
A Phase II Study on the Use of Convalescent Plasma for the Treatment of Severe COVID-19- A Propensity Score-Matched Control Analysis


 , , , , , , , , ,
, , , , , , , , ,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients’ Inclusion Criteria and Longitudinal Analyses Performed
2.3. CP Infusion Treatment Protocol
2.4. CP Donors
2.5. Detection of Anti-SARS-CoV-2 Antibodies in the Donors and Recipients
2.6. Statistical Analysis
3. Results
3.1. CP Donors
3.2. CP Recipients: Clinical Characteristics
3.3. Control Group
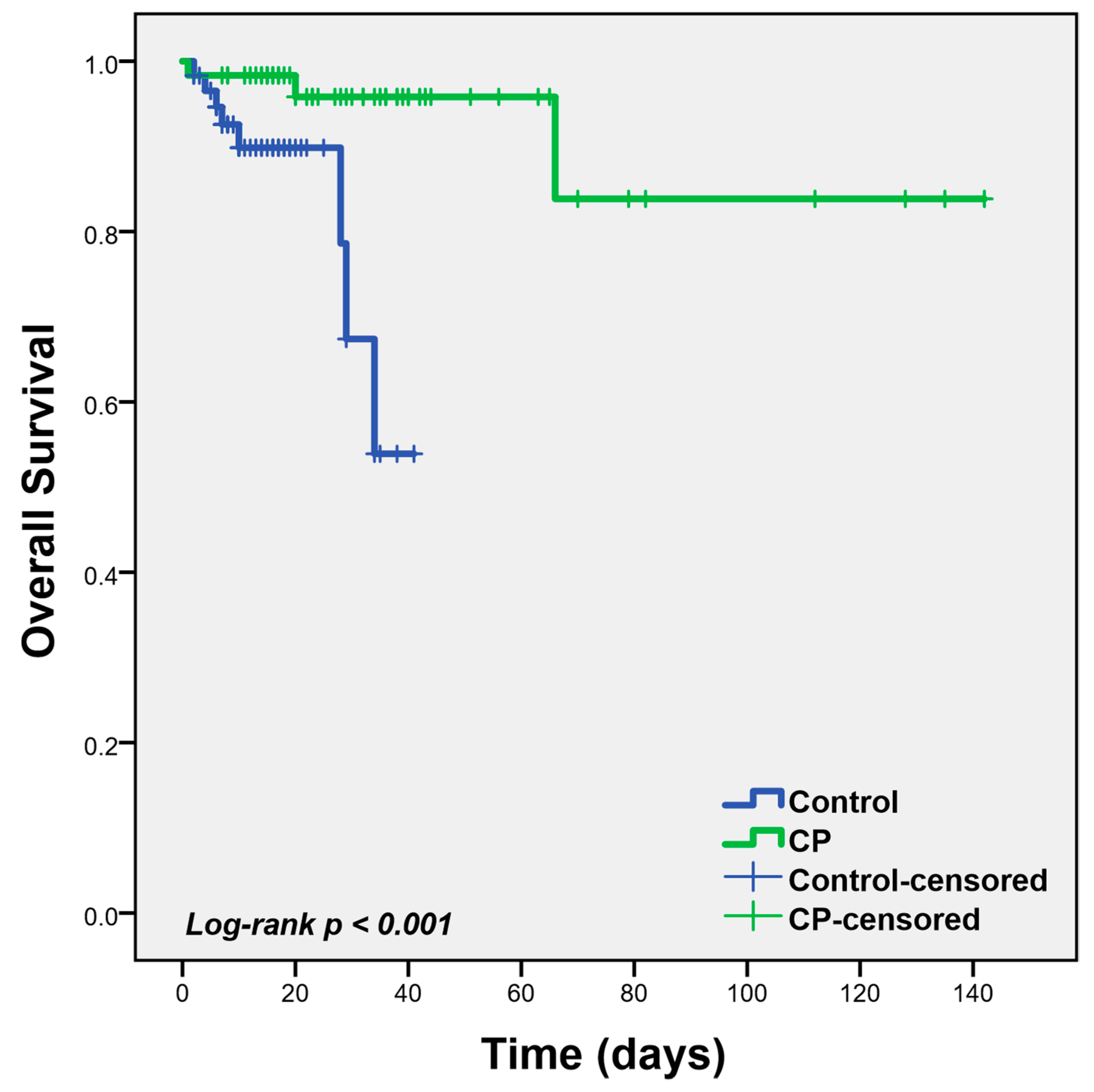
3.4. Outcomes
3.5. Adverse Events
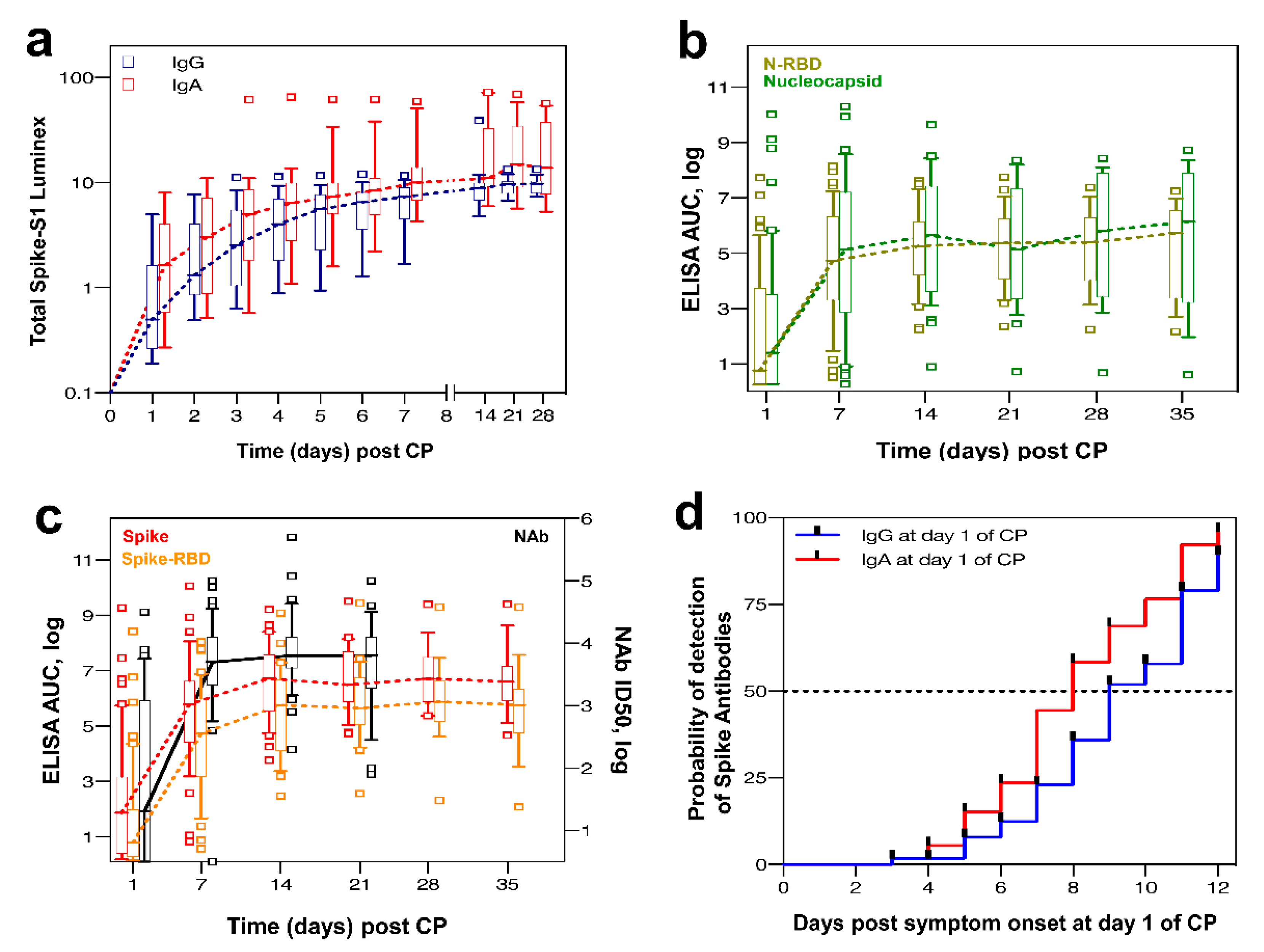
3.6. Longitudinal Analysis of Clinical and Laboratory Parameters in the CP Group
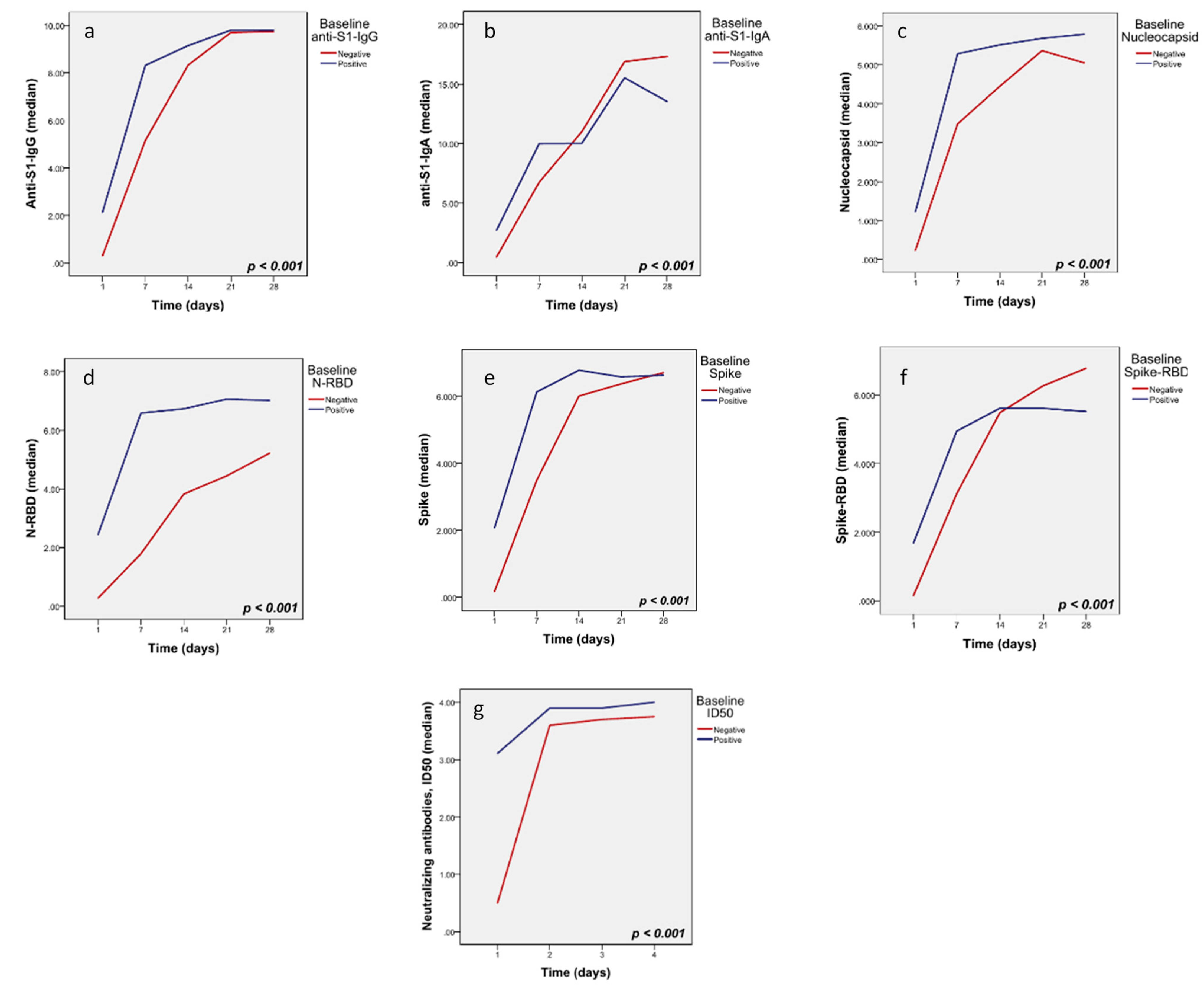
3.7. Subgroup Analysis by the Level of Antibodies at Baseline
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/publications-detail/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 1 March 2020).
- European Centre for Disease Prevention and Control. Novel Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK-Sixth Update-12 March 2020; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020. [Google Scholar]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Karpiński, T.M.; Ożarowski, M.; Seremak-Mrozikiewicz, A.; Wolski, H.; Wlodkowic, D. The 2020 race towards SARS-CoV-2 specific vaccines. Theranostics 2021, 11, 1690–1702. [Google Scholar] [CrossRef]
- Datta, P.K.; Liu, F.; Fischer, T.; Rappaport, J.; Qin, X. SARS-CoV-2 pandemic and research gaps: Understanding SARS-CoV-2 interaction with the ACE2 receptor and implications for therapy. Theranostics 2020, 10, 7448–7464. