
Risk of Hemolytic Uremic Syndrome Related to Treatment of Escherichia coli O157 Infection with Different Antimicrobial Classes

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Outcomes
2.3. Data
2.4. Analyses
2.4.1. Primary Models
2.4.2. Secondary Models
3. Results
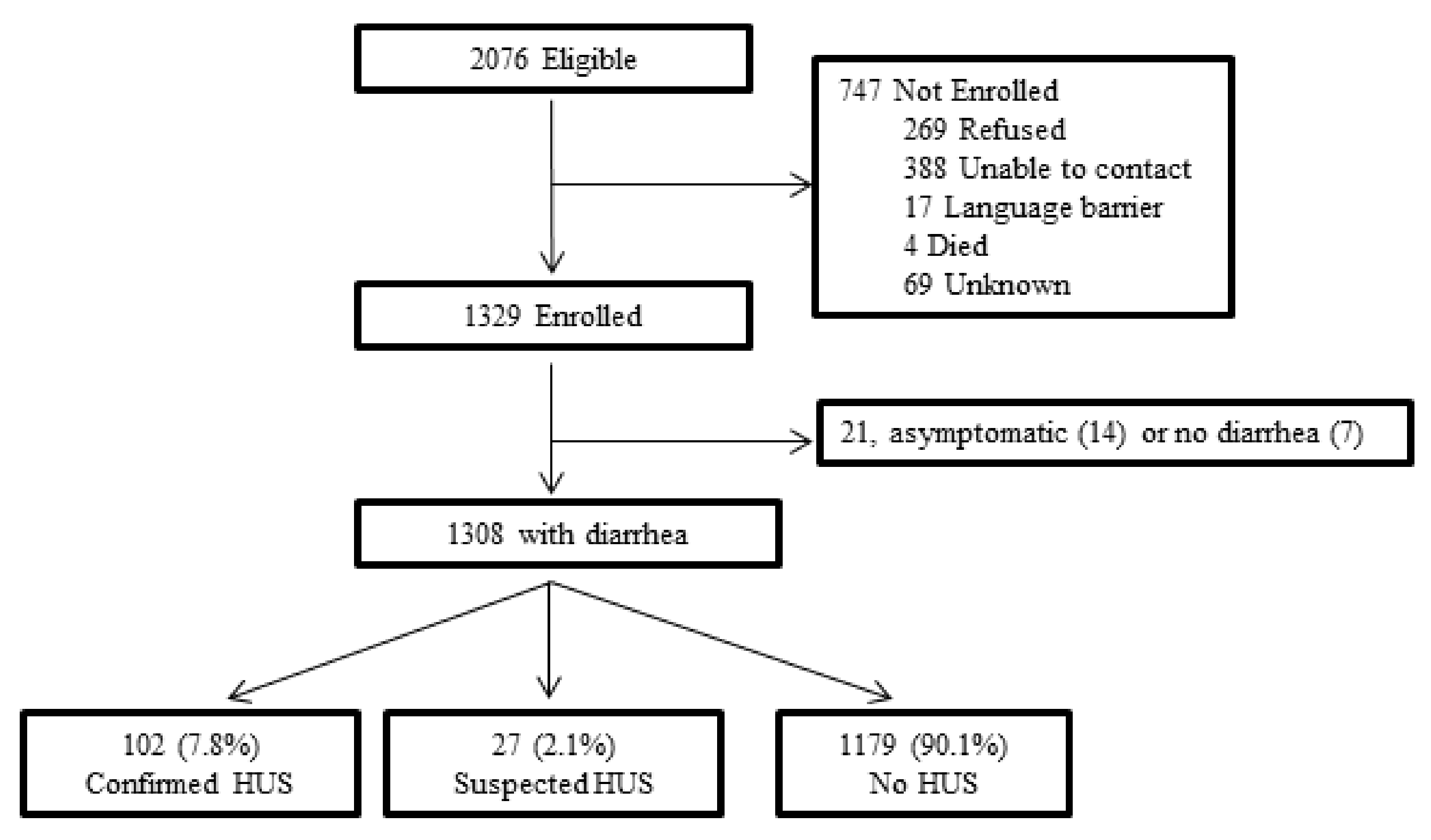
3.1. Participants and Outcomes
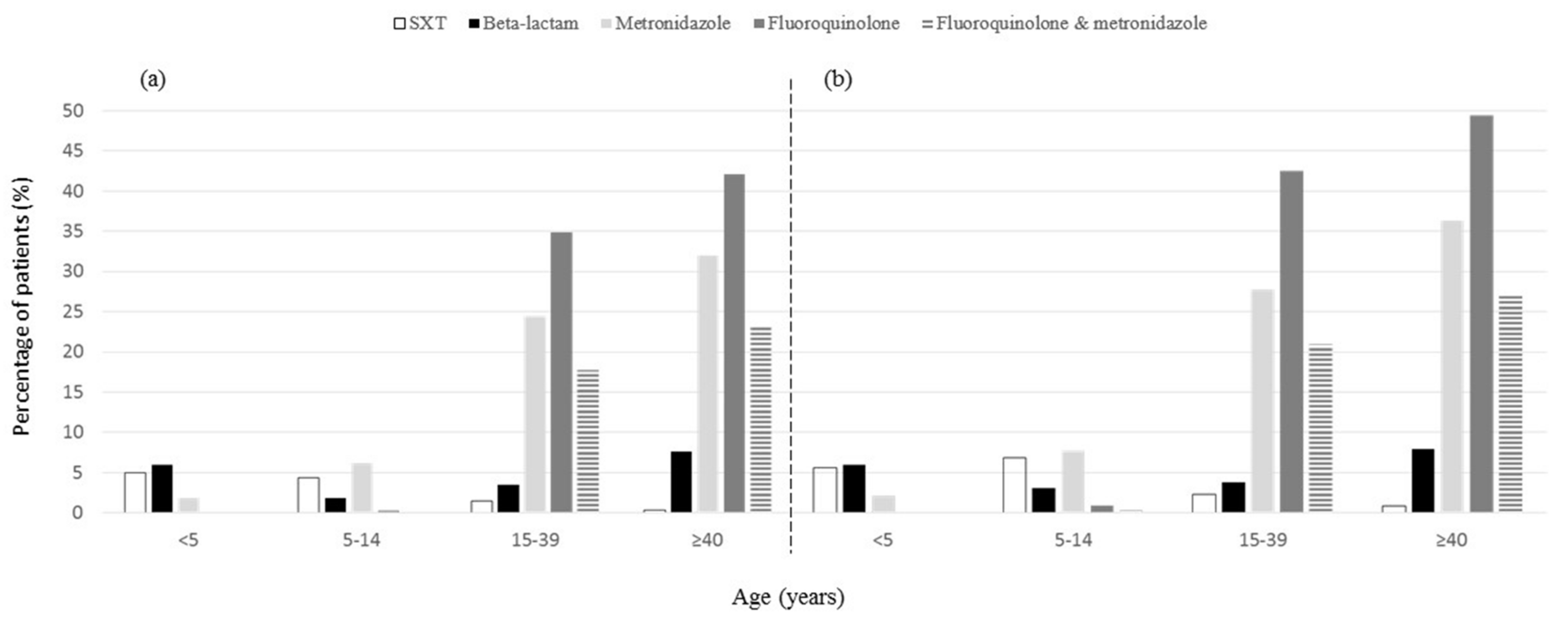
3.2. Factors Associated with Disease Severity and Antimicrobial Exposures
3.3. Antimicrobial Treatment and HUS
3.3.1. Unadjusted Analyses
3.3.2. Primary Adjusted Analyses
3.3.3. Secondary Models
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ostroff, S.M.; Kobayashi, J.M.; Lewis, J.H. Infections with Escherichia coli O157:H7 in Washington State. The first year of statewide disease surveillance. JAMA 1989, 262, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.E.; Wilker, P.R.; Reiter, P.L.; Hedican, E.B.; Bender, J.B.; Hedberg, C.W. Antibiotic treatment of Escherichia coli O157 infection and the risk of hemolytic uremic syndrome, Minnesota. Pediatr. Infect. Dis. J. 2012, 31, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.S.; Mooney, J.C.; Brandt, J.R.; Staples, A.O.; Jelacic, S.; Boster, D.R. Risk factors for the hemolytic uremic syndrome in children infected with Escherichia coli O157:H7: A multivariable analysis. Clin. Infect. Dis. 2012, 55, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shane, A.L.; Mody, R.K.; Crump, J.A.; Tarr, P.I.; Steiner, T.S.; Kotloff, K. 2017 Infectious Diseases Society of America Clinical practice guidelines for the diagnosis and management of infectious diarrhea. Clin. Infect. Dis. 2017, 65, 1963–1973. [Google Scholar] [CrossRef]
- Kakoullis, L.; Papachristodoulou, E.; Chra, P.; Panos, G. Shiga toxin-induced haemolytic uraemic syndrome and the role of antibiotics: A global overview. J. Infect. 2019, 79, 75–94. [Google Scholar] [CrossRef]
- Grif, K.; Dierich, M.P.; Karch, H.; Allerberger, F. Strain-specific differences in the amount of Shiga toxin released from enterohemorrhagic Escherichia coli O157 following exposure to subinhibitory concentrations of antimicrobial agents. Eur. J. Clin. Microbiol. Infect. Dis. 1998, 17, 761–766. [Google Scholar] [CrossRef]
