
Chronic Enteropathy in Dogs—Epidemiologic Aspects and Clinical Characteristics of Dogs Presenting at Two Swedish Animal Hospitals

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
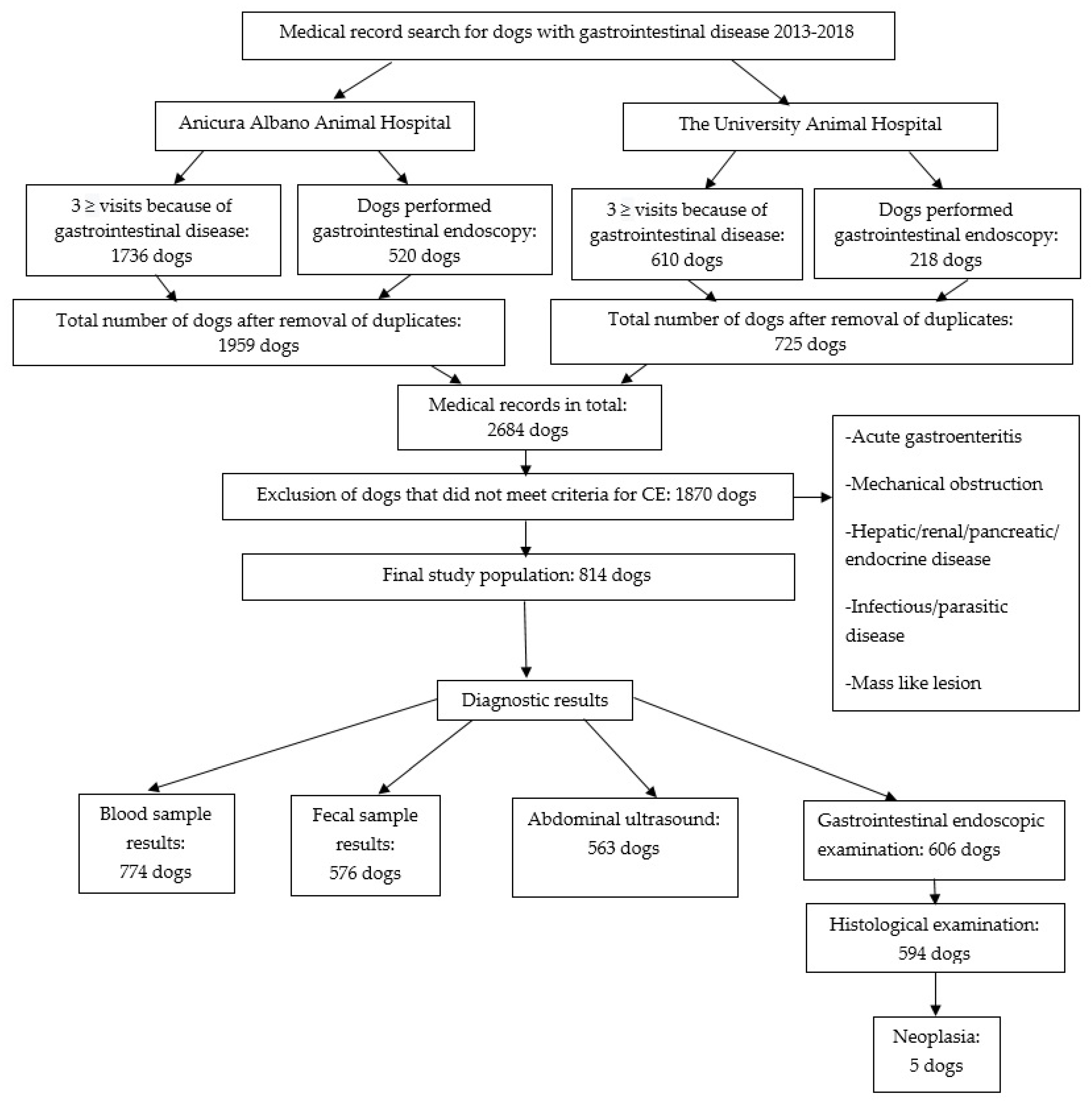
2.1. Study Population
2.2. Database
2.3. Classification of Dogs
2.4. Statistical Methods
3. Results
3.1. Study Population
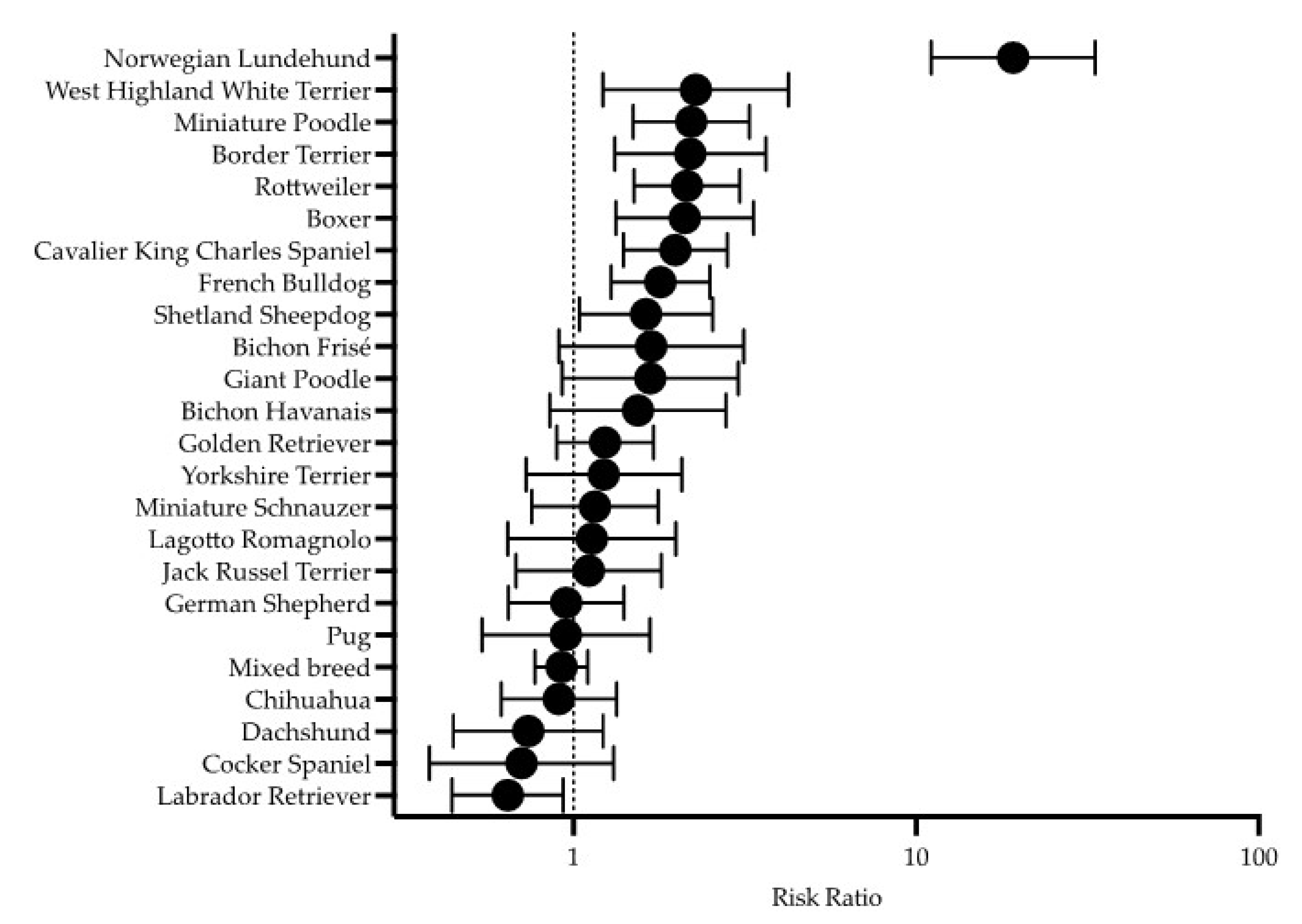
3.2. Period Prevalence and Relative Risk
3.3. Classification of Dogs
3.4. Diagnostic Results
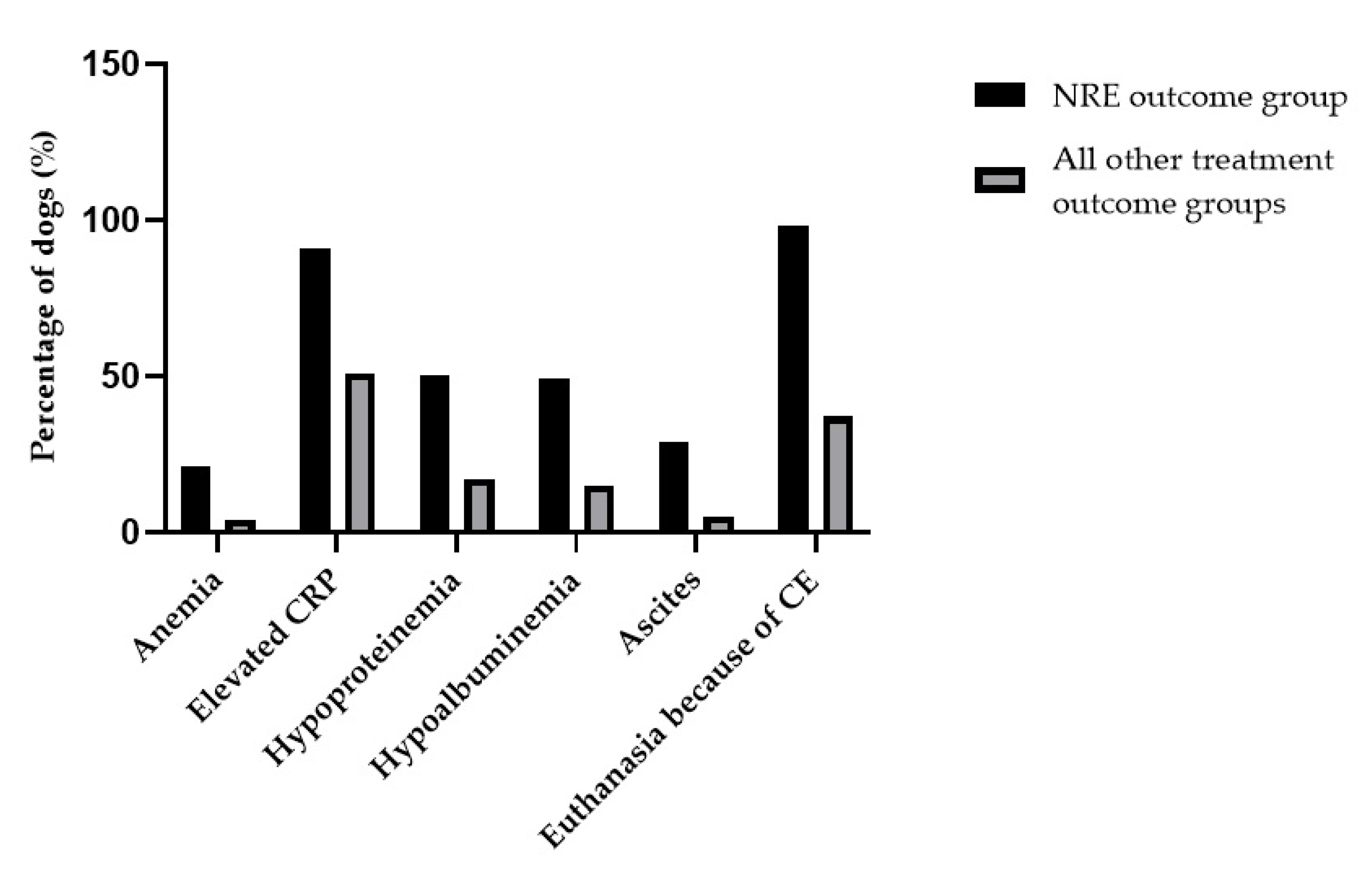
3.5. Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dandrieux, J.R.S.; Mansfield, C.S. Chronic Enteropathy in Canines: Prevalence, Impact And Management Strategies. Vet. Med. 2019, 10, 203–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dandrieux, J.R.S. Inflammatory bowel disease versus chronic enteropathy in dogs: Are they one and the same? J. Small Anim. Pract. 2016, 57, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Dandrieux, J.R.S.; Martinez Lopez, L.M.; Prakash, N.; Mansfield, C.S. Treatment response and long term follow up in nineteen dogs diagnosed with chronic enteropathy in Australia. Aust. Vet. J. 2019, 97, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Jergens, A.E.; Simpson, K.W. Inflammatory bowel disease in veterinary medicine. Front. Biosci. 2012, 4, 1404–1419. [Google Scholar] [CrossRef]
- Allenspach, K. Clinical Immunology and Immunopathology of the Canine and Feline Intestine. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 345–360. [Google Scholar] [CrossRef]
- Kathrani, A.; Werling, D.; Allenspach, K. Canine breeds at high risk of developing inflammatory bowel disease in the south-eastern UK. Vet. Rec. 2011, 169, 635. [Google Scholar] [CrossRef] [Green Version]
- Allenspach, K.; House, A.; Smith, K.; McNeill, F.M.; Hendricks, A.; Elson-Riggins, J.; Riddle, A.; Steiner, J.M.; Werling, D.; Garden, O.A.; et al. Evaluation of mucosal bacteria and histopathology, clinical disease activity and expression of Toll-like receptors in German shepherd dogs with chronic enteropathies. Vet. Microbiol. 2010, 146, 326–335. [Google Scholar] [CrossRef]
