
Serotypes in Adult Pneumococcal Pneumonia in Spain in the Era of Conjugate Vaccines

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hospital Setting, Study Period and Definitions
2.2. Bacterial Identification, Antimicrobial Susceptibility Testing and Serotyping
2.3. Statistical Analysis
3. Results
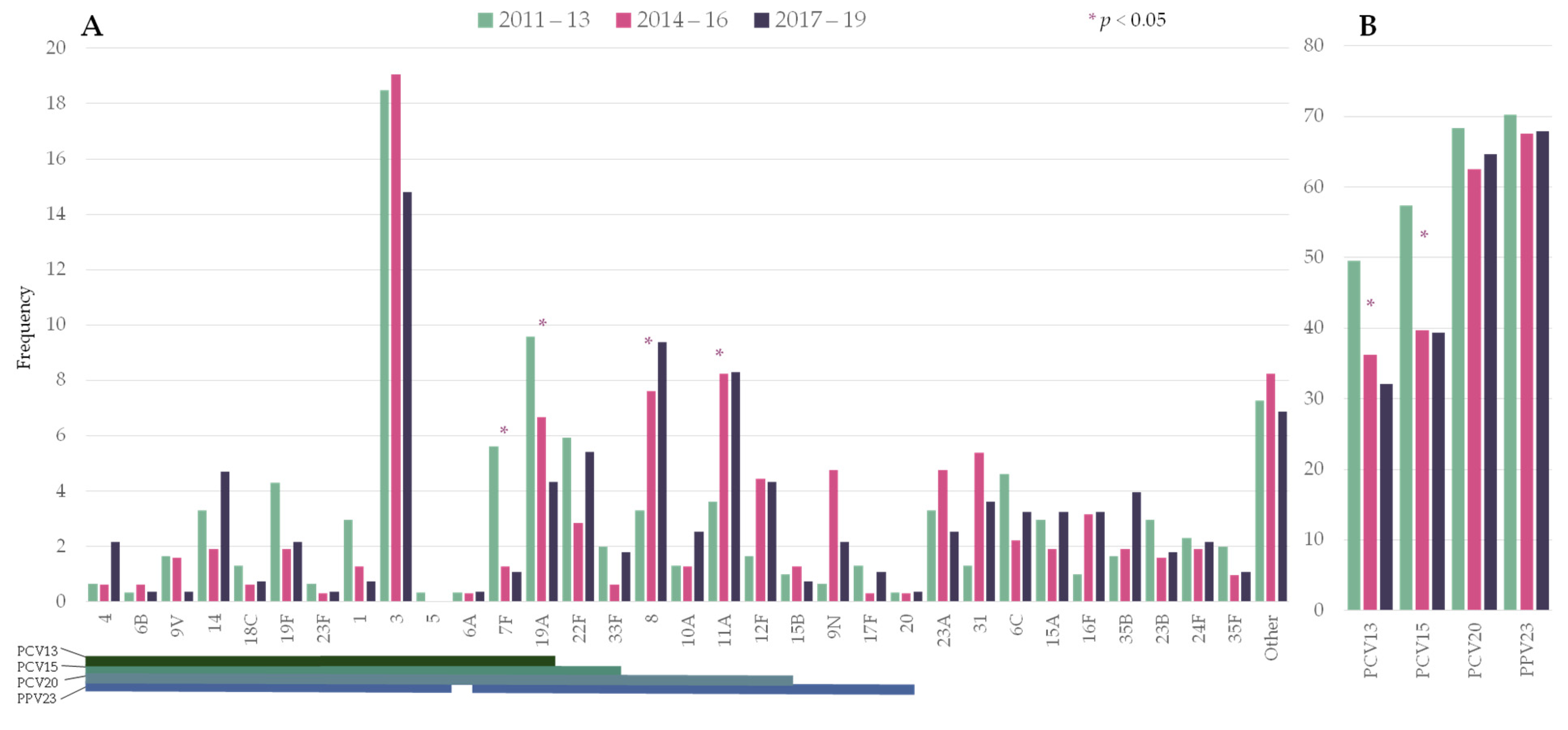
3.1. Changes in Serotype Distribution over the Study Period
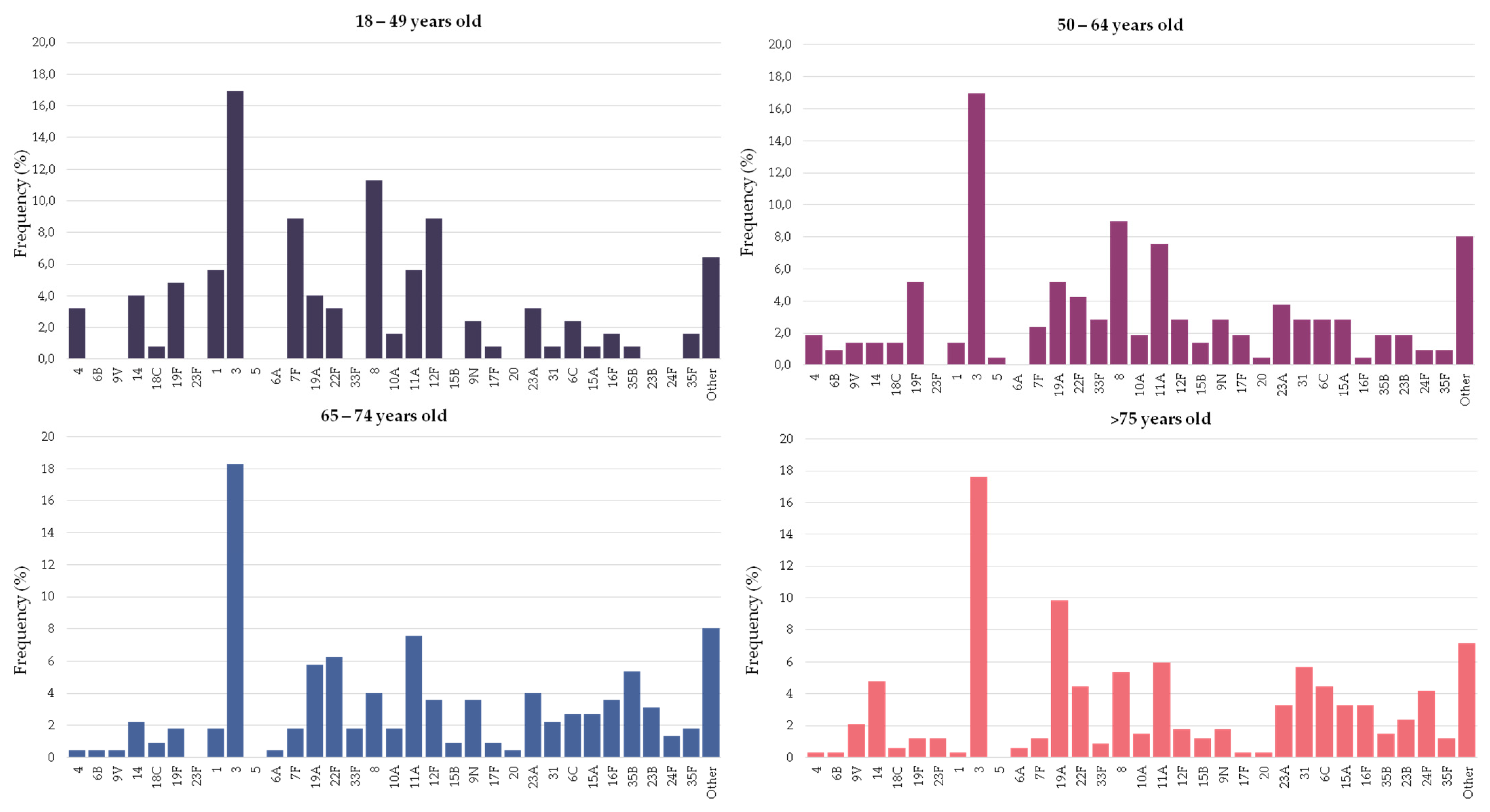
3.2. Distribution of Pneumococcal Serotypes Causing Pneumonia by Age Group
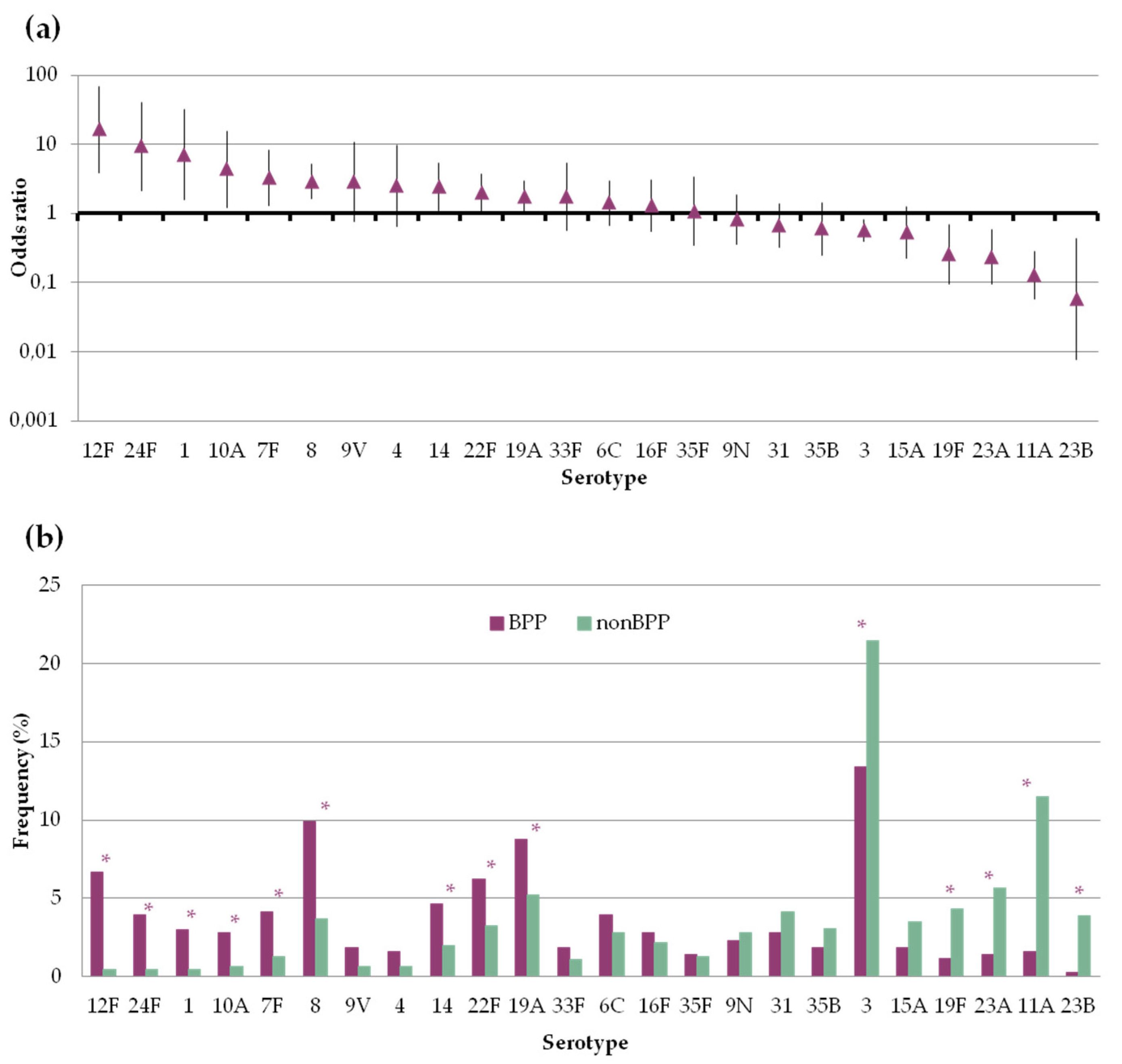
3.3. Differences in the Serotype Composition of Pneumococci Causing Bacteremic and Non-Bacteremic Pneumococcal Pneumonia
3.4. Antimicrobial Susceptibility
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Serotype | BPP n = 433 | Non–BPP n = 462 | OR (95% CI) |
|---|---|---|---|
| 12F | 29 | 2 | 16.51 (3.92–69.62) |
| 24F | 17 | 2 | 9.4 (2.16–40.93) |
| 1 | 13 | 2 | 7.12 (1.6–31.73) |
| 10A | 12 | 3 | 4.36 (1.22–15.56) |
| 7F | 18 | 6 | 3.3 (1.3–8.38) |
| 8 | 43 | 17 | 2.89 (1.62–5.14) |
| 9V | 8 | 3 | 2.88 (0.76–10.93) |
| 4 | 7 | 3 | 2.51 (0.65–9.78) |
| 14 | 20 | 9 | 2.44 (1.1–5.41) |
| 22F | 27 | 15 | 1.98 (1.04–3.78) |
| 19A | 38 | 24 | 1.76 (1.03–2.98) |
