
A Large Retrospective Assessment of Voriconazole Exposure in Patients Treated with Extracorporeal Membrane Oxygenation

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Setting
2.2. Data Sources and Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
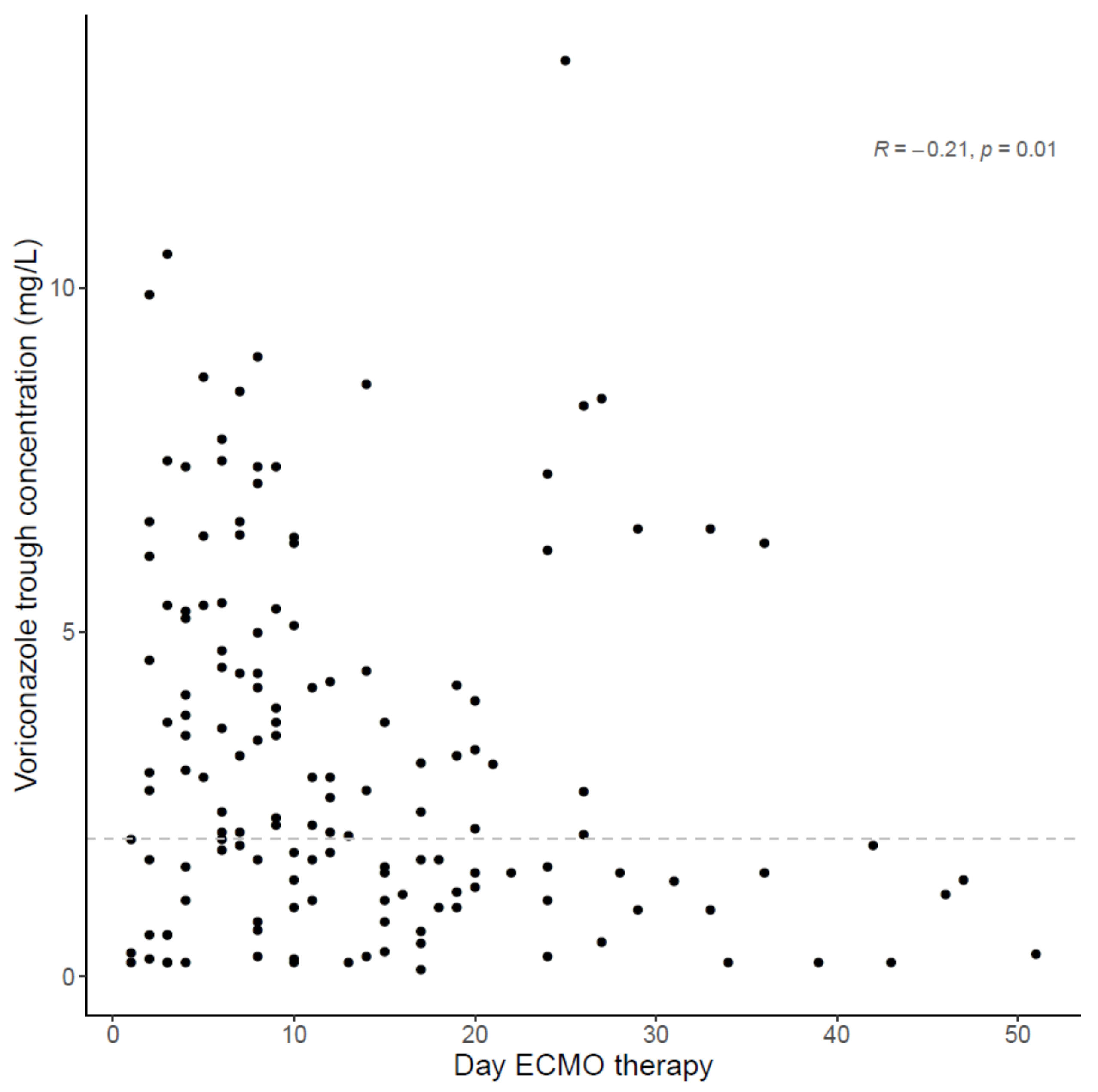
3.2. Extracorporeal Membrane Oxygenation
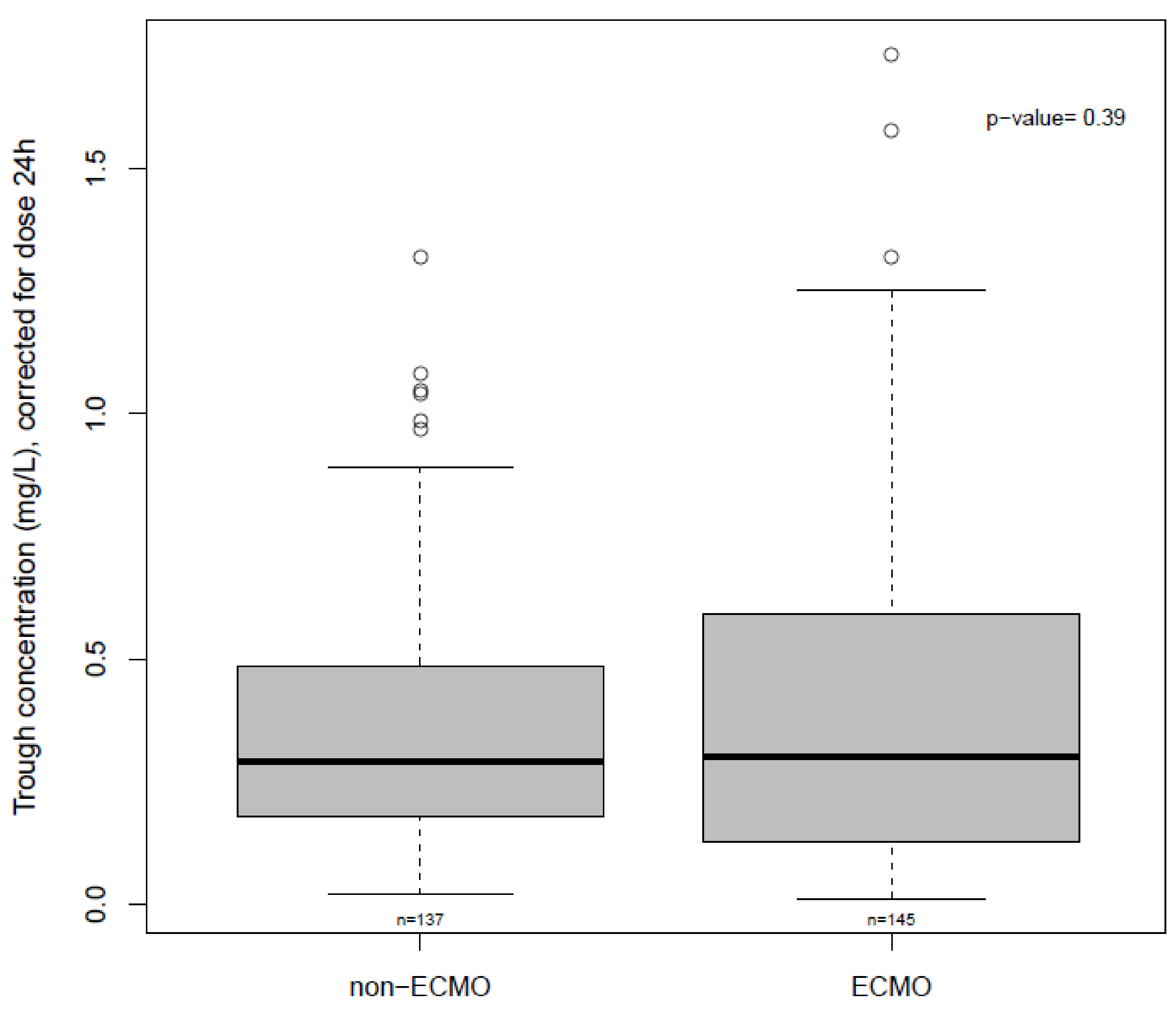
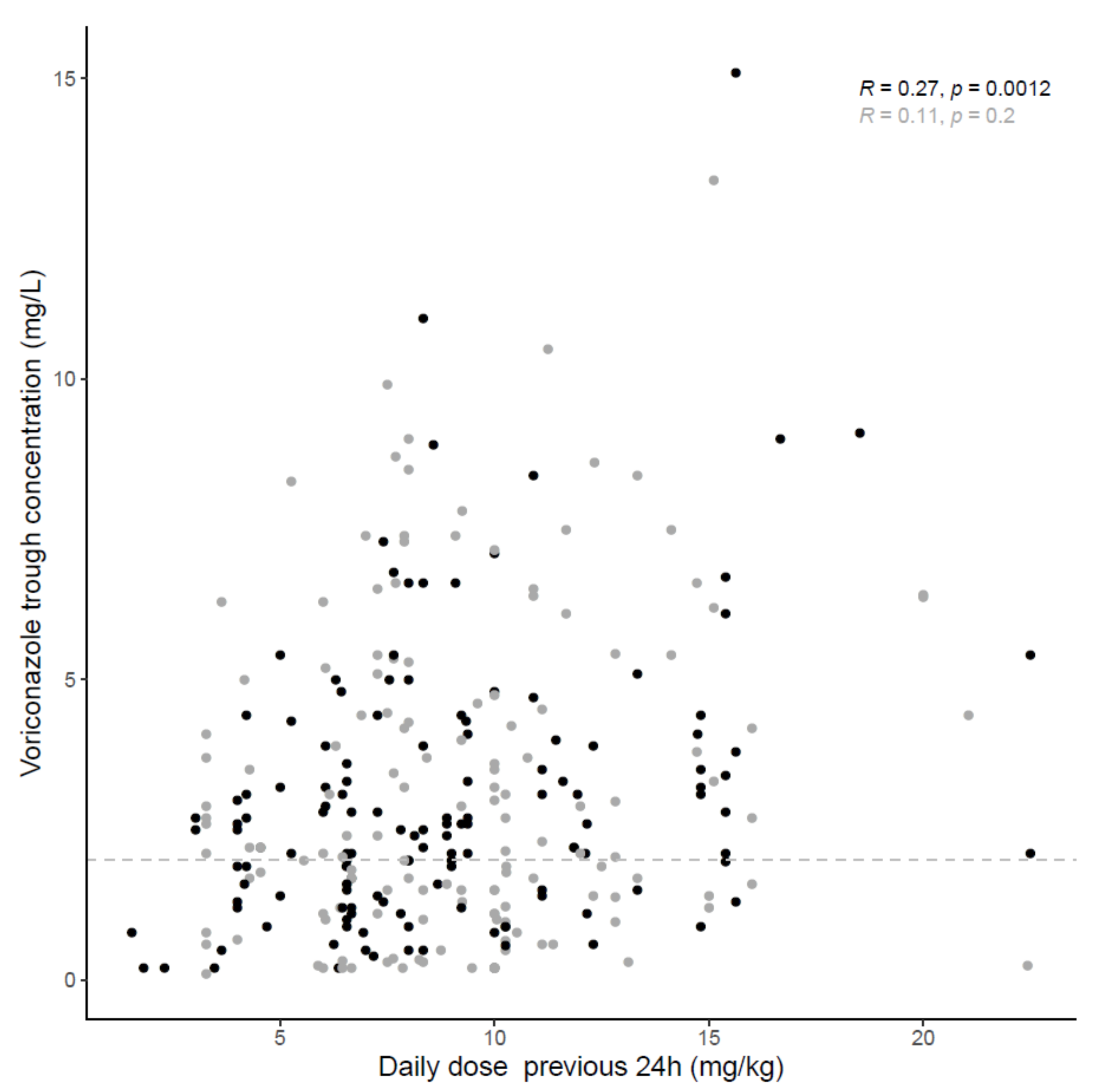
3.3. Voriconazole Concentrations
3.4. Generalized Estimating Equation (GEE) Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Leroux, S.; Ullmann, A.J. Management and diagnostic guidelines for fungal diseases in infectious diseases and clinical microbiology: Critical appraisal. Clin. Microbiol. Infect. 2013, 19, 1115–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Bouza, E. Invasive mould infections in the ICU setting: Complexities and solutions. J. Antimicrob. Chemother. 2017, 72, i39–i47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pascale, G.; Tumbarello, M. Fungal infections in the ICU: Advances in treatment and diagnosis. Curr. Opin. Crit. Care 2015, 21, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Cavayas, Y.A.; Yusuff, H.; Porter, R. Fungal infections in adult patients on extracorporeal life support. Crit. Care 2018, 22, 98. [Google Scholar] [CrossRef] [Green Version]
- Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Misset, B.; Meersseman, W.; Cardoso, T.; Paiva, J.A.; Blasco-Navalpotro, M.; De Laere, E.; Dimopoulos, G.; et al. Epidemiology of invasive aspergillosis in critically ill patients: Clinical presentation, underlying conditions, and outcomes. Crit. Care 2015, 19, 7. [Google Scholar] [CrossRef] [Green Version]