- Craven, M.; Mansfield, C.S.; Simpson, K.W. Granulomatous colitis of boxer dogs. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 433–445. [Google Scholar] [CrossRef]
- Berghoff, N.; Ruaux, C.G.; Steiner, J.M.; Williams, D.A. Gastroenteropathy in Norwegian Lundehund. Compendium 2007, 29, 456. [Google Scholar]
- Kathrani, A.; House, A.; Catchpole, B.; Murphy, A.; German, A.; Werling, D.; Allenspach, K. Polymorphisms in the Tlr4 and Tlr5 Gene Are Significantly Associated with Inflammatory Bowel Disease in German Shepherd Dogs. PLoS ONE 2010, 5, e15740. [Google Scholar]
- German, A.; Hall, E.; Day, M. Relative deficiency in IgA production by duodenal explants from German shepherd dogs with small intestinal disease. Vet. Immunol. Immunopathol. 2000, 76, 25–43. [Google Scholar] [CrossRef]
- Berghoff, N.; Steiner, J.M. Laboratory tests for the diagnosis and management of chronic canine and feline enteropathies. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 311–328. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.W.; Jergens, A.E. Pitfalls and Progress in the Diagnosis and Management of Canine Inflammatory Bowel Disease. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 381–398. [Google Scholar] [CrossRef]
- Allenspach, K.; Wieland, B.; Grone, A.; Gaschen, F. Chronic enteropathies in dogs: Evaluation of risk factors for negative outcome. J. Vet. Intern. Med. 2007, 21, 700–708. [Google Scholar] [CrossRef]
- Makielski, K.; Cullen, J.; O’Connor, A.; Jergens, A.E. Narrative review of therapies for chronic enteropathies in dogs and cats. J. Vet. Intern. Med. 2019, 33, 11–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craven, M.D.; Washabau, R.J. Comparative pathophysiology and management of protein-losing enteropathy. J. Vet. Intern. Med. 2019, 33, 383–402. [Google Scholar] [CrossRef]
- Dossin, O.; Lavoue, R. Protein-losing enteropathies in dogs. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 399–418. [Google Scholar] [CrossRef] [PubMed]
