3.4 | 0.7–9.5 | 89 |
| BOLIVIA | 15.8 | 12–20.2 | 329 |
| BRAZIL | 2.73 | 0.6–7.8 | 110 |
| COLOMBIA | 3.8 | 1–9.5 | 105 |
| CHILE | 5.6 | 0.1–27.3 | 18 |
| CUBA | 2.6 | 0.07–13.5 | 39 |
| ECUADOR | 17.5 | 10.7–26.2 | 103 |
| MEXICO | 4.5 | 0.1–22.8 | 22 |
| PARAGUAY | 18.2 | 2.3–51.8 | 11 |
| PERU | 1.3 | 0.03-0.7 | 75 |
| VENEZUELA | 5.1 | 1.4–12.6 | 78 |
| AFRICA | |||
| ANGOLA | 0 | 0–70.6 * | 3 |
| ALGERIA | 0 | 0–45.9 * | 6 |
| BURKINA FASO | 16.7 | 2.1–48.4 | 12 |
| CABO VERD | 0 | 0–97.5 * | 1 |
| CAMEROON | 14.3 | 1.8–42.8 | 14 |
| CONGO | 33.3 | 4.3–77.7 | 6 |
| EGYPT | 0 | 0–84.2 * | 2 |
| GAMBIA | 8.7 | 1.1–28 | 23 |
| IVORY COAST | 0 | 0–52.2 * | 5 |
| EQUATORIAL GUINEA | 13.6 | 7–23 | 81 |
| GABON | 0 | 0–84.2 * | 2 |
| GHANA | 14.8 | 4.2–33.7 | 27 |
| GUINEA BISSAU | 25 | 13.2–40.3 | 44 |
| GUINEA CONAKRY | 12.5 | 15.5–38.3 | 16 |
| LIBERIA | 0 | 0–97.5 * | 1 |
| MAURITANIA | 14.3 | 0.3–57.9 | 7 |
| MALI | 6.9 | 2.6–14.4 | 87 |
| MORROCCO | 4.7 | 1.7–9.9 | 128 |
| MOZAMBIQUE | 0 | 0–97.5 * | 1 |
| NIGERIA | 5.6 | 0.7–18.7 | 36 |
| RUANDA | 0 | 0–84.2 * | 2 |
| SAUDI ARABIA | 0 | 0–84.2 * | 2 |
| SENEGAL | 4.9 | 1.34–12 | 82 |
| TANZANIA | 0 | 0–60.2 | 4 |
| ASIA | |||
| AZERBAIYAN | 0 | 0–97.5 * | 1 |
| BANGLADESH | 0 | 0–45.9 * | 6 |
| BUTAN | 0 | 0–97.5 * | 1 |
| CAMBODIA | 0 | 0–97.5 * | 1 |
| CHINA | 0 | 0–26.5 | 12 |
| INDONESIA | 0 | 0–84.2 * | 2 |
| ISRAEL | 0 | 0–97.5 * | 1 |
| JORDAN | 0 | 0–97.5 * | 1 |
| INDIA | 0 | 0–28.5 * | 11 |
| LEBANNON | 0 | 0–97.5 * | 1 |
| NEPAL | 0 | 0–84.2 * | 2 |
| PAKISTAN | 0 | 0–9 | 39 |
| PHILIPPINES | 13.6 | 2.9–34.9 | 22 |
| SRI LANKA | 0 | 0–97.5 * | 1 |
| THAILAND | 0 | 0–84.2 * | 2 |
| EAST EUROPE | |||
| ARMENIA | 0 | 0–97.5 * | 1 |
| BIELORRUSSIA | 0 | 0–97.5 * | 1 |
| BOSNIA | 0 | 0–97.5 * | 1 |
| LITHUANIA | 0 | 0–97.5 * | 1 |
| MONTENEGRO | 0 | 0–97.5 * | 1 |
| POLAND | 0 | 0–97.5 * | 1 |
| CZECH REPUBLIC | 0 | 0–97.5 * | 1 |
| ROMANIA | 0 | 0–60.2 | 4 |
| RUSSIA | 0 | 0–97.5 * | 1 |
| UKRAINE | 0 | 0–84.2 * | 2 |
References
- Bisoffi, Z.; Buonfrate, D.; Montresor, A.; Requena-Méndez, A.; Muñoz, J.; Krolewiecki, A.J.; Gotuzzo, E.; Mena, M.A.; Chiodini, P.L.; Anselmi, M.; et al. Strongyloides stercoralis: A Plea for Action. PLOS Negl. Trop. Dis. 2013, 7, e2214. [Google Scholar] [CrossRef] [Green Version]
- Montes, M.; Sawhney, C.; Barros, N. Strongyloides stercoralis: There but not seen. Curr. Opin. Infect. Dis. 2010, 23, 500–504. [Google Scholar] [CrossRef]