- Kimmitt, P.T.; Harwood, C.R.; Barer, M.R. Toxin gene expression by Shiga toxin-producing Escherichia coli: The role of antibiotics and the bacterial SOS response. Emerg. Infect. Dis. 2000, 6, 458–465. [Google Scholar] [CrossRef] [Green Version]
- McGannon, C.M.; Fuller, C.A.; Weiss, A.A. Different classes of antibiotics differentially influence Shiga toxin production. Antimicrob. Agents Chemother. 2010, 54, 3790–3798. [Google Scholar] [CrossRef] [Green Version]
- Mohsin, M.; Haque, A.; Ali, A.; Sarwar, Y.; Bashir, S.; Tariq, A. Effects of ampicillin, gentamicin, and cefotaxime on the release of Shiga toxins from Shiga toxin-producing Escherichia coli isolated during a diarrhea episode in Faisalabad, Pakistan. Foodborne Pathog. Dis. 2010, 7, 85–90. [Google Scholar] [CrossRef]
- Ochoa, T.; Chen, J.; Walker, C.M.; Gonzales, E.; Cleary, T.G. Rifaximin does not induce toxin production or phage-mediated lysis of Shiga toxin-producing Escherichia coli. Antimicrob. Agents Chemother. 2007, 51, 2837–2841. [Google Scholar] [CrossRef] [Green Version]
- Yoh, M.; Frimpong, E.K.; Voravuthikunchai, S.P.; Honda, T. Effect of subinhibitory concentrations of antimicrobial agents (quinolones and macrolide) on the production of verotoxin by enterohemorrhagic Escherichia coli O157:H7. Can. J. Microbiol. 1999, 45, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Donohue-Rolfe, A.; Krautz-Peterson, G.; Ševo, M.; Parry, N.; Abeijon, C.; Tzipori, S. Gnotobiotic piglet infection model for evaluating the safe use of antibiotics against Escherichia coli O157:H7 Infection. J. Infect. Dis. 2009, 199, 486–493. [Google Scholar] [CrossRef] [Green Version]
- Freedman, S.B.; Xie, J.; Neufeld, M.S.; Hamilton, W.; Hartling, L.; Tarr, P.I. Shiga toxin–producing Escherichia coli infection, antibiotics, and risk of developing hemolytic uremic syndrome: A meta-analysis. Clin. Infect. Dis. 2016, 62, 1251–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mody, R.K.; Griffin, P.M. Editorial commentary: Increasing evidence that certain antibiotics should be avoided for Shiga toxin-producing Escherichia coli infections: More data needed. Clin. Infect. Dis. 2016, 62, 1259–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, L.H.; Demma, L.; Jones, T.F.; Hurd, S.; Vugia, D.J.; Smith, K.; Shiferaw, B.; Segler, S.; Palmer, A.; Zansky, S.; et