- Jergens, A.E.; Schreiner, C.A.; Frank, D.E.; Niyo, Y.; Ahrens, F.E.; Eckersall, P.D.; Benson, T.J.; Evans, R. A scoring index for disease activity in canine inflammatory bowel disease. J. Vet. Intern. Med. 2003, 17, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Allenspach, K.; Rizzo, J.; Jergens, A.E.; Chang, Y.M. Hypovitaminosis D is associated with negative outcome in dogs with protein losing enteropathy: A retrospective study of 43 cases. BMC Vet. Res. 2017, 13, 96. [Google Scholar] [CrossRef] [Green Version]
- Craven, M.; Simpson, J.W.; Ridyard, A.E.; Chandler, M.L. Canine inflammatory bowel disease: Retrospective analysis of diagnosis and outcome in 80 cases (1995–2002). J. Small Anim. Pract. 2004, 45, 336–342. [Google Scholar] [CrossRef]
- Jergens, A.E. Inflammatory bowel disease. Current perspectives. Vet. Clin. North Am. Small Anim. Pract. 1999, 29, 501–521. [Google Scholar] [PubMed]
- Mandigers, P.J.J.; Biourge, V.; Van Den Ingh, T.S.G.A.M.; Ankringa, N.; German, A.J.A. A Randomized, Open-Label, Positively-Controlled Field Trial of a Hydrolyzed Protein Diet in Dogs with Chronic Small Bowel Enteropathy. J. Vet. Intern. Med. 2010, 24, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.; Pengo, G.; Caldin, M.; Palumbo Piccionello, A.; Steiner, J.M.; Cohen, N.D.; Jergens, A.E.; Suchodolski, J.S. Comparison of microbiological, histological, and immunomodulatory parameters in response to treatment with either combination therapy with prednisone and metronidazole or probiotic VSL#3 strains in dogs with idiopathic inflammatory bowel disease. PLoS ONE. 2014, 9, e94699. [Google Scholar]
- Dye, T.; Diehl, K.; Wheeler, S.; Westfall, D. Randomized, Controlled Trial of Budesonide and Prednisone for the Treatment of Idiopathic Inflammatory Bowel Disease in Dogs. J. Vet. Intern. Med. 2013, 27, 1385–1391. [Google Scholar] [CrossRef] [Green Version]
- Allenspach, K.; Culverwell, C.; Chan, D. Long-term outcome in dogs with chronic enteropathies: 203 cases. Vet. Rec. 2016, 178, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benvenuti, E.; Pierini, A.; Bottero, E.; Pietra, M.; Gori, E.; Salvadori, S.; Marchetti, V. Immunosuppressant-Responsive Enteropathy and Non-Responsive Enteropathy in Dogs: Prognostic Factors, Short- and Long-Term Follow Up. Animals 2021, 11, 2637. [Google Scholar] [CrossRef]
