Presence of Infection by Mycobacterium avium subsp. paratuberculosis in the Blood of Patients with Crohn’s Disease and Control Subjects Shown by Multiple Laboratory Culture and Antibody Methods

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Diagnosis and Diagnostic Categorization
2.3. Procedures
2.3.1. MGIT Culture
2.3.2. TiKa Culture
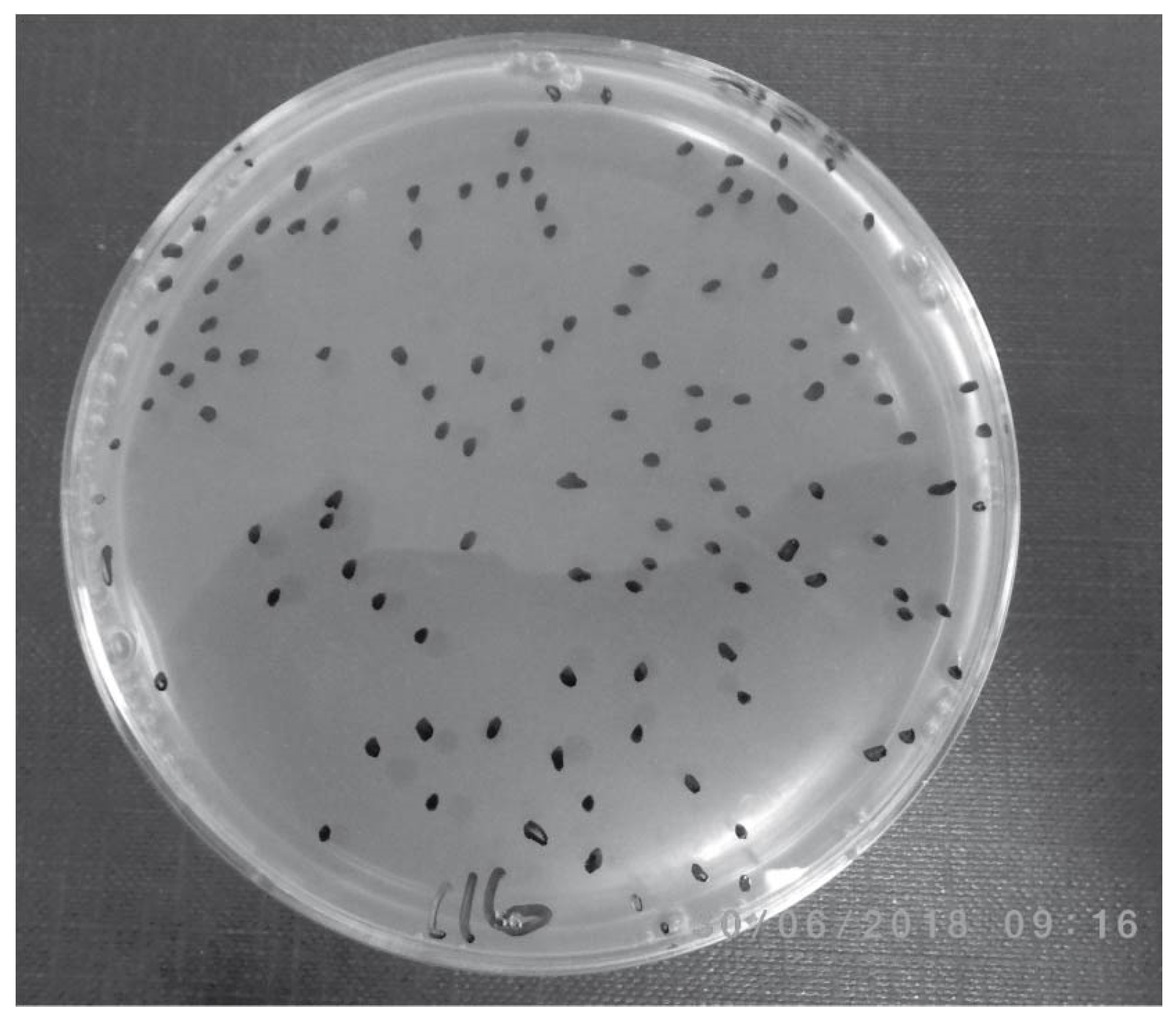
2.3.3. Pozzato Culture and Phage Amplification Assay
2.3.4. MAP Antibody Assay
2.3.5. PtpA and PknG ELISA Test
2.3.6. Hsp65 Antibody Assay
2.4. Data Analyses and Statistical Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Over, K.; Crandall, P.G.; O’Bryan, C.A.; Ricke, S.C. Current perspectives on Mycobacterium avium subsp. paratuberculosis, Johne’s disease, and Crohn’s disease: A review. Crit. Rev. Microbiol. 2011, 37, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Rathnaiah, G.; Zinniel, D.K.; Bannantine, J.P.; Stabel, J.R.; Grohn, Y.T.; Collins, M.T.; Barletta, R.G. Pathogenesis, Molecular Genetics, and Genomics of Mycobacterium avium subsp. paratuberculosis, the Etiologic Agent of Johne’s Disease. Front. Vet. Sci. 2017, 4, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chacon, O.; Bermudez, L.E.; Barletta, R.G. Johne’s disease, inflammatory bowel disease, and Mycobacterium paratuberculosis. Annu. Rev. Microbiol. 2004, 58, 329–363. [Google Scholar] [CrossRef] [Green Version]
- Bo, M.; Niegowska, M.; Frau, J.; Sechi, G.; Arru, G.; Cocco, E.; Sechi, L.A. IL-2 and Mycobacterial Lipoarabinomannan as Targets of Immune Responses in Multiple Sclerosis Patients. Microorganisms 2020, 8, 500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cossu, D.; Yokoyama, K.; Nobutaka, N.; Sechi, L.A. From Sardinia to Japan: Update on the role of MAP in multiple sclerosis. Future Microbiol. 2019, 14, 643–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slavin, Y.N.; Bo, M.; Caggiu, E.; Sechi, G.; Arru, G.; Bach, H.; Sechi, L.A. High levels of antibodies against PtpA and PknG secreted by Mycobacterium avium ssp. paratuberculosis are present in neuromyelitis optica spectrum disorder and multiple sclerosis patients. J. Neuroimmunol. 2018, 323, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Frau, J.; Cossu, D.; Sardu, C.; Mameli, G.; Coghe, G.; Lorefice, L.; Fenu, G.; Tranquilli, S.; Sechi, L.A.; Marrosu, M.G.; et al. Combining HLA-DRB1-DQB1 and Mycobacterium Avium Subspecies Paratubercolosis (MAP) antibodies in Sardinian multiple sclerosis patients: Associated or independent risk factors? BMC Neurol. 2016, 16, 148. [Google Scholar] [CrossRef]
- Mameli, G.; Cossu, D.; Caggiu, E.; Arru, G.; Niegowska, M.; Cocco, E.; Frau, J.; Marrosu, M.G.; Sechi, L.A. Soluble BAFF Level Is Not Correlated to Mycobacterium avium Subspecies paratuberculosis Antibodies and Increases after Interferon-beta Therapy in Multiple Sclerosis Patients. J. Mol. Neurosci. 2016, 60, 91–93. [Google Scholar] [CrossRef]
