
An Arabic Sedentary Behaviors Questionnaire (ASBQ): Development, Content Validation, and Pre-Testing Findings

 , , and
, , and
Abstract
:1. Background
2. Methods and Procedures
2.1. Institutional Review Board (IRB) Approval and Parental Consent
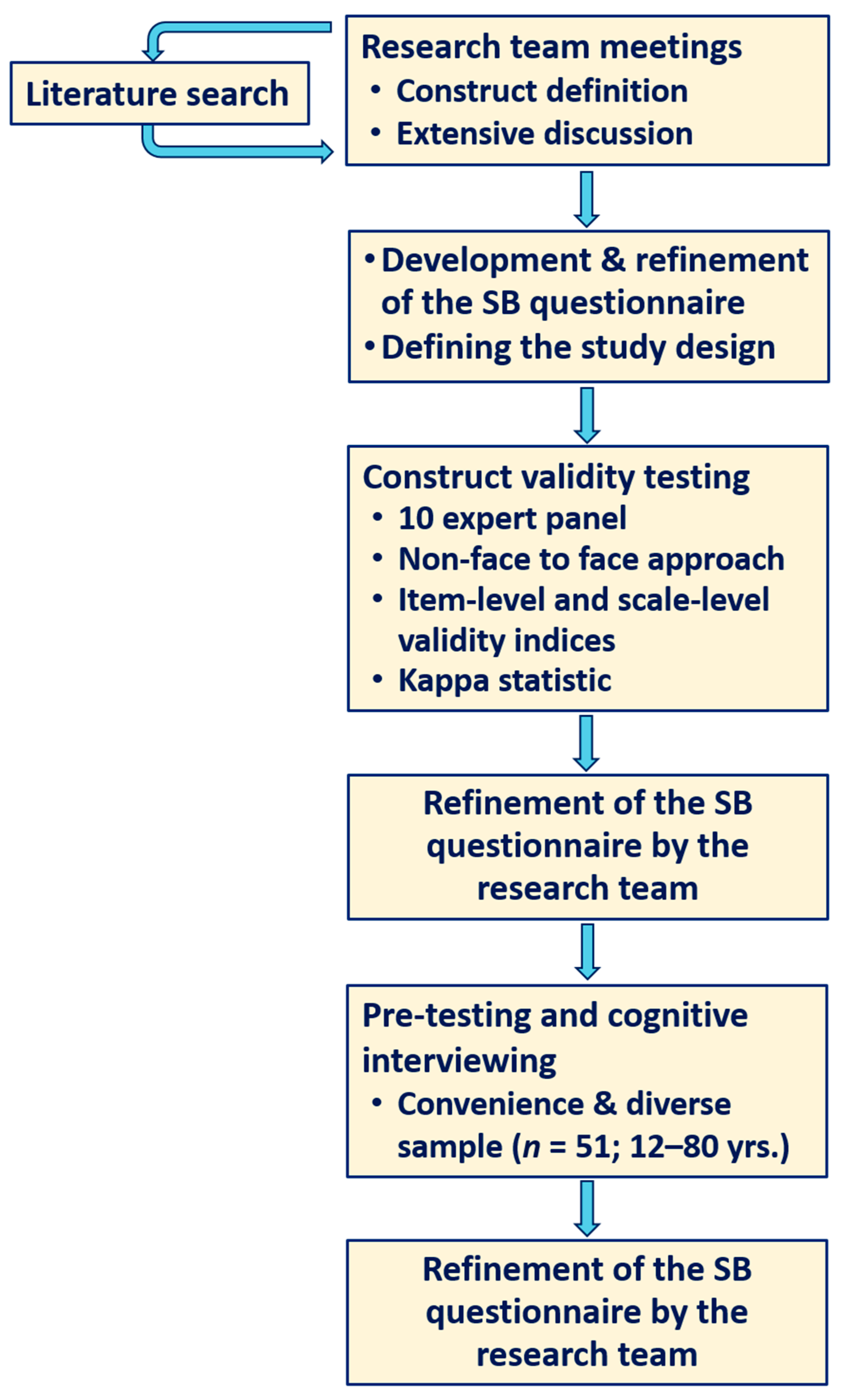
2.2. Arabic SB Questionnaire (ASBQ) Development
- It should be practical when administered and take a reasonably short time to complete (maximum 10–15 min).
- Questions should cover all domains of SB activities that expend no more than 1.5 METs (sitting, reclining, and lying down while reading, viewing a screen and non-screen-based sedentary time, socializing, sitting in a car, bus, or train, sitting at school or at work, doing hobbies or household activities while seated, etc.).