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA 2020, 323, 1612–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danzi, G.B.; Loffi, M.; Galeazzi, G.; Gherbesi, E. Acute pulmonary embolism and COVID-19 pneumonia: A random association? Eur. Heart J. 2020, 41, 1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E. Remdesivir for the Treatment of Covid-19-Preliminary Report. Reply. N. Engl. J. Med. 2020, 383, 994. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Lopes, M.I.; Bonjorno, L.P.; Giannini, M.C.; Amaral, N.B.; Menezes, P.I.; Dib, S.M.; Gigante, S.L.; Benatti, M.N.; Rezek, U.C.; Emrich-Filho, L.L.; et al. Beneficial effects of colchicine for moderate to severe COVID-19: A randomised, double-blinded, placebo-controlled clinical trial. RMD Open 2021, 7, e001455. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Sergentanis, T.N.; Pappa, V.; Politou, M.; Terpos, E.; Tsiodras, S.; Pavlakis, G.N.; Dimopoulos, M.A. The Emerging Role of Convalescent Plasma in the Treatment of COVID-19. Hemasphere 2020, 4, e409. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wong, R.; Soo, Y.O.; Wong, W.S.; Lee, C.K.; Ng, M.H.; Chan, P.; Wong, K.C.; Leung, C.B.; Cheng, G. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 44–46. [Google Scholar] [CrossRef]
- Lai, S.T. Treatment of severe acute respiratory syndrome. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 583–591. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Use of Convalescent Whole Blood or Plasma Collected from Patients Recovered from Ebola Virus Disease for Transfusion, As an Empirical Treatment during Outbreaks: Interim Guidance for National Health Authorities and Blood Transfusion Services; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Soo, Y.O.; Cheng, Y.; Wong, R.; Hui, D.S.; Lee, C.K.; Tsang, K.K.; Ng, M.H.; Chan, P.; Cheng, G.; Sung, J.J. Retrospective comparison of convalescent plasma with continuing high-dose methylprednisolone treatment in SARS patients. Clin. Microbiol. Infect. 