- Van Daele, R.; Brüggemann, R.J.; Dreesen, E.; Depuydt, P.; Rijnders, B.; Cotton, F.; Fage, D.; Gijsen, M.; Van Zwam, K.; Debaveye, Y.; et al. Pharmacokinetics and target attainment of intravenous posaconazole in critically ill patients during extracorporeal membrane oxygenation. J. Antimicrob. Chemother. 2021, 76, 1234–1241. [Google Scholar] [CrossRef]
- Wauters, J.; Baar, I.; Meersseman, P.; Meersseman, W.; Dams, K.; De Paep, R.; Lagrou, K.; Wilmer, A.; Jorens, P.; Hermans, G. Invasive pulmonary aspergillosis is a frequent complication of critically ill H1N1 patients: A retrospective study. Intensive Care Med. 2012, 38, 1761–1768. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; Van De Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; Perlin, D.S.; Lass-Flörl, C.; Hoenigl, M. COVID-19 Associated Pulmonary Aspergillosis (CAPA)-From Immunology to Treatment. J. Fungi 2020, 6, 91. [Google Scholar] [CrossRef]
- Hahn, J.; Choi, J.H.; Chang, M.J. Pharmacokinetic changes of antibiotic, antiviral, antituberculosis and antifungal agents during extracorporeal membrane oxygenation in critically ill adult patients. J. Clin. Pharm. Ther. 2017, 42, 661–671. [Google Scholar] [CrossRef]
- Mehta, N.M.; Halwick, D.R.; Dodson, B.L.; Thompson, J.E.; Arnold, J.H. Potential drug sequestration during extracorporeal membrane oxygenation: Results from an ex vivo experiment. Intensive Care Med. 2007, 33, 1018–1024. [Google Scholar] [CrossRef]
- Spriet, I.; Annaert, P.; Meersseman, P.; Hermans, G.; Meersseman, W.; Verbesselt, R.; Willems, L. Pharmacokinetics of caspofungin and voriconazole in critically ill patients during extracorporeal membrane oxygenation. J. Antimicrob. Chemother. 2009, 63, 767–770. [Google Scholar] [CrossRef] [Green Version]
