New Insights in Laboratory Testing for COVID-19 Patients: Looking for the Role and Predictive Value of Human epididymis secretory protein 4 (HE4) and the Innate Immunity of the Oral Cavity and Respiratory Tract

 ,
,  ,
, 

Abstract
:1. Background
2. Materials and Methods
3. Statistical Analysis
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Santacroce, L.; Charitos, I.; Del Prete, R. COVID-19 in Italy: An overview from the first case to date. Electron. J. Gen. Med. 2020, 17, em235. [Google Scholar] [CrossRef] [Green Version]
- Santacroce, L.; Bottalico, L.; Charitos, I.A. The Impact of COVID-19 on Italy: A Lesson for the Future. Int. J. Occup. Environ. Med. 2020, 11, 151–152. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E. Epidemiology, virology, and clinical features of severe acute respiratory syndrome -coronavirus-2 (SARS-CoV-2; Coronavirus Disease-19). Clin. Exp. Pediatr. 2020, 63, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rokni, M.; Ghasemi, V.; Tavakoli, Z. Immune responses and pathogenesis of SARS-CoV-2 during an outbreak in Iran: Comparison with SARS and MERS. Rev. Med. Virol. 2020, 30, e2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.W. There’s a New Symptom of Coronavirus, Doctors Say: Sudden Loss of Smell or Taste. 2020. Available online: https://eu.usatoday.com/story/news/health/2020/03/24/coronavirus-symptoms-loss-smell-taste/2897385001/ (accessed on 26 June 2020).
- Hopkins, C.; Kumar, N. Loss of Sense of Smell as Marker of COVID-19 Infection, ENT UK. 2020. Available online: https://www.entuk.org/sites/default/files/files/ (accessed on 26 June 2020).
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 virus targeting the CNS: Tissue distribution, host–virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Cazzolla, A.P.; Lovero, R.; Lo Muzio, L.; Testa, N.F.; Schirinzi, A.; Palmieri, G.; Pozzessere, P.; Procacci, V.; Di Comite, M.; Ciavarella, D.; et al. Taste and smell disorders in COVID-19 patients: Role of Interleukin-6. ACS Chem. Neurosci. 2020, 11, 2774–2781. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Dipalma, G.; Isacco, C.G.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral Microbiota and Immune System Crosstalk: A Translational Research. Biology 2020, 9, 131. [Google Scholar] [CrossRef]
- Wan, S.; Yi, Q.; Fan, S.; Lv, J.; Zhang, X.; Guo, L.; Lang, C.; Xiao, Q.; Xiao, K.; Yi, Z.; et al. Relationships among lymphocyte subsets, cytokines, and the pulmonary inflammation index in coronavirus (COVID-19) infected patients. Br. J. Haematol. 2020, 189, 428–437. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciceri, F.; Beretta, L.; Scandroglio, A.M.; Colombo, S.; Landoni, G.; Ruggeri, A.; Peccatori, J.; D’Angelo, A.; De Cobelli, F.; Rovere-Querini, P. Microvascular COVID-19 lung vessels obstructive thromboinflammatory syndrome (MicroCLOTS): An atypical acute respiratory distress syndrome working hypothesis. Crit. Care Resusc. 2020, 22, 95–97. [Google Scholar]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef]
