Comparison of Diagnostic Tests for Onchocerca volvulus in the Democratic Republic of Congo

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Study Participants and Sample Collection
2.3. Detection of O. volvulus in Skin Snips by Microscopy
2.4. Detection of Antibodies against O. volvulus
2.5. Data Processing and Statistical Analysis
2.6. Ethical Considerations and Informed Consent
3. Results
3.1. Demographic and Clinical Information of the Study Participants
3.2. Comparison of the Three Diagnostic Tests
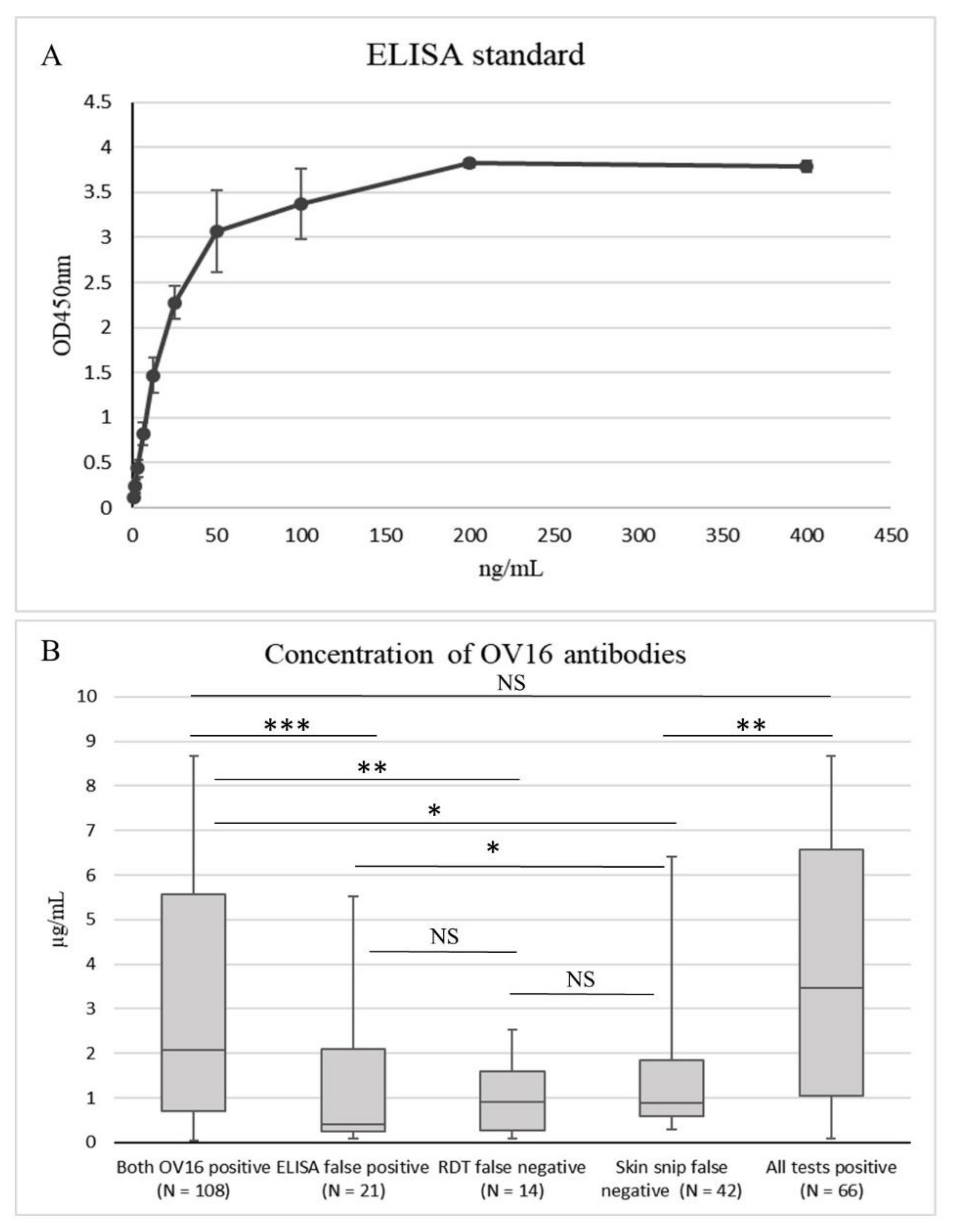
3.3. OV16 Antibody Concentration
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Onchocerciasis and Its Control; Technical report series no. 852; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Colebunders, R.; Siewe, F.N.; Hotterbeekx, A. Onchocerciasis-Associated Epilepsy, an Additional Reason for Strengthening Onchocerciasis Elimination Programs. Trends Parasitol. 2018, 34, 208–216. [Google Scholar] [CrossRef] [PubMed]
- WHO. Progress report on the elimination of human onchocerciasis, 2015–2016. Wkly. Epidemiol. Rec. 2016, 91, 505–514. [Google Scholar]
- Tekle, A.H.; Zouré, H.G.; Mounkaila, N.; Boussinesq, M.; Coffeng, L.E.; Stolk, W.; Remme, J.H.F. Progress towards onchocerciasis elimination in the participating countries of the African Programme for Onchocerciasis Control: Epidemiological evaluation results. Infect. Dis. Poverty 2016, 5, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amazigo, U. The African Programme for Onchocerciasis Control (APOC). Ann. Trop. Med. Parasitol. 2008, 102, 19–22. [Google Scholar] [CrossRef]
- WHO. Guidelines for Stopping Mass Drug Administration and Verifying Elimination of Human Onchocerciasis: Criteria and Procedures; WHO Press: Geneva, Switzerland, 2016. [Google Scholar]
- Weil, G.J.; Steel, C.; Liftis, F.; Li, B.-W.; Mearns, G.; Lobos, E.; Nutman, T.B. A Rapid-Format Antibody Card Test for Diagnosis of Onchocerciasis. J. Infect. Dis. 2000, 182, 1796–1799. [Google Scholar] [CrossRef] [Green Version]
- Lipner, E.M.; Dembele, N.; Souleymane, S.; Alley, W.S.; Prevots, D.R.; Toe, L.; Boatin, B.; Weil, G.J.; Nutman, T.B. Field Applicability of a Rapid-Format Anti–Ov-16 Antibody Test for the Assessment of Onchocerciasis Control Measures in Regions of Endemicity. J. Infect. Dis. 2006, 194, 216–221. [Google Scholar] [CrossRef]