- Cossu, D.; Yokoyama, K.; Sechi, L.A.; Otsubo, S.; Tomizawa, Y.; Momotani, E.; Hattori, N. Humoral response against host-mimetic homologous epitopes of Mycobacterium avium subsp. paratuberculosis in Japanese multiple sclerosis patients. Sci. Rep. 2016, 6, 29227. [Google Scholar] [CrossRef] [Green Version]
- Mameli, G.; Cocco, E.; Frau, J.; Marrosu, M.G.; Sechi, L.A. Epstein Barr Virus and Mycobacterium avium subsp. paratuberculosis peptides are recognized in sera and cerebrospinal fluid of MS patients. Sci. Rep. 2016, 6, 22401. [Google Scholar] [CrossRef] [PubMed]
- Mameli, G.; Madeddu, G.; Cossu, D.; Galleri, G.; Manetti, R.; Babudieri, S.; Mura, M.S.; Sechi, L.A. Immune response induced by Epstein-Barr virus and Mycobacterium avium subsp. paratuberculosis peptides in current and past infectious mononucleosis: A risk for multiple sclerosis? Eur. J. Neurol. 2016, 23, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Frau, J.; Cossu, D.; Coghe, G.; Lorefice, L.; Fenu, G.; Porcu, G.; Sardu, C.; Murru, M.R.; Tranquilli, S.; Marrosu, M.G.; et al. Role of interferon-beta in Mycobacterium avium subspecies paratuberculosis antibody response in Sardinian MS patients. J. Neurol. Sci. 2015, 349, 249–250. [Google Scholar] [CrossRef] [PubMed]
- Cossu, D.; Mameli, G.; Galleri, G.; Cocco, E.; Masala, S.; Frau, J.; Marrosu, M.G.; Manetti, R.; Sechi, L.A. Human interferon regulatory factor 5 homologous epitopes of Epstein-Barr virus and Mycobacterium avium subsp. paratuberculosis induce a specific humoral and cellular immune response in multiple sclerosis patients. Mult. Scler. 2015, 21, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Dow, C.T.; Sechi, L.A. Cows Get Crohn’s Disease and They’re Giving Us Diabetes. Microorganisms 2019, 7, 466. [Google Scholar] [CrossRef] [Green Version]
- Bo, M.; Arru, G.; Niegowska, M.; Erre, G.L.; Manchia, P.A.; Sechi, L.A. Association between Lipoprotein Levels and Humoral Reactivity to Mycobacterium avium subsp. paratuberculosis in Multiple Sclerosis, Type 1 Diabetes Mellitus and Rheumatoid Arthritis. Microorganisms 2019, 7, 423. [Google Scholar] [CrossRef] [Green Version]
- Niegowska, M.; Rapini, N.; Biet, F.; Piccinini, S.; Bay, S.; Lidano, R.; Manca Bitti, M.L.; Sechi, L.A. Seroreactivity against Specific L5P Antigen from Mycobacterium avium subsp. paratuberculosis in Children at Risk for T1D. PLoS ONE 2016, 11, e0157962. [Google Scholar] [CrossRef] [Green Version]
- Hesam Shariati, S.; Alaei, A.; Keshavarz, R.; Mosavari, N.; Rabbani, A.; Niegowska, M.; Sechi, L.A.; Feizabadi, M.M. Detection of Mycobacterium avium subsp. paratuberculosis in Iranian patients with type 1 diabetes mellitus by PCR and ELISA. J. Infect. Dev. Ctries. 2016, 10, 857–862. [Google Scholar] [CrossRef] [Green Version]