al. Hemolytic uremic syndrome and death in persons with Escherichia coli O157:H7 infection, Foodborne Diseases Active Surveillance Network sites, 2000–2006. Clin. Infect. Dis. 2009, 49, 1480–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aquino, J.; Custer, J.W.; Rau, R.E. Hematology. In The Harriet Lane Handbook: A Manual for Pediatric House Officers; Elsevier Mosby: Philadelphia, PA, USA, 2009; pp. 359–386. [Google Scholar]
- Guerrant, R.L.; Van Gilder, T.; Steiner, T.; Thielman, N.M.; Slutsker, L.; Tauxe, R.V.; Hennessy, T.; Griffin, P.M.; Dupont, H.; Sack, R.B.; et al. Practice guidelines for the management of infectious diarrhea. Clin. Infect. Dis. 2001, 32, 331–351. [Google Scholar] [CrossRef]
- Wong, C.S.; Jelacic, S.; Habeeb, R.L.; Watkins, S.L.; Tarr, P.I. The risk of the hemolytic–uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N. Engl. J. Med. 2000, 342, 1930–1936. [Google Scholar] [CrossRef] [Green Version]
- Launders, N.; Byrne, L.; Jenkins, C.; Harker, K.; Charlett, A.; Adak, G.K. Disease severity of Shiga toxin-producing E. coli O157 and factors influencing the development of typical haemolytic uraemic syndrome: A retrospective cohort study, 2009–2012. BMJ Open 2016, 6, e009933. [Google Scholar] [CrossRef] [Green Version]
- Skinner, C.; Zhang, G.; Patfield, S.; He, X. An in vitro combined antibiotic-antibody treatment eliminates toxicity from Shiga toxin-producing Escherichia coli. Antimicrob. Agents Chemother. 2015, 59, 5435–5444. [Google Scholar] [CrossRef] [Green Version]
- Russo, L.M.; Melton-Celsa, A.; O’Brien, A.D. Shiga toxin (Stx) type 1a reduces the oral toxicity of Stx type 2a. J. Infect. Dis. 2016, 213, 1271–1279. [Google Scholar] [CrossRef] [Green Version]
- Pavia, A.T.; Nichols, C.R.; Green, D.P.; Tauxe, R.V.; Mottice, S.; Greene, K.D.; Wells, J.G.; Siegler, R.L.; Brewer, E.D.; Hannon, D.; et al. Hemolytic-uremic syndrome during an outbreak of Escherichia coli O157:H7 infections in institutions for mentally retarded persons: Clinical and epidemiologic observations. J. Pediatr. 1990, 116, 544–551. [Google Scholar] [CrossRef]
