
Validation of an In-House ELISA Method in the Diagnosis of Cutaneous Leishmaniasis Caused by Leishmania donovani in Hambantota District, Sri Lanka

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Sample Collection
2.2.1. Patients with Cutaneous Leishmaniasis (CL)
2.2.2. Control Groups
2.3. Molecular Diagnosis
2.4. ELISA to Detect Anti-rKRP42 IgG in Serum and Urine
2.5. Rapid Test (Kalazar Detect™) to Detect Anti-rK39 Antibodies in a Subset of Patients with Confirmed CL
2.6. Data Management and Statistical Analysis
2.7. Ethical Considerations
3. Results
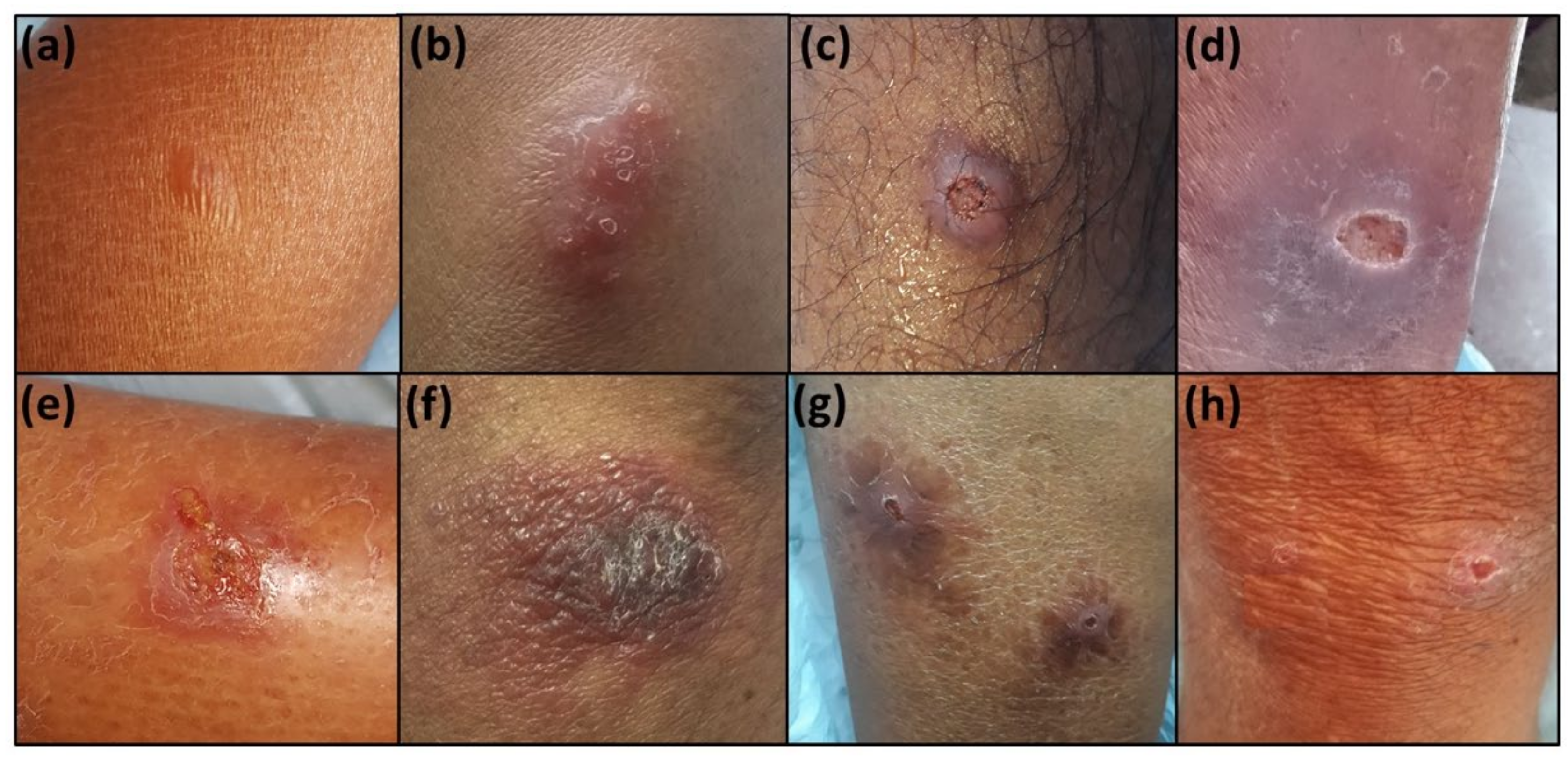
3.1. Clinical and Demographic Data
3.2. Laboratory Diagnosis of CL Patients
3.2.1. Nested PCR Method (Reference Standard of the Study)
3.2.2. Giemsa Stained SSS Microscopy
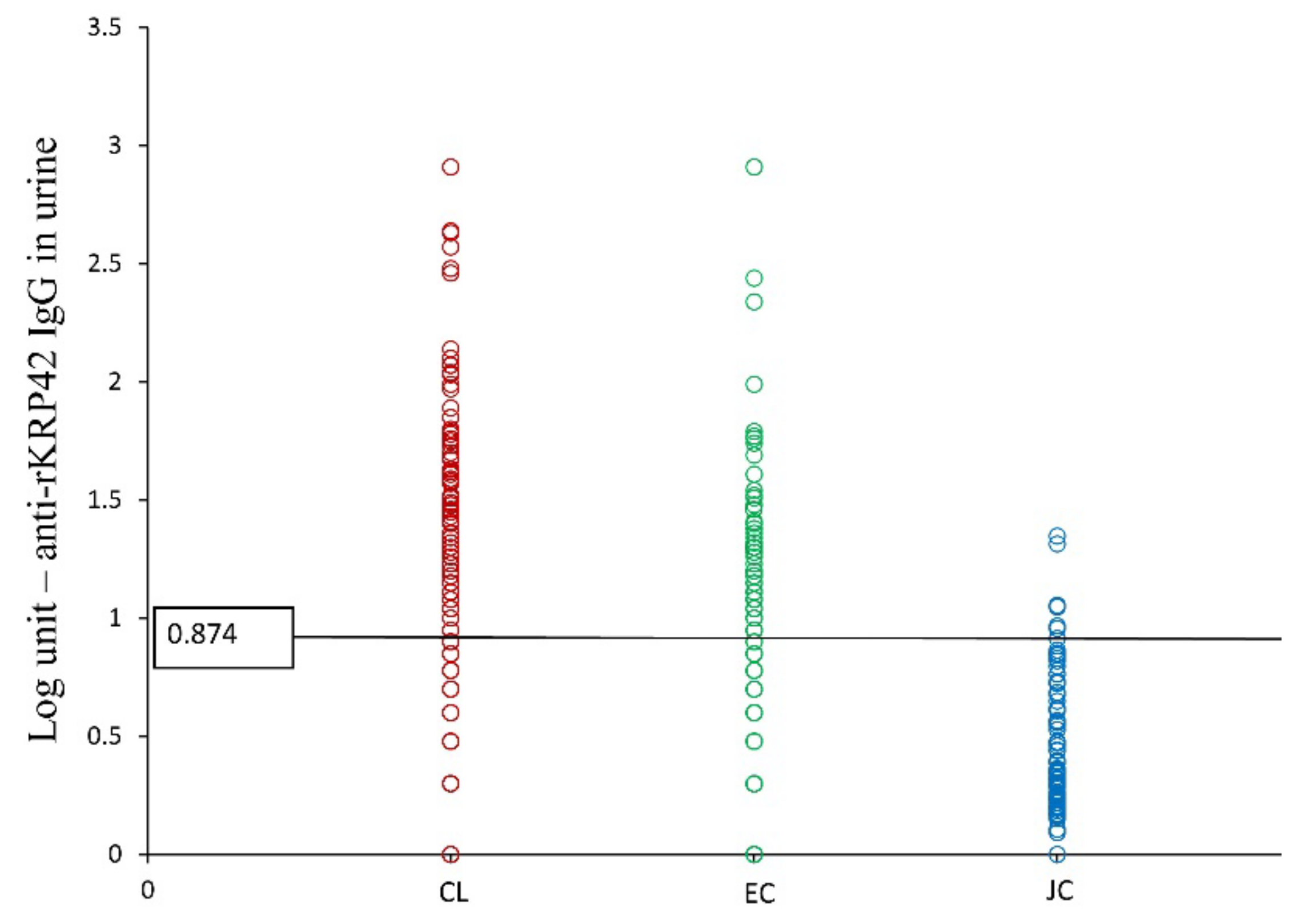
3.2.3. Serum and Urine Anti-rKRP42 IgG ELISA: Calculation of Cutoff Values and Determination of Sensitivity and Specificity
3.2.4. Sensitivity, Specificity, PPV, and NPP of Anti-rKRP42 IgG Serum and Urine ELISAs among CL, EC, and JC
3.3. Correlation between Serum and Urine Anti-rKRP42 IgG Titers
3.4. Combination of SSS and Serum rKRP42 ELISA
3.5. The Test Capability in the Diagnosis of Clinically Doubtful Lesions
3.6. CL Cases Tested by rK39 Rapid Test (Kalazar Detect™)
3.7. Clinico-Demographic Correlations of CL Patients (n = 190) against rKRP42 Serum ELISA
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leishmaniasis, 2 March 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis (accessed on 15 April 2020).
- Karunaweera, N.; Pratlong, F.; Siriwardane, H.; Ihalamulla, R.; Dedet, J. Sri Lankan cutaneous leishmaniasis is caused by Leishmania donovani zymodeme MON-37. Trans. R. Soc. Trop. Med. Hyg. 2003, 97, 380–381. [Google Scholar] [CrossRef]
- Guernaoui, S.; Boumezzough, A.; Pesson, B.; Pichon, G. Entomological investigations in Chichaoua: An emerging epidemic focus of cutaneous leishmaniasis in Morocco. J. Med. Entomol. 2005, 42, 697–701. [Google Scholar] [CrossRef]
- Semage, S.; Pathirana, K.; Agampodi, S. Cutaneous leishmaniasis in Mullaitivu, Sri Lanka: A missing endemic district in the leishmaniasis surveillance system. Int. J. Infect. Dis. 2014, 25, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Athukorale, D.N.; Seneviratne, J.K.; Ihalamulla, R.L.; Premaratne, U.N. Locally acquired cutaneous leishmaniasis in Sri Lanka. J. Trop. Med. Hyg. 1992, 95. [Google Scholar]