2004, 10, 676–678. [Google Scholar] [CrossRef] [Green Version]
- Rojas, M.; Rodríguez, Y.; Monsalve, D.M.; Acosta-Ampudia, Y.; Camacho, B.; Gallo, J.E.; Rojas-Villarraga, A.; Ramírez-Santana, C.; Díaz-Coronado, J.C.; Manrique, R.; et al. Convalescent plasma in Covid-19: Possible mechanisms of action. Autoimmun. Rev. 2020, 19, 102554. [Google Scholar] [CrossRef] [PubMed]
- Abolghasemi, H.; Eshghi, P.; Cheraghali, A.M.; Imani Fooladi, A.A.; Bolouki Moghaddam, F.; Imanizadeh, S.; Moeini Maleki, M.; Ranjkesh, M.; Rezapour, M.; Bahramifar, A.; et al. Clinical efficacy of convalescent plasma for treatment of COVID-19 infections: Results of a multicenter clinical study. Transfus. Apher. Sci. 2020, 59, 102875. [Google Scholar] [CrossRef]
- Agarwal, A.; Mukherjee, A.; Kumar, G.; Chatterjee, P.; Bhatnagar, T.; Malhotra, P. Convalescent plasma in the management of moderate covid-19 in adults in India: Open label phase II multicentre randomised controlled trial (PLACID Trial). BMJ 2020, 371, m3939. [Google Scholar] [CrossRef]
- Altuntas, F.; Ata, N.; Yigenoglu, T.N.; Bascı, S.; Dal, M.S.; Korkmaz, S.; Namdaroglu, S.; Basturk, A.; Hacıbekiroglu, T.; Dogu, M.H.; et al. Convalescent plasma therapy in patients with COVID-19. Transfus. Apher. Sci. 2021, 60, 102955. [Google Scholar] [CrossRef]
- Avendaño-Solà, C.; Ramos-Martínez, A.; Muñez-Rubio, E.; Ruiz-Antorán, B.; de Molina, R.M.; Torres, F.; Fernández-Cruz, A.; Callejas-Díaz, A.; Calderón, J.; Payares-Herrera, C.; et al. Convalescent Plasma for COVID-19: A multicenter, randomized clinical trial. medRxiv 2020. [Google Scholar] [CrossRef]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [Green Version]