- Can be applicable to a wide range of age groups from adolescents to elderly.
- Sedentary time is summed to account for total sedentary time in hours and minutes per weekday and on weekends.
- All possible psychometric properties testing must be conducted when developing and validating the instrument, including content validity, internal consistency, construct validity, reliability, and criterion validity, using an objective method such as the activPAL accelerometer as a criterion measure.
2.3. Content Validity Testing
2.4. Pre-Testing the ASBQ
- What do you think the question is about?
- Is the question clear and understandable? If not, how can it be made clearer?
- Do you have any questions about the items?
- How could the wording be clearer?
- Are there activities that we omitted?
- Did any of the questions make you feel uncomfortable?
2.5. Anthropometric Measurements
2.6. Computational and Statistical Analyses of the Data
3. Results
3.1. Content Validity Findings
3.2. Pre-Test Findings
4. Discussion
4.1. Strengths and Limitations
4.2. Future Steps
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Dedication
References
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; on behalf of SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Cao, C.; Kantor, E.D.; Nguyen, L.H.; Zheng, X.; Park, Y.; Giovannucci, E.L.; Matthews, C.E.; Colditz, G.A.; Cao, Y.; et al. Trends in Sedentary Behavior among the US Population, 2001–2016. JAMA 2019, 321, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- López-Fernández, J.; López-Valenciano, A.; Mayo, X.; Liguori, G.; Lamb, M.A.; Copeland, R.J.; Jiménez, A. No changes in adolescent’s sedentary behaviour across Europe between 2002 and 2017. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health. Preventive Health Behaviors. In The 2019 World Health Survey of Saudi Arabia; Ministry of Health: Riyadh, Saudi Arabia, 2021. Available online: https://www.moh.gov.sa/en/Ministry/Statistics/Indicator/Documents/2-Preventive-Health-Behaviors.pdf (accessed on 22 February 2021).
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary Time and Its Association with Risk for Disease Incidence, Mortality, and Hospitalization in Adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Gorber, S.C.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. S3), S240–S265. [Google Scholar] [CrossRef]
- González, K.; Fuentes, J.; Márquez, J.L. Physical Inactivity, Sedentary Behavior and Chronic Diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J.H. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef]
- Bauman, A.E.; Chau, J.Y.; Ding, D.; Bennie, J. Too Much Sitting and Cardio-Metabolic Risk: An Update of Epidemiological Evidence. Curr. Cardiovasc. Risk Rep. 2013, 7, 293–298. [Google Scholar] [CrossRef]
- Frydenlund, G.; Jørgensen, T.; Toft, U.; Pisinger, C.; Aadahl, M. Sedentary leisure time behavior, snacking habits and cardiovascular biomarkers: The Inter99 Study. Eur. J. Prev. Cardiol. 2012, 19, 1111–1119. [Google Scholar] [CrossRef]
- Pereira, S.M.P.; Ki, M.; Power, C. Sedentary Behaviour and Biomarkers for Cardiovascular Disease and Diabetes in Mid-Life: The Role of Television-Viewing and Sitting at Work. PLoS ONE 2012, 7, e31132. [Google Scholar] [CrossRef] [PubMed]
- Hartman, Y.A.W.; Tillmans, L.C.M.; Benschop, D.L.; Hermans, A.N.L.; Nijssen, K.M.R.; Eijsvogels, T.M.H.; Willems, P.H.G.M.; Tack, C.J.; Hopman, M.T.E.; Claassen, J.A.H.R.; et al. Long-Term and Acute Benefits of Reduced Sitting on Vascular Flow and Function. Med. Sci. Sports Exerc. 2021, 53, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.B.; Bauman, A.; Tolstrup, J.S. Total sitting time and the risk of incident diabetes in Danish adults (the DANHES cohort) over 5 years: A prospective study. Br. J. Sports Med. 2016, 50, 1382–1387. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behavior; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 24 June 2021).