- Mané, C.; Delmas, C.; Porterie, J.; Jourdan, G.; Verwaerde, P.; Marcheix, B.; Concordet, D.; Georges, B.; Ruiz, S.; Gandia, P. Influence of extracorporeal membrane oxygenation on the pharmacokinetics of ceftolozane/tazobactam: An ex vivo and in vivo study. J. Transl. Med. 2020, 18, 213. [Google Scholar] [CrossRef]
- Putowski, Z.; Szczepańska, A.; Czok, M.; Krzych, Ł. Veno-Venous Extracorporeal Membrane Oxygenation in COVID-19-Where Are We Now? Int. J. Environ. Res. Public Health 2021, 18, 1173. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, S.; Papy, E.; Da Silva, D.; Nataf, P.; Massias, L.; Wolff, M.; Bouadma, L. Potential voriconazole and caspofungin sequestration during extracorporeal membrane oxygenation. Intensive Care Med. 2009, 35, 183–184. [Google Scholar] [CrossRef]
- Schulz, J.; Kluwe, F.; Mikus, G.; Michelet, R.; Kloft, C. Novel insights into the complex pharmacokinetics of voriconazole: A review of its metabolism. Drug Metab. Rev. 2019, 51, 247–265. [Google Scholar] [CrossRef] [PubMed]
- Quintard, H.; Papy, E.; Massias, L.; Lasocki, S.; Arnaud, P.; Desmonts, J.M.; Montravers, P. The pharmacokinetic profile of voriconazole during continuous high-volume venovenous hemofiltration in a critically ill patient. Ther. Drug Monit. 2008, 30, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, A.; Thiboutot, Z.; Ferreira, V.; Benoit, P.; Grandjean Lapierre, S.; Hétu, P.O.; Halwagi, A. Voriconazole Sequestration During Extracorporeal Membrane Oxygenation for Invasive Lung Aspergillosis: A Case Report. ASAIO J. 2021. [Google Scholar] [CrossRef]