- Niegowska, M.; Rapini, N.; Piccinini, S.; Mameli, G.; Caggiu, E.; Manca Bitti, M.L.; Sechi, L.A. Type 1 Diabetes at-risk children highly recognize Mycobacterium avium subspecies paratuberculosis epitopes homologous to human Znt8 and Proinsulin. Sci. Rep. 2016, 6, 22266. [Google Scholar] [CrossRef] [Green Version]
- Masala, S.; Cossu, D.; Piccinini, S.; Rapini, N.; Mameli, G.; Manca Bitti, M.L.; Sechi, L.A. Proinsulin and MAP3865c homologous epitopes are a target of antibody response in new-onset type 1 diabetes children from continental Italy. Pediatr. Diabetes 2015, 16, 189–195. [Google Scholar] [CrossRef]
- Bo, M.; Erre, G.L.; Bach, H.; Slavin, Y.N.; Manchia, P.A.; Passiu, G.; Sechi, L.A. PtpA and PknG Proteins Secreted by Mycobacterium avium subsp. paratuberculosis are Recognized by Sera from Patients with Rheumatoid Arthritis: A Case-Control Study. J. Inflamm. Res. 2019, 12, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Naser, A.; Odeh, A.K.; Sharp, R.C.; Qasem, A.; Beg, S.; Naser, S.A. Polymorphisms in TNF Receptor Superfamily 1B (TNFRSF1B:rs3397) are Linked to Mycobacterium avium paratuberculosis Infection and Osteoporosis in Rheumatoid Arthritis. Microorganisms 2019, 7, 646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bo, M.; Erre, G.L.; Niegowska, M.; Piras, M.; Taras, L.; Longu, M.G.; Passiu, G.; Sechi, L.A. Interferon regulatory factor 5 is a potential target of autoimmune response triggered by Epstein-barr virus and Mycobacterium avium subsp. paratuberculosis in rheumatoid arthritis: Investigating a mechanism of molecular mimicry. Clin. Exp. Rheumatol. 2018, 36, 376–381. [Google Scholar] [PubMed]
- Zhang, P.; Minardi, L.M.; Kuenstner, J.T.; Zhang, S.T.; Zekan, S.M.; Kruzelock, R. Serological Testing for Mycobacterial Heat Shock Protein Hsp65 Antibody in Health and Diseases. Microorganisms 2019, 8, 47. [Google Scholar] [CrossRef] [Green Version]
- Pierce, E.S. How did Lou Gehrig get Lou Gehrig’s disease? Mycobacterium avium subspecies paratuberculosis in manure, soil, dirt, dust and grass and amyotrophic lateral sclerosis (motor neurone disease) clusters in football, rugby and soccer players. Med. Hypotheses 2018, 119, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Biet, F.; Gendt, L.; Anton, E.; Ballot, E.; Hugot, J.P.; Johanet, C. Serum antibodies to Mycobacterium avium subspecies paratuberculosis combined with anti-Saccharomyces cerevisiae antibodies in Crohn’s disease patients: Prevalence and diagnostic role. Dig. Dis. Sci. 2011, 56, 1794–1800. [Google Scholar] [CrossRef] [PubMed]