- Gharbharan, A.; Jordans, C.C.E.; Geurtsvankessel, C.; den Hollander, J.G.; Karim, F.; Mollema, F.P.N.; Stalenhoef-Schukken, J.E.; Dofferhoff, A.; Ludwig, I.; Koster, A.; et al. Convalescent Plasma for COVID-19. A randomized clinical trial. medRxiv 2020. [Google Scholar] [CrossRef]
- Joyner, M.J.; Senefeld, J.W.; Klassen, S.A.; Mills, J.R.; Johnson, P.W.; Theel, E.S.; Wiggins, C.C.; Bruno, K.A.; Klompas, A.M.; Lesser, E.R.; et al. Effect of Convalescent Plasma on Mortality among Hospitalized Patients with COVID-19: Initial Three-Month Experience. medRxiv 2020. [Google Scholar] [CrossRef]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients With Severe and Life-threatening COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 460–470. [Google Scholar] [CrossRef]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early High-Titer Plasma Therapy to Prevent Severe Covid-19 in Older Adults. N. Engl. J. Med. 2021, 384, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.T.H.; Lin, H.M.; Baine, I.; Wajnberg, A.; Gumprecht, J.P.; Rahman, F.; Rodriguez, D.; Tandon, P.; Bassily-Marcus, A.; Bander, J.; et al. Convalescent plasma treatment of severe COVID-19: A propensity score-matched control study. Nat. Med. 2020, 26, 1708–1713. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Clinical Memorandum: EUA 26382: Emergency Use Authorization (EUA) Request (Original Request 8/12/20; Amended Request 8/23/20). 12 August 2020. Available online: https://www.fda.gov/media/141481/download (accessed on 1 February 2021).
