Efficacy of Helicobacter pylori Eradication Therapy on Platelet Recovery in Pediatric Immune Thrombocytopenic Purpura-Case Series and a Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Diagnosis of H. Pylori Infection, and Eradication Therapy
2.3. Assessment of Treatment Efficacy
2.4. Systematic Review
2.4.1. Defining the Clinical Question
2.4.2. Identification of Evidence
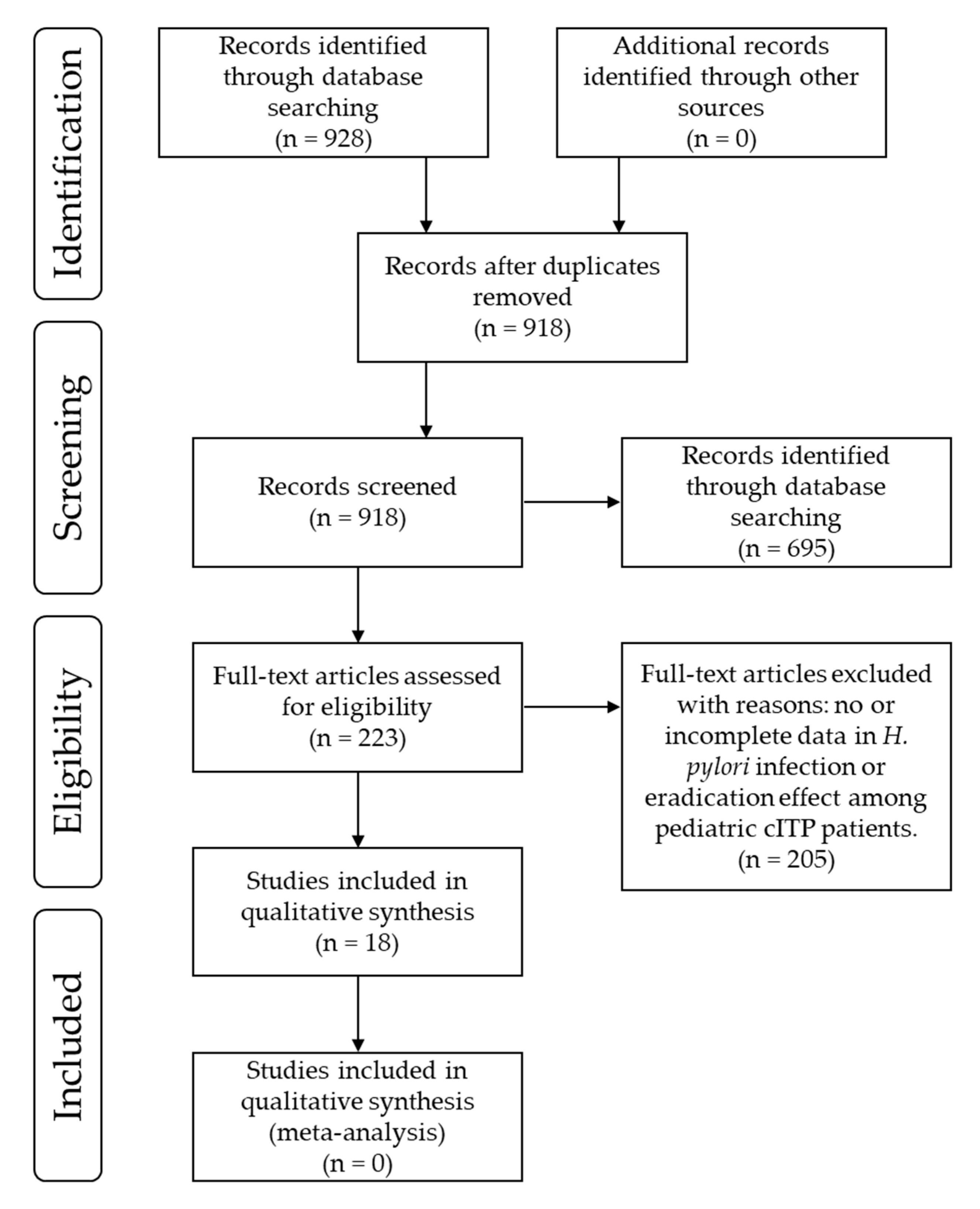
2.4.3. Study Selection
2.4.4. Data Extraction
2.4.5. Study Quality Assessment
3. Results
3.1. Retrospective Analysis
3.2. Remission Case Report
3.3. Systematic Review
3.3.1. Study Selection and Characteristics of Included Studies
3.3.2. Risk of Bias
3.3.3. The Prevalence of H. Pylori Infection and Platelet Response Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fox, J.G.; Wang, T.C. Inflammation, atrophy, and gastric cancer. J. Clin. Investig. 2007, 117, 60–69. [Google Scholar] [CrossRef]
- Franceschi, F.; Zuccala, G.; Roccarina, D.; Gasbarrini, A. Clinical effects of Helicobacter pylori outside the stomach. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 234–242. [Google Scholar] [CrossRef]
- Goni, E.; Franceschi, F. Helicobacter pylori and extragastric diseases. Helicobacter 2016, 21 (Suppl. S1), 45–48. [Google Scholar] [CrossRef]
- Rodeghiero, F.; Stasi, R.; Gernsheimer, T.; Michel, M.; Provan, D.; Arnold, D.M.; Bussel, J.B.; Cines, D.B.; Chong, B.H.; Cooper, N.; et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from an international working group. Blood 2009, 113, 2386–2393. [Google Scholar] [CrossRef]
- George, J.N.; Woolf, S.H.; Raskob, G.E.; Wasser, J.S.; Aledort, L.M.; Ballem, P.J.; Blanchette, V.S.; Bussel, J.B.; Cines, D.B.; Kelton, J.G.; et al. Idiopathic thrombocytopenic purpura: A practice guideline developed by explicit methods for the American Society of Hematology. Blood 1996, 88, 3–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neylon, A.J.; Saunders, P.W.; Howard, M.R.; Proctor, S.J.; Taylor, P.R. Clinically significant newly presenting autoimmune thrombocytopenic purpura in adults: A prospective study of a population-based cohort of 245 patients. Br. J. Haematol. 2003, 122, 966–974. [Google Scholar] [CrossRef] [Green Version]
- Kuhne, T.; Buchanan, G.R.; Zimmerman, S.; Michaels, L.A.; Kohan, R.; Berchtold, W.; Imbach, P. A prospective comparative study of 2540 infants and children with newly diagnosed idiopathic thrombocytopenic purpura (ITP) from the Intercontinental Childhood ITP Study Group. J. Pediatrics 2003, 143, 605–608. [Google Scholar] [CrossRef]