- Cama, V.A.; Feleke, S.M.; McDonald, C.; Wiegand, R.E.; Cantey, P.T.; Arcury-Quandt, A.; Eberhard, M.; Abanyie, F.; Smith, J.; Jenks, M.H.; et al. Evaluation of an OV-16 IgG4 Enzyme-Linked Immunosorbent Assay in Humans and Its Application to Determine the Dynamics of Antibody Responses in a Non-Human Primate Model of Onchocerca volvulus Infection. Am. J. Trop. Med. Hyg. 2018, 99, 1041–1048. [Google Scholar] [CrossRef] [Green Version]
- Lont, Y.L.; Coffeng, L.E.; De Vlas, S.J.; Golden, A.; Santos, T.D.L.; Domingo, G.J.; Stolk, W. Modelling Anti-Ov16 IgG4 Antibody Prevalence as an Indicator for Evaluation and Decision Making in Onchocerciasis Elimination Programmes. PLoS Negl. Trop. Dis. 2017, 11, e0005314. [Google Scholar] [CrossRef]
- Dieye, Y.; Storey, H.L.; Barrett, K.L.; Gerth-Guyette, E.; Di Giorgio, L.; Golden, A.; Faulx, D.; Kalnoky, M.; Ndiaye, M.K.N.; Sy, N.; et al. Feasibility of utilizing the SD BIOLINE Onchocerciasis IgG4 rapid test in onchocerciasis surveillance in Senegal. PLoS Negl. Trop. Dis. 2017, 11, e0005884. [Google Scholar] [CrossRef]
- Golden, A.; Faulx, D.; Kalnoky, M.; Stevens, E.; Yokobe, L.; Peck, R.; Karabou, P.; Banla, M.; Rao, R.; Adade, K.; et al. Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis. Parasites Vectors 2016, 9, 338. [Google Scholar] [CrossRef] [Green Version]
- Richards, F.; Aziz, N.A.; Katabarwa, M.; Rodríguez-Pérez, M.A.; Unnasch, T.R.; Silva, R.L.; Fernández-Santos, N.A.; Bekele, F.; Monroy, Z.M.; Tadesse, Z.; et al. Operational Performance of the Onchocerca volvulus “OEPA” Ov16 ELISA Serological Assay in Mapping, Guiding Decisions to Stop Mass Drug Administration, and Posttreatment Surveillance Surveys. Am. J. Trop. Med. Hyg. 2018, 99, 749–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colebunders, R.; Mandro, M.; Mukendi, D.; Dolo, H.; Suykerbuyk, P.; Van Oijen, M.; Hopkins, A.; Kaiser, C.; Chaccour, C. Ivermectin Treatment in Patients With Onchocerciasis-Associated Epilepsy: Protocol of a Randomized Clinical Trial. JMIR Res. Protoc. 2017, 6, e137. [Google Scholar] [CrossRef] [PubMed]
- Mandro, M.; Fodjo, J.N.S.; Dusabimana, A.; Mukendi, D.; Haesendonckx, S.; Lokonda, R.; Nakato, S.; Nyisi, F.; Abhafule, G.; Wonya’Rossi, D.; et al. Single versus Multiple Dose Ivermectin Regimen in Onchocerciasis-Infected Persons with Epilepsy Treated with Phenobarbital: A Randomized Clinical Trial in the Democratic Republic of Congo. Pathogens 2020, 9, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenaerts, E.; Mandro, M.; Mukendi, D.; Suykerbuyk, P.; Dolo, H.; Wonya’Rossi, D.; Nyisi, F.; Ensoy-Musoro, C.; Laudisoit, A.; Hotterbeekx, A.; et al. High prevalence of epilepsy in onchocerciasis endemic health areas in Democratic Republic of the Congo. Infect. Dis. Poverty 2018, 7, 68. [Google Scholar] [CrossRef]