- Venkataraman, T.; Frieman, M.B. The role of epidermal growth factor receptor (EGFR) signaling in SARS coronavirus-induced pulmonary fibrosis. Antivir. Res. 2017, 143, 142–150. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Ma, S. The cytokine storm and factors determining the sequence and severity of organ dysfunction in multiple organ dysfunction syndrome. Am. J. Emerg. Med. 2008, 26, 711–715. [Google Scholar] [CrossRef]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. China Medical Treatment Expert Group for COVID-19. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; Sun, R.; Tian, Z.; Xu, X.; Wei, H. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl. Sci. Rev. 2020, 13, nwaa041. [Google Scholar] [CrossRef] [Green Version]
- Vabret, N.; Britton, G.J.; Gruber, C.; Hegde, S.; Kim, J.; Kuksin, M.; Levantovsky, R.; Malle, L.; Moreira, A.; Park, M.D.; et al. Immunology of COVID-19: Current state of the science. Immunity 2020, 52, 910–941. [Google Scholar] [CrossRef] [PubMed]
- Schirinzi, A.; Cazzolla, A.P.; Mascolo, E.; Palmieri, G.; Pesce, F.; Gesualdo, L.; Santacroce, L.; Ballini, A.; Lovero, R.; Di Serio, F. Determination of the upper reference limit of Human epididymis secretory protein 4 (HE4) in healthy male individuals and correlation with renal and fertility markers. Endocr. Metab. Immune Disord. Drug Targets 2020. [Google Scholar] [CrossRef] [PubMed]
- Bingle, L.; Cross, S.S.; High, A.S.; Wallace, W.A.; Rassl, D.; Yuan, G.; Hellstrom, I.; Campos, M.A.; Bingle, C.D. WFDC2 (HE4): A potential role in the innate immunity of the oral cavity and respiratory tract and the development of adenocarcinomas of the lung. Respir. Res. 2006, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- Galgano, M.T.; Hampton, G.M.; Frierson, H.F. Comprehensive analysis of HE4 expression in normal and malignant human tissues. Mod. Pathol. 2006, 19, 847–853. [Google Scholar] [CrossRef] [Green Version]
- Kirchhoff, C.; Habben, I.; Ivell, R.; Krull, N. A Major Human Epididymis-Specific cDNA Encodes a Protein with Sequence Homology to Extracellular Proteinase Inhibitors1. Biol. Reprod. 1991, 45, 350–357. [Google Scholar] [CrossRef]