| 33F | 8 | 5 | 1.72 (0.56–5.3) |
| 6C | 17 | 13 | 1.41 (0.68–2.94) |
| 16F | 12 | 10 | 1.29 (0.55–3.01) |
| 35F | 6 | 6 | 1.07 (0.34–3.34) |
| 9N | 10 | 13 | 0.82 (0.35–1.88) |
| 31 | 12 | 19 | 0.66 (0.32–1.39) |
| 35B | 8 | 14 | 0.6 (0.25–1.45) |
| 3 | 58 | 99 | 0.57 (0.4–0.81) |
| 15A | 8 | 16 | 0.52 (0.22–1.24) |
| 19F | 5 | 20 | 0.26 (0.1–0.69) |
| 23A | 6 | 26 | 0.24 (0.1–0.58) |
| 11A | 7 | 53 | 0.13 (0.06–0.28) |
| 23B | 1 | 18 | 0.06 (0.01–0.43) |
References
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Simonetti, A.F.; van Werkhoven, C.H.; Schweitzer, V.A.; Viasus, D.; Carratalà, J.; Postma, D.F.; Oosterheert, J.J.; Bonten, M.J.M. Predictors for individual patient antibiotic treatment effect in hospitalized community-acquired pneumonia patients. Clin. Microbiol. Infect. 2017, 23, 774.e1–774.e7. [Google Scholar] [CrossRef] [Green Version]
- Darbà, J.; Marsà, A. Hospital incidence, in-hospital mortality and medical costs of pneumococcal disease in Spain (2008–2017): A retrospective multicentre study. Curr. Med. Res. Opin. 2021, 37, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Càmara, J.; Marimón, J.M.; Cercenado, E.; Larrosa, N.; Quesada, M.D.; Fontanals, D.; Cubero, M.; Pérez-Trallero, E.; Fenoll, A.; Liñares, J.; et