- Fodjo, J.N.S.; Mandro, M.; Mukendi, D.; Tepage, F.; Menon, S.; Nakato, S.; Nyisi, F.; Abhafule, G.; Wonya’Rossi, D.; Anyolito, A.; et al. Onchocerciasis-associated epilepsy in the Democratic Republic of Congo: Clinical description and relationship with microfilarial density. PLoS Negl. Trop. Dis. 2019, 13, e0007300. [Google Scholar] [CrossRef]
- Prost, A.; Prod’hon, J. Parasitological diagnosis of onchocerciasis. A critical review of present methods (author’s transl). Med. Trop. Rev. Corps Sante Colonial 1978, 38, 519–532. [Google Scholar]
- Golden, A.; Stevens, E.J.; Yokobe, L.; Faulx, D.; Kalnoky, M.; Peck, R.; Valdez, M.; Steel, C.; Karabou, P.; Banla, M.; et al. A Recombinant Positive Control for Serology Diagnostic Tests Supporting Elimination of Onchocerca volvulus. PLoS Negl. Trop. Dis. 2016, 10, e0004292. [Google Scholar] [CrossRef] [Green Version]
- Somo, R.M.; Fobi, G.; Ngosso, A.; Dinga, J.S.; LaFleur, C.; Enyong, P.A.; Ngolle, E.M.; Agnamey, P. A Study of Onchocerciasis with Severe Skin and Eye Lesions in a Hyperendemic Zone in the Forest of Southwestern Cameroon: Clinical, Parasitologic, and Entomologic Findings. Am. J. Trop. Med. Hyg. 1993, 48, 14–19. [Google Scholar] [CrossRef]
- Stingl, P. Onchocerciasis: Clinical presentation and host parasite interactions in patients of Southern Sudan. Int. J. Dermatol. 1997, 36, 23–28. [Google Scholar] [CrossRef]
- Murdoch, M.E.; Murdoch, I.E.; Evans, J.R.; Yahaya, H.; Njepuome, N.; Cousens, S.; Jones, B.R.; Abiose, A. Pre-control relationship of onchocercal skin disease with onchocercal infection in Guinea Savanna, Northern Nigeria. PLoS Negl. Trop. Dis. 2017, 11, e0005489. [Google Scholar] [CrossRef]
- Lobos, E.; Weiss, N.; Karam, M.; Taylor, H.R.; Ottesen, E.; Nutman, T. An immunogenic Onchocerca volvulus antigen: A specific and early marker of infection. Science 1991, 251, 1603–1605. [Google Scholar] [CrossRef] [PubMed]
- Bennuru, S.; Oduro-Boateng, G.; Osigwe, C.; Del Valle, P.; Golden, A.; Ogawa, G.M.; Cama, V.; Lustigman, S.; Nutman, T.B. Integrating Multiple Biomarkers to Increase Sensitivity for the Detection of Onchocerca volvulus Infection. J. Infect. Dis. 2019, 221, 1805–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiele, E.A.; Cama, V.A.; Sleshi, M.; Abanyie, F.; Lakwo, T.; Mekasha, S.; Cantey, P.T.; Kebede, A. Detection of Onchocerca volvulus in Skin Snips by Microscopy and Real-Time Polymerase Chain Reaction: Implications for Monitoring and Evaluation Activities. Am. J. Trop. Med. Hyg. 2016, 94, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Persons with Epilepsy (n = 285) |