- Rasheed, A.M.; Fatak, D.F.; Hashim, H.A.; Maulood, M.F.; Kabah, K.K.; Almusawi, Y.A.; Abdulamir, A.S. The therapeutic potential of convalescent plasma therapy on treating critically-ill COVID-19 patients residing in respiratory care units in hospitals in Baghdad, Iraq. Infez. Med. 2020, 28, 357–366. [Google Scholar]
- Salazar, E.; Christensen, P.A.; Graviss, E.A.; Nguyen, D.T.; Castillo, B.; Chen, J.; Lopez, B.V.; Eagar, T.N.; Yi, X.; Zhao, P.; et al. Treatment of Coronavirus Disease 2019 Patients with Convalescent Plasma Reveals a Signal of Significantly Decreased Mortality. Am. J. Pathol. 2020, 190, 2290–2303. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L.; et al. Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, N.; Giunta, D.H.; Pérez, L.G.; Sánchez, M.D.L.; et al. A Randomized Trial of Convalescent Plasma in Covid-19 Severe Pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar] [CrossRef]
- Ye, M.; Fu, D.; Ren, Y.; Wang, F.; Wang, D.; Zhang, F.; Xia, X.; Lv, T. Treatment with convalescent plasma for COVID-19 patients in Wuhan, China. J. Med. Virol. 2020, 92, 1890–1901. [Google Scholar] [CrossRef] [Green Version]
- Shenoy, A.G.; Hettinger, A.Z.; Fernandez, S.J.; Blumenthal, J.; Baez, V. Early mortality benefit with COVID-19 convalescent plasma: A matched control study. Br. J. Haematol. 2021, 192, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Budhiraja, S.; Dewan, A.; Aggarwal, R.; Singh, O.; Juneja, D.; Pathak, S.; Singh, Y.P.; Gupta, A.; Rai, R.; Indrayan, A.; et al. Effectiveness of convalescent plasma in Indian patients with COVID-19. Blood Cells Mol. Dis. 2021, 88, 102548. [Google Scholar] [CrossRef]
- Allahyari, A.; Seddigh-Shamsi, M.; Mahmoudi, M.; Amel Jamehdar, S.; Amini, M.; Mozdourian, M.; Javidarabshahi, Z.; Eslami Hasan Abadi, S.; Amini, S.; Sedaghat, A.; et al. Efficacy and safety of convalescent plasma therapy in severe COVID-19 patients with acute respiratory distress syndrome. Int. Immunopharmacol. 2021, 93, 107239. [Google Scholar] [CrossRef] [PubMed]
- Tworek, A.; Jaroń, K.; Uszyńska-Kałuża, B.; Rydzewski, A.; Gil, R.; Deptała, A.; Franek, E.; Wójtowicz, R.; Życińska, K.; Walecka, I.; et al. Convalescent plasma treatment is associated with lower mortality and better outcomes in high-risk COVID-19 patients—propensity-score matched case-control study. Int. J. Infect. Dis. 2021, 105, 209–215. [Google Scholar] [CrossRef] [PubMed]
- AlShehry, N.; Zaidi, S.Z.A.; AlAskar, A.; Al Odayani, A.; Alotaibi, J.M.; AlSagheir, A.; Al-Eyadhy, A.; Balelah, S.; Salam, A.; Zaidi, A.R.Z.; et al. Safety and Efficacy of Convalescent Plasma for Severe COVID-19: Interim Report of a Multicenter Phase II Study from Saudi Arabia. Saudi J. Med. Med. Sci. 2021, 9, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Glingani, C.; Morandi, M.; Corghi, G.; Cerzosimo, S.; Beduzzi, G.; Storti, A.; Di Stasi, V.; Rastrelli, G.; Vignozzi, L.; et al. Safety and efficacy of convalescent plasma in elderly COVID-19 patients: The RESCUE trial. Mayo Clin. Proc. Innov. Qual. Outcomes 2021. [Google Scholar] [CrossRef]
- Balcells, M.E.; Rojas, L.; Le Corre, N.; Martínez-Valdebenito, C.; Ceballos, M.E.; Ferrés, M.; Chang, M.; Vizcaya, C.; Mondaca, S.; Huete, Á.; et al. Early versus deferred anti-SARS-CoV-2 convalescent plasma in patients admitted for COVID-19: A randomized phase II clinical trial. PLoS Med. 2021, 18, e1003415. [Google Scholar] [CrossRef]
- Donato, M.L.; Park, S.; Baker, M.; Korngold, R.; Morawski, A.; Geng, X.; Tan, M.; Ip, A.; Goldberg, S.; Rowley, S.; et al. Clinical and laboratory evaluation of patients with SARS-CoV-2 pneumonia treated with high-titer convalescent plasma. JCI Insight 2021, 6. [Google Scholar] [CrossRef]
- Kurtz, P.; Righy, C.; Gadelha, M.; Bozza, F.A.; Bozza, P.T.; Gonçalves, B.; Bastos, L.S.L.; Vale, A.M.; Higa, L.M.; Castilho, L.; et al. Effect of Convalescent Plasma in Critically Ill Patients With COVID-19: An Observational Study. Front. Med. (Lausanne) 2021, 8, 630982. [Google Scholar] [CrossRef] [PubMed]
- Sostin, O.V.; Rajapakse, P.; Cruser, B.; Wakefield, D.; Cruser, D.; Petrini, J. A matched cohort study of convalescent plasma therapy for COVID-19. J. Clin. Apher. 2021. [Google Scholar] [CrossRef] [PubMed]
- Klapholz, M.; Pentakota, S.R.; Zertuche, J.P.; McKenna, M.; Roque, W.; Forsberg, M.; Packer, J.; Lal, D.S.; Dever, L. Matched Cohort Study of Convalescent COVID-19 Plasma Treatment in Severely or Life Threateningly Ill COVID-19 Patients. Open Forum Infect. Dis. 2021, 8, ofab001. [Google Scholar] [CrossRef]
- FDA Issues Emergency Use Authorization for Convalescent Plasma as Potential Promising COVID–19 Treatment, An-other Achievement in Administration’s Fight Against Pandemic. Available online: https://www.fda.gov/news-events/press-announcements/fda-issues-emergency-use-authorization-convalescent-plasma-potential-promising-covid-19-treatment (accessed on 1 February 2021).