- Rosthoj, S.; Hedlund-Treutiger, I.; Rajantie, J.; Zeller, B.; Jonsson, O.G.; Elinder, G.; Wesenberg, F.; Henter, J.I. Duration and morbidity of newly diagnosed idiopathic thrombocytopenic purpura in children: A prospective Nordic study of an unselected cohort. J. Pediatrics 2003, 143, 302–307. [Google Scholar] [CrossRef]
- Donato, H.; Picon, A.; Martinez, M.; Rapetti, M.C.; Rosso, A.; Gomez, S.; Rossi, N.; Bacciedoni, V.; Schvartzman, G.; Riccheri, C.; et al. Demographic data, natural history, and prognostic factors of idiopathic thrombocytopenic purpura in children: A multicentered study from Argentina. Pediatric Blood Cancer 2009, 52, 491–496. [Google Scholar] [CrossRef]
- Imbach, P.; Kuhne, T.; Muller, D.; Berchtold, W.; Zimmerman, S.; Elalfy, M.; Buchanan, G.R. Childhood ITP: 12 months follow-up data from the prospective registry I of the Intercontinental Childhood ITP Study Group (ICIS). Pediatric Blood Cancer 2006, 46, 351–356. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Franceschi, F.; Tartaglione, R.; Landolfi, R.; Pola, P.; Gasbarrini, G. Regression of autoimmune thrombocytopenia after eradication of Helicobacter pylori. Lancet 1998, 352, 878. [Google Scholar] [CrossRef]
- Asahi, A.; Nishimoto, T.; Okazaki, Y.; Suzuki, H.; Masaoka, T.; Kawakami, Y.; Ikeda, Y.; Kuwana, M. Helicobacter pylori eradication shifts monocyte Fcgamma receptor balance toward inhibitory FcgammaRIIB in immune thrombocytopenic purpura patients. J. Clin. Investig. 2008, 118, 2939–2949. [Google Scholar] [CrossRef]
- Jarque, I.; Andreu, R.; Llopis, I.; De la Rubia, J.; Gomis, F.; Senent, L.; Jimenez, C.; Martin, G.; Martinez, J.A.; Sanz, G.F.; et al. Absence of platelet response after eradication of Helicobacter pylori infection in patients with chronic idiopathic thrombocytopenic purpura. Br. J. Haematol. 2001, 115, 1002–1003. [Google Scholar] [CrossRef]
- Kohda, K.; Kuga, T.; Kogawa, K.; Kanisawa, Y.; Koike, K.; Kuroiwa, G.; Hirayama, Y.; Sato, Y.; Niitsu, Y. Effect of Helicobacter pylori eradication on platelet recovery in Japanese patients with chronic idiopathic thrombocytopenic purpura and secondary autoimmune thrombocytopenic purpura. Br. J. Haematol. 2002, 118, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Ando, K.; Shimamoto, T.; Tauchi, T.; Ito, Y.; Kuriyama, Y.; Gotoh, A.; Miyazawa, K.; Kimura, Y.; Kawai, T.; Ohyashiki, K. Can eradication therapy for Helicobacter pylori really improve the thrombocytopenia in idiopathic thrombocytopenic purpura? Our experience and a literature review. Int. J. Hematol. 2003, 77, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Hashino, S.; Mori, A.; Suzuki, S.; Izumiyama, K.; Kahata, K.; Yonezumi, M.; Chiba, K.; Kondo, T.; Ota, S.; Toyashima, N.; et al. Platelet recovery in patients with idiopathic thrombocytopenic purpura after eradication of Helicobacter pylori. Int. J. Hematol. 2003, 77, 188–191. [Google Scholar] [CrossRef]