- Zhang, X.; McDaniel, A.D.; Wolf, L.E.; Keusch, G.T.; Waldor, M.K.; Acheson, D.W. Quinolone antibiotics induce Shiga toxin-encoding bacteriophages, toxin production, and death in mice. J. Infect. Dis. 2000, 181, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Geerdes-Fenge, H.F.; Löbermann, M.; Nürnberg, M.; Fritzsche, C.; Koball, S.; Henschel, J.; Höhn, R.; Schober, H.C.; Mitzner, S.; Podbielski, A.; et al. Ciprofloxacin reduces the risk of hemolytic uremic syndrome in patients with Escherichia coli O104:H4-associated diarrhea. Infection 2013, 41, 669–673. [Google Scholar] [CrossRef]
- Pedersen, M.G.; Hansen, C.; Riise, E.; Persson, S.; Olsen, K.E.P. Subtype-specific suppression of Shiga toxin 2 released from Escherichia coli upon exposure to protein synthesis inhibitors. J. Clin. Microbiol. 2008, 46, 2987–2991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohara, T.; Kojio, S.; Taneike, I.; Nakagawa, S.; Gondaira, F.; Tamura, Y.; Gejyo, F.; Zhang, H.-M.; Yamamoto, T. Effects of azithromycin on Shiga toxin production by Escherichia coli and subsequent host inflammatory response. Antimicrob. Agents Chemother. 2002, 46, 3478–3483. [Google Scholar] [CrossRef] [Green Version]
- Soysal, N.; Mariani-Kurkdjian, P.; Smail, Y.; Liguori, S.; Gouali, M.; Loukiadis, E.; Fach, P.; Bruyand, M.; Blanco, J.; Bidet, P.; et al. Enterohemorrhagic Escherichia coli hybrid pathotype O80:H2 as a new therapeutic challenge. Emerg. Infect. Dis. 2016, 22, 1604–1612. [Google Scholar] [CrossRef] [Green Version]
- Vonberg, R.P.; Höhle, M.; Aepfelbacher, M.; Bange, F.C.; Campos, C.B.; Claussen, K.; Christner, M.; Cramer, J.P.; Haller, H.; Hornef, M.; et al. Duration of fecal shedding of Shiga toxin–producing Escherichia coli O104:H4 in patients infected during the 2011 outbreak in Germany: A multicenter study. Clin. Infect. Dis. 2013, 56, 1132–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadwgan, A.; Laing, R.; Dargie, L.; Beadsworth, M.; MacKenzie, A.R.; Douglas, J. Three years experience of adults admitted to hospital in north-east Scotland with E. coli O157. Scott. Med. J. 2002, 47, 112–114. [Google Scholar] [CrossRef]
- Crawford, L.C.; Crawford, M.L.; Moore, S. Hemolytic-uremic syndrome in a grandmother. Emerg. Infect. Dis. 2010, 16, 1792–1795. [Google Scholar] [CrossRef]