- Brüggemann, R.J.; Antonius, T.; Heijst, A.; Hoogerbrugge, P.M.; Burger, D.M.; Warris, A. Therapeutic drug monitoring of voriconazole in a child with invasive aspergillosis requiring extracorporeal membrane oxygenation. Ther. Drug Monit. 2008, 30, 643–646. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.L.; Chittick, P.J.; Richardson, C.L. Decreasing voriconazole requirement in a patient after extracorporeal membrane oxygenation discontinuation: A case report. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2020, e13545. [Google Scholar] [CrossRef]
- Raffaeli, G.; Cavallaro, G.; Allegaert, K.; Koch, B.C.P.; Mosca, F.; Tibboel, D.; Wildschut, E.D. Sequestration of Voriconazole and Vancomycin Into Contemporary Extracorporeal Membrane Oxygenation Circuits: An In Vitro Study. Front. Pediatr. 2020, 8, 468. [Google Scholar] [CrossRef] [PubMed]
- Cies, J.J.; Moore, W.S., 2nd; Giliam, N.; Low, T.; Marino, D.; Deacon, J.; Enache, A.; Chopra, A. Oxygenator impact on voriconazole in extracorporeal membrane oxygenation circuits. Perfusion 2020, 35, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Winiszewski, H.; Rougny, A.C.; Lagoutte-Renosi, J.; Millon, L.; Capellier, G.; Navellou, J.C.; Piton, G.; Clairet, A.L. The pharmacokinetic challenge of treating invasive aspergillosis complicating severe influenzae assisted by extracorporeal membrane oxygenation. Crit. Care 2018, 22, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myrianthefs, P.; Markantonis, S.L.; Evaggelopoulou, P.; Despotelis, S.; Evodia, E.; Panidis, D.; Baltopoulos, G. Monitoring plasma voriconazole levels following intravenous administration in critically ill patients: An observational study. Int. J. Antimicrob. Agents 2010, 35, 468–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoenigl, M.; Duettmann, W.; Raggam, R.B.; Seeber, K.; Troppan, K.; Fruhwald, S.; Prueller, F.; Wagner, J.; Valentin, T.; Zollner-Schwetz, I.; et