
Development of an Ultrasound Technique to Evaluate the Popliteal Complex in the Horse

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
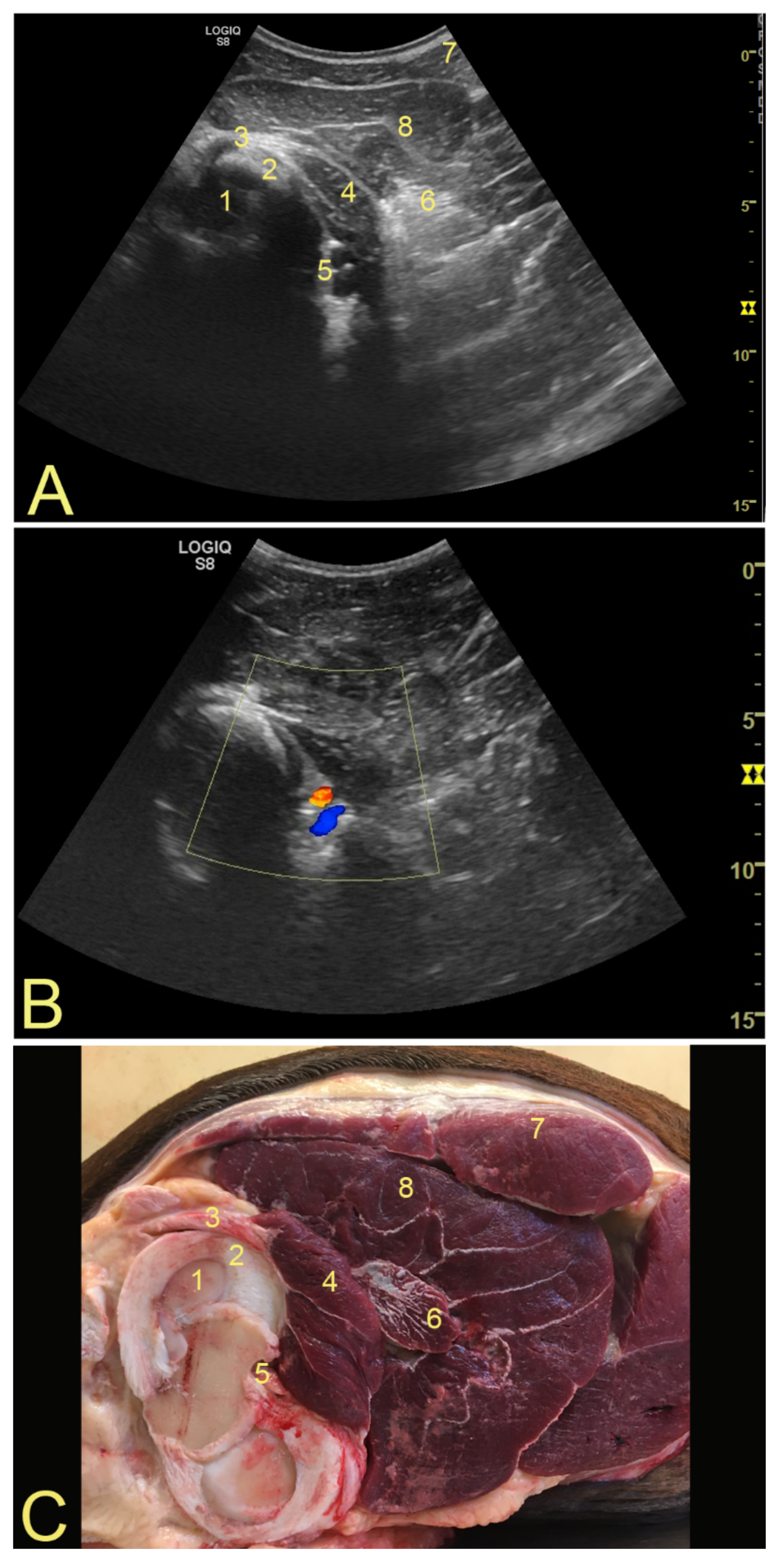
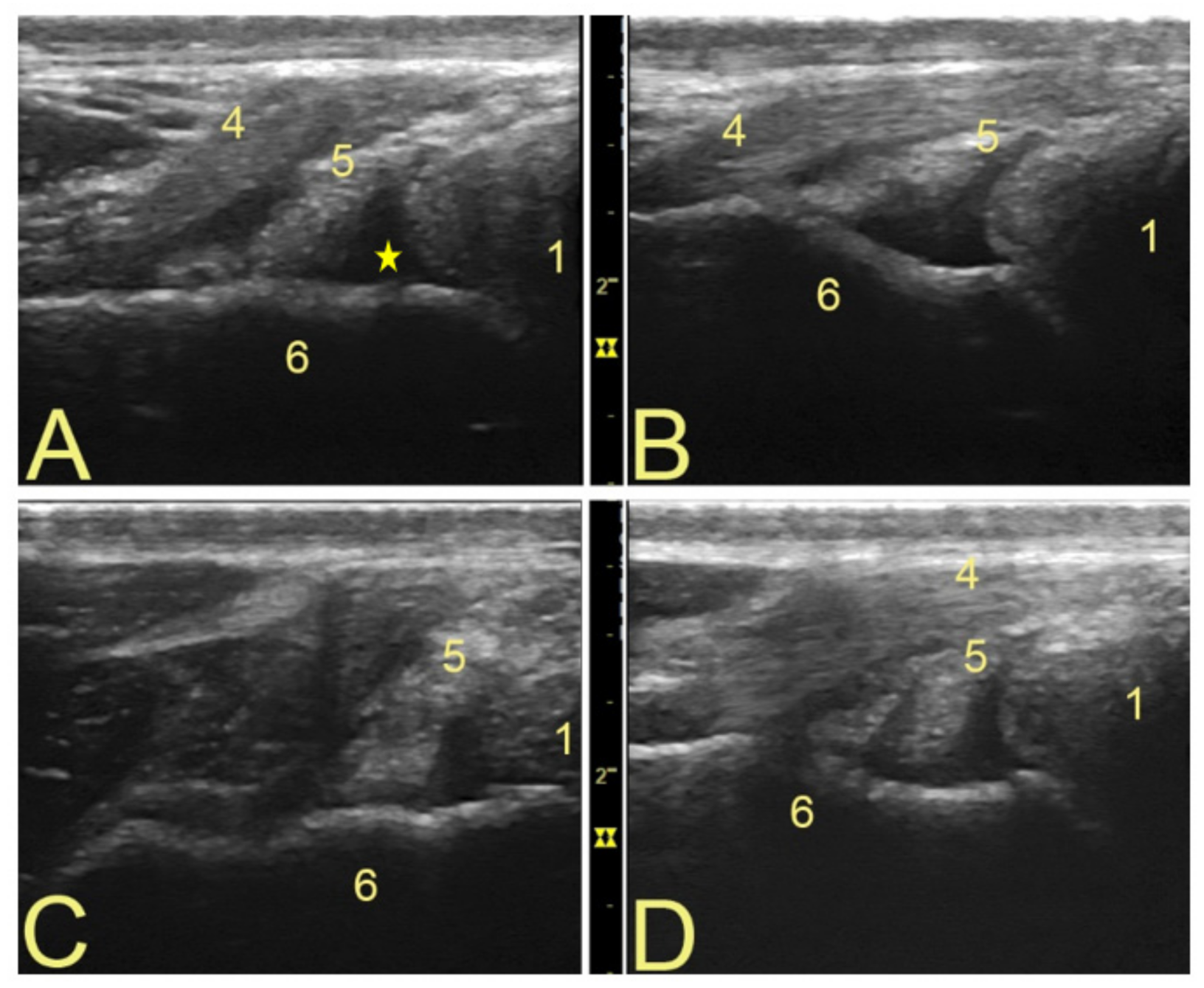
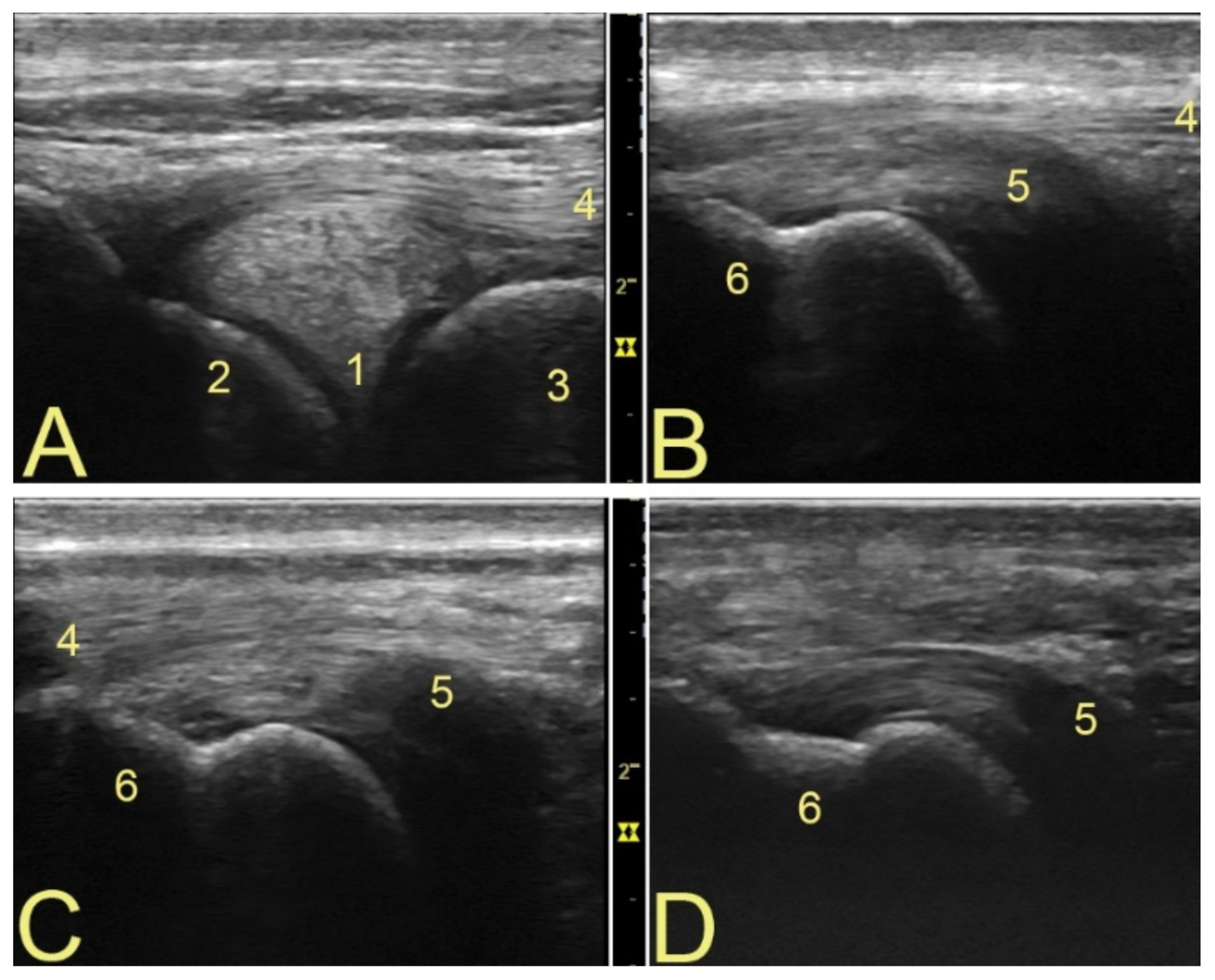
3.1. Anatomical Landmarks for Probe Positioning and Technical Settings
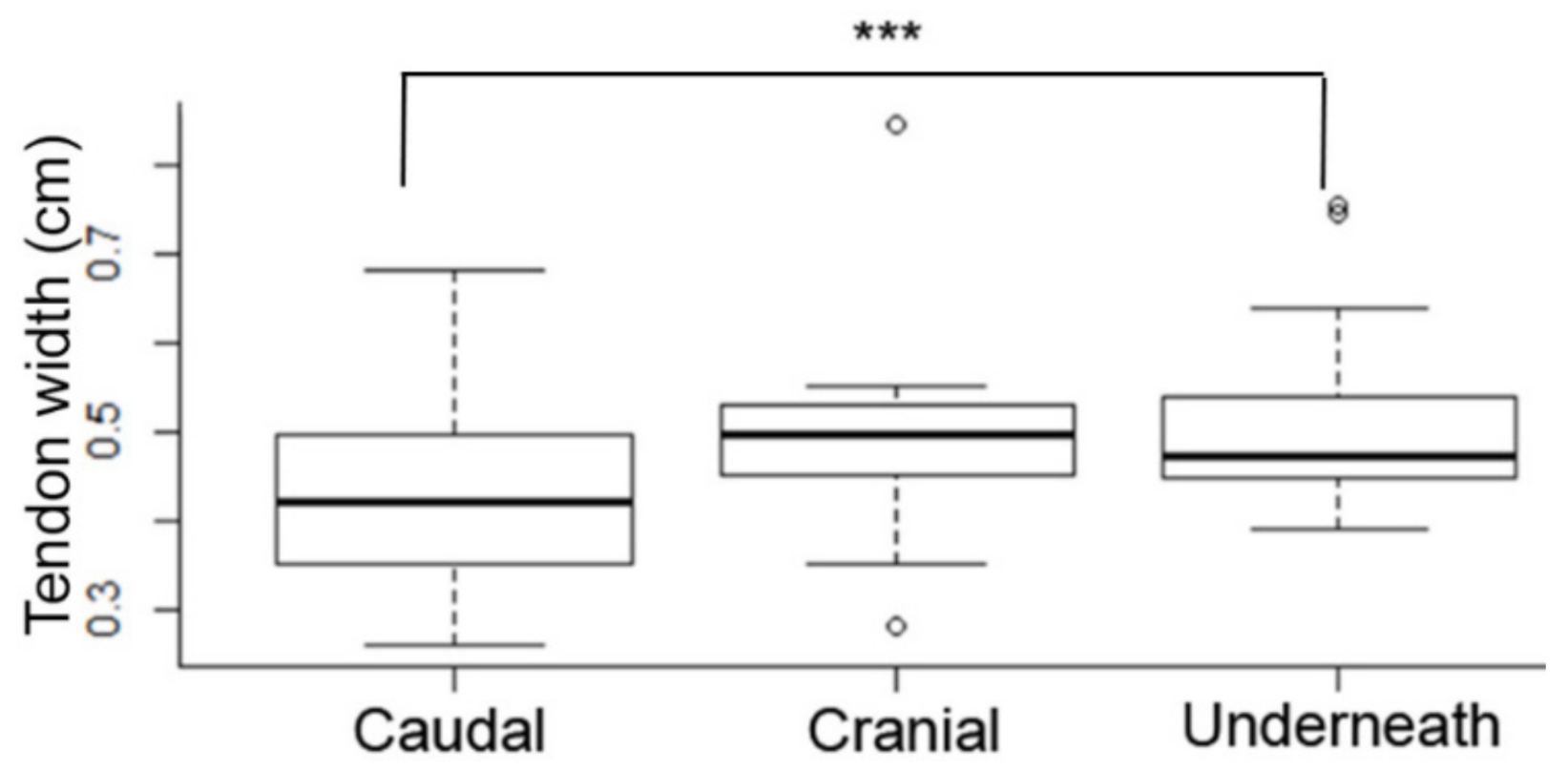
3.2. Popliteal Complex Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Simonnet, M.-L.; Rooze, M.; Feipel, V. The proximal attachments of the popliteus muscle: A quantitative study and clinical significance. Surg. Radiol. Anat. 2003, 25, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Griffith, C.J.; Laprade, R.F.; Coobs, B.R.; Olson, E.J. Anatomy and biomechanics of the posterolateral aspect of the canine knee. J. Orthop. Res. 2007, 25, 1231–1242. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.A.; Stuart, M.J.; Whelan, D.B. Posterolateral Instability of the Knee: Evaluation, Treatment, Results. Sports