- Van der Ploeg, H.P.; Hillsdon, M. Is sedentary behaviour just physical inactivity by another name? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 142. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in Sedentary Time. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting Time, Physical Activity, and Risk of Mortality in Adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Thosar, S.S.; Bielko, S.L.; Mather, K.J.; Johnston, J.D.; Wallace, J.P. Effect of Prolonged Sitting and Breaks in Sitting Time on Endothelial Function. Med. Sci. Sports Exerc. 2015, 47, 843–849. [Google Scholar] [CrossRef] [Green Version]
- Prince, S.A.; Leblanc, A.G.; Colley, R.C.; Saunders, T.J. Measurement of sedentary behaviour in population health surveys: A review and recommendations. PeerJ 2017, 5, e4130. [Google Scholar] [CrossRef] [Green Version]
- Carr, L.J.; Mahar, M.T. Accuracy of Intensity and Inclinometer Output of Three Activity Monitors for Identification of Sedentary Behavior and Light-Intensity Activity. J. Obes. 2011, 2012, 1–9. [Google Scholar] [CrossRef]
- Pedišić, Ž.; Bauman, A. Accelerometer-based measures in physical activity surveillance: Current practices and issues. Br. J. Sports Med. 2015, 49, 219–223. [Google Scholar] [CrossRef]
- Cliff, D.; Hesketh, K.D.; Vella, S.A.; Hinkley, T.; Tsiros, M.; Ridgers, N.; Carver, A.; Veitch, J.; Parrish, A.; Hardy, L.; et al. Objectively measured sedentary behaviour and health and development in children and adolescents: Systematic review and meta-analysis. Obes. Rev. 2016, 17, 330–344. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Davis, M.; Stathi, A.; Hamer, M. Associations between multiple indicators of objectively-measured and self-reported sedentary behaviour and cardiometabolic risk in older adults. Prev. Med. 2011, 54, 82–87. [Google Scholar] [CrossRef]
- Prince, S.A.; Cardilli, L.; Reed, J.L.; Saunders, T.J.; Kite, C.; Douillette, K.; Fournier, K.; Buckley, J.P. A comparison of self-reported and device measured sedentary behaviour in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 31. [Google Scholar] [CrossRef]
- Rivière, F.; Aubert, S.; Omorou, A.Y.; Ainsworth, E.; Vuillemin, A. Taxonomy-based content analysis of sedentary behavior questionnaires: A systematic review. PLoS ONE 2018, 13, e0193812. [Google Scholar] [CrossRef] [Green Version]
- Chaabane, S.; Chaabna, K.; Abraham, A.; Mamtani, R.; Cheema, S. Physical activity and sedentary behaviour in the Middle East and North Africa: An overview of systematic reviews and meta-analysis. Sci. Rep. 2020, 10, 1–24. [Google Scholar] [CrossRef]
- Chau, J.Y.; Van Der Ploeg, H.; Dunn, S.; Kurko, J.; Bauman, A.E. Validity of the Occupational Sitting and Physical Activity Questionnaire. Med. Sci. Sports Exerc. 2012, 44, 118–125. [Google Scholar] [CrossRef]
- Clark, B.K.; Winkler, E.; Healy, G.N.; Gardiner, P.G.; Dunstan, D.W.; Owen, N.; Reeves, M.M. Adults’ Past-Day Recall of Sedentary Time: Reliability, validity, and responsiveness. Med. Sci. Sports Exerc. 2013, 45, 1198–1207. [Google Scholar] [CrossRef] [Green Version]
- Marshall, A.L.; Miller, Y.D.; Burton, N.W.; Brown, W.J. Measuring Total and Domain-Specific Sitting: A study of reliability and validity. Med. Sci. Sports Exerc. 2010, 42, 1094–1102. [Google Scholar] [CrossRef]
- Rosenberg, D.E.; Norman, G.J.; Wagner, N.; Patrick, K.; Calfas, K.J.; Sallis, J.F. Reliability and Validity of the Sedentary Behavior Questionnaire (SBQ) for Adults. J. Phys. Act. Heal. 2010, 7, 697–705. [Google Scholar] [CrossRef]
- Wijndaele, K.; Bourdeaudhuij, I.D.E.; Godino, J.G.; Lynch, B.M.; Griffin, S.J.; Westgate, K.; Brage, S. Reliability and Validity of a Domain-Specific Last 7-d Sedentary Time Questionnaire. Med. Sci. Sports Exerc. 2014, 46, 1248–1260. [Google Scholar] [CrossRef] [Green Version]