- Hino, M.; Yamane, T.; Park, K.; Takubo, T.; Ohta, K.; Kitagawa, S.; Higuchi, K.; Arakawa, T. Platelet recovery after eradication of Helicobacter pylori in patients with idiopathic thrombocytopenic purpura. Ann. Hematol. 2003, 82, 30–32. [Google Scholar] [CrossRef] [PubMed]
- Michel, M.; Cooper, N.; Jean, C.; Frissora, C.; Bussel, J.B. Does Helicobater pylori initiate or perpetuate immune thrombocytopenic purpura? Blood 2004, 103, 890–896. [Google Scholar] [CrossRef] [Green Version]
- Ando, T.; Tsuzuki, T.; Mizuno, T.; Minami, M.; Ina, K.; Kusugami, K.; Takamatsu, J.; Adachi, K.; El-Omar, E.; Ohta, M.; et al. Characteristics of Helicobacter pylori-induced gastritis and the effect of H. pylori eradication in patients with chronic idiopathic thrombocytopenic purpura. Helicobacter 2004, 9, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, K.; Kuwana, M.; Kurata, Y.; Imamura, M.; Harada, H.; Sakamaki, H.; Teramura, M.; Koda, K.; Nomura, S.; Sugihara, S.; et al. Is eradication therapy useful as the first line of treatment in Helicobacter pylori-positive idiopathic thrombocytopenic purpura? Analysis of 207 eradicated chronic ITP cases in Japan. Int. J. Hematol. 2005, 81, 162–168. [Google Scholar] [CrossRef]
- Stasi, R.; Rossi, Z.; Stipa, E.; Amadori, S.; Newland, A.C.; Provan, D. Helicobacter pylori eradication in the management of patients with idiopathic thrombocytopenic purpura. Am. J. Med. 2005, 118, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Yujiri, T.; Shinohara, K.; Inoue, Y.; Sato, Y.; Fujii, Y.; Okubo, M.; Zaitsu, Y.; Ariyoshi, K.; Nakamura, Y.; et al. Molecular mimicry by Helicobacter pylori CagA protein may be involved in the pathogenesis of H. pylori-associated chronic idiopathic thrombocytopenic purpura. Br. J. Haematol. 2004, 124, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Cruciani, M.; Mengoli, C.; Pizzolo, G.; Veneri, D. Effect of Helicobacter pylori eradication on platelet count in idiopathic thrombocytopenic purpura: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2007, 60, 237–246. [Google Scholar] [CrossRef]
- Satake, M.; Nishikawa, J.; Fukagawa, Y.; Akashi, K.; Okamoto, T.; Yoshida, T.; Hirano, A.; Maetani, N.; Iida, Y.; Sakaida, I. The long-term efficacy of Helicobacter pylori eradication therapy in patients with idiopathic thrombocytopenic purpura. J. Gastroenterol. Hepatol. 2007, 22, 2233–2237. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, Y.; Kanamori, H.; Yamato, H.; Ehira, N.; Kawamura, T.; Umehara, S.; Mori, A.; Obara, S.; Ogura, N.; Tanaka, J.; et al. Randomized study of Helicobacter pylori eradication therapy and proton pump inhibitor monotherapy for idiopathic thrombocytopenic purpura. Ann. Hematol. 2005, 84, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, K.; Miyakawa, Y.; Kurata, Y.; Kuwana, M.; Tomiyama, Y.; Murata, M. Reference guide for management of adult idiopathic thrombocytopenic purpura (ITP) 2012 version. Rinsho Ketsueki 2012, 53, 433–442. [Google Scholar] [PubMed]
- Kato, S.; Shimizu, T.; Toyoda, S.; Ishige, T.; Ida, S.; Ushijima, K.; Kamiya, S.; Kuwabara, K.; Konno, M.; Fujimura, S.; et al. The Updated JSPGHAN Guidelines for the Management of Helicobacter pylori Infection in Childhood, 2018. J. Jpn. Soc. Pediatric Gastroenterol. Hepatol. Nutr. 2018, 32, 92–136. [Google Scholar]
- Takahashi, Y.; Miyakawa, Y.; Mori, M.; Kunishima, S.; Higashigawa, M.; Kobayashi, N.; Sasahara, Y.; Maeda, N.; Nakadate, H.; Bessho, F.; et al. Treatment Guide for Refractory Immune Thrombocytopenia in Children for 2019. Jpn. J. Pediatric Hematol. Oncol. 2019, 56, 61–68. [Google Scholar]
- Kato, S.; Ozawa, K.; Konno, M.; Tajiri, H.; Yoshimura, N.; Shimizu, T.; Fujisawa, T.; Abukawa, D.; Minoura, T.; Iinuma, K. Diagnostic accuracy of the 13C-urea breath test for childhood Helicobacter pylori infection: A multicenter Japanese study. Am. J. Gastroenterol. 2002, 97, 1668–1673. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_7.0_Breakpoint_Tables.pdf (accessed on 22 February 2020).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.; Miraglia, V.; Branciforte, F.; Matarese, S.M.; Zecca, M.; Bisogno, G.; Parodi, E.; Amendola, G.; Giordano, P.; Jankovic, M.; et al. Effect of eradication of Helicobacter pylori in children with chronic immune thrombocytopenia: A prospective, controlled, multicenter study. Pediatric Blood Cancer 2011, 56, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, M.; Capozzi, L.; Russo, R. Effect of Helicobacter pylori eradication on platelet count in children with chronic idiopathic thrombocytopenic purpura. Hematology 2009, 14, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Maghbool, M.; Maghbool, M.; Shahriari, M.; Karimi, M. Does Helicobacter pylori play a role in the pathogenesis of childhood chronic idiopathic thrombocytopenic purpura? Pediatric Rep. 2009, 1, e2. [Google Scholar] [CrossRef] [Green Version]
- Treepongkaruna, S.; Sirachainan, N.; Kanjanapongkul, S.; Winaichatsak, A.; Sirithorn, S.; Sumritsopak, R.; Chuansumrit, A. Absence of platelet recovery following Helicobacter pylori eradication in childhood chronic idiopathic thrombocytopenic purpura: A multi-center randomized controlled trial. Pediatric Blood Cancer 2009, 53, 72–77. [Google Scholar] [CrossRef]