- Griffin, P.M.; Olmstead, L.C.; Petras, R.E. Escherichia coli O157:H7-associated colitis. A clinical and histological study of 11 cases. Gastroenterology 1990, 99, 142–149. [Google Scholar] [CrossRef]
- Griffin, P.M.; Ostroff, S.M.; Tauxe, R.V.; Greene, K.D.; Wells, J.G.; Lewis, J.H.; Blake, P.A. Illnesses associated with Escherichia coli O157:H7 infections. A broad clinical spectrum. Ann. Intern. Med. 1988, 109, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Brandt, L.J.; Feuerstadt, P.; Longstreth, G.F.; Boley, S.J. ACG clinical guideline: Epidemiology, risk factors, patterns of presentation, diagnosis, and management of colon ischemia (CI). Am. J. Gastroenterol. 2015, 110, 18–44. [Google Scholar] [CrossRef] [PubMed]
- Greenbloom, S.L.; Steinhart, A.H.; Greenberg, G.R. Combination ciprofloxacin and metronidazole for active Crohn’s disease. Can. J. Gastroenterol. 1998, 12, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.O. Diverticulitis. N. Engl. J. Med. 2007, 357, 2057–2066. [Google Scholar] [CrossRef]
- Buteau, C.; Proulx, F.; Chaibou, M.; Raymond, D.; Clermont, M.-J.; Mariscalco, M.M.; Lebel, M.H.; Seidman, E. Leukocytosis in children with Escherichia coli O157:H7 enteritis developing the hemolytic-uremic syndrome. Pediatr. Infect. Dis. J. 2000, 19, 642–647. [Google Scholar] [CrossRef] [PubMed]
- National Advisory Committee on Microbiological Criteria for Foods. Response to questions posed by the Food and Drug Administration regarding virulence factors and attributes that define foodborne Shiga toxin-producing Escherichia coli (STEC) as severe human pathogens. J. Food. Prot. 2019, 82, 724–767. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Suspected HUS a (n = 27) | Confirmed HUS a (n = 102) |
|---|---|---|
| Age, median (range) in years | 4.3 (1.3–77.6) | 4.3 (1.1–73.7) |
| Female, % | 52 | 53.9 |
| Median days to first medical encounter, (IQR) | 2 (1–3) | 2 (1–2) |
| Median days to HUS diagnosis, (IQR) | 6.5 (4–9) | 6 (5–7) |
| Highest WBC, median (IQR) in cells × 109/L b | 18.3 (13.3–25.1) | 15.9 (11.8–24.2) |
| Documentation of laboratory criteria used to define confirmed HUS c: | ||
| Elevated creatinine, % | 38 | 100 |
| Low hemoglobin or hematocrit, % | 64 | 100 |
| Platelet count < 150 × 109/L, % | 65 | 100 |