al. Decrease of invasive pneumococcal disease (IPD) in adults after introduction of pneumococcal 13-valent conjugate vaccine in Spain. PLoS ONE 2017, 12, e0175224. [Google Scholar] [CrossRef]
- Bonten, M.J.M.; Huijts, S.M.; Bolkenbaas, M.; Webber, C.; Patterson, S.; Gault, S.; van Werkhoven, C.H.; van Deursen, A.M.M.; Sanders, E.A.M.; Verheij, T.J.M.; et al. Polysaccharide Conjugate Vaccine against Pneumococcal Pneumonia in Adults. N. Engl. J. Med. 2015, 372, 1114–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, N.J.; Waight, P.A.; Burbidge, P.; Pearce, E.; Roalfe, L.; Zancolli, M.; Slack, M.; Ladhani, S.N.; Miller, E.; Goldblatt, D. Serotype-specific effectiveness and correlates of protection for the 13-valent pneumococcal conjugate vaccine: A postlicensure indirect cohort study. Lancet Infect. Dis. 2014, 14, 839–846. [Google Scholar] [CrossRef]
- Vila-Córcoles, A.; Ochoa-Gondar, O.; de Diego, C.; Satué, E.; Vila-Rovira, A.; Aragón, M. Pneumococcal vaccination coverages by age, sex and specific underlying risk conditions among middle-aged and older adults in Catalonia, Spain, 2017. Eurosurveillance 2019, 24, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, E.D.; Berg, A.T.; Austrian, R.; Schroeder, D.; Parcells, V.; Margolis, A.; Adair, R.K.; Clemens, J.D. The protective efficacy of polyvalent pneumococcal polysaccharide vaccine. N. Engl. J. Med. 1991, 325, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Koivula, I.; Stén, M.; Leinonen, M.; Mäkelä, P.H. Clinical efficacy of pneumococcal vaccine in the elderly: A randomized, single-blind population-based trial. Am. J. Med. 1997, 103, 281–290. [Google Scholar] [CrossRef]
- Ortqvist, A.; Hedlund, J.; Burman, L.A.; Elbel, E.; Hofer, M.; Leinonen, M.; Lindblad, I.; Sundelof, S.; Kalin, M.; Aufwerber, E.; et al. Randomised trial of 23-valent pneumococcal capsular polysaccharide vaccine in prevention of pneumonia in middle-aged and elderly people. Lancet 1998, 351, 399–403. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, version 11.0; The European Committee on Antimicrobial Susceptibility Testing: Växjö, Sweden, 2021. [Google Scholar]
- List of Oligonucleotide Primers Used in 41 Conventional Multiplex PCR Assays for Pneumococcal Serotype Deduction of 70 Serotypes. CDC 2006. Available online: https://www.cdc.gov/streplab/downloads/pcr-oligonucleotide-primers.pdf (accessed on 30 August 2021).