- Alam, M.Z.; Haralambous, C.; Kuhls, K.; Gouzelou, E.; Sgouras, D.N.; Soteriadou, K.; Schnur, L.; Pratlong, F.; Schönian, G. The paraphyletic composition of Leishmania donovani zymodeme MON-37 revealed by multilocus microsatellite typing. Microbes Infect. 2009, 11, 707–715. [Google Scholar] [CrossRef]
- Gajapathy, K.; Peiris, L.B.; Goodacre, S.L.; Silva, A.; Jude, P.J.; Surendran, S.N. Molecular identification of potential leishmaniasis vector species within the Phlebotomus (Euphlebotomus) argentipes species complex in Sri Lanka. Parasites Vectors 2013, 6, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilango, K. A taxonomic reassessment of the Phlebotomus argentipes species complex (Diptera: Psychodidae: Phlebotominae). J. Med. Entomol. 2010, 47, 1–15. [Google Scholar] [CrossRef]
- Rajapaksa, U.; Ihalamulla, R.L.; Karunaweera, N. First report of mucosal tissue localisation of leishmaniasis in Sri Lanka. Ceylon Med. J. 2005, 50, 90–91. [Google Scholar]
- Ranasinghe, S.; Zhang, W.-W.; Wickremasinghe, R.; Abeygunasekera, P.; Chandrasekharan, V.; Athauda, S.; Mendis, S.; Hulangamuwa, S.; Matlashewski, G.; Pratlong, F.J.P. Leishmania donovani zymodeme MON-37 isolated from an autochthonous visceral leishmaniasis patient in Sri Lanka. Pathog. Glob. Health 2012, 106, 421–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosypal, A.C.; Tripp, S.; Kinlaw, C.; Hailemariam, S.; Tidwell, R.R.; Lindsay, D.S.; Rajapakse, R.P.V.J.; Sreekumar, C.; Dubey, J.P. Surveillance for Antibodies to Leishmania spp. in Dogs from Sri Lanka. J. Parasitol. 2010, 96, 230–231. [Google Scholar] [CrossRef]
- Abayaweera, C.A.; Siriwardana, Y.; Abeywardana, T.J.; Rathnayaka, R.M.; Kumarasinghe, H.G.; Karunaweera, N.D. Dogs as a Possible Animal Reservoir for Leishmaniasis in Dickwella. In Annual Research Proceedings; University of Colombo: Colombo, Sri Lanka, 2010. [Google Scholar]
- Ranawaka, R.; Abeygunasekara, P.; Weerakoon, H. Correlation of clinical, parasitological and histopathological diagnosis of cutaneous leishmaniasis in an endemic region in Sri Lanka. Ceylon Med. J. 2013, 57, 149. [Google Scholar] [CrossRef]
- Mandal, J.; Dubey, M.L.; Malla, N.; Varma, N.; Bhatia, P.; Khurana, S. Evaluation of direct agglutination test, rk39 Test, and ELISA for the diagnosis of visceral leishmaniasis. Am. J. Trop. Med. Hyg. 2008, 79, 76–78. [Google Scholar] [CrossRef]