- Mardani, R.; Vasmehjani, A.A.; Zali, F.; Gholami, A.; Nasab, S.D.M.; Kaghazian, H.; Kaviani, M.; Ahmadi, N. Laboratory parameters in detection of COVID-19 patients with positive RT-PCR; a diagnostic accuracy study. Arch. Acad. Emerg. Med. 2020, 8, e43. [Google Scholar] [PubMed]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Damen, J.A.A.; Debray, T.P.A.; De Vos, M.; et al. Prediction models for diagnosis and prognosis of covid-19 infection: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Kermali, M.; Khalsa, R.K.; Pillai, K.; Ismail, Z.; Harky, A. The role of biomarkers in diagnosis of COVID-19—A systematic review. Life Sci. 2020, 254, 117788. [Google Scholar] [CrossRef]
- Yu, B.; Li, X.; Chen, J.; Ouyang, M.; Zhang, H.; Zhao, X.; Tang, L.; Luo, Q.; Xu, M.; Yang, L. Evaluation of variation in D-dimer levels among COVID-19 and bacterial pneumonia: A retrospective analysis. J. Thromb. Thrombolysis 2020, 50, 548–557. [Google Scholar] [CrossRef]
- Marietta, M.; Ageno, W.; Artoni, A.; De Candia, E.; Gresele, P.; Marchetti, M.; Marcucci, R.; Tripodi, A. COVID-19 and haemostasis: A position paper from Italian Society on Thrombosis and Haemostasis (SISET). Blood Transfus. 2020, 18, 167–169. [Google Scholar]
- Pagaduan, J.V.; Tam, E.; Devaraj, S. Validation of the Procalcitonin Assay on the Abbott Architect i1000. J. Appl. Lab. Med. 2019, 3, 936–942. [Google Scholar] [CrossRef]
- Charitos, I.A.; Ballini, A.; Bottalico, L.; Cantore, S.; Passarelli, P.C.; Inchingolo, F.; D’Addona, A.; Santacroce, L. Special features of SARS-CoV2 in daily practice. World J. Clin. Cases 2020, 8, 3920. [Google Scholar] [CrossRef] [PubMed]
- Di Serio, F.; Lovero, R.; D’Agostino, D.; Nisi, L.; Miragliotta, G.; Contino, R.; Man, A.; Ciccone, M.M.; Santacroce, L. Evaluation of procalcitonin, Vitamin D and C-reactive protein levels in septic patients with positive emocoltures. Our preliminary experience. Acta Med. Mediterr. 2016, 32, 1911–1914. [Google Scholar]
- Zaninotto, M.; Mion, M.M.; Cosma, C.; Rinaldi, D.; Plebani, M. Presepsin in risk stratification of SARS-CoV-2 patients. Clin. Chim. Acta 2020, 507, 161–163. [Google Scholar] [CrossRef]
- Wei, X.; Su, J.; Yang, K.; Wei, J.; Wan, H.; Cao, X.; Tan, W.; Wang, H. Elevations of serum cancer biomarkers correlate with severity of COVID-19. J. Med. Virol. 2020, 92, 2036–2041. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Patel, S.K.; Pathak, M.; Yatoo, M.I.; Tiwari, R.; Malik, Y.S.; Singh, R.; Sah, R.; Rabaan, A.A.; Bonilla-Aldana, D.K. An update on SARS-CoV-2/COVID-19 with particular reference to its clinical pathology, pathogenesis, immunopathology and mitigation strategies. Travel Med. Infect. Dis. 2020, 37, 101755. [Google Scholar] [CrossRef]