- Hanquet, G.; Krizova, P.; Valentiner-Branth, P.; Ladhani, S.N.; Nuorti, J.P.; Lepoutre, A.; Mereckiene, J.; Knol, M.; Winje, B.A.; Ciruela, P.; et al. Effect of childhood pneumococcal conjugate vaccination on invasive disease in older adults of 10 European countries: Implications for adult vaccination. Thorax 2019, 74, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000–17: A prospective national observational cohort study. Lancet Infect. Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [Green Version]
- González-Díaz, A.; Càmara, J.; Ercibengoa, M.; Cercenado, E.; Larrosa, N.; Quesada, M.D.; Fontanals, D.; Cubero, M.; Marimón, J.M.; Yuste, J.; et al. Emerging non-13-valent pneumococcal conjugate vaccine (PCV13) serotypes causing adult invasive pneumococcal disease in the late-PCV13 period in Spain. Clin. Microbiol. Infect. 2020, 26, 753–759. [Google Scholar] [CrossRef]
- Torres, A.; Menéndez, R.; España, P.P.; Fernández-Villar, J.A.; Marimón, J.M.; Cilloniz, C.; Méndez, R.; Egurrola, M.; Botana-Rial, M.; Ercibengoa, M.; et al. The Evolution and Distribution of Pneumococcal Serotypes in Adults Hospitalized With Community-Acquired Pneumonia in Spain Using a Serotype-Specific Urinary Antigen Detection Test: The CAPA Study, 2011–2018. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pick, H.; Daniel, P.; Rodrigo, C.; Bewick, T.; Ashton, D.; Lawrence, H.; Baskaran, V.; Edwards-Pritchard, R.C.; Sheppard, C.; Eletu, S.D.; et al. Pneumococcal serotype trends, surveillance and risk factors in UK adult pneumonia, 2013-18. Thorax 2020, 75, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Isturiz, R.; Grant, L.; Gray, S.; Alexander-Parrish, R.; Jiang, Q.; Jodar, L.; Peyrani, P.; Ford, K.D.; Pride, M.W.; Self, W.H.; et al. Expanded Analysis of 20 Pneumococcal Serotypes Associated With Radiographically Confirmed Community-acquired Pneumonia in Hospitalized US Adults. Clin. Infect. Dis. 2021, 1–7. [Google Scholar] [CrossRef]
- Choi, E.H.; Zhang, F.; Lu, Y.; Malley, R. Strains Reduces the Protective Effect of Anti-Type 3 CPS Antibodies. Clin. Vaccine Immunol. 2016, 23, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Miguel, S.; Domenech, M.; González-Camacho, F.; Sempere, J.; Vicioso, D.; Sanz, J.C.; Comas, L.G.; Ardanuy, C.; Fenoll, A.; Yuste, J. Nationwide Trends of Invasive Pneumococcal Disease in Spain From 2009 Through 2019 in Children and Adults During the Pneumococcal Conjugate Vaccine Era. Clin. Infect. Dis. 2020, 1–10. [Google Scholar] [CrossRef]
- Silva-Costa, C.; Gomes-Silva, J.; Teodoro, I.; Ramirez, M.; Melo-Cristino, J. Invasive pneumococcal disease in adults in portugal: The importance of serotypes 8 and 3 (2015–2018). Microorganisms 2021, 9, 1016. [Google Scholar] [CrossRef]
