
Time to Positivity in Blood Culture Bottles Inoculated with Sonication Fluid from Fracture-Related Infections
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection and Microbiological Methods
2.3. Outcome Parameters
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Microbiological Findings
3.2.1. Pathogen Spectrum
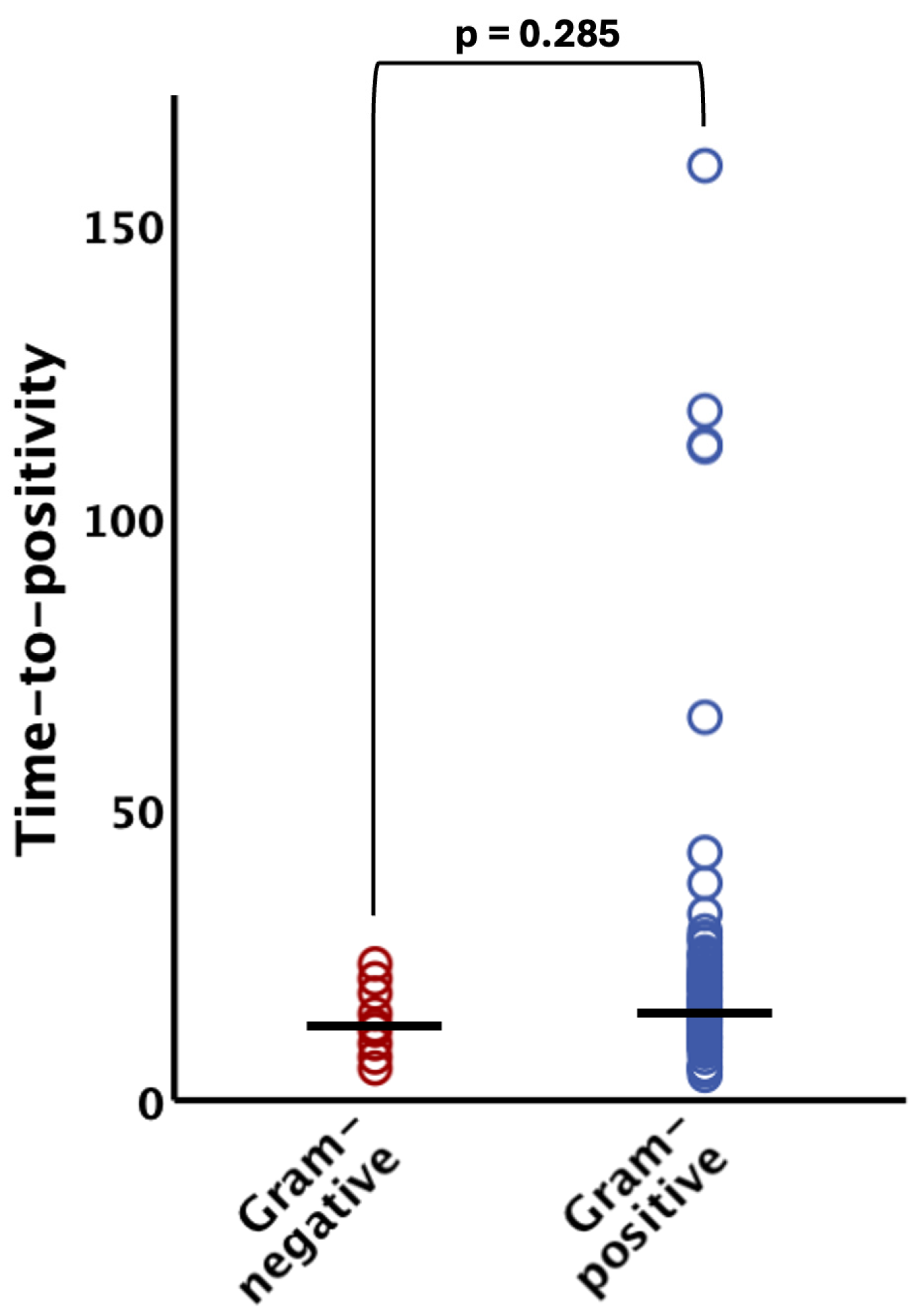
3.2.2. Time to Positivity
4. Discussion
- Positive bacterial detection was achieved in 78.7% by incubation of sonication fluids into blood culture bottles in FRI cases and bacteria could be evidenced within 24 h in 87.7% of culture-positive cases.