- Euesden, J.; Danese, A.; Lewis, C.M.; Maughan, B. A bidirectional relationship between depression and the autoimmune disorders—New perspectives from the National Child Development Study. PLoS ONE 2017, 12, e0173015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niegowska, M.; Paccagnini, D.; Burrai, C.; Palermo, M.; Sechi, L.A. Antibodies against Proinsulin and Homologous MAP Epitopes Are Detectable in Hashimoto’s Thyroiditis Sardinian Patients, an Additional Link of Association. PLoS ONE 2015, 10, e0133497. [Google Scholar] [CrossRef]
- Lin, T.M.; Chen, W.S.; Sheu, J.J.; Chen, Y.H.; Chen, J.H.; Chang, C.C. Autoimmune rheumatic diseases increase dementia risk in middle-aged patients: A nationwide cohort study. PLoS ONE 2018, 13, e0186475. [Google Scholar] [CrossRef] [Green Version]
- Arru, G.; Caggiu, E.; Paulus, K.; Sechi, G.P.; Mameli, G.; Sechi, L.A. Is there a role for Mycobacterium avium subspecies paratuberculosis in Parkinson’s disease? J. Neuroimmunol. 2016, 293, 86–90. [Google Scholar] [CrossRef]
- McClure, H.M.; Chiodini, R.J.; Anderson, D.C.; Swenson, R.B.; Thayer, W.R.; Coutu, J.A. Mycobacterium paratuberculosis infection in a colony of stumptail macaques (Macaca arctoides). J. Infect. Dis. 1987, 155, 1011–1019. [Google Scholar] [CrossRef]
- Ellingson, J.L.; Anderson, J.L.; Koziczkowski, J.J.; Radcliff, R.P.; Sloan, S.J.; Allen, S.E.; Sullivan, N.M. Detection of viable Mycobacterium avium subsp. paratuberculosis in retail pasteurized whole milk by two culture methods and PCR. J. Food Prot. 2005, 68, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Grant, I.R.; Ball, H.J.; Rowe, M.T. Incidence of Mycobacterium paratuberculosis in bulk raw and commercially pasteurized cows’ milk from approved dairy processing establishments in the United Kingdom. Appl. Environ. Microbiol. 2002, 68, 2428–2435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.H.; Kumar, N.; Sohal, H.S.; Singh, A.V.; Singh, P.K.; Agrawal, N.S.; Gupta, S.; Chaubey, K.K.; Kumar, A.; Rawat, K.D.; et al. First Mass Screening of the Human Population to Estimate the Bio-load of Mycobacterium avium Subspecies paratuberculosis in North India. J. Biol. Sci. 2014, 14, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Abubakar, I.; Myhill, D.; Aliyu, S.H.; Hunter, P.R. Detection of Mycobacterium avium subspecies paratuberculosis from patients with Crohn’s disease using nucleic acid-based techniques: A systematic review and meta-analysis. Inflamm. Bowel Dis. 2008, 14, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Feller, M.; Huwiler, K.; Stephan, R.; Altpeter, E.; Shang, A.; Furrer, H.; Pfyffer, G.E.; Jemmi, T.; Baumgartner, A.; Egger, M. Mycobacterium avium subspecies paratuberculosis and Crohn’s disease: A systematic review and meta-analysis. Lancet Infect. Dis. 2007, 7, 607–613. [Google Scholar] [CrossRef]
- Naser, S.A.; Ghobrial, G.; Romero, C.; Valentine, J.F. Culture of Mycobacterium avium subspecies paratuberculosis from the blood of patients with Crohn’s disease. Lancet 2004, 364, 1039–1044. [Google Scholar] [CrossRef]