- Xiang, J.; Wen, J.; Yuan, X.; Xiong, S.; Zhou, X.; Liu, C.; Min, X. Potential Biochemical Markers to Identify Severe Cases among COVID-19 Patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Chhikara, N.; Saraswat, M.; Tomar, A.K.; Dey, S.; Singh, S.; Yadav, S. Human epididymis protein-4 (HE-4): A novel cross-class protease inhibitor. PLoS ONE 2012, 7, e47672. [Google Scholar] [CrossRef] [Green Version]
- Madanchi, H.; Shoushtari, M.; Kashani, H.; Sardari, S. Antimicrobial peptides of the vaginal innate immunity and their role in the fight against sexually transmitted diseases. New Microbes New Infect. 2020, 34, 100627. [Google Scholar] [CrossRef]
- Dhochak, N.; Singhal, T.; Kabra, S.; Lodha, R. Pathophysiology of COVID-19: Why Children Fare Better than Adults? Indian J. Pediatrics 2020, 87, 537–546. [Google Scholar] [CrossRef]
- Vardhana, S.A.; Wolchok, J.D. The many faces of the anti-COVID immune response. J. Exp. Med. 2020, 217, e20200678. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.-C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045.e9. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The Human Respiratory System and its Microbiome at a Glimpse. Biology 2020, 9, 318. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A. Coronavirus Disease 2019 (COVID-19) pandemic burst and its relevant consequences in dental practice. Open Dent. 2020, 14, 111–112. [Google Scholar] [CrossRef]
- Pham, V.H.; Gargiulo, I.C.; Nguyen, K.C.D.; Le, S.H.; Tran, D.K.; Nguyen, Q.V.; Pham, H.T.; Aityan, S.; Pham, S.T.; Cantore, S.; et al. Rapid and sensitive diagnostic procedure for multiple detection of pandemic Coronaviridae family members SARS-CoV-2, SARS-CoV, MERS-CoV and HCoV: A translational research and cooperation between the Phan Chau Trinh University in Vietnam and University of Bari “Aldo Moro” in Italy. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7173–7191. [Google Scholar]
- Ballini, A.; Cantore, S.; Scacco, S.; Coletti, D.; Tatullo, M. Mesenchymal stem cells as promoters, enhancers, and playmakers of the translational regenerative medicine 2018. Stem Cells Int. 2018, 2018, 6927401. [Google Scholar] [CrossRef] [Green Version]
- Santacroce, L.; Charitos, I.A.; Bottalico, L. A successful history: Probiotics and their potential as antimicrobials. Expert Rev. Anti-Infect. Ther. 2019, 17, 635–645. [Google Scholar] [CrossRef]
- Ballini, A.; Gnoni, A.; De Vito, D.; Dipalma, G.; Cantore, S.; Gargiulo, I.C.; Saini, R.; Santacroce, L.; Topi, S.; Scarano, A.; et al. Effect of probiotics on the occurrence of nutrition absorption capacities in healthy children: A randomized double-blinded placebo-controlled pilot study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8645–8657. [Google Scholar]