- Olsen, A.; Van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, S.; Verweij, J.J.; Magnussen, P. Strongyloidiasis—The most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [Green Version]
- Buonfrate, D.; Baldissera, M.; Abrescia, F.; Bassetti, M.; Caramaschi, G.; Giobbia, M.; Mascarello, M.; Rodari, P.; Scattolo, N.; Napoletano, G.; et al. Epidemiology ofStrongyloides stercoralisin northern Italy: Results of a multicentre case–control study, February 2013 to July 2014. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [Green Version]
- Pacheco-Tenza, M.I.; Ruiz-Maciá, J.A.; Navarro-Cots, M.; Gregori-Colomé, J.; Cepeda-Rodrigo, J.M.; Llenas-García, J. Strongyloides stercoralis infection in a Spanish regional hospital: Not just an imported disease. Enfermedades Infecc. y Microbiol. Clin. (English ed.) 2018, 36, 24–28. [Google Scholar] [CrossRef]
- Genta, R.M. Global Prevalence of Strongyloidiasis: Critical Review with Epidemiologic Insights into the Prevention of Disseminated Disease. Clin. Infect. Dis. 1989, 11, 755–767. [Google Scholar] [CrossRef]
- Requena-Méndez, A.; Buonfrate, D.; Bisoffi, Z.; Gutiérrez, J.M. Advances in the Diagnosis of Human Strongyloidiasis. Curr. Trop. Med. Rep. 2014, 1, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The Laboratory Diagnosis and Follow Up of Strongyloidiasis: A Systematic Review. PLoS Neglected Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef]
- Gonzalez, A.; Gallo, M.; Valls, M.E.; Muñoz, J.; Puyol, L.; Pinazo, M.J.; Mas, J.; Gascon, J.; Viana, L.D.G.; De Assis, T.S.M.; et al. Clinical and epidemiological features of 33 imported Strongyloides stercoralis infections. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 613–616. [Google Scholar] [CrossRef]
- Sorvillo, F.; Mori, K.; Sewake, W.; Fishman, L. Sexual transmission of Strongyloides stercoralis among homosexual men. Sex. Transm. Infect. 1983, 59, 342. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Junyent, J.; Paredes-Zapata, D.; Parras, E.R.D.L.; González-Costello, J.; Ruiz-Arranz, Á; Cañizares, R.; Saugar, J.M.; Muñoz, J. Real-Time Polymerase Chain Reaction in Stool Detects Transmission of Strongyloides stercoralis from an Infected Donor to Solid Organ Transplant Recipients. Am. J. Trop. Med. Hyg. 2016, 94, 897–899. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Junyent, J.; Paredes, D.; Hurtado, J.C.; Requena-Mendez, A.; Ruiz, A.; Valls, M.E.; Vila, J.; Muñoz, J. High seroprevalence of Strongyloides stercoralis among individuals from endemic areas considered for solid organ transplant donation: A retrospective serum-bank based study. PLoS Neglected Trop. Dis. 2018, 12, e0007010. [Google Scholar] [CrossRef]