- FDA In Brief: FDA Updates Emergency Use Authorization for COVID-19 Convalescent Plasma to Reflect New Data. Available online: https://www.fda.gov/news-events/fda-brief/fda-brief-fda-updates-emergency-use-authorization-covid-19-convalescent-plasma-reflect-new-data#:~:text=Today%2C%20the%20FDA%20is%20revising,patients%20who%20have%20impaired%20humoral (accessed on 1 February 2021).
- Terpos, E.; Politou, M.; Sergentanis, T.N.; Mentis, A.; Rosati, M.; Stellas, D.; Bear, J.; Hu, X.; Felber, B.K.; Pappa, V.; et al. Anti-SARS-CoV-2 Antibody Responses in Convalescent Plasma Donors Are Increased in Hospitalized Patients; Subanalyses of a Phase 2 Clinical Study. Microorganisms 2020, 8, 1885. [Google Scholar] [CrossRef]
- Schmidt, F.; Weisblum, Y.; Muecksch, F.; Hoffmann, H.H.; Michailidis, E.; Lorenzi, J.C.C.; Mendoza, P.; Rutkowska, M.; Bednarski, E.; Gaebler, C.; et al. Measuring SARS-CoV-2 neutralizing antibody activity using pseudotyped and chimeric viruses. J. Exp. Med. 2020, 217. [Google Scholar] [CrossRef]
- Jones, A.E.; Trzeciak, S.; Kline, J.A. The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation. Crit. Care Med. 2009, 37, 1649–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyner, M.J.; Carter, R.E.; Senefeld, J.W.; Klassen, S.A.; Mills, J.R.; Johnson, P.W.; Theel, E.S.; Wiggins, C.C.; Bruno, K.A.; Klompas, A.M.; et al. Convalescent Plasma Antibody Levels and the Risk of Death from Covid-19. N. Engl. J. Med. 2021, 384, 1015–1027. [Google Scholar] [CrossRef]
- Liu, M.; Chen, Z.; Dai, M.Y.; Yang, J.H.; Chen, X.B.; Chen, D.; You, H.; Guo, X.; Leng, Y.; Yu, L.; et al. Lessons learned from early compassionate use of convalescent plasma on critically ill patients with Covid-19. Transfusion 2020, 60, 2210–2216. [Google Scholar] [CrossRef]
- Perotti, C.; Baldanti, F.; Bruno, R.; Del Fante, C.; Seminari, E.; Casari, S.; Percivalle, E.; Glingani, C.; Musella, V.; Belliato, M.; et al. Mortality reduction in 46 severe Covid-19 patients treated with hyperimmune plasma. A proof of concept single arm multicenter trial. Haematologica 2020, 105, 2834–2840. [Google Scholar] [CrossRef]
- Cantore, I.; Valente, P. Convalescent plasma from COVID 19 patients enhances intensive care unit survival rate. A preliminary report. Transfus. Apher. Sci. 2020, 59, 102848. [Google Scholar] [CrossRef]
- Joyner, M.J.; Bruno, K.A.; Klassen, S.A.; Kunze, K.L.; Johnson, P.W.; Lesser, E.R.; Wiggins, C.C.; Senefeld, J.W.; Klompas, A.M.; Hodge, D.O.; et al. Safety Update: COVID-19 Convalescent Plasma in 20,000 Hospitalized Patients. Mayo Clin. Proc. 2020, 95, 1888–1897. [Google Scholar] [CrossRef] [PubMed]
- Katzelnick, L.C.; Gresh, L.; Halloran, M.E.; Mercado, J.C.; Kuan, G.; Gordon, A.; Balmaseda, A.; Harris, E. Antibody-dependent enhancement of severe dengue disease in humans. Science 2017, 358, 929–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smatti, M.K.; Al Thani, A.A.; Yassine, H.M. Viral-Induced Enhanced Disease Illness. Front. Microbiol. 2018, 9, 2991. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.; Foo, S.S.; Bruzzone, R.; Dinh, L.V.; King, N.J.; Mahalingam, S. Fc receptors in antibody-dependent enhancement of viral infections. Immunol. Rev. 2015, 268, 340–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Convalescent Plasma Group (n = 59) | Control Group (n = 59) | p-Value | |
|---|---|---|---|
| Age, median (IQR) | 59 (18.0) | 59 (20) | 0.893 |
| <60 years % | 45.8 | 50.8 | |
| ≥60 years % | 55.2 | 49.2 | |