- Sá-Leao, R.; Pinto, F.; Aguiar, S.; Nunes, S.; Carriço, J.A.; Frazao, N.; Gonçalves-Sousa, N.; Melo-Cristino, J.; De Lencastre, H.; Ramirez, M. Analysis of invasiveness of pneumococcal serotypes and clones circulating in portugal before widespread use of conjugate vaccines reveals heterogeneous behavior of clones expressing the same serotype. J. Clin. Microbiol. 2011, 49, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Càmara, J.; Grau, I.; González-Diáz, A.; Tubau, F.; Calatayud, L.; Cubero, M.; Domínguez, M.Á.; Linãres, J.; Yuste, J.; Pallarés, R.; et al. A historical perspective of MDR invasive pneumococcal disease in Spanish adults. J. Antimicrob. Chemother. 2021, 76, 507–515. [Google Scholar] [CrossRef]
- Lindstrand, A.; Galanis, I.; Darenberg, J.; Morfeldt, E.; Naucler, P.; Blennow, M.; Alfvén, T.; Henriques-Normark, B.; Örtqvist, Å. Unaltered pneumococcal carriage prevalence due to expansion of non-vaccine types of low invasive potential 8 years after vaccine introduction in Stockholm, Sweden. Vaccine 2016, 34, 4565–4571. [Google Scholar] [CrossRef] [Green Version]
- McCurdy, S.P.; Sheets, A.J.; Cammarata, S.K.; Vidal, J.E. Serotype distribution and antimicrobial susceptibility of Streptococcus pneumoniae isolates from a Phase III community-acquired bacterial pneumonia (CABP) trial. JAC-Antimicrob. Resist. 2021, 3, 1–5. [Google Scholar] [CrossRef]
- Gounder, P.P.; Bruden, D.; Rudolph, K.; Zulz, T.; Hurlburt, D.; Thompson, G.; Bruce, M.G.; Hennessy, T.W. Re-emergence of pneumococcal colonization by vaccine serotype 19F in persons aged ≥5 years after 13-valent pneumococcal conjugate vaccine introduction—Alaska, 2008–2013. Vaccine 2018, 36, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Suaya, J.A.; Mendes, R.E.; Sings, H.L.; Arguedas, A.; Reinert, R.R.; Jodar, L.; Isturiz, R.E.; Gessner, B.D. Streptococcus pneumoniae serotype distribution and antimicrobial nonsusceptibility trends among adults with pneumonia in the United States, 2009‒2017. J. Infect. 2020, 81, 557–566. [Google Scholar] [CrossRef]
- Rockett, R.J.; Oftadeh, S.; Bachmann, N.L.; Timms, V.J.; Kong, F.; Gilbert, G.L.; Sintchenko, V. Genome-wide analysis of Streptococcus pneumoniae serogroup 19 in the decade after the introduction of pneumococcal conjugate vaccines in Australia. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Naucler, P.; Galanis, I.; Petropoulos, A.; Granath, F.; Morfeldt, E.; Örtqvist, Å.; Henriques-Normark, B. Chronic disease and immunosuppression increase the risk for non-vaccine serotype pneumococcal disease—A nationwide population-based study. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Muñoz-Almagro, C.; Esteva, C.; Fernandez de Sevilla, M.; Selva, L.; Gene, A.; Pallares, R. Emergence of invasive pneumococcal disease caused by multidrug-resistant serotype 19A among children in Barcelona. J. Infect. 2009, 59, 75–82. [Google Scholar] [CrossRef]
- Ouldali, N.; Varon, E.; Levy, C.; Angoulvant, F.; Georges, S.; Ploy, M.C.; Kempf, M.; Cremniter, J.; Cohen, R.; Bruhl, D.L.; et al. Invasive pneumococcal disease incidence in children and adults in France during the pneumococcal conjugate vaccine era: An interrupted time-series analysis of data from a 17-year national prospective surveillance study. Lancet Infect. Dis. 2021, 21, 137–147. [Google Scholar] [CrossRef]