- Nordheim, E.; Storrø, M.O.; Natvik, A.K.; Kro, G.B.; Midtvedt, K.; Reisaeter, A.V.; Hagness, M.; Fevang, B.; Pettersen, F.O. Donor-derived strongyloidiasis after organ transplantation in Norway. Transpl. Infect. Dis. 2018, 21, e13008. [Google Scholar] [CrossRef] [Green Version]
- Camargo, L.F.A.; Kamar, N.; Gotuzzo, E.; Wright, A.J. Schistosomiasis and Strongyloidiasis Recommendations for Solid-Organ Transplant Recipients and Donors. Transplantation 2018, 102, S27–S34. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Méndez, A.; Angheben, A.; Muñoz, J.; Gobbi, F.; Ende, J.V.D.; Bisoffi, Z. Severe strongyloidiasis: A systematic review of case reports. BMC Infect. Dis. 2013, 13, 78. [Google Scholar] [CrossRef] [Green Version]
- Requena-Méndez, A.; Muñoz, J.; Gomez-Junyent, J.; Bisoffi, Z.; Buonfrate, D.; Zammarchi, L. Evidence-Based Guidelines for Screening and Management of Strongyloidiasis in Non-Endemic Countries. Am. J. Trop. Med. Hyg. 2017, 97, 645–652. [Google Scholar] [CrossRef]
- Asundi, A.; Beliavsky, A.; Liu, X.J.; Akaberi, A.; Schwarzer, G.; Bisoffi, Z.; Requena-Méndez, A.; Shrier, I.; Greenaway, C. Prevalence of strongyloidiasis and schistosomiasis among migrants: A systematic review and meta-analysis. Lancet Glob. Heal. 2019, 7, e236–e248. [Google Scholar] [CrossRef] [Green Version]
- Luvira, V.; Chantawat, N.; Naaglor, T.; Dekumyoy, P.; Mungthin, M.; Trakulhun, K.; Phiboonbanakit, D.; Pakdee, W. Comparative Diagnosis of Strongyloidiasis in Immunocompromised Patients. Am. J. Trop. Med. Hyg. 2016, 95, 401–404. [Google Scholar] [CrossRef] [Green Version]
- Agbata, E.N.; Morton, R.L.; Bisoffi, Z.; Bottieau, E.; Greenaway, C.; Biggs, B.-A.; Montero, N.; Tran, A.; Rowbotham, N.; Arevalo-Rodriguez, I.; et al. Effectiveness of Screening and Treatment Approaches for Schistosomiasis and Strongyloidiasis in Newly-Arrived Migrants from Endemic Countries in the EU/EEA: A Systematic Review. Int. J. Environ. Res. Public Heal. 2018, 16, 11. [Google Scholar] [CrossRef] [Green Version]
- ECDC. Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA; ECDC: Stockholm, Sweden, 2018.