| Gender, % | 0.564 | ||
| Female | 32.2 | 37.3 | |
| Male | 67.8 | 62.7 | |
| Comorbidities, % | 61.0 | 62.7 | 0.393 |
| Diabetes | 19.3 | 28.3 | 0.269 |
| Arterial hypertension | 29.8 | 37.7 | 0.382 |
| Coronary artery disease | 7.0 | 13.2 | 0.282 |
| Heart failure | 3.5 | 9.4 | 0.205 |
| Pulmonary disease | 14.0 | 9.4 | 0.457 |
| Renal impairment | 8.8 | 11.3 | 0.276 |
| Solid tumor | 1.8 | 7.5 | 0.658 |
| Hematological malignancy | 3.5 | 1.9 | 0.603 |
| Symptoms, % | |||
| Fever | 98.2 | 96.6 | 0.571 |
| Myalgia | 8.8 | 10.3 | 0.775 |
| Cough | 56.1 | 48.3 | 0.401 |
| Dyspnea | 36.8 | 53.4 | 0.08 |
| Loss of taste | 8.8 | 3.4 | 0.235 |
| Anosmia | 5.3 | 5.2 | 0.983 |
| Diarrhea | 19.3 | 19.0 | 0.964 |
| Baseline laboratory parameters, median (IQR) | |||
| Lymphocytes, (109/L, NR: 1.1–4.0) | 1.17 (0.7) | 1.02 (0.6) | 0.207 |
| Platelets, (109/L, NR: 130–400) | 196 (101.5) | 197 (75.3) | 0.721 |
| CRP, (mg/L, NR: 0.00–6.00) | 47 (50.3) | 44.8 (71.9) | 0.772 |
| Fibrinogen, (mg/dL, NR: 200–400) | 485 (173) | 477 (253.9) | 0.631 |
| LDH, (U/L, NR: 135–225) | 315 (167.8) | 277 (127.3) | 0.165 |
| Ferritin, (ng/mL, NR: 13–150) | 597 (451.5) | 474 (167.9) | 0.443 |
| Intereukin-6, (pg/mL, NR: <7) | 30.5 (43.6) | ||
| SARS-CoV-2 PCR CT value | 26.8 (6.9) | 27.5 (9.3) | 0.700 |
| Percentage of infiltrates at baseline CT, % | 0.117 | ||
| <25 | 29.1 | 39.6 | |
| 25–50 | 38.2 | 43.8 | |
| 50–75 | 25.5 | 8.3 | |
| ≥75% | 7.3 | 8.3 | |
| Concomitant dexamethasone, % | 59.3 | 49.2 | 0.270 |
| Baseline SOFA score | 5 (4) | 4 (4) | 0.295 |
| Time from first symptom to diagnosis, median (IQR) | 3 (4] | 4 (3) | 0.265 |
| Time from first symptom to CP infusion, median (IQR) | 7 (4) | ||
| Time from diagnosis to CP infusion, median (IQR) | 3 (3) |
| Convalescent Plasma Group (n = 59) | Control Group (n = 59) | p-Value 1 | |
|---|---|---|---|
| Status at day 14 | n (%) | n (%) | 0.249 |
| Discharged | 21 (35.6) | 31 (52.5) | |
| Hospitalized | 30 (50.8) | 18 (30.5) | |
| In ICU | 8 (13.6) | 5 (8.5) | |
| Death | 0 (0.0) | 5 (8.5) | |
| Status at day 28 | n (%) | n (%) | 0.566 |
| Discharged | 48 (81.4) | 46 (78.0) | |
| Hospitalized | 5 (8.5) | 5 (8.5) | |
| In ICU | 5 (8.5) | 3 (5.1) | |
| Death | 1 (1.7) | 5 (8.5) | |
| Status at end of follow-up | n (%) | n (%) | 0.106 |
| Discharged | 56 (94.9 | 51 (86.4) | |
| Hospitalized | 0 (0.0) | 0 (0.0) | |
| In ICU | 1 (1.7) | 0 (0.0) | |
| Death | 2 (3.4) | 8 (13.6) | |
| Follow-up, median (IQR) | 29 (24) | 10 (11) | <0.001 |
| Duration of hospital stay, median (IQR) | 15 (10) | 10 (11) | 0.006 |
| Admission to ICU, n (%) | 16 (27.1) | 9 (15.3) | 0.116 |
| Exit from ICU, n (%) | 13 (22.0) | 2 (3.4) | 0.014 |
| Time to exit from ICU, median (IQR) | 12.5 (37.25) | 7 (NC) | 0.824 |
| Intubation, n (%) | 16 (27.1) | 8 (13.6) | 0.068 |
| Extubation, n (%) | 13 (22.0) | 1 (1.7) | 0.006 |
| Time to extubation, median (IQR) | 15 (35.5) | 17.5 (NC) | 0.837 |
| Duration of oxygen support, median (IQR) | 7 (11.5) | NA | |
| Achievement of negative PCR, n (%) | 37 (62.7) | 19 (52.8) | 0.167 |
| Time to PCR negativity, median (IQR) | 14 (14) | 9.5 (14.8) | 0.007 |
| Variables 2 | HR (95%CI) | p-Value 1 |
|---|---|---|
| Age | 1.08 (1.01–1.14) | 0.024 |
| Male gender | 1.22 (0.34–4.35) | 0.761 |
| Percentage of infiltrates at CT | 2.53 (1.24–5.19) | 0.011 |
| Baseline SOFA score | 1.29 (0.98–1.72) | 0.073 |
| Dexamethasone co-medication | 1.43 (0.39–5.19) | 0.586 |