- Affuso, O.; Stevens, J.; Catellier, D.; McMurray, R.G.; Ward, D.S.; Lytle, L.; Sothern, M.S.; Young, D.R. Validity of self-reported leisure-time sedentary behavior in adolescents. J. Negat. Results Biomed. 2011, 10, 2. [Google Scholar] [CrossRef] [Green Version]
- Cabanas-Sánchez, V.; Martínez-Gómez, D.; Esteban-Cornejo, I.; Castro-Piñero, J.; Conde-Caveda, J.; Veiga, Ó.L. Reliability and validity of the Youth Leisure-time Sedentary Behavior Questionnaire (YLSBQ). J. Sci. Med. Sport 2018, 21, 69–74. [Google Scholar] [CrossRef]
- Chu, A.H.Y.; Ng, S.H.X.; Koh, D.; Müller-Riemenschneider, F. Domain-Specific Adult Sedentary Behaviour Questionnaire (ASBQ) and the GPAQ Single-Item Question: A Reliability and Validity Study in an Asian Population. Int. J. Environ. Res. Public Health 2018, 15, 739. [Google Scholar] [CrossRef] [Green Version]
- Csizmadi, I.; Neilson, H.K.; Kopciuk, K.A.; Khandwala, F.; Liu, A.; Friedenreich, C.; Yasui, Y.; Rabasa-Lhoret, R.; Bryant, H.E.; Lau, D.C.W.; et al. The Sedentary Time and Activity Reporting Questionnaire (STAR-Q): Reliability and Validity against Doubly Labeled Water and 7-Day Activity Diaries. Am. J. Epidemiol. 2014, 180, 424–435. [Google Scholar] [CrossRef] [Green Version]
- De Moraes, A.C.F.; Nascimento-Ferreira, M.V.; de Moraes Forjaz, C.L.; Aristizabal, J.C.; Azzaretti, L.; Nascimento Junior, W.V.; Miguel-Berges, M.L.; Skapino, E.; Delgado, C.; Moreno, L.A.; et al. Reliability and validity of a sedentary behavior questionnaire for South American pediatric population: SAYCARE study. BMC Med. Res. Methodol. 2020, 20, 5–10. [Google Scholar] [CrossRef]
- Dontje, M.L.; Dall, P.M.; Skelton, D.A.; Gill, J.M.R.; Chastin, S.F.M.; Seniors USP on behalf of the Seniors USP Team. Reliability, minimal detectable change and responsiveness to change: Indicators to select the best method to measure sedentary behaviour in older adults in different study designs. PLoS ONE 2018, 13, e0195424. [Google Scholar] [CrossRef] [Green Version]
- Felez-Nobrega, M.; Bort-Roig, J.; Dowd, K.; Wijndaele, K.; Puig-Ribera, A. Validation study of the Spanish version of the Last-7-d Sedentary Time Questionnaire (SIT-Q-7d-Sp) in young adults. PLoS ONE 2019, 14, e0217362. [Google Scholar] [CrossRef] [Green Version]
- Fowles, J.R.; O’Brien, M.W.; Wojcik, W.R.; d’Entremont, L.; Shields, C.A. A pilot study: Validity and reliability of the CSEP−PATH PASB-Q and a new leisure time physical activity questionnaire to assess physical activity and sedentary behaviours. Appl. Physiol. Nutr. Metab. 2017, 42, 677–680. [Google Scholar] [CrossRef] [Green Version]
- Gomersall, S.R.; Pavey, T.G.; Clark, B.K.; Jasman, A.; Brown, W.J. Validity of a Self-Report Recall Tool for Estimating Sedentary Behavior in Adults. J. Phys. Act. Health 2015, 12, 1485–1491. [Google Scholar] [CrossRef]
- Han, H.; Gabriel, K.P.; Kohl, H.W. Evaluations of Validity and Reliability of a Transtheoretical Model for Sedentary Behavior among College Students. Am. J. Health Behav. 2015, 39, 601–609. [Google Scholar] [CrossRef]
- Hardy, L.L.; Booth, M.L.; Okely, A.D. The reliability of the Adolescent Sedentary Activity Questionnaire (ASAQ). Prev. Med. 2007, 45, 71–74. [Google Scholar] [CrossRef]
- Klakk, H.; Wester, C.T.; Olesen, L.G.; Rasmussen, M.G.; Kristensen, P.L.; Pedersen, J.; Grøntved, A. The development of a questionnaire to assess leisure time screen-based media use and its proximal correlates in children (SCREENS-Q). BMC Public Health 2020, 20, 664. [Google Scholar] [CrossRef]
- Lynch, B.M.; Friedenreich, C.M.; Khandwala, F.; Liu, A.; Nicholas, J.; Csizmadi, I. Development and testing of a past year measure of sedentary behavior: The SIT-Q. BMC Public Health 2014, 14, 899. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, T.; So, R.; Takahashi, M. Workers’ physical activity data contribute to estimating maximal oxygen consumption: A questionnaire study to concurrently assess workers’ sedentary behavior and cardiorespiratory fitness. BMC Public Health 2020, 20, 22. [Google Scholar] [CrossRef]