al. Potential factors for inadequate voriconazole plasma concentrations in intensive care unit patients and patients with hematological malignancies. Antimicrob. Agents Chemother. 2013, 57, 3262–3267. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Li, M.; Yan, J.; Gao, L.; Zhou, L.; Wang, Y.; Li, Q.; Wang, J.; Chen, T.; Wang, T.; et al. Voriconazole therapeutic drug monitoring in critically ill patients improves efficacy and safety of antifungal therapy. Basic Clin. Pharmacol. Toxicol. 2020, 127, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.; Gordon, M.; Villarreal, E.; Peruccioni, M.; Marqués, M.R.; Poveda-Andrés, J.L.; Castellanos-Ortega, Á.; Ramirez, P. Impact of voriconazole plasma concentrations on treatment response in critically ill patients. J. Clin. Pharm. Ther. 2019, 44, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Yi, W.M.; Schoeppler, K.E.; Jaeger, J.; Mueller, S.W.; MacLaren, R.; Fish, D.N.; Kiser, T.H. Voriconazole and posaconazole therapeutic drug monitoring: A retrospective study. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 60. [Google Scholar] [CrossRef]
- Sebaaly, J.C.; MacVane, S.H.; Hassig, T.B. Voriconazole concentration monitoring at an academic medical center. Am. J. Health-Syst. Pharm. 2016, 73, S14–S21. [Google Scholar] [CrossRef]
- Lewis, R.; Brüggemann, R.; Padoin, C.; Maertens, J.; Marchetti, O.; Groll, A.; Joneson, E.; Arendrup, M. Triazole Antifungal Therapeutic Drug Monitoring. ECIL 6 Meeting 2015. Available online: http://www.ecil-leukaemia.com/telechargements2015/ECIL6-Triazole-TDM-07-12-2015-Lewis-R-et-al.pdf (accessed on 17 May 2021).