- Pietra, M.; Galiazzo, G.; Bresciani, F.; Morini, M.; Licarini, S.; Turba, M.E.; Amaducci, G.; Bettini, G.; Fracassi, F.; Ostanello, F. Evaluation of Prognostic Factors, including Duodenal P-Glycoprotein Expression, in Canine Chronic Enteropathy. Animals 2021, 11, 2315. [Google Scholar] [CrossRef]
- Marchesi, M.C.; Timpano, C.C.; Busechian, S.; Pieramati, C.; Rueca, F. The role of diet in managing inflamatory bowel disease affected dogs: A retrospective cohort study on 76 cases. Vet. Ital. 2017, 53, 297–302. [Google Scholar]
- Flesjå, K.; Yri, T. Protein-losing enteropathy in the Lundehund. J. Small Anim. Pract. 1977, 18, 11–23. [Google Scholar] [CrossRef]
- Lilliehöök, I.; Gunnarsson, L.; Zakrisson, G.; Tvedten, H. Diseases associated with pronounced eosinophilia: A study of 105 dogs in Sweden. J. Small Anim. Pract. 2000, 41, 248–253. [Google Scholar] [CrossRef]
- Sykes, J.E.; Weiss, D.J.; Buoen, L.C.; Blauvelt, M.M.; Hayden, D.W. Idiopathic hypereosinophilic syndrome in 3 Rottweilers. J. Vet. Intern. Med. 2001, 15, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.W.; Dogan, B.; Rishniw, M.; Goldstein, R.E.; Klaessig, S.; McDonough, P.L.; German, A.J.; Yates, R.M.; Russell, D.G.; Johnson, S.E.; et al. Adherent and Invasive Escherichia coli Is Associated with Granulomatous Colitis in Boxer Dogs. Infect. Immun. 2006, 74, 4778–4792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, E.J.; Rutgers, H.C.; Scholes, S.F.E.; Middleton, D.J.; Tennant, B.J.; King, N.M.; Kelly, D.F. Histiocytic ulcerative colitis in boxer dogs in the UK. J. Small Anim. Pract. 1994, 35, 509–515. [Google Scholar] [CrossRef]
- Kawano, K.; Shimakura, H.; Nagata, N.; Masashi, Y.; Suto, A.; Suto, Y.; Uto, S.; Ueno, H.; Hasegawa, T.; Ushigusa, T.; et al. Prevalence of food-responsive enteropathy among dogs with chronic enteropathy in Japan. J. Vet. Med. Sci. 2016, 78, 1377–1380. [Google Scholar] [CrossRef] [Green Version]
- Läkemedelsverket, Dosering av antibiotika till hund—Ny rekommendation. Inf. Läkemedelsverket 2016, 27, 4–17.