| Red blood cell fragmentation, % | 100 | 100 |
| Characteristic | Frequency of Confirmed HUS, % | Confirmed HUS/Total Patients a, No./No. | p Value b |
|---|---|---|---|
| All patients | 7.8 | 102/1308 | |
| Age in years | |||
| <5 | 23.9 | 76/318 | <0.001 |
| 5 to <15 | 10.5 | 34/323 | |
| 15 to <40 | 3.5 | 12/339 | |
| ≥40 | 2.1 | 7/328 | |
| Sex | |||
| Female | 8.0 | 55/685 | 0.76 |
| Male | 7.6 | 47/622 | |
| Race | |||
| White | 7.9 | 88/1113 | 0.98 |
| Black | 9 | 4/47 | |
| Asian | 4 | 1/27 | |
| Other | 8 | 3/40 | |
| Unknown | 7 | 6/81 | |
| Feverc | |||
| No | 4.5 | 33/731 | <0.001 |
| Yes | 12.2 | 63/516 | |
| Vomiting c | |||
| No | 2.3 | 16/686 | <0.001 |
| Yes | 14.1 | 86/612 | |
| Bloody stool c | |||
| No | 6.8 | 10/148 | 0.74 |
| Yes | 7.9 | 91/1150 | |
| Day of illness at time of first medical encounter | |||
| 1–3 | 9.2 | 77/837 | 0.03 |
| 4–7 | 5.8 | 23/396 | |
| >7 | 3 | 2/75 | |
| Acetaminophen use c | |||
| No | 5.8 | 55/946 | <0.001 |
| Yes | 13.5 | 40/296 | |
| Nonsteroidal anti-inflammatory drug use c | |||
| No | 7.2 | 77/1063 | 0.22 |
| Yes | 10.1 | 18/179 | |
| Antimotility drug use c | |||
| No | 8.2 | 78/955 | 0.15 |
| Yes | 5.4 | 15/278 | |
| Initial WBC (×109/L) d | |||
| 3.9–10.3 | 4.9 | 15/304 | 0.02 |
| 10.4–13.4 | 6.1 | 14/231 | |
| 13.5–7.1 | 9.8 | 15/153 | |
| 17.2–71.0 | 12.6 | 16/127 |
| Characteristic | Frequency of Documented Antimicrobial Use, % | Used Antimicrobials/Total Patients No./No. | p Value a |
|---|---|---|---|
| All patients | 31.0 | 406/1308 | |
| Age in years | |||
| <5 | 12.6 | 40/318 | <0.001 |
| 5 to <15 | 11.5 | 37/323 | |
| 15 to <40 | 45.4 | 154/339 | |
| ≥40 | 53.4 | 175/328 | |
| Sex | |||
| Female | 32.1 | 220/685 | 0.37 |
| Male | 29.7 | 185/622 | |
| Race | |||
| White | 32.3 | 359/1113 | 0.09 |
| Black | 30 | 14/47 | |
| Asian | 30 | 8/27 | |
| Other | 15 | 6/40 | |
| Unknown | 24 | 19/81 | |
| Fever b | |||
| No | 31.6 | 231/731 | 0.49 |
| Yes | 29.7 | 153/516 | |
| Vomiting b | |||
| No | 30.9 | 212/686 | 0.86 |
| Yes | 31.4 | 192/612 | |
| Bloody stool b | |||
| No | 15.5 | 23/148 | <0.001 |
| Yes | 32.7 | 376/1150 | |
| Day of illness at time of first medical encounter | |||
| 1–3 | 34.8 | 291/837 | <0.001 |
| 4–7 | 28.5 | 113/396 | |