- Naser, S.A.; Collins, M.T.; Crawford, J.T.; Valentine, J.F. Culture of Mycobacterium avium subspecies paratuberculosis (MAP) from the blood of patients with Crohn’s disease: A follow-up blind multi center investigation. Open Inflamm. J. 2009, 2, 22–23. [Google Scholar] [CrossRef]
- Kuenstner, J.T.; Naser, S.; Chamberlin, W.; Borody, T.; Graham, D.Y.; McNees, A.; Hermon-Taylor, J.; Hermon-Taylor, A.; Dow, C.T.; Thayer, W.; et al. The Consensus from the Mycobacterium avium ssp. paratuberculosis (MAP) Conference 2017. Front. Public Health 2017, 5, 208. [Google Scholar] [CrossRef]
- Bull, T.J.; Munshi, T.; Mikkelsen, H.; Hartmann, S.B.; Sorensen, M.R.; Garcia, J.S.; Lopez-Perez, P.M.; Hofmann, S.; Hilpert, K.; Jungersen, G. Improved Culture Medium (TiKa) for Mycobacterium avium Subspecies paratuberculosis (MAP) Matches qPCR Sensitivity and Reveals Significant Proportions of Non-viable MAP in Lymphoid Tissue of Vaccinated MAP Challenged Animals. Front. Microbiol. 2016, 7, 2112. [Google Scholar] [CrossRef]
- Bull, T.J.; McMinn, E.J.; Sidi-Boumedine, K.; Skull, A.; Durkin, D.; Neild, P.; Rhodes, G.; Pickup, R.; Hermon-Taylor, J. Detection and verification of Mycobacterium avium subsp. paratuberculosis in fresh ileocolonic mucosal biopsy specimens from individuals with and without Crohn’s disease. J. Clin. Microbiol. 2003, 41, 2915–2923. [Google Scholar] [CrossRef] [Green Version]
- Swift, B.M.; Convery, T.W.; Rees, C.E. Evidence of Mycobacterium tuberculosis complex bacteraemia in intradermal skin test positive cattle detected using phage-RPA. Virulence 2016, 7, 779–788. [Google Scholar] [CrossRef] [Green Version]
- Pozzato, N.; Gwozdz, J.; Gastaldelli, M.; Capello, K.; Dal Ben, C.; Stefani, E. Evaluation of a rapid and inexpensive liquid culture system for the detection of Mycobacterium avium subsp. paratuberculosis in bovine faeces. J. Microbiol. Methods 2011, 84, 413–417. [Google Scholar] [CrossRef]
- Grant, I.R.; Foddai, A.C.G.; Tarrant, J.C.; Kunkel, B.; Hartmann, F.A.; McGuirk, S.; Hansen, C.; Talaat, A.M.; Collins, M.T. Viable Mycobacterium avium ssp. paratuberculosis isolated from calf milk replacer. J. Dairy Sci. 2017, 100, 9723–9735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foddai, A.; Elliott, C.T.; Grant, I.R. Optimization of a phage amplification assay to permit accurate enumeration of viable Mycobacterium avium subsp. paratuberculosis cells. Appl. Environ. Microbiol. 2009, 75, 3896–3902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernstein, C.N.; Blanchard, J.F.; Rawsthorne, P.; Collins, M.T. Population-based case control study of seroprevalence of Mycobacterium paratuberculosis in patients with Crohn’s disease and ulcerative colitis. J. Clin. Microbiol. 2004, 42, 1129–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach, H.; Ko, H.H.; Raizman, E.A.; Attarian, R.; Cho, B.; Biet, F.; Enns, R.; Bressler, B. Immunogenicity of Mycobacterium avium subsp. paratuberculosis proteins in Crohn’s disease patients. Scand. J. Gastroenterol. 2011, 46, 30–39. [Google Scholar] [CrossRef]