- Vaish, M.; Bhatia, A.; Reed, S.; Chakravarty, J.; Sundar, S. Evaluation of rK28 antigen for serodiagnosis of visceral Leishmaniasis in India. Clin. Microbiol. Infect. 2012, 18, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, P.; Bhaskar, K.R.H.; Hossain, F.; Khan, A.A.; Vallur, A.C.; Duthie, M.S.; Hamano, S.; Salam, A.; Huda, M.M.; Khan, G.M.; et al. Evaluation of diagnostic performance of rK28 ELISA using urine for diagnosis of visceral leishmaniasis. Parasites Vector. 2016, 9, 383. [Google Scholar] [CrossRef] [Green Version]
- Duarte, M.C.; Pimenta, D.; Menezes-Souza, D.; Magalhães, R.D.M.; Diniz, J.L.C.P.; Costa, L.E.; Fumagalli, M.A.C.; Lage, P.S.; Bartholomeu, D.C.; Alves, M.J.M.; et al. Proteins Selected in Leishmania (Viannia) braziliensis by an Immunoproteomic Approach with Potential Serodiagnosis Applications for Tegumentary Leishmaniasis. Clin. Vaccine Immunol. 2015, 22, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, A.M.R.; Costa, L.E.; Salles, B.C.; Santos, T.T.; Ramos, F.F.; Lima, M.; Chávez-Fumagalli, M.A.; Silvestre, B.; Portela, S.; Roatt, B.; et al. An ELISA immunoassay employing a conserved Leishmania hypothetical protein for the serodiagnosis of visceral and tegumentary leishmaniasis in dogs and humans. Cell. Immunol. 2017, 318, 42–48. [Google Scholar] [CrossRef]
- Lima, M.P.; Costa, L.E.; Duarte, M.C.; Menezes-Souza, D.; Salles, B.C.S.; Santos, T.T.D.O.; Ramos, F.F.; Chávez-Fumagalli, M.A.; Kursancew, A.C.S.; Ambrósio, R.P.; et al. Evaluation of a hypothetical protein for serodiagnosis and as a potential marker for post-treatment serological evaluation of tegumentary leishmaniasis patients. Parasitol. Res. 2017, 116, 1197–1206. [Google Scholar] [CrossRef]
- Siriwardana, Y.D.; Deepachandi, B.; Ranasinghe, S.; Soysa, P.; Karunaweera, N. Evidence for seroprevalence in human localized cutaneous Leishmaniasis caused by Leishmania donovani in Sri Lanka. BioMed Res. Int. 2018, 2018, 9320367. [Google Scholar] [CrossRef] [Green Version]
- Deepachandi, B.; Weerasinghe, S.; Ranasinghe, S.; Andrahennadi, T.P.; Wickramanayake, M.N.; Siri, S.; Karunaweera, N.; Chandrasekharan, V.; Chatterjee, M.; Soysa, P.; et al. First Serological Study Revealing High Humoral Response and Evidence for Antigenic Heterogeneity in Leishmania donovani Induced CL in Sri Lanka. BioMed Res. Int. 2020, 2020, 1–11. [Google Scholar] [CrossRef]