- Streptococcus species, Staphylococcus aureus, and Gram-negative bacteria exhibited the shortest time to positivity (TTP) in our cohort, with 100% of these microorganisms being detected within 48 h after inoculation.
- Only Cutibacterium acnes and certain coagulase-negative Staphylococci were identified after more than 72 h
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Iliaens, J.; Onsea, J.; Hoekstra, H.; Nijs, S.; Peetermans, W.E.; Metsemakers, W.-J. Fracture-Related Infection in Long Bone Fractures: A Comprehensive Analysis of the Economic Impact and Influence on Quality of Life. Injury 2021, 52, 3344–3349. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.-J.; Smeets, B.; Nijs, S.; Hoekstra, H. Infection after Fracture Fixation of the Tibia: Analysis of Healthcare Utilization and Related Costs. Injury 2017, 48, 1204–1210. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.; Rupp, M.; Lang, S.; Alt, V. The Epidemiology of Fracture-Related Infections in Germany. Sci. Rep. 2021, 11, 10443. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-Related Infection: A Consensus on Definition from an International Expert Group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Govaert, G.A.M.; Kuehl, R.; Atkins, B.L.; Trampuz, A.; Morgenstern, M.; Obremskey, W.T.; Verhofstad, M.H.J.; McNally, M.A.; Metsemakers, W.-J.; Fracture-Related Infection (FRI) Consensus Group. Diagnosing Fracture-Related Infection: Current Concepts and Recommendations. J. Orthop. Trauma 2020, 34, 8–17. [Google Scholar] [CrossRef] [PubMed]
- de Mesy Bentley, K.L.; Trombetta, R.; Nishitani, K.; Bello-Irizarry, S.N.; Ninomiya, M.; Zhang, L.; Chung, H.L.; McGrath, J.L.; Daiss, J.L.; Awad, H.A.; et al. Evidence of Staphylococcus aureus Deformation, Proliferation, and Migration in Canaliculi of Live Cortical Bone in Murine Models of Osteomyelitis. J. Bone Miner. Res. 2017, 32, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Hofstee, M.I.; Riool, M.; Terjajevs, I.; Thompson, K.; Stoddart, M.J.; Richards, R.G.; Zaat, S.A.J.; Moriarty, T.F. Three-Dimensional In Vitro Staphylococcus aureus Abscess Communities Display Antibiotic Tolerance and Protection from Neutrophil Clearance. Infect. Immun. 2020, 88, e00293-20. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, W.; Sommer, U.; Sethi, S.; Domann, E.; Thormann, U.; Schütz, I.; Lips, K.S.; Chakraborty, T.; Schnettler, R.; Alt, V. Intracellular Proliferation of S. aureus in Osteoblasts and Effects of Rifampicin and Gentamicin on S. Aureus Intracellular Proliferation and Survival. Eur. Cells Mater. 2014, 28, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Yano, M.H.; Klautau, G.B.; da Silva, C.B.; Nigro, S.; Avanzi, O.; Mercadante, M.T.; Salles, M.J.C. Improved Diagnosis of Infection Associated with Osteosynthesis by Use of Sonication of Fracture Fixation Implants. J. Clin. Microbiol. 2014, 52, 4176–4182. [Google Scholar] [CrossRef]
- Zhai, Z.; Li, H.; Qin, A.; Liu, G.; Liu, X.; Wu, C.; Li, H.; Zhu, Z.; Qu, X.; Dai, K. Meta-Analysis of Sonication Fluid Samples from Prosthetic Components for Diagnosis of Infection after Total Joint Arthroplasty. J. Clin. Microbiol. 2014, 52, 1730–1736. [Google Scholar] [CrossRef]