- Bach, H.; Richard-Greenblatt, M.; Bach, E.; Chaffer, M.; Lai, W.; Keefe, G.; Begg, D.J. Protein Kinase G Induces an Immune Response in Cows Exposed to Mycobacterium avium Subsp. paratuberculosis. Biomed. Res. Int. 2018, 2018, 1450828. [Google Scholar] [CrossRef] [Green Version]
- Bach, H.; Papavinasasundaram, K.G.; Wong, D.; Hmama, Z.; Av-Gay, Y. Mycobacterium tuberculosis virulence is mediated by PtpA dephosphorylation of human vacuolar protein sorting 33B. Cell Host Microbe 2008, 3, 316–322. [Google Scholar] [CrossRef] [Green Version]
- Tasara, T.; Stephan, R. Development of an F57 sequence-based real-time PCR assay for detection of Mycobacterium avium subsp. paratuberculosis in milk. Appl. Environ. Microbiol. 2005, 71, 5957–5968. [Google Scholar] [CrossRef] [Green Version]
- Magombedze, G.; Ngonghala, C.N.; Lanzas, C. Evaluation [corrected] of the “Iceberg Phenomenon” in Johne’s disease through mathematical modelling. PLoS ONE 2013, 8, e76636. [Google Scholar] [CrossRef]
- Graham, D.Y. RHB-104, a Fixed-Dose, Oral Antibiotic Combination against Mycobacterium Avium Paratuberculosis (MAP) Infection, Is Effective in Moderately to Severely Active Crohn’s Disease. In Proceedings of the Annual Scientific Meeting and Postgraduate Course (ACG), San Antonio, TX, USA, 25–30 October 2019; pp. 25–30. [Google Scholar]



{kind=link}
{kind=link}
| Variable | CD Patients (2 also Had UC) (n = 61) | UC Patients only (n = 14) | Non-CD Patients (Including UC only Subjects) (n = 140) |
|---|---|---|---|
| Age, N | 61 | 13 | 130 |
| Mean (SD) | 46.2 (15.5) | 44.1 (17.3) | 52.6 (17.4) |
| Median (Range) | 47.0 (21.0–72.0) | 42.0 (24.0–80.0) | 57.5 (17.0–85.0) |
| Gender, N (%) | |||
| Female (%) | 33 (54.1%) | 7 (50.0%) | 82 (58.6%) |
| Male (%) | 28 (45.9%) | 7 (50.0%) | 58 (41.4%) |
| HB Index, N | 60 | 13 | NA |
| Mean (SD) | 2.4 (2.0) | 1.5 (1.8) | NA |
| Median (Range) | 2.0 (0.0–7.0) | 1.0 (0.0–5.0) | NA |
| Subject Category | Detection Method | |||
|---|---|---|---|---|
| Phage Assay | Pozzato Culture | TiKa Culture † | MGIT Culture | |
| CD *(n = 61) | 28 (46%) | 35 (57%) | 22 (36%) | 15 (25%) |
| UC only (n = 14) | 6 (43%) | 10 (71%) | 1 (7%) | 4 (29%) |
| Non-CD ** (n = 140) | 85 (61%) | 89 (64%) | 42 (30%) | 21 (15%) |
| All subjects (n = 201) | 113 (56%) | 124 (62%) | 64 (32%) | 36 (18%) |
| Variable | N | CD Patients (n = 61) | Non-CD Patients (n = 140) | Odds Ratio | Fisher’s Exact p-Value |
|---|---|---|---|---|---|
| Age, overall | 191 | 61 (31.9%) | 130 (68.1%) | 0.003 | |