- Hostutler, R.A.; Luria, B.J.; Johnson, S.E.; Weisbrode, S.E.; Sherding, R.G.; Jaeger, J.Q.; Guilford, W.G. Antibiotic-responsive histiocytic ulcerative colitis in 9 dogs. J. Vet. Intern. Med. 2004, 18, 499–504. [Google Scholar] [CrossRef]
- Mansfield, C.; James, F.; Craven, M.; Davies, D.; O’Hara, A.; Nicholls, P.; Dogan, B.; MacDonough, S.; Simpson, K. Remission of Histiocytic Ulcerative Colitis in Boxer Dogs Correlates with Eradication of Invasive Intramucosal Escherichia coli. J. Vet. Intern. Med. 2009, 23, 964–969. [Google Scholar] [CrossRef] [Green Version]
- Westermarck, E.; Skrzypczak, T.; Harmoinen, J.; Steiner, J.M.; Ruaux, C.G.; Williams, D.A.; Eerola, E.; Sundbäck, P.; Rinkinen, M. Tylosin-responsive chronic diarrhea in dogs. J. Vet. Intern. Med. 2005, 19, 177–186. [Google Scholar] [CrossRef]
- Kilpinen, S.; Spillmann, T.; Syrjä, P.; Skrzypczak, T.; Louhelainen, M.; Westermarck, E. Effect of tylosin on dogs with suspected tylosin-responsive diarrhea: A placebo-controlled, randomized, double-blinded, prospective clinical trial. Acta Vet. Scand. 2011, 53, 26. [Google Scholar] [CrossRef] [Green Version]
- Jergens, A.E.; Crandell, J.; Morrison, J.A.; Deitz, K.; Pressel, M.; Ackermann, M.; Suchodolski, J.; Steiner, J.M.; Evans, R. Comparison of Oral Prednisone and Prednisone Combined with Metronidazole for Induction Therapy of Canine Inflammatory Bowel Disease: A Randomized-Controlled Trial. J. Vet. Intern. Med. 2010, 24, 269–277. [Google Scholar] [CrossRef]
- Kilpinen, S.; Spillmann, T.; Westermarck, E. Efficacy of two low-dose oral tylosin regimens in controlling the relapse of diarrhea in dogs with tylosin-responsive diarrhea: A prospective, single-blinded, two-arm parallel, clinical field trial. Acta Vet. Scand. 2014, 56, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaitman, J.; Ziese, A.-L.; Pilla, R.; Minamoto, Y.; Blake, A.B.; Guard, B.C.; Isaiah, A.; Lidbury, J.A.; Steiner, J.M.; Unterer, S.; et al. Fecal Microbial and Metabolic Profiles in Dogs with Acute Diarrhea Receiving Either Fecal Microbiota Transplantation or Oral Metronidazole. Front. Vet. Sci. 2020, 7, 192. [Google Scholar] [CrossRef] [PubMed]
- Pilla, R.; Gaschen, F.; Barr, J.W.; Olson, E.; Honneffer, J.; Guard, B.C.; Blake, A.B.; Villanueva, D.; Khattab, M.R.; Alshawaqfeh, M.K.; et al. Effects of metronidazole on the fecal microbiome and metabolome in healthy dogs. J. Vet. Intern. Med. 2020, 34, 1853–1866. [Google Scholar] [CrossRef] [PubMed]
- Pinna, C.; Vecchiato, C.G.; Grandi, M.; Mammi, L.M.E.; Stefanelli, C.; Biagi, G. In Vitro Evaluation of the Effects of Tylosin on the Composition and Metabolism of Canine Fecal Microbiota. Animals 2020, 10, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manchester, A.C.; Webb, C.B.; Blake, A.B.; Sarwar, F.; Lidbury, J.A.; Steiner, J.M.; Suchodolski, J.S. Long-term impact of tylosin on fecal microbiota and fecal bile acids of healthy dogs. J. Vet. Intern. Med. 2019, 33, 2605–2617. [Google Scholar] [CrossRef] [PubMed]
- Otoni, C.C.; Heilmann, R.M.; García-Sancho, M.; Sainz, A.; Ackermann, M.R.; Suchodolski, J.S.; Steiner, J.M.; Jergens, A.E. Serologic and fecal markers to predict response to induction therapy in dogs with idiopathic inflammatory bowel disease. J. Vet. Intern. Med. 2018, 32, 999–1008. [Google Scholar] [CrossRef]
- Garcia-Sancho, M.; Rodriguez-Franco, F.; Sainz, A.; Mancho, C.; Rodríguez, A. Evaluation of clinical, macroscopic, and histopathologic response to treatment in nonhypoproteinemic dogs with lymphocytic-plasmacytic enteritis. J. Vet. Intern. Med. 2007, 21, 11–17. [Google Scholar] [CrossRef]