- Bisogno, G.; Errigo, G.; Rossetti, F.; Sainati, L.; Pusiol, A.; Da Dalt, L.; Colleselli, P.; Grotto, P.; Carli, M. The role of Helicobacter pylori in children with chronic idiopathic thrombocytopenic purpura. J. Pediatric Hematol. Oncol. 2008, 30, 53–57. [Google Scholar] [CrossRef]
- Hamidieh, A.A.; Arzanian, M.T.; Gachkar, L.; Pasha, F. Helicobacter pylori infection in children with chronic idiopathic thrombocytopenic purpura. J. Pediatric Hematol. Oncol. 2008, 30, 96–97. [Google Scholar] [CrossRef]
- Miyajima, Y.; Kitase, Y.; Suzuki, T.; Hayashi, N.; Sakamoto, M.; Ohe, H.; Kidokoro, H.; Kubota, T.; Kato, Y.; Ogawa, A.; et al. Clinical featues and role of Helicobacter pylori infection in children with idiopathic thrombocytopenic purpura. J. Jpn. Assoc. Rural Med. 2008, 57, 59–65. [Google Scholar] [CrossRef]
- Kato, F.; Arai, A.; Wada, E.; Sugihara, S. Helicobacter pylori Infection in Children with Idiopathic Thrombocytopenic Purpura and the Efficacy of Eradication Therapy. J. Tokyo Women’s Med. Univ. 2007, 77, E40–E45. [Google Scholar]
- Loffredo, G.; Marzano, M.G.; Migliorati, R.; Miele, E.; Menna, F.; Poggi, V.; Staiano, A. The relationship between immune thrombocytopenic purpura and Helicobacter pylori infection in children: Where is the truth? Eur. J. Pediatrics 2007, 166, 1067–1068. [Google Scholar] [CrossRef]
- Neefjes, V.M.; Heijboer, H.; Tamminga, R.Y. H. pylori infection in childhood chronic immune thrombocytopenic purpura. Haematologica 2007, 92, 576. [Google Scholar] [CrossRef]
- Wu, K.S.; Hsiao, C.C.; Yu, H.R.; Huang, E.Y.; Mai, W.L.; Sheen, J.M. Helicobacter pylori infection and childhood idiopathic thrombocytopenic purpura. Acta Paediatr. Taiwanica Taiwan Er Ke Yi Xue Hui Za Zhi 2007, 48, 263–266. [Google Scholar]
- Hayashi, H.; Okuda, M.; Aoyagi, N.; Yoshiyama, M.; Miyashiro, E.; Kounami, S.; Yoshikawa, N. Helicobacter pylori infection in children with chronic idiopathic thrombocytopenic purpura. Pediatrics Int. Off. J. Jpn. Pediatric Soc. 2005, 47, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Yetgin, S.; Demir, H.; Arslan, D.; Unal, S.; Kocak, N. Autoimmune thrombocytopenic purpura and Helicobacter pylori infection effectivity during childhood. Am. J. Hematol. 2005, 78, 318. [Google Scholar] [CrossRef] [PubMed]
- Jaing, T.H.; Yang, C.P.; Hung, I.J.; Chiu, C.H.; Chang, K.W. Efficacy of Helicobacter pylori eradication on platelet recovery in children with chronic idiopathic thrombocytopenic purpura. Acta Paediatr. 2003, 92, 1153–1157. [Google Scholar] [CrossRef]