- Mensah, K.; ACTI-Cités consortium; Maire, A.; Oppert, J.-M.; Dugas, J.; Charreire, H.; Weber, C.; Simon, C.; Nazare, J.-A.; Bastian, T. Assessment of sedentary behaviors and transport-related activities by questionnaire: A validation study. BMC Public Health 2016, 16, 753. [Google Scholar] [CrossRef] [Green Version]
- Scholes, S.; Coombs, N.; Pedisic, Z.; Mindell, J.S.; Bauman, A.; Rowlands, A.V.; Stamatakis, E. Age- and Sex-Specific Criterion Validity of the Health Survey for England Physical Activity and Sedentary Behavior Assessment Questionnaire as Compared With Accelerometry. Am. J. Epidemiol. 2014, 179, 1493–1502. [Google Scholar] [CrossRef] [Green Version]
- Whitfield, G.P.; Gabriel, K.K.P.; Kohl, H.W., 3rd. Assessing Sitting across Contexts: Development of the Multicontext Sitting Time Questionnaire. Res. Q. Exerc. Sport 2013, 84, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Verbestel, V.; De Henauw, S.; Bammann, K.; Barba, G.; Hadjigeorgiou, C.; Eiben, G.; Konstabel, K.; Kovács, E.; Pitsiladis, Y.; Reisch, L.; et al. Are context-specific measures of parental-reported physical activity and sedentary behaviour associated with accelerometer data in 2–9-year-old European children? Public Health Nutr. 2015, 18, 860–868. [Google Scholar] [CrossRef]
- Cook, D.A.; Beckman, T.J. Current Concepts in Validity and Reliability for Psychometric Instruments: Theory and Application. Am. J. Med. 2006, 119, 166.e7–166.e16. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. ABC of Content Validation and Content Validity Index Calculation. Educ. Med. J. 2019, 11, 49–54. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Beck, C.T.; Gable, R.K. Ensuring Content Validity: An Illustration of the Process. J. Nurs. Meas. 2001, 9, 201–215. [Google Scholar] [CrossRef]
- Perneger, T.V.; Courvoisier, D.S.; Hudelson, P.M.; Gayet-Ageron, A. Sample size for pre-tests of questionnaires. Qual. Life Res. 2014, 24, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Beatty, P.C.; Willis, G.B. Research Synthesis: The Practice of Cognitive Interviewing. Public Opin. Q. 2007, 71, 287–311. [Google Scholar] [CrossRef] [Green Version]
- Willis, G.B.; Artino, A.R. What Do Our Respondents Think We’re Asking? Using Cognitive Interviewing to Improve Medical Education Surveys. J. Grad. Med Educ. 2013, 5, 353–356. [Google Scholar] [CrossRef] [Green Version]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi-Majd, H.; Nikanfar, A.-R. Design and Implementation Content Validity Study: Development of an instrument for measuring Patient-Centered Communication. J. Caring Sci. 2015, 4, 165–178. [Google Scholar] [CrossRef]
- Cicchetti, D.V.; Sparrow, S.A. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am. J. Ment. Defic. 1981, 86, 127–137. [Google Scholar]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-square for model fit in confirmatory factor analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef]
- Cole, D.A. Utility of confirmatory factor analysis in test validation research. J. Consult. Clin. Psychol. 1987, 55, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Butler, G.P.; Roberts, K.C.; Lapointe, P.; MacKenzie, A.M.; Colley, R.C.; Foley, M.; Saunders, T.J.; Thompson, W. Developing content for national population health surveys: An example using a newly developed sedentary behaviour module. Arch. Public Health 2019, 77, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Saudi Arabia Country Cooperation Strategy 2011–2016; WHO: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/113227 (accessed on 23 June 2021).
- Saudi Vision 2030. Vision Realization Programs. Available online: https://www.vision2030.gov.sa/v2030/vrps/ (accessed on 23 June 2021).