- Trampuz, A.; Piper, K.E.; Jacobson, M.J.; Hanssen, A.D.; Unni, K.K.; Osmon, D.R.; Mandrekar, J.N.; Cockerill, F.R.; Steckelberg, J.M.; Greenleaf, J.F.; et al. Sonication of Removed Hip and Knee Prostheses for Diagnosis of Infection. N. Engl. J. Med. 2007, 357, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Portillo, M.E.; Salvadó, M.; Trampuz, A.; Siverio, A.; Alier, A.; Sorli, L.; Martínez, S.; Pérez-Prieto, D.; Horcajada, J.P.; Puig-Verdie, L. Improved Diagnosis of Orthopedic Implant-Associated Infection by Inoculation of Sonication Fluid into Blood Culture Bottles. J. Clin. Microbiol. 2015, 53, 1622–1627. [Google Scholar] [CrossRef]
- Tarabichi, S.; Goh, G.S.; Zanna, L.; Qadiri, Q.S.; Baker, C.M.; Gehrke, T.; Citak, M.; Parvizi, J. Time to Positivity of Cultures Obtained for Periprosthetic Joint Infection. J. Bone Jt. Surg. Am. 2023, 105, 107–112. [Google Scholar] [CrossRef]
- Talsma, D.T.; Ploegmakers, J.J.W.; Jutte, P.C.; Kampinga, G.; Wouthuyzen-Bakker, M. Time to Positivity of Acute and Chronic Periprosthetic Joint Infection Cultures. Diagn. Microbiol. Infect. Dis. 2021, 99, 115178. [Google Scholar] [CrossRef]
- Tamma, P.D.; Avdic, E.; Li, D.X.; Dzintars, K.; Cosgrove, S.E. Association of Adverse Events With Antibiotic Use in Hospitalized Patients. JAMA Intern. Med. 2017, 177, 1308–1315. [Google Scholar] [CrossRef]
- Hamilton, F.; Evans, R.; Ghazal, P.; MacGowan, A. Time to Positivity in Bloodstream Infection Is Not a Prognostic Marker for Mortality: Analysis of a Prospective Multicentre Randomized Control Trial. Clin. Microbiol. Infect. 2022, 28, 136.e7–136.e13. [Google Scholar] [CrossRef]
- Hsieh, Y.-C.; Chen, H.-L.; Lin, S.-Y.; Chen, T.-C.; Lu, P.-L. Short Time to Positivity of Blood Culture Predicts Mortality and Septic Shock in Bacteremic Patients: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2022, 22, 142. [Google Scholar] [CrossRef]
- Siméon, S.; Le Moing, V.; Tubiana, S.; Duval, X.; Fournier, D.; Lavigne, J.-P.; Erpelding, M.-L.; Gustave, C.-A.; Desage, S.; Chirouze, C.; et al. Time to Blood Culture Positivity: An Independent Predictor of Infective Endocarditis and Mortality in Patients with Staphylococcus aureus Bacteraemia. Clin. Microbiol. Infect. 2019, 25, 481–488. [Google Scholar] [CrossRef]
- Peng, G.; Liu, Q.; Guan, Z.; Liu, M.; Sun, X.; Zhu, X.; Chen, J.; Feng, W.; Li, J.; Zeng, J.; et al. Diagnostic Accuracy of Sonication Fluid Cultures from Prosthetic Components in Periprosthetic Joint Infection: An Updated Diagnostic Meta-Analysis. J. Orthop. Surg. Res. 2023, 18, 175. [Google Scholar] [CrossRef] [PubMed]
- Onsea, J.; Depypere, M.; Govaert, G.; Kuehl, R.; Vandendriessche, T.; Morgenstern, M.; McNally, M.; Trampuz, A.; Metsemakers, W.-J. Accuracy of Tissue and Sonication Fluid Sampling for the Diagnosis of Fracture-Related Infection: A Systematic Review and Critical Appraisal. J. Bone Jt. Infect. 2018, 3, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Peel, T.N.; Dylla, B.L.; Hughes, J.G.; Lynch, D.T.; Greenwood-Quaintance, K.E.; Cheng, A.C.; Mandrekar, J.N.; Patel, R. Improved Diagnosis of Prosthetic Joint Infection by Culturing Periprosthetic Tissue Specimens in Blood Culture Bottles. mBio 2016, 7, e01776-15. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Govaert, G.; Dudareva, M.; Morgenstern, M.; Metsemakers, W.-J. Definition and Diagnosis of Fracture-Related Infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Podleska, L.E.; Lendemans, S.; Schmid, E.; Hussmann, B.; Nast-Kolb, D.; Taeger, G. Sample Taking during Orthopedic Surgery: Sensitivity and Specificity Using the BACTEC Blood Culture System. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Minassian, A.M.; Newnham, R.; Kalimeris, E.; Bejon, P.; Atkins, B.L.; Bowler, I.C. Use of an Automated Blood Culture System (BD BACTECTM) for Diagnosis of Prosthetic Joint Infections: Easy and Fast. BMC Infect. Dis. 2014, 14, 233. [Google Scholar] [CrossRef] [PubMed]
- Kummer, F.; Hergan, D.J.; Thut, D.C.; Pahk, B.; Jazrawi, L.M. Suture Loosening and Its Effect on Tendon Fixation in Knotless Double-Row Rotator Cuff Repairs. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Depypere, M.; Kuehl, R.; Metsemakers, W.-J.; Senneville, E.; McNally, M.A.; Obremskey, W.T.; Zimmerli, W.; Atkins, B.L.; Trampuz, A. Recommendations for Systemic Antimicrobial Therapy in Fracture-Related Infection: A Consensus From an International Expert Group. J. Orthop. Trauma 2020, 34, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.-J.; Morgenstern, M.; Senneville, E.; Borens, O.; Govaert, G.A.M.; Onsea, J.; Depypere, M.; Richards, R.G.; Trampuz, A.; Verhofstad, M.H.J.; et al. General Treatment Principles for Fracture-Related Infection: Recommendations from an International Expert Group. Arch. Orthop. Trauma Surg. 2020, 140, 1013–1027. [Google Scholar] [CrossRef]
- Hellebrekers, P.; Verhofstad, M.H.J.; Leenen, L.P.H.; Varol, H.; van Lieshout, E.M.M.; Hietbrink, F. The Effect of Early Broad-Spectrum versus Delayed Narrow-Spectrum Antibiotic Therapy on the Primary Cure Rate of Acute Infection after Osteosynthesis. Eur. J. Trauma Emerg. Surg. 2020, 46, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.D.; Heintz, B.H.; Mosher, H.J.; Livorsi, D.J.; Egge, J.A.; Lund, B.C. Risk of Acute Kidney Injury and Clostridioides Difficile Infection With Piperacillin/Tazobactam, Cefepime, and Meropenem With or Without Vancomycin. Clin. Infect. Dis. 2021, 73, e1579–e1586. [Google Scholar] [CrossRef]
- Baertl, S.; Walter, N.; Engelstaedter, U.; Ehrenschwender, M.; Hitzenbichler, F.; Alt, V.; Rupp, M. What Is the Most Effective Empirical Antibiotic Treatment for Early, Delayed, and Late Fracture-Related Infections? Antibiotics 2022, 11, 287. [Google Scholar] [CrossRef]
- Lambregts, M.M.C.; Bernards, A.T.; van der Beek, M.T.; Visser, L.G.; de Boer, M.G. Time to Positivity of Blood Cultures Supports Early Re-Evaluation of Empiric Broad-Spectrum Antimicrobial Therapy. PLoS ONE 2019, 14, e0208819. [Google Scholar] [CrossRef] [PubMed]
- Puerta-Alcalde, P.; Cardozo, C.; Suárez-Lledó, M.; Rodríguez-Núñez, O.; Morata, L.; Fehér, C.; Marco, F.; Del Río, A.; Martínez, J.A.; Mensa, J.; et al. Current Time-to-Positivity of Blood Cultures in Febrile Neutropenia: A Tool to Be Used in Stewardship de-Escalation Strategies. Clin. Microbiol. Infect. 2019, 25, 447–453. [Google Scholar] [CrossRef]