Med. Arthrosc. Rev. 2010, 18, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Quinn, S.; Wensel, J.; Kim, J.; Demlow, T. Diagnosis of popliteus injuries with MR imaging. Skelet. Radiol. 1995, 24, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Singer, E.R.; Barnes, J.; Saxby, F.; Murray, J.K. Injuries in the event horse: Training versus competition. Vet. J. 2008, 175, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Swor, T.M.; Dabareiner, R.M.; Honnas, C.M.; Cohen, N.D.; Black, J.B. Musculoskeletal problems associated with lameness and poor performance in cutting horses: 200 cases (2007–2015). J. Am. Vet. Med. Assoc. 2019, 254, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Cuevas-Ramos, G.; Cova, M.; Arguelles, D.; Prades, M. Anatomical variations of the equine popliteal tendon. J. Vet. Sci. 2019, 20, e36. [Google Scholar] [CrossRef] [PubMed]
- Rosas, H.G. Unraveling the Posterolateral Corner of the Knee. Radiogr. 2016, 36, 1776–1791. [Google Scholar] [CrossRef] [PubMed]
- Ebling, A.J.; Slack, J.; Reef, V.B. Imaging diagnosis-avulsion of the origin of the popliteal tendon in a horse. Vet. Radiol. Ultrasound 2008, 49, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, C.-R.; Marta, P. Case Report of a Complex Lateral Femorotibial Joint Injury with Popliteal Tendonitis in a Foal. J. Equine Vet. Sci. 2020, 91, 103144. [Google Scholar] [CrossRef] [PubMed]
- Hoegaerts, M.; Nicaise, M.; Van Bree, H.; Saunders, J.H. Cross-sectional anatomy and comparative ultrasonography of the equine medial femorotibial joint and its related structures. Equine Vet. J. 2010, 37, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Adrian, A.M.; Barrett, M.F.; Werpy, N.M.; Kawcak, C.E.; Chapman, P.L.; Goodrich, L.R. A comparison of arthroscopy to ultrasonography for identification of pathology of the equine stifle. Equine Vet. J. 2016, 49, 314–321. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, H.D.; Bladon, B.M. An alternative arthroscopic approach to the caudal pouches of the equine lateral femorotibial joint. Equine Vet. J. 2020, 52, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, N.C.; Kaiser, L.J.; Hauptman, J.; Clayton, H.M. Dynamic mobilisation exercises increase cross sectional area ofmusculus multifidus. Equine Vet. J. 2011, 43, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, S.P.; More, S.R.; Riascos, R.; Lemos, D.F.; Swischuk, L.E. Comprehensive Review of the Anatomy, Function, and Imaging of the Popliteus and Associated Pathologic Conditions. Radiographics 2014, 34, 496–513. [Google Scholar] [CrossRef] [PubMed]
- Skyhar, M.J.; Warren, R.F.; Ortiz, G.J.; Schwartz, E.; Otis, J.C. The effects of sectioning of the posterior cruciate ligament and the posterolateral complex on the articular contact pressures within the knee. J. Bone Jt. Surg. 1993, 75, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Scott, G.S.P.; Crawford, W.H.; Colahan, P.T. Arthroscopic findings in horses with subtle radiographic evidence of osteochondral lesions of the medial femoral condyle: 15 cases (1995–2002). J. Am. Vet. Med. Assoc. 2004, 224, 1821–1826. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Møller-Jensen, M.; Blomquist, M.H.; Mortensen, C.L.; Olsson, I.K.C.; Cuevas-Ramos, G. Development of an Ultrasound Technique to Evaluate the Popliteal Complex in the Horse. Animals 2022, 12, 800. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12070800
Møller-Jensen M, Blomquist MH, Mortensen CL, Olsson IKC, Cuevas-Ramos G. Development of an Ultrasound Technique to Evaluate the Popliteal Complex in the Horse. Animals. 2022; 12(7):800. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12070800
Chicago/Turabian StyleMøller-Jensen, Merete, Michaela Hansen Blomquist, Camilla Lamhauge Mortensen, Isolde Katharina Christersdotter Olsson, and Gabriel Cuevas-Ramos. 2022. "Development of an Ultrasound Technique to Evaluate the Popliteal Complex in the Horse" Animals 12, no. 7: 800. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12070800