
Combined Therapy with Intravenous Immunoglobulins, Letermovir and (Val-)Ganciclovir in Complicated Courses of CMV-Infection in Transplant Recipients

 , , , , and
, , , , and 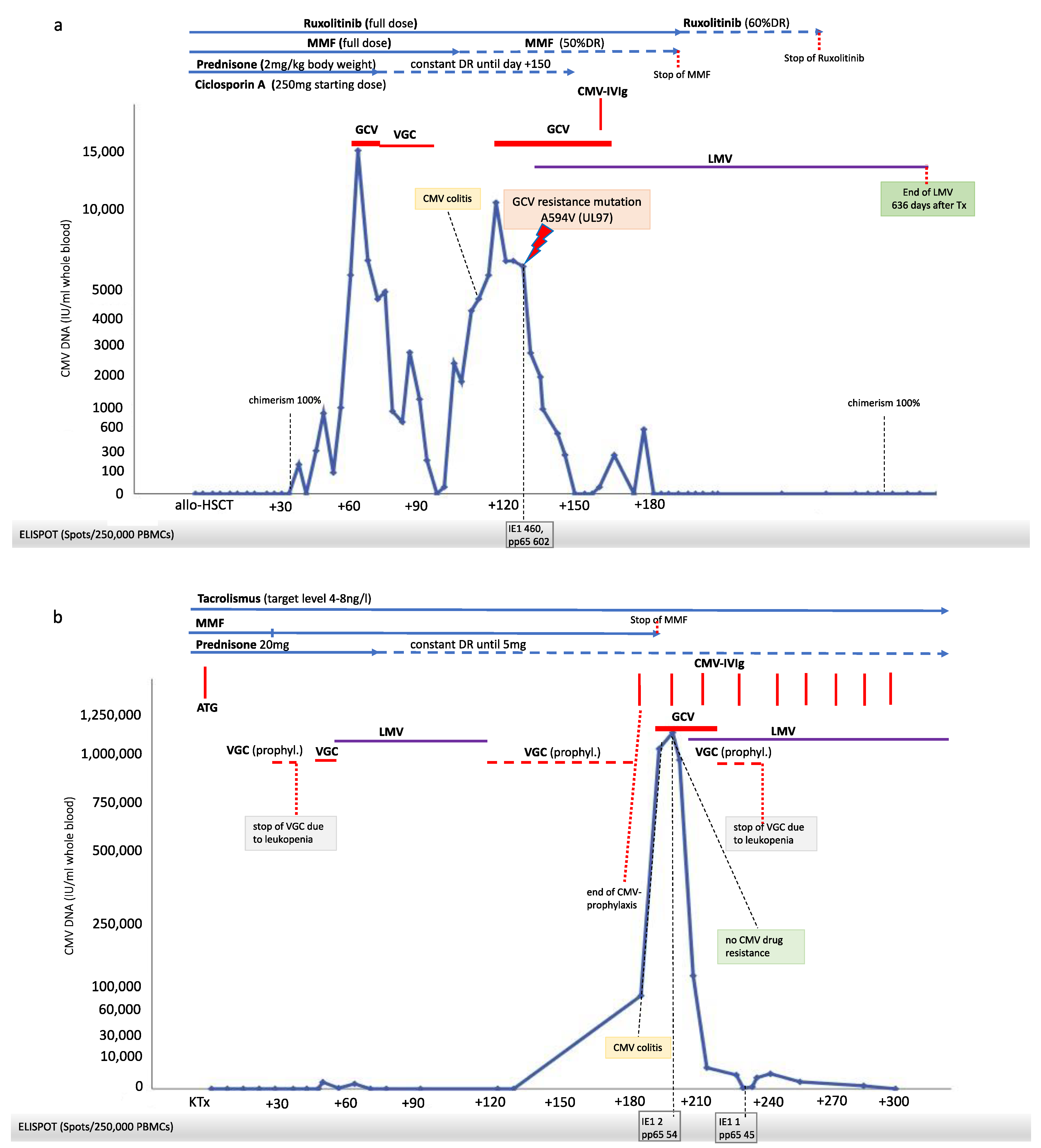{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
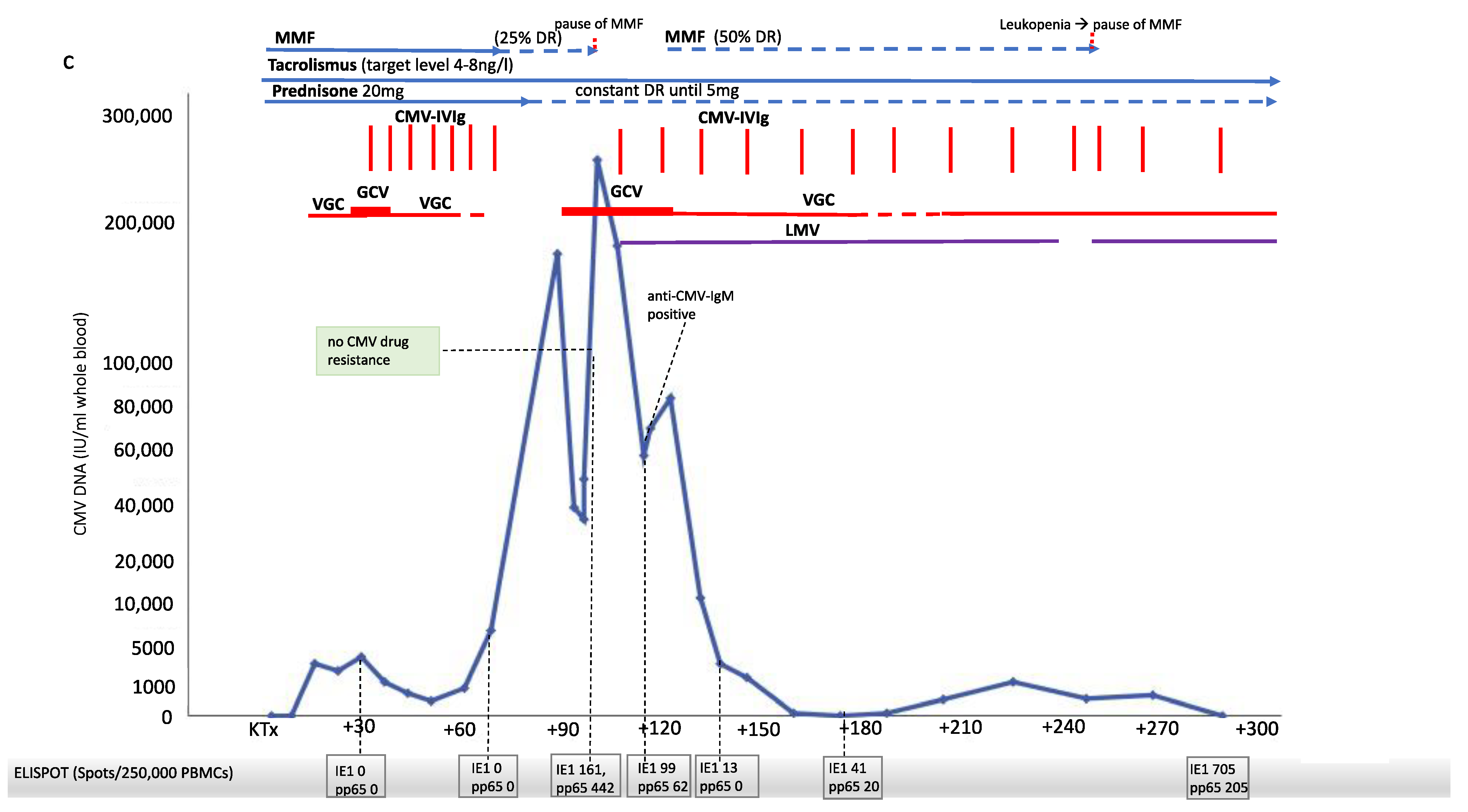
3. Clinical Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Keyzer, K.; Van Laecke, S.; Peeters, P.; Vanholder, R. Human cytomegalovirus and kidney transplantation: A clinician’s update. Am. J. Kidney Dis. 2011, 58, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Deleenheer, B.; Spriet, I.; Maertens, J. Pharmacokinetic drug evaluation of letermovir prophylaxis for cytomegalovirus in hematopoietic stem cell transplantation. Expert Opin. Drug Metab. Toxicol. 2018, 14, 1197–1207. [Google Scholar] [CrossRef] [PubMed]
- Kotton, C.N.; Kumar, D.; Caliendo, A.M.; Huprikar, S.; Chou, S.; Danziger-Isakov, L.; Humar, A. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation 2018, 102, 900–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowman, L.J.; Melaragno, J.I.; Brennan, D.C. Letermovir for the management of cytomegalovirus infection. Expert Opin. Investig. Drugs 2017, 26, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Razonable, R.R.; Humar, A. Cytomegalovirus in solid organ transplant recipients—Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13512. [Google Scholar] [CrossRef] [PubMed]
- Marty, F.M.; Ljungman, P.; Chemaly, R.F.; Maertens, J.; Dadwal, S.S.; Duarte, R.F.; Haider, S.; Ullmann, A.J.; Katayama, Y.; Brown, J.; et al. Letermovir Prophylaxis for Cytomegalovirus in Hematopoietic-Cell Transplantation. N. Engl. J. Med. 2017, 377, 2433–2444. [Google Scholar] [CrossRef] [PubMed]
- Winstead, R.J.; Kumar, D.; Brown, A.; Yakubu, I.; Song, C.; Thacker, L.; Gupta, G. Letermovir prophylaxis in solid organ transplant—Assessing CMV breakthrough and tacrolimus drug interaction. Transpl. Infect. Dis. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Schubert, L.; Fisecker, L.; Thalhammer, F.; Burgmann, H.; Steininger, C. Letermovir for the compassionate therapeutic use of cytomegalovirus infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Haidar, G.; Boeckh, M.; Singh, N. Cytomegalovirus Infection in Solid Organ and Hematopoietic Cell Transplantation: State of the Evidence. J. Infect. Dis. 2020, 221, S23–S31. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Chin-Hong, P.; Kayler, L.; Wojciechowski, D.; Limaye, A.P.; Osama Gaber, A.; Ball, S.; Mehta, A.K.; Cooper, M.; Blanchard, T.; et al. A prospective multicenter observational study of cell-mediated immunity as a predictor for cytomegalovirus infection in kidney transplant recipients. Am. J. Transplant. 2019, 19, 2505–2516. [Google Scholar] [CrossRef] [PubMed]
- Herling, M.; Schröder, L.; Awerkiew, S.; Chakupurakal, G.; Holtick, U.; Kaiser, R.; Pfister, H.; Scheid, C.; Di Cristanziano, V. Persistent CMV infection after allogeneic hematopoietic stem cell transplantation in a CMV-seronegative donor-to-positive recipient constellation: Development of multidrug resistance in the absence of anti-viral cellular immunity. J. Clin. Virol. 2016, 74, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Chiereghin, A.; Potena, L.; Borgese, L.; Gibertoni, D.; Squarzoni, D.; Turello, G.; Petrisli, E.; Piccirilli, G.; Gabrielli, L.; Grigioni, F.; et al. Monitoring of Cytomegalovirus (CMV)-Specific Cell-Mediated Immunity in Heart Transplant Recipients: Clinical Utility of the QuantiFERON-CMV Assay for Management of Posttransplant CMV Infection. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gliga, S.; Korth, J.; Krawczyk, A.; Wilde, B.; Horn, P.A.; Witzke, O.; Lindemann, M.; Fiedler, M. T-Track-CMV and QuantiFERON-CMV assays for prediction of protection from CMV reactivation in kidney transplant recipients. J. Clin. Virol. 2018, 105, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Aryal, S.; Katugaha, S.B.; Cochrane, A.; Brown, A.W.; Nathan, S.D.; Shlobin, O.A.; Ahmad, K.; Marinak, L.; Chun, J.; Fregoso, M.; et al. Single-center experience with use of letermovir for CMV prophylaxis or treatment in thoracic organ transplant recipients. Transpl. Infect. Dis. 2019, 21, e13166. [Google Scholar] [CrossRef] [PubMed]