- Ashbee, H.R.; Barnes, R.A.; Johnson, E.M.; Richardson, M.D.; Gorton, R.; Hope, W.W. Therapeutic drug monitoring (TDM) of antifungal agents: Guidelines from the British Society for Medical Mycology. J. Antimicrob. Chemother. 2014, 69, 1162–1176. [Google Scholar] [CrossRef] [Green Version]
- Mulla, H.; Lawson, G.; Peek, G.J.; Firmin, R.K.; Upton, D.R. Plasma concentrations of midazolam in neonates receiving extracorporeal membrane oxygenation. ASAIO J. 2003, 49, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaindl, T.; Andes, D.; Engelhardt, M.; Saulay, M.; Larger, P.; Groll, A.H. Variability and exposure-response relationships of isavuconazole plasma concentrations in the Phase 3 SECURE trial of patients with invasive mould diseases. J. Antimicrob. Chemother. 2019, 74, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maertens, J.A.; Rahav, G.; Lee, D.G.; Ponce-de-León, A.; Ramírez Sánchez, I.C.; Klimko, N.; Sonet, A.; Haider, S.; Diego Vélez, J.; Raad, I.; et al. Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: A phase 3, randomised, controlled, non-inferiority trial. Lancet 2021, 397, 499–509. [Google Scholar] [CrossRef]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef]
- Zurl, C.; Waller, M.; Schwameis, F.; Muhr, T.; Bauer, N.; Zollner-Schwetz, I.; Valentin, T.; Meinitzer, A.; Ullrich, E.; Wunsch, S.; et al. Isavuconazole Treatment in a Mixed Patient Cohort with Invasive Fungal Infections: Outcome, Tolerability and Clinical Implications of Isavuconazole Plasma Concentrations. J. Fungi 2020, 6, 90. [Google Scholar] [CrossRef]
- Zhao, Y.; Seelhammer, T.G.; Barreto, E.F.; Wilson, J.W. Altered Pharmacokinetics and Dosing of Liposomal Amphotericin B and Isavuconazole during Extracorporeal Membrane Oxygenation. Pharmacotherapy 2020, 40, 89–95. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Extracorporeal Membrane Oxygenation (n = 69 Patients) | |
|---|---|
| Type of ECMO | |
| VV-ECMO, n (%) | 51 (74) |
| VA-ECMO, n (%) | 7 (10) |
| Switch between VV- and VA-ECMO, n (%) | 11 (16) |
| Oxygenator, n (%) | |
| Medos HILITE® 7000 LT (Medos Medizintechnik AG) | 36 (52) |
| Medos HILITE® 2400 LT (Medos Medizintechnik AG) | 1 (1.5) |
| Novalung® Heart and Lung Therapy System (Xenios) | 1 (1.5) |
| CardiohelpTM life support system (Maquet) | 1 (1.5) |
| Quadrox-D oxygenator (Maquet) | 2 (3) |
| AffinityTM oxygenation system (Medtronic) | 1 (1.5) |
| LivaNova ECMO oxygenators (Livanova) | 8 (12) |
| A.L.ONE ECMO oxygenator family (Eurosets) | 2 (3) |
| Unknown | 17 (25) |
| Bloodpump, n (%) | |
| Deltastream DP3 (Medos Medizintechnik AG) | 27 (39) |
| Jostra Rotaflow (Maquet) | 6 (9) |
| Cardiohelp (Maquet) | 2 (3) |
| Biomedicus (Medtronic) | 2 (3) |
| CentriMag (Levitronix) | 6 (9) |
| Revolution sorin (Livanova) | 11 (16) |
| Unknown | 15 (22) |
| At least one circuit change (or one of its components), n (%) | 22 (31.9) |
| Median (IQR) duration ECMO, days | 19 (11–33) |
| Continuous Renal Replacement Therapy During Study Period (CRRT) (n = 69 Patients) | |
| CRRT, n (%) | 35 (50.7) |
| CVVH, n (%) | 31 (88.6) |
| CVVHDF, n (%) | 4 (11.4) |
| Sampling Characteristics | Total | ECMO | Non-ECMO | p-Value c |