- Siriwardana, Y.; Zhou, G.; Deepachandi, B.; Akarawita, J.; Wickremarathne, C.; Warnasuriya, W.; Udagedara, C.; Ranawaka, R.R.; Kahawita, I.; Ariyawansa, D.; et al. Trends in Recently Emerged Leishmania donovani Induced Cutaneous Leishmaniasis, Sri Lanka, for the First 13 Years. BioMed Res. Int. 2019, 2019, 4093603. [Google Scholar] [CrossRef]
- Akagi, H.; Hussain, S.M.; Hashiguchi, Y.; Kimura, E.; Islam, M.; Itoh, M.; Ekram, A.R.M.S.; Islam, A.U. Production of recombinant kinesin-related protein of leishmania donovani and its application in the serodiagnosis of visceral leishmaniasis. Am. J. Trop. Med. Hyg. 2007, 76, 902–905. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.; Takesue, A.; Kimura, E.; Itoh, M.; Rahman, A.; Islam, A.U.; Ekram, A.R.M.S.; Hashiguchi, Y.; Takagi, H. Enzyme-linked immunosorbent assay to detect urinary antibody against recombinant rKRP42 antigen made from Leishmania donovani for the diagnosis of visceral leishmaniasis. Am. J. Trop. Med. Hyg. 2008, 79, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Karunaweera, N.D.; Ginige, S.; Senanayake, S.; Silva, H.; Manamperi, N.; Samaranayake, N.; Siriwardana, Y.; Gamage, D.; Senerath, U.; Zhou, G. Spatial Epidemiologic Trends and Hotspots of Leishmaniasis, Sri Lanka, 2001–2018. Emerg. Infect. Dis. 2020, 26, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Tai, N.; Osman, O.; El Fari, M.; Presber, W.; Schönian, G. Genetic heterogeneity of ribosomal internal transcribed spacer in clinical samples of Leishmania donovani spotted on filter paper as revealed by single-strand conformation polymorphisms and sequencing. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 575–579. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Cupolillo, E.; Grimaldi Jr, G.; Momen, H.; Beverley, S.M. Intergenic region typing (IRT): A rapid molecular approach to the characterization and evolution of Leishmania. Mol. Biochem. Parasitol. 1995, 73, 145–155. [Google Scholar] [CrossRef]
- Schönian, G.; Schnur, L.; El Fari, M.; Oskam, L.; Kolesnikov, A.A.; Sokolowska-Köhler, W.; Presber, W. Genetic heterogeneity in the species Leishmania tropica revealed by different PCR-based methods. Trans. R. Soc. Trop. Med. Hyg. 2001, 95, 217–224. [Google Scholar] [CrossRef]
- Koarashi, Y.; Cáceres, A.G.; Saca, F.M.Z.; Flores, E.E.P.; Trujillo, A.C.; Alvares, J.L.A.; Yoshimatsu, K.; Arikawa, J.; Katakura, K.; Hashiguchi, Y.; et al. Identification of causative Leishmania species in Giemsa-stained smears prepared from patients with cutaneous leishmaniasis in Peru using PCR-RFLP. Acta Trop. 2016, 158, 83–87. [Google Scholar] [CrossRef]