- Rajantie, J.; Klemola, T. Helicobacter pylori and idiopathic thrombocytopenic purpura in children. Blood 2003, 101, 1660. [Google Scholar] [CrossRef] [Green Version]
- Sakai, M.; Fujisawa, K.; Ohara, A.; Shirahata, A. Childhood Idiopathic Thrombocytopenic Purpura and Helicobacter pylor. Jpn. J. Pediatric Hematol. 2003, 17, 413–417. [Google Scholar]
- Amiri, M. Impact of Helicobacter pylori Eradication Therapy on Platelet Counts in Patients with Chronic Idiopathic Thrombocytopenic Purpura. Glob. J. Health Sci. 2015, 8, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Brito, H.S.; Braga, J.A.; Loggetto, S.R.; Machado, R.S.; Granato, C.F.; Kawakami, E. Helicobacter pylori infection & immune thrombocytopenic purpura in children and adolescents: A randomized controlled trial. Platelets 2015, 26, 336–341. [Google Scholar] [CrossRef]


{kind=link}
| Number of Patients | Mean Age, Standard Deviation, and Range (Years) | |
|---|---|---|
| Total | 33 | 9.05 ± 4.35 (0.67–15.92) |
| Gender | ||
| Male | 15 | 9.61 ± 3.97 (0.67–14.67) |
| Female | 18 | 8.57 ± 4.70 (2.33–15.92) |
| H. pylori infection | ||
| Evaluated | 20 | 8.34 ± 4.28 (0.67–15.91) |
| Positive | 3 | 9.83 ± 3.25 (6.5–13.0) |
| Negative | 17 | 8.08 ± 4.48 (0.67–15.92) |
| Unknown | 13 | 10.13 ± 4.37 (3.25–15.67) |
| Eradication therapy | Success rate: 100% | |
| Responder | 1 | 10.0 † |
| Nonresponder | 2 | 6.5 †, 13.0 † |
| First Author (Year) | Country | Prevalence of H. pylori Infection | Response to H. pylori Eradication Therapy † | Study Design (Risk of Bias Score) | Definition of cITP | Platelet Count Defined As Platelet Response (×104/μL) | Follow-Up Duration (Months) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Platelet Count (×104/μL) | Duration (Months) | |||||||||
| Amiri M (2015) [33] | Iran | 43.5% | (10/23 cases) | 75.0% | (6/8 cases) | CO (NOS: 9) | <10 | >12 | Compared statistically | 6 |
| Brito HS (2015) [34] | Brazil | 25.9% | (22/85 cases) | 61.5% | (8/13 cases) | RCT (Jadad: 3) | <15 | >6 | CR > 15 PR > 5 and Δ > 2 | 12 |
| Russo G (2011) [35] | Italy | 25.8% | (50/194 cases) | 39.4% | (13/33 cases) | CO (NOS: 8) | <10 | >12 | CR > 15 PR > 5 and Δ > 3 | 12 |
| Ferrara M (2009) [36] | Italy | 33.3% | (8/24 cases) | 100% | (8/8 cases) | CO (NOS: 8) | <50 | >6 | CR > 15 PR > Δ > 5 | 12 |
| Maghbool M (2009) [37] | Iran | 16.7% | (5/30 cases) | 100% | (5/5 cases) | CCS (NOS: 8) | <10 | >6 | CR > 15 PR > 5 | 12 |
| Treepongkaruna S (2009) [38] | Thailand | 29.1% | (16/55 cases) | 14.3% | (2/14 cases) | RCT (Jadad: 3) | <10 | >6 | >10 | 12 |
| Bisogno G (2008) [39] | Italy | 33.3% | (8/24 cases) | 37.5% | (3/8 cases) | CO (NOS: 9) | <10 | >6 | CR > 15 PR > 5 and Δ > 3 | >6 |