- Inchingolo, F.; Dipalma, G.; Cirulli, N.; Cantore, S.; Saini, R.S.; Altini, V.; Santacroce, L.; Ballini, A.; Saini, R. Microbiological results of improvement in periodontal condition by administration of oral probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1323–1328. [Google Scholar] [PubMed]
- Ballini, A.; Santacroce, L.; Cantore, S.; Bottalico, L.; Dipalma, G.; Vito, D.; Saini, R.; Inchingolo, F. Probiotics Improve Urogenital Health in Women. Open Access Maced. J. Med. Sci. 2018, 6, 1845–1850. [Google Scholar] [CrossRef] [Green Version]
- Lamy, P.J.; Plassot, C.; Pujol, J.L. Serum HE4: An Independent Prognostic Factor in Non-Small Cell Lung Cancer. PLoS ONE 2015, 10, e0128836. [Google Scholar] [CrossRef] [Green Version]
- Gąsiorowska, E.; Magnowska, M.; Iżycka, N.; Warchoł, W.; Nowak-Markwitz, E. The role of HE4 in differentiating benign and malignant endometrial pathology. Ginekol. Pol. 2016, 87, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Kappelmayer, J.; Antal-Szalmás, P.; Nagy, B., Jr. Human epididymis protein 4 (HE4) in laboratory medicine and an algorithm in renal disorders. Clin. Chim. Acta 2015, 438, 35–42. [Google Scholar] [CrossRef]
- Huang, J.; Chen, J.; Huang, Q. Diagnostic value of HE4 in ovarian cancer: A meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 231, 35–42. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| - age > 18 years - laboratory-confirmed COVID-19 infection (reverse transcription-polymerase chain reaction, RT-PCR) | - patients without a laboratory-confirmed diagnosis of COVID-19 infection - patients with olfactory or gustatory dysfunctions before the epidemic (congenital anosmia, side effects of drugs, previous surgery or radiotherapy in the oral and nasal cavities, head injury, sinonasal diseases, allergic rhinitis) - patients with systemic diseases (iron deficiency, autoimmune diseases) - patients with some malignant neoplasms (ovarian cancer, pulmonary and breast adenocarcinoma, renal carcinoma, urinary tract and bladder carcinoma, oral carcinoma) - patients with cystic fibrosis - patients with neurodegenerative disorders (Parkinson’s disease, disease Alzheimer’s disease, dementia) and with major depression |
| General Characteristics | |
| Gender | Age (years) |
| Male 58 (67.4%) | 68 ± 12.6 |
| Female 28 (32.6%) | 65 ± 15.1 |
| Days from COVID-19 symptoms onset | 4 ± 1 |
| Day of duration chemosensitive disorders | 21 ± 7 |
| Clinical classification | |
| SEVERE 31 (36.1%) | 65 ± 13 |
| Male 24 (77.4%) | 65 ± 13.4 |
| Female 7 (22.6%) | 64 ± 12.5 |
| MILD 36 (41.8%) | 65 ± 15.3 |
| Male 20 (55.6%) | 67 ± 12.9 |
| Female 16 (44.46%) | 67 ± 12.9 |
| CRITICAL 19 (22.1%) | 75 ± 6.9 |
| Male 13 (68.4%) | 74 ± 7.7 |
| Female 6 (31.6%) | 75 ± 6.7 |
| Associated Symptoms | |