- Bakker, E.A.; Hartman, Y.A.W.; Hopman, M.T.E.; Hopkins, N.D.; Graves, L.E.F.; Dunstan, D.W.; Healy, G.N.; Eijsvogels, T.M.H.; Thijssen, D.H.J. Validity and reliability of subjective methods to assess sedentary behaviour in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 75. [Google Scholar] [CrossRef] [PubMed]
- Saunders, T.J.; Prince, S.A.; Tremblay, M.S. Clustering of children’s activity behaviour: The use of self-report versus direct measures. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hazzaa, H.M. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int. J. Health Sci. 2018, 12, 50–64. [Google Scholar]
- Ekelund, U.; Brage, S.; Froberg, K.; Harro, M.; Anderssen, S.A.; Sardinha, L.; Riddoch, C.; Andersen, L.B. TV Viewing and Physical Activity Are Independently Associated with Metabolic Risk in Children: The European Youth Heart Study. PLOS Med. 2006, 3, e488. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef]
- Martinez-Gomez, D.; Rey-López, J.P.; Chillón, P.; Gómez-Martínez, S.; Vicente-Rodríguez, G.; Martín-Matillas, M.; Garcia-Fuentes, M.; Delgado, M.; Moreno, L.A.; Veiga, O.L.; et al. Excessive TV viewing and cardiovascular disease risk factors in adolescents. The AVENA cross-sectional study. BMC Public Health 2010, 10, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platat, C.; Perrin, A.-E.; Oujaa, M.; Wagner, A.; Haan, M.-C.; Schlienger, J.-L.; Simon, C. Diet and physical activity profiles in French preadolescents. Br. J. Nutr. 2006, 96, 501–503. [Google Scholar]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Abahussain, N.A.; Qahwaji, D.M.; Alahmadi, M.A.; Musaiger, A.O. Association of dietary habits with levels of physical activity and screen time among adolescents living in Saudi Arabia. J. Hum. Nutr. Diet. 2014, 27 (Suppl. S2), 204–213. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]


{kind=link}
| Domain | Item | Time |
|---|---|---|
| Leisure sitting time | 1. Watching movies, TV, videos (regardless of the source-TV, computer, phone) | [ ] hrs. [ ] min |
| 2. Playing computer/video games | [ ] hrs. [ ] min | |
| 3. Internet surfing or using social media for fun | [ ] hrs. [ ] min | |
| Education or mentally active reading sitting time | 4. Doing homework/studying | [ ] hrs. [ ] min |
| 5. Reading for fun | [ ] hrs. [ ] min | |
| Talking, listening or resting sitting time | 6. Sitting and talking with family or friends in person or via internet | [ ] hrs. [ ] min |
| 7. Listening to Quran, Radio, or music (without doing anything else) | [ ] hrs. [ ] min | |
| 8. Resting (lying down, but not taking a nap, etc.) | [ ] hrs. [ ] min | |
| Doing craft or hobby sitting time | 9. Doing hobbies that require thinking/reasoning (doing puzzles, playing cards, doing crossword puzzles, etc.) | [ ] hrs. [ ] min |
| 10. Doing simple crafts or art work while sitting (like drawing, painting, knitting, sewing, etc.) | [ ] hrs. [ ] min | |
| Transportation sitting time | 11. Using transportation while sitting (in car, bus, train, subway or motorbike) | [ ] hrs. [ ] min |
| Household sitting time | 12. Doing household tasks while seated (cooking, ironing, slicing foods, etc.) | [ ] hrs. [ ] min |
| 13. Engaged in other activities than the above while seated, name them: | [ ] hrs. [ ] min |
| Item No. | Experts Relevance Ratings | Expert Agreement | Item-Level Content Validity Index (I-CVI) | Universal Agreement (UA) | Modified Kappa Agreement | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||||