- Buonfrate, D.; Angheben, A.; Gobbi, F.; Munoz, J.; Requena-Méndez, A.; Gotuzzo, E.; Mena, M.A.; Bisoffi, Z. Imported Strongyloidiasis: Epidemiology, Presentations, and Treatment. Curr. Infect. Dis. Rep. 2012, 14, 256–262. [Google Scholar] [CrossRef]
- Salas-Coronas, J.; Cuenca-Gómez, J.Á.; Soriano-Pérez, M.J.; Cabezas-Fernández, M.T.; Lozano-Serrano, A.B.; Vázquez-Villegas, J. Newly Arrived African Migrants to Spain: Epidemiology and Burden of Disease. Am. J. Trop. Med. Hyg. 2018, 98, 319–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, J.M.; Leon, R.; Andreu, M.; Parras, E.R.D.L.; Rodríguez-Díaz, J.C.; Esteban, A.; Saugar, J.M.; Torrus, D. Serological study of Trypanosoma cruzi, Strongyloides stercoralis, HIV, human T cell lymphotropic virus (HTLV) and syphilis infections in asymptomatic Latin-American immigrants in Spain. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Martelli, G.; Di Girolamo, C.; Zammarchi, L.; Angheben, A.; Morandi, M.; Tais, S.; Degani, M.; El Hamad, I.; Caligaris, S.; Ciannameo, A.; et al. Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: A cross-sectional study. Clin. Microbiol. Infect. 2017, 23, 335.e1–335.e5. [Google Scholar] [CrossRef] [Green Version]
- Khalil, H.M.; Makled, M.K.; E Azab, M.; Abdalla, H.M.; A El Sherif, E.; Nassef, N.S. Opportunistic parasitic infections in immunocompromised hosts. J. Egypt. Soc. Parasitol. 1991, 21, 657–668. [Google Scholar]
- de Paula, F.M.; de Castro, E.; Goncalves-Pires, M.; Marcal, M.; Campos, D.M.; Costa-Cruz, J.M. Parasitological and immunological diagnoses of strongyloidiasis in immunocompromised and non-immunocompromised children at Uberlandia, State of Minas Gerais, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2000, 42, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Salvador, F.; Molina, I.; Sulleiro, E.; Burgos, J.; Curran, A.; Eynde, E.V.D.; Del Saz, S.V.; Navarro, J.; Crespo, M.; Ocaña, I.; et al. Tropical Diseases Screening in Immigrant Patients with Human Immunodeficiency Virus Infection in Spain. Am. J. Trop. Med. Hyg. 2013, 88, 1196–1202. [Google Scholar] [CrossRef] [Green Version]
- Winnicki, W.; Eder, M.; Mazal, P.; Mayer, F.J.; Sengölge, G.; Wagner, L. Prevalence of Strongyloides stercoralis infection and hyperinfection syndrome among renal allograft recipients in Central Europe. Sci. Rep. 2018, 8, 15406. [Google Scholar] [CrossRef]
- Puerta-Alcalde, P.; Gómez-Junyent, J.; Requena-Mendez, A.; Pinazo, M.J.; Alvarez-Martínez, M.J.; Rodriguez, N.; Gascón, J.; Muñoz, J. High prevalence of S. Stercoralis infection among patients with Chagas disease: A retrospective case-control study. PLoS Neglected Trop. Dis. 2018, 12, e0006199. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, A.E.; Weld, L.H.; Barnett, E.D.; So, H.; Coyle, C.; Greenaway, C.; Stauffer, W.; Leder, K.; Lopez-Velez, R.; Gautret, P.; et al. Spectrum of illness in international migrants seen at GeoSentinel clinics in 1997-2009, part 2: Migrants resettled internationally and evaluated for specific health concerns. Clin. Infect. Dis. 2013, 56, 925–933. [Google Scholar] [CrossRef] [Green Version]
- Laoraksawong, P.; Sanpool, O.; Rodpai, R.; Thanchomnang, T.; Kanarkard, W.; Maleewong, W.; Kraiklang, R.; Intapan, P.M. Current high prevalences of Strongyloides stercoralis and Opisthorchis viverrini infections in rural communities in northeast Thailand and associated risk factors. BMC Public Health 2018, 18, 940. [Google Scholar] [CrossRef] [Green Version]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic Accuracy of Five Serologic Tests for Strongyloides stercoralis Infection. PLoS Neglected Trop. Dis. 2014, 8, e2640. [Google Scholar] [CrossRef] [Green Version]