- Ranasinghe, S.; Wickremasinghe, R.; Hulangamuwa, S.; Sirimanna, G.; Opathella, N.; Maingon, R.D.; Chandrasekharan, V. Polymerase chain reaction detection of LeishmaniaDNA in skin biopsy samples in Sri Lanka where the causative agent of cutaneous leishmaniasis is Leishmania donovani. Mem. Inst. Oswaldo Cruz. 2015, 110, 1017–1023. [Google Scholar] [CrossRef] [Green Version]
- Sharma, U.; Singh, S. Immunobiology of leishmaniasis. Indian J. Exp. Biol. 2009, 47, 412–423. [Google Scholar] [PubMed]
- Nakkash, H.; Makki, R.; Nahhas, G.; Knio, K.; Nuwayri-Salti, N. Detection of Leishmania parasites in the blood of patients with isolated cutaneous leishmaniasis. Int. J. Infect. Dis. 2011, 15, e491–e494. [Google Scholar] [CrossRef] [Green Version]
- Fagundes-Silva, G.; Vieira-Gonçalves, R.; Nepomuceno, M.; De Souza, M.; Favoret, S., Jr.; Oliveira-Neto, M.; Da-Cruz, A.; Gomes-Silva, A. Decrease in anti-Leishmania IgG3 and IgG1 after cutaneous leishmaniasis lesion healing is correlated with the time of clinical cure. Parasite Immunol. 2012, 34, 486–491. [Google Scholar] [CrossRef]
- Rodriguez, V.; Centeno, M.; Ulrich, M. The IgG isotypes of specific antibodies in patients with American cutaneous leishmaniasis; relationship to the cell-mediated immune response. Parasite Immunol. 1996, 18, 341–345. [Google Scholar] [CrossRef]
- Ozbılge, H.; Aksoy, N.; Gurel, M.S.; Yazar, S. IgG and IgG subclass antibodies in patients with active cutaneous leishmaniasis. J. Med. Microbiol. 2006, 55, 1329–1331. [Google Scholar] [CrossRef] [Green Version]
- Al-Qadhi, B.N.; Musa, I.S.; Hummadi, Y.M.K.A.-M. Comparative immune study on cutaneous leishmaniasis patients with single and multiple sores. J. Parasit. Dis. 2013, 39, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, R.L. Leishmania tropica (Kinetoplastida: Trypanosomatidae)—A perplexing parasite. Folia Parasitol. 2003, 50, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Magalhães, A.; Carvalho, L.P.; Costa, R.; Pita, M.S.; Cardoso, T.M.; Machado, P.R.; Carvalho, E.M.; Arruda, S.; Carvalho, A.M. Anti-Leishmania IgG is a marker of disseminated leishmaniasis caused by Leishmania braziliensis. Int. J. Infect. Dis. 2021, 106, 83–90. [Google Scholar] [CrossRef]