| Q-1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 9 | 0.90 | 0 | 0.90 |
| Q-5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-6 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-9 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-10 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-11 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-12 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 | 0.90 | 0 | 0.90 |
| Q-13 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-14 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 | 0.70 | 0 | 0.69 |
| Q-15 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 1 | 1 | 1 |
| Q-16 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 8 | 0.80 | 0 | 0.80 |
| Average Item relevance | 0.94 | 0.94 | 1 | 0.88 | 1 | 0.94 | 1 | 1 | 1 | 0.88 | 9.56 | S-CVI = 0.96 | S-CVI/UA = 0.75 | 0.96 |
| Average relevance across the 10 experts = 0.96 | ||||||||||||||
| Item No. | Relevant (Rating 3 or 4) | Not Relevant (Rating 1 or 2) | Item-Level Content Validity Index (I-CVI) * | Content Validity Ration ** | Interpretation |
|---|---|---|---|---|---|
| Q-1 | 10 | 0 | 1 | 1 | Appropriate |
| Q-2 | 10 | 0 | 1 | 1 | Appropriate |
| Q-3 | 10 | 0 | 1 | 1 | Appropriate |
| Q-4 | 9 | 1 | 0.90 | 0.80 | Appropriate |
| Q-5 | 10 | 0 | 1 | 1 | Appropriate |
| Q-6 | 10 | 0 | 1 | 1 | Appropriate |
| Q-7 | 10 | 0 | 1 | 1 | Appropriate |
| Q-8 | 10 | 0 | 1 | 1 | Appropriate |
| Q-9 | 10 | 0 | 1 | 1 | Appropriate |
| Q-10 | 10 | 0 | 1 | 1 | Appropriate |
| Q-11 | 10 | 0 | 1 | 1 | Appropriate |
| Q-12 | 9 | 1 | 0.90 | 0.80 | Appropriate |
| Q-13 | 10 | 0 | 1 | 1 | Appropriate |
| Q-14 | 7 | 3 | 0.70 | 0.40 | Need Revision *** |
| Q-15 | 10 | 0 | 1 | 1 | Appropriate |
| Q-16 | 8 | 2 | 0.80 | 0.60 | Appropriate |
| Item | Category | Value |
|---|---|---|
| Age (years) | Mean (SD) | 38.3 (18.2) |
| Age category | Adolescents—12–17 years (%) | 23.5% (12) |
| Young Adults—18–35 (%) | 23.5% (12) | |
| Middle age—36–49 (%) | 23.5% (12) | |
| Older Adults 50+ (%) | 29.5% (15) | |
| Sex (%) | h | 49% (25) |
| Body weight (kg) | Mean (SD) | 72.9 (15.3) |
| Height (cm) | Mean (SD) | 162.4 (8.1) |
| BMI (kg/m2) | Mean (SD) | 27.7 (5.9) |
| Underweight (%) | 5.9% (3) | |
| Normal weight (%) | 29.4% (15) | |
| Overweight (%) | 31.4% (16) | |
| Obese (%) | 33.3% (17) | |
| Education | High school or less (%) | 45% (23) |
| College degree (%) | 33.4% (17) | |
| Postgraduate degree (%) | 21.6% (11) | |
| Working status | Not working (%) | 27.4% (14) |
| Working online (%) | 31.4% (16) | |
| Working in-person (%) | 41.2% (21) |
| Item Number (Question) | Participant Understanding of the Intended Meaning | The Content Was Clear for the Participant | The Wording Was Clear for the Participant |
|---|---|---|---|
| 1 | 100% (51) | 98% (50) | 90.2% (46) |
| 2 | 100% (51) | 98% (50) | 90.2% (46) |
| 3 | 98% (50) | 96.1% (49) | 96.1% (49) |
| 4 | 100% (51) | 94.1% (48) | 96.1% (49) |
| 5 | 98% (50) | 98% (50) | 98% (50) |
| 6 | 98% (50) | 94.1% (48) | 98% (50) |
| 7 | 98% (50) | 88.2% (45) | 88.2% (45) |
| 8 | 100% (51) | 96.1% (49) | 94.1% (48) |
| 9 | 100% (51) | 100% (51) | 100% (51) |
| 10 | 100% (51) | 98% (50) | 100% (51) |
| 11 | 98% (50) | 94.1% (48) | 96.1% (49) |
| 12 | 100% (51) | 100% (51) | 100% (51) |
| 13 | 100% (51) | 90.2% (46) | 94.1% (48) |
| 14 | 92.2% (47) | 94.1% (48) | 98% (50) |
| 15 | 100% (51) | 94.1% (48) | 100% (51) |
| 16 | 96.1% (49) | 96.1% (49) | 92.2% (47) |
| Overall (%) | 98.6% | 95.6% | 95.7% |
| Variable | Classification | Total Sedentary Time (Hours/Day) | |||||