- Heilmann, R.M.; Berghoff, N.; Mansell, J.; Grützner, N.; Parnell, N.K.; Gurtner, C.; Suchodolski, J.S.; Steiner, J.M. Association of fecal calprotectin concentrations with disease severity, response to treatment, and other biomarkers in dogs with chronic inflammatory enteropathies. J. Vet. Intern. Med. 2018, 32, 679–692. [Google Scholar] [CrossRef]
- Heilmann, R.M.; Volkmann, M.; Otoni, C.C.; Grützner, N.; Kohn, B.; Jergens, A.E.; Steiner, J.M. Fecal S100A12 concentration predicts a lack of response to treatment in dogs affected with chronic enteropathy. Vet. J. 2016, 215, 96–100. [Google Scholar] [CrossRef]
- White, R.; Atherly, T.; Guard, B.; Rossi, G.; Wang, C.; Mosher, C.; Webb, C.; Hill, S.; Ackermann, M.; Sciabarra, P.; et al. Randomized, controlled trial evaluating the effect of multi-strain probiotic on the mucosal microbiota in canine idiopathic inflammatory bowel disease. Gut Microbes 2017, 8, 451–466. [Google Scholar] [CrossRef] [Green Version]
- Pietra, M.; Fracassi, F.; Diana, A.; Gazzotti, T.; Bettini, G.; Peli, A.; Morini, M.; Pagliuca, G.; Roncada, P. Plasma concentrations and therapeutic effects of budesonide in dogs with inflammatory bowel disease. Am. J. Vet. Res. 2013, 74, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, V.; Lubas, G.; Lombardo, A.; Corazza, M.; Guidi, G.; Cardini, G. Evaluation of Erythrocytes, Platelets, and Serum Iron Profile in Dogs with Chronic Enteropathy. Vet. Med. Int. 2010, 2010, 716040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkmann, M.; Steiner, J.M.; Fosgate, G.T.; Zentek, J.; Hartmann, S.; Kohn, B. Chronic Diarrhea in Dogs—Retrospective Study in 136 Cases. J. Vet. Intern. Med. 2017, 31, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Toresson, L.; Steiner, J.M.; Suchodolski, J.S.; Spillmann, T. Oral Cobalamin Supplementation in Dogs with Chronic Enteropathies and Hypocobalaminemia. J. Vet. Intern. Med. 2016, 30, 101–107. [Google Scholar] [CrossRef]
- Berghoff, N.; Suchodolski, J.S.; Steiner, J.M. Association between serum cobalamin and methylmalonic acid concentrations in dogs. Vet. J. 2012, 191, 306–311. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Information Rate (n = 814) | Variable | Overall (n = 814) | Food Responsive (n = 93) | Immunosuppressant Responsive (n = 449) | Antibiotic Responsive (n = 9) | Non Responsive (n = 42) | Non Classified (n = 221) | |
|---|---|---|---|---|---|---|---|---|
| Study population | 814/814 | Sex (male/female) | 463/351 | 52/41 | 246/203 | 6/3 | 23/19 | 136/85 |
| 113/814 | Median BCS (1- 9/9) | 4 (3–5) | 4 (4–5) | 4 (4–5) | 4(4) | 3 (3–4) | 4 (3–4) | |
| 702//814 | Median body weight (kg) | 11.1 (6.5–25.9) | 12.3 (6.4–27.6) | 10.0 (6.3–23.7) | 9.0 (6.2–14.1) | 12.2 (7.6–30.2) | 15.3 (7.5–28.9) | |
| 814/814 | Median age at first visit (years) | 3.8 (1.8–6.7) | 3.8 (1.5–6.0) | 3.7 (1.8–6.6) | 4.1 (0.8–8.1) | 5.0 (3.5–9.1) | 3.9 (1.9–6.8) | |
| 814/814 | Median age at last visit (years) | 7.6 (4.8–10) | 7.5 (4.8–9.3) | 7.9 (5.5–10.6) | 8.0 (2.5–12.8) | 6.4 (3.7–9.1) | 7.0 (4.2–9.5) | |
| 251/814 | Median age at death (years) | 9.2 (6.5–11.5) | 8.9 (6.9–10.8) | 10.3 (7.5–12.4) | 11.3 (7.9–14.8) | 6.6 (3.8–9.2) | 8.8 (6.6–11.2) | |
| 814/814 | Median time of follow up (years) | 2.8 (0.9–4.6) | 3.1 (1.1–4.5) | 3.3 (1.5–5.2) | 3.3 (1.7–4.3) | 0.3 (0.1–0.7) | 2.1 (0.4–3.6) | |
| 244/814 | Euthanasia because of CE (yes/no) | 116/128 | 3/9 | 42/82 | 1/1 | 41/1 | 29/35 | |
| Presenting signs | 759/814 | Vomiting (yes/no) | 598/161 | 64/25 | 350/71 | 5/4 | 29/8 | 150/53 |
| 764/814 | Diarrhea (yes/no) | 574/190 | 67/25 | 298/115 | 8/1 | 35/5 | 166/44 | |