| ≤52 | 91 | 39 (42.9%) | 52 (57.1%) | 2.66 (1.42, 4.99) | |
| >52 | 100 | 22 (22.0%) | 78 (78.0%) | Reference | |
| Gender, overall | 201 | 61 (30.3%) | 140 (69.7%) | 0.64 | |
| Male | 86 | 28 (32.6%) | 58 (67.4%) | 1.20 (0.65, 2.20) | |
| Female | 115 | 33 (28.7%) | 82 (71.3%) | Reference | |
| MGIT Culture, overall | 201 | 61 (30.3%) | 140 (69.7%) | 0.11 | |
| Positive | 36 | 15 (41.7%) | 21 (58.3%) | 1.85 (0.88, 3.89) | |
| Negative | 165 | 46 (27.9%) | 119 (72.1%) | Reference | |
| TiKa Culture, overall | 199 | 60 (30.2%) | 139 (69.8%) | 0.41 | |
| Positive | 64 | 22 (34.4%) | 42 (65.6%) | 1.34 (0.71, 2.53) | |
| Negative | 135 | 38 (28.1%) | 97 (71.9%) | Reference | |
| Pozzato Culture, overall | 201 | 61 (30.3%) | 140 (69.7%) | 0.43 | |
| Negative | 77 | 26 (33.8%) | 51 (66.2%) | 1.30 (0.70, 2.39) | |
| Positive | 124 | 35 (28.2%) | 89 (71.8%) | Reference | |
| Phage Assay, overall | 201 | 61 (30.3%) | 140 (69.7%) | 0.064 | |
| Negative | 88 | 33 (37.5%) | 55 (62.5%) | 1.82 (0.99, 3.34) | |
| Positive | 113 | 28 (24.8%) | 85 (75.2%) | Reference | |
| Hsp65 Antibody, overall | 201 | 61 (30.3%) | 140 (69.7%) | 0.020 | |
| >0.74 | 89 | 35 (39.3%) | 54 (60.7%) | 2.14 (1.16, 3.95) | |
| ≤0.74 | 112 | 26 (23.2%) | 86 (76.8%) | Reference | |
| PknG Antibody, overall | 200 | 61 (30.5%) | 139 (69.5%) | 0.35 | |
| Negative | 120 | 40 (33.3%) | 80 (66.7%) | 1.40 (0.75, 2.63) | |
| Positive | 80 | 21 (26.3%) | 59 (73.8%) | Reference | |
| PtpA Antibody, overall | 200 | 61 (30.5%) | 139 (69.5%) | 0.73 | |
| Negative | 146 | 46 (31.5%) | 100 (68.5%) | 1.20 (0.60, 2.39) | |
| Positive | 54 | 15 (27.8%) | 39 (72.2%) | Reference | |
| MAP IDEXX Ab, overall | 201 | 61 (30.3%) | 140 (69.7%) | 0.62 | |
| Positive | 135 | 43 (31.9%) | 92 (68.1%) | 1.25 (0.65, 2.39) | |
| Negative | 66 | 18 (27.3%) | 48 (72.7%) | Reference |
| Lab/Detection Method | ||||||||
|---|---|---|---|---|---|---|---|---|
| Subject Category | Naser/ MGIT Culture | Bull/ TiKa Culture | Grant/ Pozzato Culture | Grant/ Phage Assay | Potula/ IDEXX ELISA | Bach/ PtpA | Bach/ PknG | Zhang/ Hsp65 |
| CD patients (n = 61) | 15 (24.6%) | 22 (36.1%) | 35 (57.4%) | 28 (45.9%) | 43 (70.5%) | 14 (23.0%) | 21 (34.4%) | 39 (63.6) |
| UC patients (n = 14) | 4 (28.6%) | 1 (7.1%) | 10 (71.4%) | 6 (42.8%) | 8 (57.1%) | 4 (28.6%) | 3 (21.4%) | 6 (42.8%) |
| Non-CD or UC with autoimmune condition (n = 58) | 9 (15.5%) | 19 (32.7%) | 34 (58.6%) | 36 (62.0%) | 40 (68.9%) | 12 (20.7%) | 30 (51.7%) | 23 (39.6%) |
| Non-CD, non-UC and non-autoimmune condition (n = 68) | 8 (11.8%) | 22 (32.3%) | 44 (64.7%) | 43 (63.2%) | 44 (64.7%) | 23 (11.8%) | 26 (38.2%) | 26 (64.7%) |
| Assay Method | CD vs. Non-CD | CD + UC vs. Non-CD + UC | ||||
|---|---|---|---|---|---|---|
| n | Adjusted Odds Ratio (95% CI) | p-Value | n | Adjusted Odds Ratio (95% CI) | p-Value | |