| >7 | 3 | 2/75 | |
| Acetaminophen b | <0.001 | ||
| No | 34.0 | 323/946 | |
| Yes | 20.8 | 62/296 | |
| Nonsteroidal anti-inflammatory drugs b | |||
| No | 32.1 | 341/1063 | 0.04 |
| Yes | 24.6 | 44/179 | |
| Antimotility drugs b | |||
| No | 28.3 | 270/955 | 0.001 |
| Yes | 40.3 | 112/278 | |
| Highest WBC (×109/L) c | |||
| 3.9–10.3 | 34.2 | 104/304 | 0.04 |
| 10.4–13.4 | 42.0 | 97/231 | |
| 13.5–17.1 | 47.7 | 73/153 | |
| 17.2–71.0 | 40.9 | 52/127 |
| Antimicrobial Exposure | HUS b | Crude Odds Ratio for HUS | 95% CI | Adjusted Odds Ratio for HUS c | 95% CI | |||
|---|---|---|---|---|---|---|---|---|
| Confirmed (n = 102) No. (%) | Suspected (n = 27) No. (%) | None (n = 1179) No. (%) | Patients in Adjusted Model d No. | |||||
| Any antimicrobial | 23 (22.5) | 9 (33) | 374 (31.7) | 0.63 | 0.39–1.01 | 1.37 | 0.73–2.57 | 1155 |
| Fluoroquinolone | 5 (4.9) | 2 (7) | 250 (21.2) | 0.20 | 0.08–0.51 | 0.30 | 0.04–2.53 | 1024 |
| Metronidazole | 12 (11.8) | 4 (15) | 198 (16.8) | 0.62 | 0.33–1.16 | 1.72 | 0.65–4.59 | 990 |
| Macrolide | 0 (0) | 0 (0) | 12 (1.0) | 0.61 e | 0.00–2.94 | f | 827 | |
| β-lactam | 10 (9.8) | 4 (15) | 48 (4.1) | 2.12 | 1.03–4.36 | 2.80 | 1.14–6.89 | 854 |
| SXT | 8 (7.8) | 2 (7) | 26 (2.2) | 3.13 | 1.18–7.42 | 2.37 | 0.85–6.60 | 811 |
| Antimicrobial Exposure | HUS b | Crude Odds Ratio for HUS | 95% CI | Adjusted Odds Ratio for HUS c | 95% CI | |||
|---|---|---|---|---|---|---|---|---|
| Confirmed (n = 102) No. (%) | Suspected (n = 27) No. (%) | None (n = 1179) No. (%) | No. Patients in Adjusted Model d | |||||
| Any antimicrobial | 10 (9.8) | 4 (14.8) | 211 (17.9) | 0.50 | 0.26–0.97 | 0.83 | 0.35–1.96 | 1155 |
| Fluoroquinolone | 2 (2.0) | 1 (3.7) | 137 (11.6) | 0.15 | 0.04–0.63 | f | 1081 | |
| Metronidazole | 5 (4.9) | 3 (11.1) | 112 (9.5) | 0.47 | 0.19–1.18 | 0.78 | 0.17–3.52 | 1062 |
| Macrolide | 0 (0) | 0 (0) | 8 (0.7) | 0.96 e | 0.00–4.85 | f | 985 | |
| β-lactam | 4 (3.9) | 1 (3.7) | 23 (2.0) | 1.83 | 0.62–5.41 | 1.86 | 0.44–7.84 | 982 |
| TMP/SMX | 5 (4.9) | 1 (3.7) | 11 (0.9) | 4.78 | 1.63–14.06 | 2.64 | 0.59–11.96 | 968 |
| Category a | HUS Definition b | Source of Antibiotic Exposure Data c | No. Patients Included | WBC Included as Model Covariate d | Adjusted OR e | 95% CI |