|---|---|---|---|---|
| Voriconazole Trough Concentrations of Sample Set A a | ||||
| Voriconazole Administration and Sampling | ||||
| Number of Cmin | 282 | 145 | 137 | NA |
| Trough concentration (mg/L), median (IQR) | 2.5 (1.3–4.3) | 2.4 (1.2–4.7) | 2.5 (1.4–3.9) | 0.58 |
| Previous daily dose (mg/kg), median (IQR) | 8.33 (6.6–11.1) | 9.2 (6.7–10.9) | 8.1 (6.5–11.1) | 0.76 |
| Number of Cmin per patient, median (IQR) | 3 (1–5) | 2 (1–3) | 3 (1–6) | NA |
| Severity of illness and type of RRT | ||||
| CRRT24, n (%) | 102 (36) | 78 (54) | 24 (18) | 0.03 |
| IHD24, n (%) | 33 (12) | 0 (0) | 33 (24) | <0.0001 |
| SOFA score on sampling day, median (IQR) | 11 (8–15) (n = 187) | 14 (11–17) (n = 90) | 8 (6–12) (n = 97) | <0.0001 |
| Variability | ||||
| Inter-subject variability (Cmin/dose) (%CV) | 43 | 47 | 46 | NA |
| Intra-subject variability (Cmin/dose) (%CV) | 73 | 78 | 60 | NA |
| Voriconazole trough concentrations of SAMPLE SET B b | ||||
| Voriconazole administration and sampling | ||||
| Number of Cmin | 337 | 190 | 147 | NA |
| Subtherapeutic Cmin (<2 mg/L), n (%) | 163 (48) | 106 (56) | 57 (39) | 0.80 |
| Therapeutic Cmin (2–5.5 mg/L), n (%) | 131 (39) | 55 (29) | 76 (52) | 0.37 |
| Supratherapeutic Cmin (>5.5 mg/L), n (%) | 43 (13) | 29 (15) | 14 (10) | 0.40 |
| Previous daily dose (mg/kg), median (IQR) | 8.3 (6.5–10.9) | 8.33 (6.6–10.9) | 8.0 (6.4–10.7) | 0.84 |
| Number of Cmin per patient, median (IQR) | 3 (2–6) | 2 (1–3) | 3 (1–7) | NA |
| Severity of illness and type of RRT | ||||
| CRRT24, n (%) | 127 (38) | 98 (52) | 29 (20) | 0.04 |
| IHD24, n (%) | 35 (10) | 0 (0) | 35 (24) | <0.0001 |
| SOFA score on sampling day, median (IQR) | 11 (8–15) (n = 215) | 13 (10–17) (n = 110) | 8 (6–12) (n = 105) | <0.0001 |
| Variability | ||||
| Inter-subject variability (Cmin/dose) (%CV) | 52 | 59 | 49 | NA |
| Intra-subject variability (Cmin/dose) (%CV) | 78 | 81 | 61 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Daele, R.; Bekkers, B.; Lindfors, M.; Broman, L.M.; Schauwvlieghe, A.; Rijnders, B.; Hunfeld, N.G.M.; Juffermans, N.P.; Taccone, F.S.; Coimbra Sousa, C.A.; et al. A Large Retrospective Assessment of Voriconazole Exposure in Patients Treated with Extracorporeal Membrane Oxygenation. Microorganisms 2021, 9, 1543. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071543
Van Daele R, Bekkers B, Lindfors M, Broman LM, Schauwvlieghe A, Rijnders B, Hunfeld NGM, Juffermans NP, Taccone FS, Coimbra Sousa CA, et al. A Large Retrospective Assessment of Voriconazole Exposure in Patients Treated with Extracorporeal Membrane Oxygenation. Microorganisms. 2021; 9(7):1543. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071543
Chicago/Turabian StyleVan Daele, Ruth, Britt Bekkers, Mattias Lindfors, Lars Mikael Broman, Alexander Schauwvlieghe, Bart Rijnders, Nicole G. M. Hunfeld, Nicole P. Juffermans, Fabio Silvio Taccone, Carlos Antônio Coimbra Sousa, and et al. 2021. "A Large Retrospective Assessment of Voriconazole Exposure in Patients Treated with Extracorporeal Membrane Oxygenation" Microorganisms 9, no. 7: 1543. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071543