- Phillips, M.T.; Warren, J.L.; Givon-Lavi, N.; Tothpal, A.; Regev-Yochay, G.; Dagan, R.; Weinberger, D.M. Evaluating post-vaccine expansion patterns of pneumococcal serotypes. Vaccine 2020, 38, 7756–7763. [Google Scholar] [CrossRef]
- González-Díaz, A.; Machado, M.P.; Càmara, J.; Yuste, J.; Varon, E.; Domenech, M.; Del Grosso, M.; Marimón, J.M.; Cercenado, E.; Larrosa, N.; et al. Two multi-fragment recombination events resulted in the β-lactam-resistant serotype 11A-ST6521 related to Spain9V-ST156 pneumococcal clone spreading in south-western Europe, 2008 to 2016. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Shoji, H.; Vázquez-Sánchez, D.A.; Gonzalez-Diaz, A.; Cubero, M.; Tubau, F.; Santos, S.; García-Somoza, D.; Liñares, J.; Yuste, J.; Martí, S.; et al. Overview of pneumococcal serotypes and genotypes causing diseases in patients with chronic obstructive pulmonary disease in a Spanish hospital between 2013 and 2016. Infect. Drug Resist. 2018, 11, 1387–1400. [Google Scholar] [CrossRef] [Green Version]
- Domenech, A.; Ardanuy, C.; Calatayud, L.; Santos, S.; Tubau, F.; Grau, I.; Verdaguer, R.; Dorca, J.; Pallares, R.; Martin, R.; et al. Serotypes and genotypes of Streptococcus pneumoniae causing pneumonia and acute exacerbations in patients with chronic obstructive pulmonary disease. J. Antimicrob. Chemother. 2011, 66, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Van Hoek, A.J.; Sheppard, C.L.; Andrews, N.J.; Waight, P.A.; Slack, M.P.E.; Harrison, T.G.; Ladhani, S.N.; Miller, E. Pneumococcal carriage in children and adults two years after introduction of the thirteen valent pneumococcal conjugate vaccine in England. Vaccine 2014, 32, 4349–4355. [Google Scholar] [CrossRef]
- Desmet, S.; Wouters, I.; Van Heirstraeten, L.; Beutels, P.; Van Damme, P.; Malhotra-Kumar, S.; Maes, P.; Verhaegen, J.; Peetermans, W.E.; Lagrou, K.; et al. In-depth analysis of pneumococcal serotypes in Belgian children (2015–2018): Diversity, invasive disease potential, and antimicrobial susceptibility in carriage and disease. Vaccine 2021, 39, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Càmara, J.; Cubero, M.; Martín-Galiano, A.J.; García, E.; Grau, I.; Nielsen, J.B.; Worning, P.; Tubau, F.; Pallarés, R.; Ángeles Domínguez, M.; et al. Evolution of the b-lactam-resistant Streptococcus pneumoniae PMEN3 clone over a 30 year period in Barcelona, Spain. J. Antimicrob. Chemother. 2018, 73, 2941–2951. [Google Scholar] [CrossRef] [Green Version]
- Riedel, S.; Beekmann, S.E.; Heilmann, K.P.; Richter, S.S.; Garcia-De-Lomas, J.; Ferech, M.; Goosens, H.; Doern, G.V. Antimicrobial use in Europe and antimicrobial resistance in Streptococcus pneumoniae. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 485–490. [Google Scholar] [CrossRef]



| Serotype | Vaccine Type | 18–64 (%) n = 336 | >64 (%) n = 559 | p-Value | |||
|---|---|---|---|---|---|---|---|
| PCV13 | PCV15 | PCV20 | PPV23 | ||||
| 3 | X | X | X | X | 17.0 | 17.9 | NS |
| 8 | X | X | 9.8 | 4.8 | 0.006 | ||
| 11A | X | X | 6.8 | 6.6 | NS | ||