|---|---|
| Age: median (IQR) | 21 (15–30) |
| Male: n (%) | 147 (51.6%) |
| Weight (kg): median (IQR) | 45.8 (35–51) |
| Height (cm): median (IQR) | 152 (143–160) |
| Received ivermectin: n, (%) | 6 (2%) |
| Itching 1: n (%) | 105 (36.8%) |
| Abnormal skin #: n (%) | 42 (14.7%) |
| Papular skin: n (%) | 8 (19.0%) |
| Leopard skin: n (%) | 10 (23.8%) |
| Lizard skin: n (%) | 12 (28.6%) |
| Unspecified: n (%) | 18 (42.8%) |
| Onchocerca nodules 2: n (%) | 17 (5.9%) |
| O. volvulus microfilariae present in skin snip: n (%) | 105 (36.8%) |
| Microfilariae load: median (IQR) | 18.5 (6.5–72.0) |
| Positive OV16 ELISA: n (%) | 143 (50.2%) |
| Concentration OV16 antibodies (µg/mL): median (IQR) | 1.66 (0.47–4.46) |
| Positive OV16 RDT: n (%) | 112 (39.3%) |
| O. volvulus infection *: n (%) | 147 (51.6%) |
| Skin Snip | OV16 ELISA | OV16 RDT | Total | |
|---|---|---|---|---|
| All negative | - | - | - | 115 |
| All OV16 false negative | + | - | - | 23 |
| ELISA false positive | - | + | - | 21 |
| RDT false negative | + | + | - | 14 |
| RDT false positive | - | - | + | 2 |
| ELISA false negative | + | - | + | 2 |
| Skin snip false negative | - | + | + | 42 |
| All positive | + | + | + | 66 |
| True Negative | 138 | 117 | 136 | NA |
| False Negative | 42 | 25 | 37 | NA |
| True Positive | 105 | 122 | 110 | NA |
| False Positive | 0 | 21 | 2 | NA |
| Sensitivity | 71.4% | 83% | 74.8% | NA |
| Specificity | 100% | 84.8% | 98.6% | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hotterbeekx, A.; Perneel, J.; Mandro, M.; Abhafule, G.; Siewe Fodjo, J.N.; Dusabimana, A.; Abrams, S.; Kumar-Singh, S.; Colebunders, R. Comparison of Diagnostic Tests for Onchocerca volvulus in the Democratic Republic of Congo. Pathogens 2020, 9, 435. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9060435
Hotterbeekx A, Perneel J, Mandro M, Abhafule G, Siewe Fodjo JN, Dusabimana A, Abrams S, Kumar-Singh S, Colebunders R. Comparison of Diagnostic Tests for Onchocerca volvulus in the Democratic Republic of Congo. Pathogens. 2020; 9(6):435. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9060435
Chicago/Turabian StyleHotterbeekx, An, Jolien Perneel, Michel Mandro, Germain Abhafule, Joseph Nelson Siewe Fodjo, Alfred Dusabimana, Steven Abrams, Samir Kumar-Singh, and Robert Colebunders. 2020. "Comparison of Diagnostic Tests for Onchocerca volvulus in the Democratic Republic of Congo" Pathogens 9, no. 6: 435. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9060435