- Harvey, K.; Esposito, D.H.; Han, P.; Kozarsky, P.; O Freedman, D.; Plier, D.A.; Sotir, M.J. Surveillance for travel-related disease—GeoSentinel Surveillance System, United States, 1997–2011. MMWR. Surveill. Summ. 2013, 62, 1–23. [Google Scholar]

| Variable | Frequency |
|---|---|
| Age (n = 1943) | |
| Median (IQR) | 38 (31–48) |
| Group | |
| <25 | 201 (10.34%) |
| 26–39 | 846 (43.54%) |
| 40–54 | 652 (33.56%) |
| >54 | 244 (12.56%) |
| Male sex (n = 1634) | 947 (57.96%) |
| Hospitals | |
| Clinic | 902 |
| Vall d’Hebron | 411 |
| Hospital Poniente | 303 |
| Hospital Mar | 198 |
| Hospital Sant Pau | 70 |
| Hospital Bellvitge | 64 |
| Departments or units | |
| General services | 77 |
| Autoimmune/Rheumatology | 86 |
| Transplant units | 150 |
| Hemato-Oncology | 101 |
| International Health | 804 |
| HIV units | 709 |
| Other | 21 |
| Continents (n = 1876) | |
| Africa | 600 |
| North Africa | 141 |
| SSA | 459 |
| America | 1106 |
| South America | 934 |
| Central America &Caribe | 172 |
| Asia | 103 |
| South-Central Asia | 61 |
| South-East Asia Middle East | 273 |
| East Asia | 12 |
| Europe | 67 |
| West Europe | 53 |
| East Europe | 14 |
| Percentage (CI) | A: Immunosuppressed Units * (%) | B: Other Non Immunosuppressed Units from the Hospital ** (%) | C: Tropical Diseases Units | p-Value *** | |
|---|---|---|---|---|---|
| South-America | 9.6 (7.8–11.7) | 30/558 (5.38%) | 1/11 (9.1) | 59/365 (16.2%) | <0.001 |
| Central America and Caribbean | 7 (3.7–11.9) | 5/128 (3.91) | 0/8 (0) | 7/36 (19.44) | 0.04 |
| North African | 4.3 (1.6–9.1) | 3/90 (3.3) | 0/3 | 3/47 (6.4) | 0.658 |
| Sub-Saharan Africa | 10.9 (8.2–14.1) | 12/155 (7.7) | 1/6 (16.7) | 37/298 (12.4) | 0.286 |
| Middle East | 0 (0–70.6) | 0/2 | 0 | 0 | --- |
| South-Central Asia | 0 (0–58.7) | 0/29 | 0/5 | 0/27 | |
| South-East Asia | 11.1 (2.4–29.2) | 2/19 (10.5) | 0/2 | 1/6 (16.7) | 0.801 |
| East Asia | 0 (0–26.4) | 0/5 | 0 | 0/7 | --- |
| East Europe | 7.1 (0.2–33.9) | 1/13 (7.7) | 0/1 | 0 | 0.773 |
| Western Europe (travellers with multiple travels) | 5.7 (1.2–15.7) | 3/21 (14.3) | 0/15 | 0/17 | 0.089 |
| Total | 9 (7.7–10.3) | 59/1046 (5.64) | 10/98 (10.2) | 107/803 (13.39 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requena-Méndez, A.; Salas-Coronas, J.; Salvador, F.; Gomez-Junyent, J.; Villar-Garcia, J.; Santin, M.; Muñoz, C.; González-Cordón, A.; Cabezas Fernández, M.T.; Sulleiro, E.; et al. High Prevalence of Strongyloidiasis in Spain: A Hospital-Based Study. Pathogens 2020, 9, 107. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9020107
Requena-Méndez A, Salas-Coronas J, Salvador F, Gomez-Junyent J, Villar-Garcia J, Santin M, Muñoz C, González-Cordón A, Cabezas Fernández MT, Sulleiro E, et al. High Prevalence of Strongyloidiasis in Spain: A Hospital-Based Study. Pathogens. 2020; 9(2):107. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9020107
Chicago/Turabian StyleRequena-Méndez, Ana, Joaquin Salas-Coronas, Fernando Salvador, Joan Gomez-Junyent, Judith Villar-Garcia, Miguel Santin, Carme Muñoz, Ana González-Cordón, Maria Teresa Cabezas Fernández, Elena Sulleiro, and et al. 2020. "High Prevalence of Strongyloidiasis in Spain: A Hospital-Based Study" Pathogens 9, no. 2: 107. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9020107