| 12F | X | X | 5.1 | 2.5 | 0.043 | ||
| 19F | X | X | X | X | 5.1 | 1.4 | 0.002 |
| 19A | X | X | X | X | 4.8 | 8.2 | 0.048 |
| 7F | X | X | X | X | 4.8 | 1.4 | 0.005 |
| 22F | X | X | X | 3.9 | 5.2 | NS | |
| 23A | 3.6 | 3.6 | NS | ||||
| 1 | X | X | X | X | 3.0 | 0.9 | NS |
| 9N | X | 2.7 | 3.8 | NS | |||
| 6C | 2.7 | 2.5 | NS | ||||
| 14 | X | X | X | X | 2.4 | 3.8 | NS |
| 4 | X | X | X | X | 2.4 | 0.4 | 0.014 |
| 31 | 2.1 | 4.3 | NS | ||||
| 15A | 2.1 | 3.0 | NS | ||||
| 10A | X | X | 1.8 | 1.6 | NS | ||
| 33F | X | X | X | 1.8 | 1.3 | NS | |
| 35B | 1.5 | 3.0 | NS | ||||
| 23B | 1.2 | 2.7 | NS | ||||
| 35F | 1.19 | 1.43 | NS | ||||
| 16F | 0.9 | 3.4 | 0.033 | ||||
| 9V | X | X | X | X | 0.9 | 3.0 | NS |
| 24F | 0.6 | 3.0 | 0.026 | ||||
| Other | 12.2 | 11.8 | NS | ||||
| (a) | BPP (n = 433) | Non-BPP (n = 462) | |||||
| Antibiotic | MIC50 | MIC90 | % | MIC50 | MIC90 | % | p-Value |
| Penicillin Amoxicillin | <0.06 | 1 | 26% | <0.06 | 2 | 29% | 0.29 |
| <0.06 | 1 | 11% | <0.06 | 2 | 17% | 0.009 | |
| Cefotaxime Erythromycin | <0.06 | 0.5 | 9% | <0.06 | 1 | 10% | 0.63 |
| <0.25 | >32 | 21% | <0.25 | >32 | 23% | 0.59 | |
| Levofloxacin | 1 | 1 | 1% | 0.5 | 1 | 2% | 0.44 |
| (b) | 18–64 (n = 336) | >65 (n = 559) | |||||
| Antibiotic | MIC50 | MIC90 | % | MIC50 | MIC90 | % | p-Value |
| Penicillin Amoxicillin | <0.06 | 1 | 24% | <0.06 | 2 | 30% | 0.045 |
| <0.06 | 1 | 13% | <0.06 | 2 | 14% | 0.76 | |
| Cefotaxime Erythromycin | <0.06 | 0.5 | 9% | <0.06 | 1 | 10% | 0.48 |
| <0.25 | >32 | 18% | <0.25 | >32 | 24% | 0.037 | |
| Levofloxacin | 1 | 1 | 1% | 1 | 1 | 2% | 0.39 |
| (c) | 2011–13 (n = 303) | 2017–19 (n = 277) | |||||
| Antibiotic | MIC50 | MIC90 | % | MIC50 | MIC90 | % | p-Value |
| Penicillin Amoxicillin | <0.06 | 1 | 31% | <0.06 | 2 | 26% | 0.15 |
| <0.06 | 1 | 14% | <0.06 | 2 | 15% | 0.72 | |
| Cefotaxime Erythromycin | <0.06 | 0.5 | 10% | <0.06 | 0.5 | 8% | 0.46 |
| <0.25 | >32 | 27% | <0.25 | >32 | 19% | 0.04 | |
| Levofloxacin | 1 | 1 | 2% | 1 | 1 | 1% | 0.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Delgado, L.; Càmara, J.; González-Díaz, A.; Grau, I.; Shoji, H.; Tubau, F.; Martí, S.; Domínguez, M.Á.; Carratalà, J.; Yuste, J.; et al. Serotypes in Adult Pneumococcal Pneumonia in Spain in the Era of Conjugate Vaccines. Microorganisms 2021, 9, 2245. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9112245
Fernández-Delgado L, Càmara J, González-Díaz A, Grau I, Shoji H, Tubau F, Martí S, Domínguez MÁ, Carratalà J, Yuste J, et al. Serotypes in Adult Pneumococcal Pneumonia in Spain in the Era of Conjugate Vaccines. Microorganisms. 2021; 9(11):2245. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9112245
Chicago/Turabian StyleFernández-Delgado, Lucía, Jordi Càmara, Aida González-Díaz, Immaculada Grau, Hisashi Shoji, Fe Tubau, Sara Martí, Mª Ángeles Domínguez, Jordi Carratalà, Jose Yuste, and et al. 2021. "Serotypes in Adult Pneumococcal Pneumonia in Spain in the Era of Conjugate Vaccines" Microorganisms 9, no. 11: 2245. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9112245