- Popping, S.; Dalm, V.; Lübke, N.; Cristanziano, V.D.; Kaiser, R.; Boucher, C.A.B.; Van Kampen, J.J.A. Emergence and Persistence of Letermovir-Resistant Cytomegalovirus in a Patient with Primary Immunodeficiency. In Open Forum Infectious Diseases; Oxford University Press: New York, NY, USA, 2019; Volume 6. [Google Scholar] [CrossRef]
- El Haddad, L.; Ariza-Heredia, E.; Shah, D.P.; Jiang, Y.; Blanchard, T.; Ghantoji, S.S.; El Chaer, F.; El-Haddad, D.; Prayag, A.; Nesher, L.; et al. The Ability of a Cytomegalovirus ELISPOT Assay to Predict Outcome of Low-Level CMV Reactivation in Hematopoietic Cell Transplant Recipients. J. Infect. Dis. 2019, 219, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Sabin, C.A.; Lundgren, J.D. The natural history of HIV infection. Curr. Opin. HIV AIDS 2013, 8, 311–317. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Cristanziano, V.; Affeldt, P.; Trappe, M.; Wirtz, M.; Heger, E.; Knops, E.; Kaiser, R.; Stippel, D.; Müller, R.-U.; Holtick, U.; et al. Combined Therapy with Intravenous Immunoglobulins, Letermovir and (Val-)Ganciclovir in Complicated Courses of CMV-Infection in Transplant Recipients. Microorganisms 2021, 9, 1666. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9081666
Di Cristanziano V, Affeldt P, Trappe M, Wirtz M, Heger E, Knops E, Kaiser R, Stippel D, Müller R-U, Holtick U, et al. Combined Therapy with Intravenous Immunoglobulins, Letermovir and (Val-)Ganciclovir in Complicated Courses of CMV-Infection in Transplant Recipients. Microorganisms. 2021; 9(8):1666. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9081666
Chicago/Turabian StyleDi Cristanziano, Veronica, Patrick Affeldt, Moritz Trappe, Maike Wirtz, Eva Heger, Elena Knops, Rolf Kaiser, Dirk Stippel, Roman-Ulrich Müller, Udo Holtick, and et al. 2021. "Combined Therapy with Intravenous Immunoglobulins, Letermovir and (Val-)Ganciclovir in Complicated Courses of CMV-Infection in Transplant Recipients" Microorganisms 9, no. 8: 1666. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9081666