| Felt tired | 81 (94%) |
| Asthenia | 65 (75.5%) |
| Nasal Obstruction | 23 (26.7%) |
| Small disorders | 75 (87%) |
| Taste disorders | 69 (80%) |
| Fever | 83 (96.5%) |
| Cough | 73 (84.8%) |
| Headache | 45 (52.3%) |
| Sore throat | 63 (73.2%) |
| Abdominal symptoms | 10 (11.6%) |
| Muscle or joint pains | 79 (91.8%) |
| Chest pain | 70 (81.3%) |
| Nausea | 40 (46.5%) |
| Vomit | 39 (45.3%) |
| Loss of appetite | 39 (45.3%) |
| Problems breathing | 71 (82.5%) |
| Diarrhea | 10 (11.6%) |
| Associated Pathologies | |
| Diabetes | 31 (36.04%) |
| Hypertension | 57 (66.2%) |
| Respiratory insufficiency | 36 (41.8%) |
| Gastroesophageal reflux disease | 31 (36.04%) |
| Thyroid diseases | 21 (24.4%) |
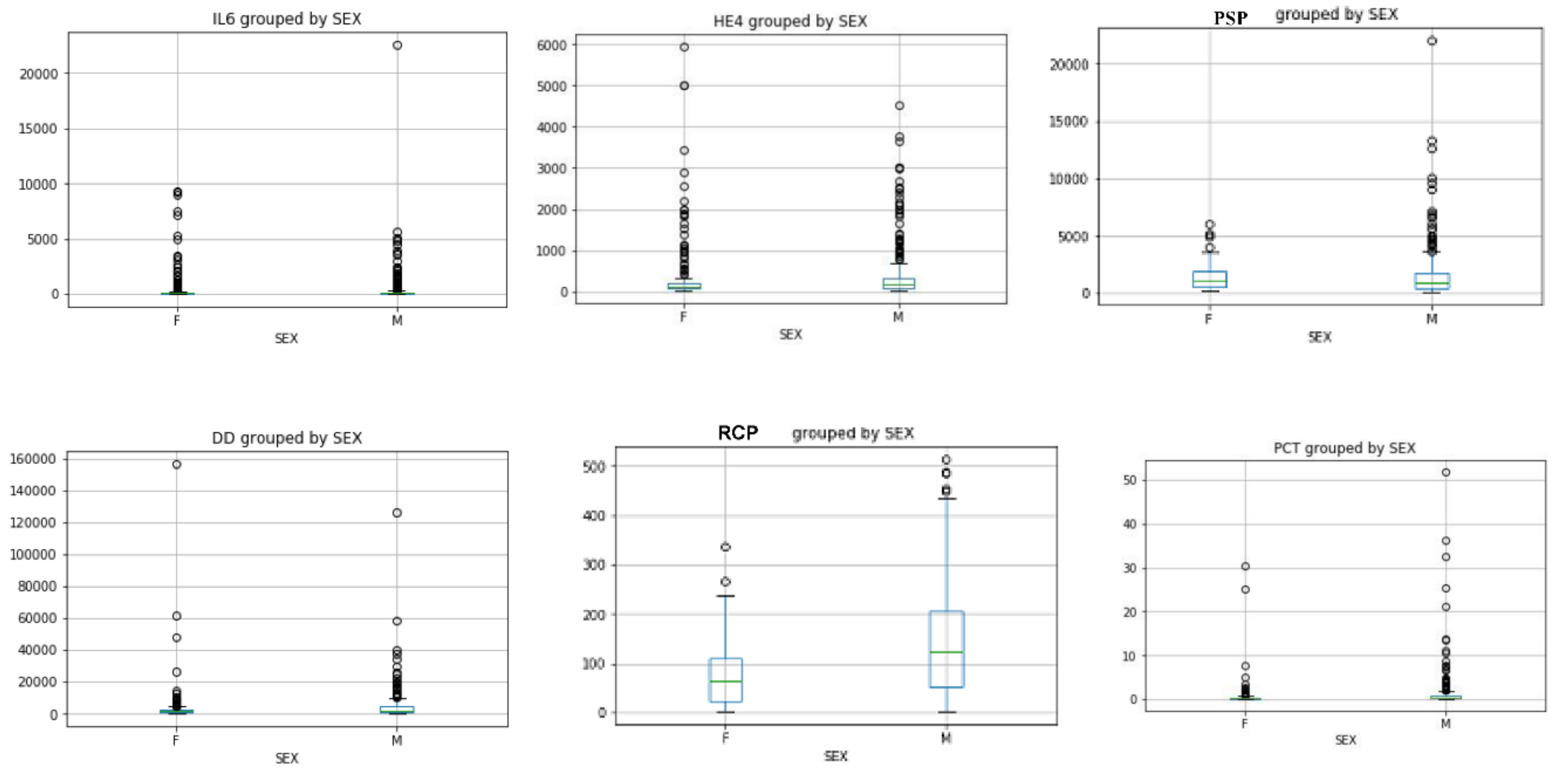
| a | Mann Whitney U test in all patients | ||
|---|---|---|---|
| Variable | p value | Mean value | |
| He4 level (CND) vs. He4 (CD) | <0.0001 | 110 vs. 1274 | |
| IL6 level (CND) vs. IL6 (CD) | <0.0001 | 256 vs. 1055 | |
| RCP (CND) vs. RCP (CD) | p = 0.0001 | 119 vs. 152 | |
| PSP (CND) vs. PSP (CD) | <0.0001 | 727 vs. 2543 | |
| PCT (CND) vs. PCT (CD) | <0.0001 | 1.19 vs. 2.01 | |
| D-Dimer (CND) vs. D-Dimer (CD) | <0.0001 | 3117 vs. 9739 | |
| b | Mann Whitney U test in mild, severe and critical (CD) patients | ||
| Variable | p value | Mean value | |
| He4 mild vs. He4 severe | <0.0001 | 91 vs. 204 | |
| He4 mild vs. He4 critical | <0.0001 | 91 vs. 1273 | |
| PSP mild vs. PSP severe | <0.0001 | 737 vs. 1234 | |
| PSP mild vs. PSP critical | <0.0001 | 737 vs. 3029 | |
| IL6 mild vs. IL6 severe | <0.0001 | 29 vs. 109 | |
| IL6 mild vs. IL6 critical | <0.0001 | 29 vs. 1598 | |
| RCP mild vs. RCP severe | <0.0001 | 81 vs. 144 | |
| RCP mild vs. RCP critical | <0.0001 | 81 vs. 153 | |
| PCT mild vs. PCT severe | <0.0001 | 0.72 vs. 0.80 | |
| PCT mild vs. PCT critical | <0.0001 | 0.72 vs. 2.6 | |
| D-Dimer mild vs. D-Dimer severe | <0.0001 | 2091 vs. 3075 | |
| D-Dimer mild vs. D-Dimer critical | <0.0001 | 2091 vs. 9756 | |
| c | Pearson’s linear correlation coefficients in all patients | ||
| Variable | Pearson Coefficient (r) | 95% confidence intervals | p value |
| He4 vs. IL6 | 0.797 | 0.763 to 0.826 | <0.05 |
| He4 vs. PSP | 0.621 | 0.565 to 0.671 | <0.05 |
| He4 vs. PCT | 0.447 | 0.376 to 0.513 | <0.05 |
| He4 vs. D-Dimer | 0.367 | 0.290 to 0.439 | <0.05 |
| He4 vs. RCP | 0.327 | 0.249 to 0.402 | <0.05 |
| Pearson’s linear correlation coefficients in mild patients | |||
| He4 vs. D-Dimer | 0.2004 | 0.069 to 0.324 | 0.0029 |
| He4 vs. IL6 | 0.42 | 0.306 to 0.542 | <0.0001 |
| He4 vs. RCP | 0.144 | 0.01 to 0.272 | =0.0323 |
| He4 vs. PSP | 0.323 | 0.199 to 0.437 | <0.0001 |
| He4 vs. PCT | 0.043 | −0.089 to 0.175 | =0.523 |