| Using Culture only | 191 | 191 | ||||
| MGIT Culture (+ vs. −) | 2.36 (1.06, 5.28) | 0.037 | 3.19 (1.40, 7.23) | 0.006 | ||
| Using Antibody only | 191 | 190 | ||||
| Hsp65 Antibody (>0.74 vs. ≤0.74) | 2.40 (1.25, 4.61) | 0.009 | 1.32 (1.05, 1.67) ‡ | 0.016 | ||
| PknG Antibody (− vs. +) | NS | 2.18 (1.12, 4.23) | 0.022 | |||
| Using both Culture and Antibody | 191 | 190 | ||||
| MGIT Culture (+ vs. −) | 2.54 (1.11, 5.81) | 0.027 | 3.51 (1.51, 8.16) | 0.004 | ||
| Hsp65 Antibody (>0.74 vs. ≤0.74) | 2.51 (1.29, 4.88) | 0.007 | 2.30 (1.19, 4.45) | 0.013 | ||
| PknG Antibody (− vs. +) | NS | 2.13 (1.08, 4.20) | 0.030 | |||
| Phage Assay Result | Comparator Test Results | Total | Agreement between Tests | |
|---|---|---|---|---|
| N (%) | % | |||
| Pozzato + | Pozzato − | |||
| Phage assay + | 76 (38%) | 37 (18%) | 113 (56%) | 58% |
| Phage assay − | 48 (24%) | 40 (20%) | 88 (44%) | |
| Total N (%) | 124 (62%) | 77 (38%) | 201 | |
| TiKa + | TiKa − | |||
| Phage assay + | 35 (18%) | 76 (38%) | 111 (56%) | 47% |
| Phage assay − | 29 (14%) | 59 (30%) | 88 (44%) | |
| Total N (%) | 64 (32%) | 135 (68%) | 199 * | |
| MGIT + | MGIT − | |||
| Phage assay + | 22 (11%) | 91 (45%) | 113 (56%) | 48% |
| Phage assay − | 14 (7%) | 74 (37%) | 88 (44%) | |
| Total N (%) | 36 (18%) | 165 (82%) | 201 | |
| Any culture + | All culture − | |||
| Phage assay + | 91 (45%) | 22 (11%) | 113 (56%) | 56% |
| Phage assay − | 66 (33%) | 22 (11%) | 88 (44%) | |
| Total N (%) | 157 (78%) | 44 (22%) | 201 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuenstner, J.T.; Potula, R.; Bull, T.J.; Grant, I.R.; Foddai, A.; Naser, S.A.; Bach, H.; Zhang, P.; Yu, D.; Lu, X.; et al. Presence of Infection by Mycobacterium avium subsp. paratuberculosis in the Blood of Patients with Crohn’s Disease and Control Subjects Shown by Multiple Laboratory Culture and Antibody Methods. Microorganisms 2020, 8, 2054. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8122054
Kuenstner JT, Potula R, Bull TJ, Grant IR, Foddai A, Naser SA, Bach H, Zhang P, Yu D, Lu X, et al. Presence of Infection by Mycobacterium avium subsp. paratuberculosis in the Blood of Patients with Crohn’s Disease and Control Subjects Shown by Multiple Laboratory Culture and Antibody Methods. Microorganisms. 2020; 8(12):2054. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8122054
Chicago/Turabian StyleKuenstner, J. Todd, Raghava Potula, Tim J. Bull, Irene R. Grant, Antonio Foddai, Saleh A. Naser, Horacio Bach, Peilin Zhang, Daohai Yu, Xiaoning Lu, and et al. 2020. "Presence of Infection by Mycobacterium avium subsp. paratuberculosis in the Blood of Patients with Crohn’s Disease and Control Subjects Shown by Multiple Laboratory Culture and Antibody Methods" Microorganisms 8, no. 12: 2054. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8122054