- Haimi-Cohen, Y.; Vellozzi, E.M.; Rubin, L.G. Initial Concentration of Staphylococcus Epidermidis in Simulated Pediatric Blood Cultures Correlates with Time to Positive Results with the Automated, Continuously Monitored BACTEC Blood Culture System. J. Clin. Microbiol. 2002, 40, 898–901. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, R.; Tschudin-Sutter, S.; Morgenstern, M.; Dangel, M.; Egli, A.; Nowakowski, A.; Suhm, N.; Theilacker, C.; Widmer, A.F. Time-Dependent Differences in Management and Microbiology of Orthopaedic Internal Fixation-Associated Infections: An Observational Prospective Study with 229 Patients. Clin. Microbiol. Infect. 2019, 25, 76–81. [Google Scholar] [CrossRef]
- Kim, J.; Gregson, D.B.; Ross, T.; Laupland, K.B. Time to Blood Culture Positivity in Staphylococcus aureus Bacteremia: Association with 30-Day Mortality. J. Infect. 2010, 61, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.D.; Dash, S.; Cantey, J.R.; Marculescu, C.E. Higher Risk of Failure of Methicillin-Resistant Staphylococcus aureus Prosthetic Joint Infections. Clin. Orthop. Relat. Res. 2007, 461, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, M.; Erichsen, C.; Militz, M.; Xie, Z.; Peng, J.; Stannard, J.; Metsemakers, W.-J.; Schaefer, D.; Alt, V.; Søballe, K.; et al. The AO Trauma CPP Bone Infection Registry: Epidemiology and Outcomes of Staphylococcus aureus Bone Infection. J. Orthop. Res. 2021, 39, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Yong, T.M.; Rackard, F.A.; Dutton, L.K.; Sparks, M.B.; Harris, M.B.; Gitajn, I.L. Analyzing Risk Factors for Treatment Failure in Fracture-Related Infection. Arch. Orthop. Trauma Surg. 2023, 143, 1387–1392. [Google Scholar] [CrossRef]
- Kandel, C.E.; Jenkinson, R.; Daneman, N.; Backstein, D.; Hansen, B.E.; Muller, M.P.; Katz, K.C.; Widdifield, J.; Bogoch, E.; Ward, S.; et al. Predictors of Treatment Failure for Hip and Knee Prosthetic Joint Infections in the Setting of 1- and 2-Stage Exchange Arthroplasty: A Multicenter Retrospective Cohort. Open Forum Infect. Dis. 2019, 6, ofz452. [Google Scholar] [CrossRef]
- Ma, C.-Y.; Lu, Y.-D.; Bell, K.L.; Wang, J.-W.; Ko, J.-Y.; Wang, C.-J.; Kuo, F.-C. Predictors of Treatment Failure After 2-Stage Reimplantation for Infected Total Knee Arthroplasty: A 2- to 10-Year Follow-Up. J. Arthroplast. 2018, 33, 2234–2239. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Tornero, E.; Claret, G.; Bosch, J.; Martinez-Pastor, J.C.; Combalia, A.; Soriano, A. Withholding Preoperative Antibiotic Prophylaxis in Knee Prosthesis Revision: A Retrospective Analysis on Culture Results and Risk of Infection. J. Arthroplast. 2017, 32, 2829–2833. [Google Scholar] [CrossRef] [PubMed]