| Pearson’s linear correlation coefficients in severe patients | |||
| He4 vs. D-Dimer | 0.346 | 0.213 to 0.466 | <0.0001 |
| He4 vs. IL6 | 0.48 | 0.336 to 0.563 | <0.0001 |
| He4 vs. RCP | 0.173 | 0.0.30 to 0.308 | =0.0174 |
| He4 vs. PSP | 0.329 | 0.195 to 0.451 | <0.0001 |
| He4 vs. PCT | 0.192 | 0.50 to 0.326 | = 0.0082 |
| Pearson’s linear correlation coefficients in critical patients (CD) | |||
| He4 vs. D-Dimer | 0.009 | −0.191 to 0.173 | = 0.922 |
| He4 vs. IL6 | 0.69 | 0.581 to 0.775 | <0.0001 |
| He4 vs. RCP | 0.173 | 0.030 to 0.308 | =0.017 |
| He4 vs. PSP | 0.128 | −0.054 to 0.304 | =0.168 |
| He4 vs. PCT | 0.192 | 0.050 to 0.326 | =0.008 |
| Variable | Spearman’s rank coefficient correlation (rs) in CND patients | 95% confidence intervals | p value |
|---|---|---|---|
| He4 vs. IL6 | 0.70 | 0.65 to 0.74 | <0.0001 |
| He4 vs. PSP | 0.498 | 0.421 to 0.562 | <0.0001 |
| He4 vs. PCT | 0.39 | 0.30 to 0.47 | <0.0001 |
| He4 vs. D-Dimer | 0.211 | 0.116 to 0.302 | <0.0001 |
| He4 vs. RCP | 0.30 | 0.21 to 0.38 | <0.0001 |
| Variable | Spearman’s rank coefficient correlation (rs) in mild patients | 95% confidence intervals | p value |
| He4 mild vs. IL6 mild | 0.65 | 0.520 to 0.687 | <0.0001 |
| He4 mild vs. PSP mild | 0.408 | 0.292 to 0.513 | <0.0001 |
| He4 mild vs. PCT mild | 0.37 | 0.249 to 0.479 | <0.0001 |
| He4 mild vs. D-Dimer mild | 0.229 | 0.099 to 0.351 | =0.0006 |
| He4 mild vs. RCP mild | 0.32 | 0.196 to 0.434 | <0.0001 |
| Variable | Spearman’s rank coefficient correlation (rs) in severe patients | 95% confidence intervals | p value |
| He4 severe vs. IL6 severe | 0.633 | 0.352 to 0.685 | <0.0001 |
| He4 severe vs. PSP severe | 0.510 | 0.422 to 0.589 | <0.0001 |
| He4 severe vs. PCT severe | 0.112 | 0.0312 to 0.251 | <0.0001 |
| He4 severe vs. D-Dimer severe | 0.288 | 0.132 to 0.401 | <0.0001 |
| He4 severe vs. RCP severe | 0.294 | 0.0154 to 0.335 | <0.0001 |
| Variable | Spearman’s rank coefficient correlation (rs) in critical patients (CD patients) | 95% confidence intervals | p value |
| He4 critical vs. IL6 critical | 0.698 | 0.58 to 0.77 | <0.0001 |
| He4 critical vs. PSP critical | 0.345 | 0.174 to 0.496 | =0.0001 |
| He4 critical vs. PCTcritical | 0.43 | 0.27 to 0.57 | <0.0001 |
| He4 cfitical vs. D-Dimer critical | 0.151 | −0.032 to 0.325 | =0.105 |
| He4 critical vs. RCP critical | −0.08 | −0.26 to 0.102 | =0.383 |
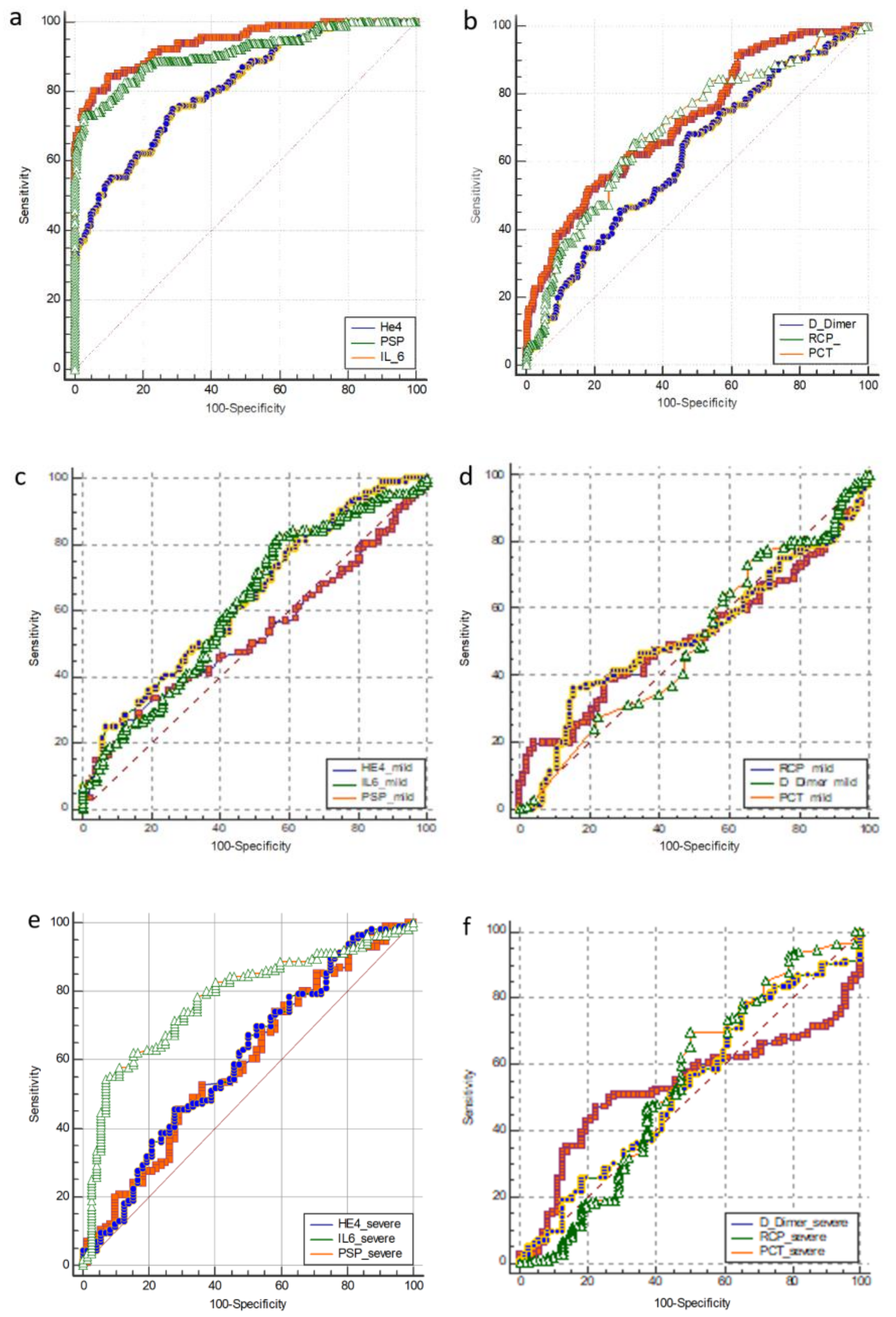
| All Patients | ||||||
|---|---|---|---|---|---|---|
| Parameter | AUC | 95% confidence intervals | Cut off | Sensitivity | Specifity | p value |
| He4 | 0.92 | 0.898 to 0.95 | 359 | 80 | 92 | <0.0001 |
| IL-6 | 0.91 | 0.88 to 0.934 | 212 | 73 | 93 | <0.0001 |