| 503/814 | Anorexia (yes/no) | 282/221 | 33/32 | 157/108 | 2/6 | 21/10 | 69/65 | |
| 269/814 | Weight loss (yes/no) | 184/85 | 14/14 | 93/47 | 1/1 | 22/2 | 54/21 | |
| 469/814 | Activity (decreased/normal) | 247/222 | 29/29 | 124/114 | 1/5 | 21/13 | 72/61 | |
| 764/814 | Hematochezia (yes/no) | 31/733 | 5/87 | 16/398 | 0/9 | 2/38 | 8/201 | |
| 67/814 | Stool frequency (increased/normal) | 41/26 | 8/6 | 17/10 | 2/0 | 3/1 | 11/9 | |
| 250/814 | Pruritus (yes/no) | 205/45 | 17/12 | 122/17 | 2/0 | 6/3 | 58/13 |
| Information Rate (n = 814) | Variable | Overall (n = 814) | Food Responsive (n = 93) | Immunosuppressant Responsive (n = 449) | Antibiotic Responsive (n = 9) | Non Responsive (n = 42) | Non Classified (n = 221) | |
|---|---|---|---|---|---|---|---|---|
| Blood samples | 814/814 | Blood samples taken (yes/no) | 792/22 | 91/2 | 438/11 | 9/0 | 42/0 | 212/9 |
| Blood sample results | 814/814 | Blood sample results available (yes/no) | 774/40 | 90/3 | 428/21 | 8/1 | 42/0 | 206/15 |
| 632/814 | Anemia (yes/no) | 32/600 | 2/70 | 14/333 | 1/6 | 8/31 | 7/160 | |
| 637/814 | Leukocytosis (yes/no) | 65/572 | 5/66 | 31/320 | 1/6 | 11/28 | 17/152 | |
| 637/814 | Leukopenia (yes/no) | 18/619 | 0/71 | 11/340 | 0/7 | 0/39 | 7/162 | |
| 218/814 | Eosinophilia (yes/no) | 32/186 | 6/23 | 14/85 | 0/3 | 2/20 | 10/55 | |
| 267/814 | Elevated CRP (yes/no) | 145/122 | 26/19 | 52/72 | 1/0 | 20/2 | 46/29 | |
| 608/814 | Elevated creatinine (yes/no) | 13/595 | 1/70 | 5/331 | 0/7 | 3/31 | 4/156 | |
| 486/814 | Elevated urea (yes/no) | 28/458 | 3/44 | 15/276 | 0/4 | 0/19 | 10/115 | |
| 621/814 | Elevated ALT (yes/no) | 105/516 | 10/64 | 67/277 | 0/7 | 6/29 | 22/139 | |
| 126/814 | Hypocalcemia (total) (yes/no) | 15/111 | 1/19 | 10/53 | 0/1 | 2/3 | 2/35 | |
| 647/814 | Hypocobalaminemia (yes/no) | 98/549 | 6/75 | 53/294 | 0/4 | 7/29 | 32/147 | |
| 638/814 | Low folate (yes/no) | 194/444 | 18/62 | 122/221 | 0/4 | 6/29 | 48/128 | |
| 655/814 | Hypoproteinemia (yes/no) | 125/530 | 13/66 | 61/292 | 2/5 | 19/19 | 30/148 | |
| 662/814 | Hypoalbuminemia (yes/no) | 116/546 | 7/73 | 59/294 | 0/7 | 20/21 | 30/151 | |
| Other clinical signs | 550/814 | Ascites (yes/no) | 37/513 | 1/67 | 20/279 | 0/5 | 10/24 | 6/138 |
| Diagnostic imaging | 814/814 | Abdominal ultrasound (yes/no) | 563/251 | 69/24 | 305/144 | 5/4 | 36/6 | 148/73 |
| 563/814 | Ultrasonographic abnormalities GI tract (yes/no) | 335/228 | 38/31 | 199/106 | 3/2 | 23/12 | 72/77 |
| Information Rate (n = 814) | Variable | Overall (n = 814) | Food Responsive (n = 93) | Immunosuppressant Responsive (n = 449) | Antibiotic Responsive (n = 9) | Non Responsive (n = 42) | Non Classified (n = 221) | |
|---|---|---|---|---|---|---|---|---|
| GI endoscopy | 814/814 | GI endoscopy (yes/no) | 606/208 | 34/59 | 379/70 | 8/1 | 24/18 | 161/60 |
| 594/814 | Macroscopic abnormalities (yes/no) | 593/1 | 30/1 | 371/0 | 8/0 | 24/0 | 160/0 | |
| 594/814 | Histological abnormalities (yes/no) | 576/18 | 28/3 | 362/9 | 8/0 | 23/1 | 155/5 | |
| Histological results stomach | 566/814 | Normal stomach (yes/no) | 82/484 | 8/22 | 36/318 | 0/7 | 4/17 | 34/120 |
| 566/814 | Chronic gastritis (yes/no) | 337/229 | 15/15 | 224/130 | 4/3 | 10/11 | 84/70 | |
| 566/814 | Lymphoplasmacytic gastritis (yes/no) | 48/518 | 1/29 | 34/320 | 2/5 | 3/18 | 8/146 | |
| 566/814 | Eosinophilic gastritis (yes/no) | 95/471 | 6/24 | 59/295 | 1/6 | 2/19 | 27/127 | |
| 566/814 | Neoplasia (yes/no) | 4/562 | 0/30 | 1/353 | 0/7 | 2/19 | 1/153 | |
| Histological results duodenum | 493/814 | Normal duodenum (yes/no) | 106/387 | 6/17 | 63/253 | 4/2 | 1/17 | 32/98 |