- Bedenčič, K.; Kavčič, M.; Faganeli, N.; Mihalič, R.; Mavčič, B.; Dolenc, J.; Bajc, Z.; Trebše, R. Does Preoperative Antimicrobial Prophylaxis Influence the Diagnostic Potential of Periprosthetic Tissues in Hip or Knee Infections? Clin. Orthop. Relat. Res. 2016, 474, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Prieto, D.; Portillo, M.E.; Puig-Verdié, L.; Alier, A.; Gamba, C.; Guirro, P.; Martínez-Díaz, S.; Horcajada, J.P.; Trampuz, A.; Monllau, J.C. Preoperative Antibiotic Prophylaxis in Prosthetic Joint Infections: Not a Concern for Intraoperative Cultures. Diagn. Microbiol. Infect. Dis. 2016, 86, 442–445. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age (years) | 57.0 ± 17.4 |
| Sex | |
| Male | 86 (68.3%) |
| Female | 40 (31.7%) |
| Comorbidities | |
| Diabetes mellitus | 18 (11.6%) |
| PAOD | 14 (9.0%) |
| Affected bone | |
| Tibia | 51 (40.5%) |
| Foot | 28 (22.2%) |
| Femur | 15 (11.9%) |
| Spine | 9 (7.1%) |
| Fibula | 7 (5.6%) |
| Humerus | 7 (5.6%) |
| Forearm | 5 (4.0%) |
| Pelvis/Hip | 5 (4.0%) |
| Detected Pathogens | Number of Patients (%) | |
|---|---|---|
| Gram-positive bacteria | ||
| S. aureus | ||
| MSSA | 49 (40.2%) | |
| MRSA | 3 (2.5%) | |
| S. epidermidis | 27 (22.1%) | |
| Other Staphylococcus spp. | 17 (13.9%) | |
| S. hominis | 7 (5.7%) | |
| S. warneri | 2 (1.6%) | |
| S. haemolyticus | 2 (1.6%) | |
| S. pettenkoferi | 1 (0.8%) | |
| S. caprae | 1 (0.8%) | |
| S. pseudointermedius | 1 (0.8%) | |
| S. capitis | 1 (0.8%) | |
| S. arlettae | 1 (0.8%) | |
| S. lugdunensis | 1 (0.8%) | |
| Streptococcus spp. | ||
| S. dysgalactiae | 9 (7.4%) | |
| S. agalactiae | 2 (1.6%) | |
| S. pyogenes | 1 (0.8%) | |
| Alpha-haemolytic | 1 (0.8%) | |
| Enterococcus spp. | 26 (21.3%) | |
| Cutibacterium spp. | 2 (1.6%) | |
| Others | 6 (4.9%) | |
| Gram-negative bacteria | ||
| Pseudomonas aeruginosa | 6 (4.9%) | |
| Proteus spp. | 5 (4.1%) | |
| E. coli | 4 (3.3%) | |
| Enterobacter spp. | 4 (3.3%) | |
| Klebsiella spp. | 3 (2.5%) | |
| Morganella spp. | 3 (2.5%) | |
| Serratia spp. | 3 (2.5%) | |
| Sphingomonas spp. | 1 (0.8%) |
| Spinal Rods (n = 6) | IMN (n = 15) | Screws (n = 94) | Plates (n = 44) | PMMA (n = 4) | |
|---|---|---|---|---|---|
| PED | 8.0 (IQR 7.4–9.3) | 12.2 (IQR 7.4–18.5) | 12.5 (IQR 9.3–17.1) | 13.1 (IQR 9.8–20.2) | 21.7 (IQR 7.1–24.7) |
| anaerobic | 11.2 (IQR 8.3–21.6) | 10.9 (IQR 7.3–16.1) | 12.1 (IQR 10.1–19.1) | 14.2 (IQR 10.5–19.6) | 26.2 (IQR 22.1–112.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henssler, L.; Schellenberger, L.; Baertl, S.; Klute, L.; Heyd, R.; Kerschbaum, M.; Alt, V.; Popp, D. Time to Positivity in Blood Culture Bottles Inoculated with Sonication Fluid from Fracture-Related Infections. Microorganisms 2024, 12, 862. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms12050862
Henssler L, Schellenberger L, Baertl S, Klute L, Heyd R, Kerschbaum M, Alt V, Popp D. Time to Positivity in Blood Culture Bottles Inoculated with Sonication Fluid from Fracture-Related Infections. Microorganisms. 2024; 12(5):862. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms12050862
Chicago/Turabian StyleHenssler, Leopold, Lena Schellenberger, Susanne Baertl, Lisa Klute, Robert Heyd, Maximilian Kerschbaum, Volker Alt, and Daniel Popp. 2024. "Time to Positivity in Blood Culture Bottles Inoculated with Sonication Fluid from Fracture-Related Infections" Microorganisms 12, no. 5: 862. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms12050862