| RCP | 0.616 | 0.573 to 0.658 | 88 | 68 | 52 | <0.0001 |
| PSP | 0.81 | 0.77 to 0.84 | 1179 | 75 | 71 | <0.0001 |
| PCT | 0.701 | 0.66 to 0.740 | 0.37 | 65 | 68 | <0.0001 |
| D-Dimer | 0.721 | 0.680 to 0.759 | 3757 | 51 | 81 | <0.0001 |
| Mild patients | ||||||
| Parameter | AUC | 95% confidence intervals | Cut off | Sensitivity | Specifity | p value |
| He4 | 0.978 | 0.955 to 0.991 | 198 | 90 | 94 | <0.0001 |
| IL-6 | 0.96 | 0.93 to 0.979 | 96 | 88 | 98 | <0.0001 |
| RCP | 0.705 | 0.653 to 0.753 | 88 | 68 | 64 | <0.0001 |
| PSP | 0.873 | 0.832 to 0.907 | 1179 | 55 | 94 | <0.0001 |
| PCT | 0.622 | 0.565 to 0.677 | 1.07 | 36 | 86 | <0.0001 |
| D-Dimer | 0.753 | 0.703 to 0.798 | 3757 | 51 | 89 | <0.0001 |
| Severe patients | ||||||
| Parameter | AUC | 95% confidence intervals | Cut off | Sensitivity | Specifity | p value |
| He4 | 0.897 | 0.857 to 0.929 | 425 | 74.14 | 95.21 | <0.0001 |
| IL-6 | 0.851 | 0.806 to 0.890 | 212 | 73 | 94 | <0.0001 |
| RCP | 0.513 | 0.455 to 0.542 | 184 | 34 | 72 | <0.0001 |
| PSP | 0.738 | 0.684 to 0.786 | 2069 | 50 | 89.89 | <0.0001 |
| PCT | 0.622 | 0.565 to 0.677 | 1.07 | 36 | 86 | <0.0001 |
| D-Dimer | 0.683 | 0.628 to 0.735 | 5284 | 38.9 | 87.7 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schirinzi, A.; Cazzolla, A.P.; Lovero, R.; Lo Muzio, L.; Testa, N.F.; Ciavarella, D.; Palmieri, G.; Pozzessere, P.; Procacci, V.; Di Serio, F.; et al. New Insights in Laboratory Testing for COVID-19 Patients: Looking for the Role and Predictive Value of Human epididymis secretory protein 4 (HE4) and the Innate Immunity of the Oral Cavity and Respiratory Tract. Microorganisms 2020, 8, 1718. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8111718
Schirinzi A, Cazzolla AP, Lovero R, Lo Muzio L, Testa NF, Ciavarella D, Palmieri G, Pozzessere P, Procacci V, Di Serio F, et al. New Insights in Laboratory Testing for COVID-19 Patients: Looking for the Role and Predictive Value of Human epididymis secretory protein 4 (HE4) and the Innate Immunity of the Oral Cavity and Respiratory Tract. Microorganisms. 2020; 8(11):1718. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8111718
Chicago/Turabian StyleSchirinzi, Annalisa, Angela Pia Cazzolla, Roberto Lovero, Lorenzo Lo Muzio, Nunzio Francesco Testa, Domenico Ciavarella, Giuseppe Palmieri, Pietro Pozzessere, Vito Procacci, Francesca Di Serio, and et al. 2020. "New Insights in Laboratory Testing for COVID-19 Patients: Looking for the Role and Predictive Value of Human epididymis secretory protein 4 (HE4) and the Innate Immunity of the Oral Cavity and Respiratory Tract" Microorganisms 8, no. 11: 1718. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8111718