| Hamidieh AA (2008) [40] | Iran | 12.9% | (4/31 cases) | 0% | (0/4 cases) | CS (N/A) | <15 | >6 | CR > 15 PR > Δ > 5 | >6 |
| Miyajima Y (2008) [41] | Japan | 7.1% | (1/14 cases) | ND | CSS (N/A) | <10 | >6 | >15 | 3 | |
| Kato F (2007) [42] | Japan | 27.3% | (3/11 cases) | 33.3% | (1/3 cases) | CS (N/A) | <10 | >6 | >15 | 12 |
| Loffredo G (2007) [43] | Italy | 20.5% | (8/39 cases) | 0% | (0/7 cases) | CO (NOS: 6) | <10 | >6 | >12 | 12 |
| Neefjes VM (2007) [44] | The Netherlands | 6.4% | (3/47 cases) | 100% | (3/3 cases) | CCS (NOS: 5) | <10 | >12 | CR > 15 PR > 5 and twice | >6 |
| Wu KS (2007) [45] | Taiwan | 40.0% | (2/5 cases) | ND | CSS (N/A) | <50 | >6 | N/A | N/A | |
| Hayashi H (2005) [46] | Japan | 20.0% | (2/10 cases) | 100% | (1/1 cases) | CS (N/A) | <10 | >6 | >15 | 12 |
| Yetgin S (2005) [47] | Turkey | 31.4% | (11/35 cases) | 0% | (0/9 cases) | CS (N/A) | <50 | >6 | >5 within 12 months | 12 |
| Jaing TH (2003) [48] | Taiwan | 40.9% | (9/22 cases) | 55.6% | (5/9 cases) | CO (NOS: 7) | <50 | >6 | CR > 15 PR > 5 | 16 |
| Rajantie J (2003) [49] | Finland | 0% | (0/17 cases) | ND | CS (N/A) | N/D | N/D | N/A | N/A | |
| Sakai M (2003) [50] | Japan | 5.0% | (2/40 cases) | ND | CSS (N/A) | <10 | >6 | N/A | N/A | |
| This study | Japan | 15% | (3/20 cases) | 3.3% | (1/3 cases) | CS (N/A) | <10 | >6 | CR > 15, PR > 5 or twice within 2 months | 12 |
| Total † | 23.0% | (167/726 cases) | 43.8% | (56/128 cases) | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikuse, T.; Toda, M.; Kashiwagi, K.; Maruyama, K.; Nagata, M.; Tokushima, K.; Ito, N.; Tokita, K.; Kyodo, R.; Hosoi, K.; et al. Efficacy of Helicobacter pylori Eradication Therapy on Platelet Recovery in Pediatric Immune Thrombocytopenic Purpura-Case Series and a Systematic Review. Microorganisms 2020, 8, 1457. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8101457
Ikuse T, Toda M, Kashiwagi K, Maruyama K, Nagata M, Tokushima K, Ito N, Tokita K, Kyodo R, Hosoi K, et al. Efficacy of Helicobacter pylori Eradication Therapy on Platelet Recovery in Pediatric Immune Thrombocytopenic Purpura-Case Series and a Systematic Review. Microorganisms. 2020; 8(10):1457. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8101457
Chicago/Turabian StyleIkuse, Tamaki, Masanori Toda, Kosuke Kashiwagi, Kimiko Maruyama, Masumi Nagata, Kaori Tokushima, Natsuki Ito, Kazuhide Tokita, Reiko Kyodo, Kenji Hosoi, and et al. 2020. "Efficacy of Helicobacter pylori Eradication Therapy on Platelet Recovery in Pediatric Immune Thrombocytopenic Purpura-Case Series and a Systematic Review" Microorganisms 8, no. 10: 1457. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8101457