- Despommier, D.D.; Gwadz, R.W.; Hotez, P.J. Leishmania braziliensis (Vianna 1911). In Parasitic Diseases; Springer Science and Business Media LLC: New York, NY, USA, 1995; pp. 209–213. [Google Scholar]
- Figueira, C.P.; Carvalhal, D.G.F.; Almeida, R.A.; Hermida, M.D.E.-R.; Touchard, M.; Robert, P.; Pierres, A.; Bongrand, P.; Dos-Santos, W.L. Leishmania infection modulates beta-1 integrin activation and alters the kinetics of monocyte spreading over fibronectin. Sci. Rep. 2015, 5, 12862. [Google Scholar] [CrossRef] [Green Version]
- Miles, S.A.; Conrad, S.M.; Alves, R.G.; Jeronimo, S.; Mosser, D.M. A role for IgG immune complexes during infection with the intracellular pathogen Leishmania. J. Exp. Med. 2005, 201, 747–754. [Google Scholar] [CrossRef]
- Antonelli, L.; Dutra, W.O.; Almeida, R.P.; Bacellar, O.; Carvalho, E.M.; Gollob, K.J. Activated inflammatory T cells correlate with lesion size in human cutaneous leishmaniasis. Immunol. Lett. 2005, 101, 226–230. [Google Scholar] [CrossRef]
- Oliveira, F.; Bafica, A.; Rosato, A.B.; Favali, C.B.F.; Costa, J.M.; Cafe, V.; Netto, M.B.; Barral, A. Lesion Size Correlates with Leishmania Antigen-Stimulated TNF-Levels in Human Cutaneous Leishmaniasis. Am. J. Trop. Med. Hyg. 2011, 85, 70–73. [Google Scholar] [CrossRef]
- Davies, C.R.; Gavgani, A.S.M. Age, acquired immunity and the risk of visceral leishmaniasis: A prospective study in Iran. Parasitology 1999, 119, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Boggild, A.K.; Veland, N.; Miranda-Verastegui, C.; Ramos, A.P.; Valencia, B.M.; Llanos-Cuentas, A.; Low, D.E.; Arevalo, J.; Espinosa, D.A. Clinical and Demographic Stratification of Test Performance: A Pooled Analysis of Five Laboratory Diagnostic Methods for American Cutaneous Leishmaniasis. Am. J. Trop. Med. Hyg. 2010, 83, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Wijesinghe, H.; Gunathilaka, N.; Semege, S.; Pathirana, N.; Manamperi, N.; De Silva, C.; Fernando, D. Histopathology of Cutaneous Leishmaniasis Caused by Leishmania donovani in Sri Lanka. BioMed Res. Int. 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, S.F.G.; Dietze, R.; Lemos, E.M.; Corey, R. Performance of recombinant k39 antigen in the diagnosis of brazilian visceral leishmaniasis. Am. J. Trop. Med. Hyg. 2003, 68, 321–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartzell, J.D.; Weina, P.J.; Wortmann, G.W.; Yadava, A.; Aronson, N.E.; Howard, R.S. Positive rK39 serologic assay results in US servicemen with cutaneous leishmaniasis. Am. J. Trop. Med. Hyg. 2008, 79, 843–846. [Google Scholar] [CrossRef]