| Convalescent plasma infusion | 0.05 (0.01–0.43) | 0.006 |
| N_RBD (In-house ELISA), below median | 0.07 (0.007–0.76) | 0.029 |
| N_RBD (In-house ELISA), above median | 0.04 (0.002–0.62) | 0.021 |
| Spike (In-house ELISA), below median | 0.07 (0.007–0.77) | 0.029 |
| Spike (In-house ELISA), above median | 0.04 (0.002–0.61) | 0.012 |
| Spike_RBD (In-house ELISA), below median | 0.07 (0.006–0.74) | 0.027 |
| Spike_RBD (In-house ELISA), above median | 0.04 (0.002–0.58) | 0.019 |
| ID50, below median | 0.08 (0.007–0.88) | 0.039 |
| ID50, above median | 0.04 (0.003–0.55) | 0.016 |
| Variables | HR (95%CI) | p-Value 1 |
|---|---|---|
| Age | 1.04 (0.97–1.12) | 0.233 |
| Percentage of infiltrates at CT | 3.87 (1.56–9.58) | 0.003 |
| Convalescent plasma infusion | 0.04 (0.004–0.36) | 0.005 |
| Subgroup analyses by level of plasma antibodies (cut -off: median) 2 | ||
| N_RBD (In-house ELISA), below median | 0.08 (0.006–1.09) | 0.059 |
| N_RBD (In-house ELISA), above median | 0.02 (0.001–0.34) | 0.007 |
| Spike (In-house ELISA), below median | 0.10 (0.008–1.21) | 0.070 |
| Spike (In-house ELISA), above median | 0.02 (0.001–0.33) | 0.007 |
| Spike_RBD (In-house ELISA), below median | 0.08 (0.007–1.003) | 0.051 |
| Spike_RBD (In-house ELISA), above median | 0.02 (0.001–0.35) | 0.008 |
| ID50, below median | 0.14 (0.01–1.91) | 0.139 |
| ID50, above median | 0.02 (0.001–0.29) | 0.016 |
| Variables | Effect Estimate (95%CI) | p-Value # |
|---|---|---|
| Clinical status at day 14 | OR: 1.50 (0.76–2.98) | 0.244 1 |
| Clinical status at day 28 | OR: 0.77 (0.31–1.88) | 0.565 1 |
| Clinical status at end of follow-up | OR: 0.33 (0.08–1.33) | 0.119 1 |
| Hospital discharge | OR: 2.93 (0.74–11.64) | 0.127 2 |
| Time to hospital discharge | HR: 0.68 (0.46–0.99) | 0.05 3 |
| Intubation | OR: 2.37 (0.93–6.01) | 0.072 2 |
| Time to intubation | HR: 0.48 (0.19–1.21) | 0.122 3 |
| Extubation | OR: 30.3 (2.64–348.9) | 0.006 2 |
| Time to extubation | HR: 0.68 (0.08–5.44) | 0.712 3 |
| Exit from ICU | OR: 15.16 (2.02–113.3) | 0.008 2 |
| Time to exit from ICU | HR: 0.54 (0.07–4.41) | 0.566 3 |
| Achievement of PCR negativity | OR: 1.84 (0.78–4.36) | 0.168 2 |
| Time to reach PCR negativity | HR: 0.74 (0.42–1.29) | 0.741 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pappa, V.; Bouchla, A.; Terpos, E.; Thomopoulos, T.P.; Rosati, M.; Stellas, D.; Antoniadou, A.; Mentis, A.; Papageorgiou, S.G.; Politou, M.; et al. A Phase II Study on the Use of Convalescent Plasma for the Treatment of Severe COVID-19- A Propensity Score-Matched Control Analysis. Microorganisms 2021, 9, 806. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040806
Pappa V, Bouchla A, Terpos E, Thomopoulos TP, Rosati M, Stellas D, Antoniadou A, Mentis A, Papageorgiou SG, Politou M, et al. A Phase II Study on the Use of Convalescent Plasma for the Treatment of Severe COVID-19- A Propensity Score-Matched Control Analysis. Microorganisms. 2021; 9(4):806. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040806
Chicago/Turabian StylePappa, Vasiliki, Anthi Bouchla, Evangelos Terpos, Thomas P. Thomopoulos, Margherita Rosati, Dimitris Stellas, Anastasia Antoniadou, Andreas Mentis, Sotirios G. Papageorgiou, Marianna Politou, and et al. 2021. "A Phase II Study on the Use of Convalescent Plasma for the Treatment of Severe COVID-19- A Propensity Score-Matched Control Analysis" Microorganisms 9, no. 4: 806. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040806