| 493/814 | Chronic enteritis (yes/no) | 168/325 | 9/14 | 108/208 | 2/4 | 5/13 | 44/86 | |
| 493/814 | Lymphoplasmacytic enteritis (yes/no) | 95/398 | 3/20 | 58/258 | 0/6 | 7/11 | 27/103 | |
| 493/814 | Eosinophilic enteritis (yes/no) | 123/370 | 5/18 | 86/230 | 0/6 | 5/13 | 27/103 | |
| 493/814 | Neoplasia (yes/no) | 1/492 | 0/23 | 1/315 | 0/6 | 0/18 | 0/130 | |
| Histological results colon | 356/814 | Normal colon (yes/no) | 32/324 | 4/12 | 18/197 | 0/6 | 2/14 | 8/95 |
| 356/814 | Chronic colitis (yes/no) | 204/152 | 8/8 | 130/85 | 3/3 | 8/8 | 55/48 | |
| 356/814 | Lymphoplasmacytic colitis (yes/no) | 53/303 | 2/14 | 27/188 | 0/6 | 4/12 | 20/83 | |
| 356/814 | Eosinophilic colitis (yes/no) | 65/291 | 2/14 | 40/175 | 1/5 | 2/14 | 20/83 | |
| 356/814 | Granulomatous colitis (yes/no) | 2/354 | 0/16 | 0/215 | 2/4 | 0/16 | 0/103 | |
| 356/814 | Neoplasia (yes/no) | 0/356 | 0/16 | 0/215 | 0/6 | 0/16 | 0/103 |
| Variable | Overall (n = 814) | Food Responsive (n = 93) | Immunosuppressant Responsive (n = 449) | Antibiotic Responsive (n = 9) | Non Responsive (n = 42) | Non Classified (n = 221) | |
|---|---|---|---|---|---|---|---|
| Treatment | Hydrolyzed diet | 563/814 | 49/93 | 323/449 | 7/9 | 26/42 | 158/221 |
| Novel protein diet | 106/814 | 19/93 | 57/449 | 1/9 | 5/42 | 24/221 | |
| Gastrointestinal diet | 111/814 | 23/93 | 50/449 | 1/9 | 8/42 | 29/221 | |
| Home cooked diet | 18/814 | 0/93 | 10/449 | 0/9 | 1/42 | 7/221 | |
| Other diet | 14/814 | 2/93 | 9/449 | 0/9 | 2/42 | 1/221 | |
| Prednisolone/methylprednisolone | 668/814 | 6/93 | 446/449 | 7/9 | 39/42 | 170/221 | |
| Budesonide | 44/814 | 0/93 | 23/449 | 0/9 | 2/42 | 19/221 | |
| Cyclosporine | 81/814 | 1/93 | 50/449 | 0/9 | 8/42 | 22/221 | |
| Chlorambucil | 11/814 | 0/93 | 2/449 | 0/9 | 2/42 | 7/221 | |
| Sulfasalazine/olsalazine | 20/814 | 0/93 | 4/449 | 2/9 | 4/42 | 10/221 | |
| Prednisolone/methylprednisolone combined with other immunosuppressive treatment | 132/814 | 1/93 | 72/449 | 2/9 | 15/42 | 42/221 | |
| Antibiotic treatment | 341/814 | 8/93 | 138/449 | 9/9 | 28/42 | 158/221 | |
| Gastroprotectant treatment | 512/814 | 48/93 | 299/449 | 5/9 | 28/42 | 132/221 | |
| Cobalamin supplementation | 380/814 | 36/93 | 216/449 | 3/9 | 27/42 | 98/221 | |
| Folic acid supplementation | 189/814 | 21/93 | 111/449 | 1/9 | 12/42 | 44/221 | |
| Probiotics | 91/814 | 5/93 | 46/449 | 2/9 | 7/42 | 31/221 | |
| Other diseases/medication | Other diseases | 453/814 | 56/93 | 266/449 | 5/9 | 15/42 | 111/221 |
| Other medication | 281/814 | 18/93 | 158/449 | 4/9 | 20/42 | 81/221 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holmberg, J.; Pelander, L.; Ljungvall, I.; Harlos, C.; Spillmann, T.; Häggström, J. Chronic Enteropathy in Dogs—Epidemiologic Aspects and Clinical Characteristics of Dogs Presenting at Two Swedish Animal Hospitals. Animals 2022, 12, 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12121507
Holmberg J, Pelander L, Ljungvall I, Harlos C, Spillmann T, Häggström J. Chronic Enteropathy in Dogs—Epidemiologic Aspects and Clinical Characteristics of Dogs Presenting at Two Swedish Animal Hospitals. Animals. 2022; 12(12):1507. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12121507
Chicago/Turabian StyleHolmberg, Johanna, Lena Pelander, Ingrid Ljungvall, Caroline Harlos, Thomas Spillmann, and Jens Häggström. 2022. "Chronic Enteropathy in Dogs—Epidemiologic Aspects and Clinical Characteristics of Dogs Presenting at Two Swedish Animal Hospitals" Animals 12, no. 12: 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12121507