- Sharma, N.L.; Mahajan, V.K.; Negi, A.K.; Verma, G.K. The rK39 immunochromatic dipstick testing: A study for K39 seroprevalence in dogs and human leishmaniasis patients for possible animal reservoir of cutaneous and visceral leishmaniasis in endemic focus of Satluj river valley of Himachal Pradesh (India). Indian J. Dermatol. Venereol. Leprol. 2009, 75, 52–55. [Google Scholar] [CrossRef]
- Kumar, R.; Bumb, R.A.; Salotra, P. Correlation of parasitic load with interleukin-4 response in patients with cutaneous leishmaniasis due toLeishmania tropica. FEMS Immunol. Med. Microbiol. 2009, 57, 239–246. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.; Ekram, A.R.M.S.; Kimura, E.; Takagi, H.; Islam, A.U.; Hashiguchi, Y.; Rahman, A.; Itoh, M.; Takesue, A. ELISA with Recombinant rKRP42 Antigen Using Urine Samples: A Tool for Predicting Clinical Visceral Leishmaniasis Cases and Its Outbreak. Am. J. Trop. Med. Hyg. 2012, 87, 658–662. [Google Scholar] [CrossRef] [Green Version]
- Franssen, S.U.; Durrant, C.; Stark, O.; Moser, B.; Downing, T.; Imamura, H.; Dujardin, J.-C.; Sanders, M.J.; Mauricio, I.; Miles, M.A.; et al. Global genome diversity of the Leishmania donovani complex. eLife 2020, 9. [Google Scholar] [CrossRef]
- Lypaczewski, P.; Matlashewski, G. Leishmania donovani hybridisation and introgression in nature: A comparative genomic investigation. Lancet Microbe 2021, 2, e250–e258. [Google Scholar] [CrossRef]
- Bailey, S.M.; Lockwood, D.N. Cutaneous leishmaniasis. Clin. Dermatol. 2007, 25, 203–211. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number (%) | |
|---|---|---|
| Clinical diagnosis | Confirmed | 173 (91.0) |
| Doubtful | 17 (9.0) | |
| Gender | Female | 75 (39.0) |
| Male | 115 (61.0) | |
| Age | <40 years | 73 (38.4) |
| 41–60 years | 87 (45.8) | |
| >61 years | 30 (15.8) | |
| Occupation | Occupied | 132 (69.5) |
| Unoccupied | 58 (30.5) | |
| Income (LKR)) | <30,000 | 92 (48.4) |
| 30,000–50,000 | 76 (40.0) | |
| 50,000–100,000 | 16 (8.4) | |
| >100,000 | 6 (3.2) | |
| Lesion duration | < = 4 months | 127 (67.0) |
| 4–12 months | 52 (27.4) | |
| >12 months | 11 (5.8) | |
| Number of lesions | Single | 153 (80.5) |
| Multiple | 37 (19.5) | |
| Size | <2 cm | 165 (86.8) |
| >2 cm | 25 (13.2) | |