|---|---|---|---|---|---|---|
| A | Confirmed or suspected | Documented or reported | 812 | No | 3.90 | 1.80–8.43 |
| Yes | 3.71 | 1.71–8.07 | ||||
| Documented | 874 | No | 3.45 | 1.54–7.74 | ||
| Yes | 3.22 | 1.43–7.25 | ||||
| Confirmed (suspected excluded) | Documented or reported | 792 | No | 3.41 | 1.47–7.94 | |
| Yes | 3.48 | 1.49–8.14 | ||||
| Documented | 854 | No f | 2.80 | 1.14–6.89 | ||
| Yes | 2.83 | 1.15–7.01 | ||||
| Confirmed (suspected considered no HUS) | Documented or reported | 812 | No | 2.67 | 1.18–6.03 | |
| Yes | 2.74 | 1.21–6.23 | ||||
| Documented | 874 | No | 2.18 | 0.91–5.20 | ||
| Yes | 2.23 | 0.93–5.34 | ||||
| B | Confirmed (suspected excluded) | Documented or reported | 490 | No | 2.75 | 1.12–6.73 |
| Yes | 2.94 | 1.18–7.28 | ||||
| Documented | 511 | No | 1.95 | 0.77–4.94 | ||
| Yes | 2.06 | 0.80–5.29 | ||||
| Confirmed (suspected considered no HUS) | Documented or reported | 508 | No | 2.26 | 0.96–5.32 | |
| Yes | 2.41 | 1.01–5.77 | ||||
| Documented | 529 | No | 1.63 | 0.69–4.00 | ||
| Yes | 1.73 | 0.70–4.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mody, R.K.; Hoekstra, R.M.; Scott, M.K.; Dunn, J.; Smith, K.; Tobin-D’Angelo, M.; Shiferaw, B.; Wymore, K.; Clogher, P.; Palmer, A.; et al. Risk of Hemolytic Uremic Syndrome Related to Treatment of Escherichia coli O157 Infection with Different Antimicrobial Classes. Microorganisms 2021, 9, 1997. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091997
Mody RK, Hoekstra RM, Scott MK, Dunn J, Smith K, Tobin-D’Angelo M, Shiferaw B, Wymore K, Clogher P, Palmer A, et al. Risk of Hemolytic Uremic Syndrome Related to Treatment of Escherichia coli O157 Infection with Different Antimicrobial Classes. Microorganisms. 2021; 9(9):1997. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091997
Chicago/Turabian StyleMody, Rajal K., Robert M. Hoekstra, Magdalena Kendall Scott, John Dunn, Kirk Smith, Melissa Tobin-D’Angelo, Beletshachew Shiferaw, Katie Wymore, Paula Clogher, Amanda Palmer, and et al. 2021. "Risk of Hemolytic Uremic Syndrome Related to Treatment of Escherichia coli O157 Infection with Different Antimicrobial Classes" Microorganisms 9, no. 9: 1997. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091997