| Nature of the lesion | Papule | 23 (12.1) |
| Nodule | 32 (16.8) | |
| Ulcerated nodule | 76 (40.0) | |
| Dry ulcer | 26 (13.7) | |
| Wet ulcer | 14 (7.4) | |
| Plaque | 19 (10.0) | |
| Site | On limbs | 163 (85.8) |
| Elsewhere | 27 (14.2) |
| Clinical CL | Confirmed CL | Japanese Controls | |
|---|---|---|---|
| Total | 190 | 180 | 80 |
| Positives | 175 | 170 | 0 |
| Positive % | 92.1 | 94.4 | 0.0 |
| Clinical CL | Confirmed CL | Endemic Controls | Japanese Controls | |
|---|---|---|---|---|
| Total | 190 | 180 | 255 | 80 |
| Positives | 116 | 111 | 83 | 3 |
| Positive % | 61.1 | 61.7 | 32.5 | 3.75 |
| Test | Positive n (%) | Negative n (%) | p-Value ¥ | Sn (PPV) δ | Sp (NPV) δ |
|---|---|---|---|---|---|
| SSS (technician) | 5 (29.4) | 12 (70.6) | 1.000 | 25% (80%) | 0% (0%) |
| SSS (authors) | 10 (58.8) | 7 (41.2) | 0.083 | 62.5% (100%) | 100% (14.3%) |
| PCR | 16 (94.1) | 1 (5.9) | 0.0001 * | - | - |
| rKRP42 serum ELISA | 15 (88.2) | 2 (11.8) | 0.0006 * | 93.8% (100%) | 100% (50%) |
| Combination of SSS ₶ and rKRP42 Serum ELISA | 16 (94.1) | 1 (5.9) | 0.0001 * | 100% (100%) | 100% (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Silva, N.L.; De Silva, V.N.H.; Deerasinghe, A.T.H.; Rathnapala, U.L.; Kato, H.; Itoh, M.; Takagi, H.; Weerasooriya, M.V.; Yahathugoda, T.C. Validation of an In-House ELISA Method in the Diagnosis of Cutaneous Leishmaniasis Caused by Leishmania donovani in Hambantota District, Sri Lanka. Microorganisms 2022, 10, 921. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10050921
De Silva NL, De Silva VNH, Deerasinghe ATH, Rathnapala UL, Kato H, Itoh M, Takagi H, Weerasooriya MV, Yahathugoda TC. Validation of an In-House ELISA Method in the Diagnosis of Cutaneous Leishmaniasis Caused by Leishmania donovani in Hambantota District, Sri Lanka. Microorganisms. 2022; 10(5):921. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10050921
Chicago/Turabian StyleDe Silva, Nirmitha Lalindi, Viraji Nefertiti Hiromel De Silva, Arachchige Theja Hemapala Deerasinghe, Upeksha Lakmini Rathnapala, Hirotomo Kato, Makoto Itoh, Hidekazu Takagi, Mirani Vasanthamala Weerasooriya, and Thishan Channa Yahathugoda. 2022. "Validation of an In-House ELISA Method in the Diagnosis of Cutaneous Leishmaniasis Caused by Leishmania donovani in Hambantota District, Sri Lanka" Microorganisms 10, no. 5: 921. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10050921