|---|---|---|---|---|---|---|---|
| Weekdays | p-Value | Weekends | p-Value | ||||
| Mean (SD) | Correlation | Mean (SD) | Correlation | ||||
| Gender | Male | 13.4 (4.0) | −0.029 p = 0.840 | 0.840 | 14.8 (3.8) | −0.051 p = 0.724 | 0.724 |
| Female | 13.2 (3.3) | 14.4 (4.1) | |||||
| Age category | Adolescents | 14.1 (2.8) | −0.059 p = 0.680 | 0.218 | 14.5 (3.6) | −0.111 p = 0.438 | 0.360 |
| Young adult | 13.6 (3.4) | 16.3 (2.6) | |||||
| Middle age | 11.4 (3.5) | 13.6 (3.8) | |||||
| Older age | 14.0 (4.3) | 14.2 (4.9) | |||||
| BMI category | Underweight | 17.0 (0.0) | −0.385 p = 0.005 | 0.046 * | 17.3 (1.2) | −0.018 p = 0.903 | 0.532 |
| Normal weight | 14.6 (3.0) | 13.8 (4.1) | |||||
| Overweight | 12.9 (3.6) | 14.9 (4.0) | |||||
| Obesity | 11.9 (3.9) | 14.6 (3.9) | |||||
| Education | High school | 13.9 (3.5) | −0.020 p = 0.888 | 0.144 | 14.4 (3.9) | 0.018 p = 0.899 | 0.887 |
| College degree | 11.9 (3.8) | 15.0 (3.7) | |||||
| Post graduate | 14.3 (3.2) | 14.5 (4.3) | |||||
| Work status | Not working | 13.5 (4.2) | −0.099 p = 0.488 | 0.631 | 13.7 (4.9) | 0.115 p = 0.423 | 0.602 |
| Working online | 13.9 (2.8) | 15.0 (3.5) | |||||
| Working in-person | 13.8 (3.8) | 14.9 (3.5) | |||||
| Comorbidity | No | 13.5 (3.2) | −0.041 p = 0.778 | 0.152 | 14.4 (4.1) | 0.060 p = 0.673 | 0.627 |
| Yes | 13.2 (4.1) | 14.9 (3.8) | |||||
| Item (Question) Number | Correlation with Total Sedentary Time during Weekdays | Correlation with Total Sedentary Time during Weekends |
|---|---|---|
| 1 | −0.153 (p = 0.284) | - |
| 2 | −0.062 (p = 0.665) | - |
| 3 | 0.576 (p < 0.001) | 0.516 (p < 0.001) |
| 4 | 0.473 (p < 0.001) | 0.446 (p = 0.001) |
| 5 | 0.245 (p = 0.083) | 0.224 (p = 0.114) |
| 6 | 0.195 (p = 0.171) | 0.195 (p = 0.170) |
| 7 | 0.124 (p = 0.386) | 0.340 (p = 0.015) |
| 8 | 0.443 (p = 0.001) | 0.160 (p = 0.262) |
| 9 | 0.353 (p = 0.011) | 0.375 (p = 0.007) |
| 10 | 0.206 (p = 0.146) | 0.225 (p = 0.112) |
| 11 | 0.198 (p = 0.165) | 0.114 (p = 0.427) |
| 12 | 0.259 (p = 0.066) | 0.357 (p = 0.010) |
| 13 | 0.293 (p = 0.037) | 0.219 (p = 0.122) |
| 14 | 0.179 (p = 0.208) | 0.134 (p = 0.349) |
| 15 | 0.263 (p = 0.096) | 0.153 (p = 0.284) |
| 16 | −0.225 (p = 0.113) | 0.134 (p = 0.349) |
| Component | Initial Eigenvalues | Rotation Sum of Squared Loading | ||||
|---|---|---|---|---|---|---|
| Total | % Variance | Cumulative % | Total | % Variance | Cumulative % | |
| Weekdays | ||||||
| 1 | 2.446 | 18.814 | 18.814 | 1.887 | 14.517 | 14.517 |
| 2 | 1.695 | 13.039 | 31.853 | 1.521 | 11.701 | 26.218 |
| 3 | 1.544 | 11.876 | 43.729 | 1.518 | 11.679 | 37.897 |
| 4 | 1.361 | 10.473 | 54.202 | 1.509 | 11.608 | 49.505 |
| 5 | 1.047 | 8.055 | 62.257 | 1.440 | 11.076 | 60.581 |
| 6 | 1.024 | 7.881 | 70.137 | 1.242 | 9.556 | 70.137 |
| 7 | 0.876 | 6.739 | 76.876 | |||
| 8 | 0.711 | 5.470 | 82.346 | |||
| 9 | 0.684 | 5.262 | 87.608 | |||
| 10 | 0.488 | 3.757 | 91.364 | |||
| 11 | 0.450 | 3.459 | 94.824 | |||
| 12 | 0.411 | 3.165 | 97.989 | |||
| 13 | 0.261 | 2.011 | 100.00 | |||
| Weekends | ||||||
| 1 | 2.242 | 17.244 | 17.244 | 1.940 | 14.927 | 14.927 |
| 2 | 1.849 | 14.224 | 31.468 | 1.762 | 13.557 | 28.484 |
| 3 | 1.516 | 11.663 | 43.131 | 1.604 | 12.339 | 40.823 |
| 4 | 1.257 | 9.673 | 52.804 | 1.356 | 10.431 | 51.254 |
| 5 | 1.142 | 8.782 | 61.586 | 1.343 | 10.331 | 61.586 |
| 6 | 0.993 | 7.637 | 69.223 | |||
| 7 | 0.787 | 6.050 | 75.273 | |||
| 8 | 0.764 | 5.875 | 81.148 | |||
| 9 | 0.605 | 4.656 | 85.804 | |||
| 10 | 0.569 | 4.381 | 90.185 | |||
| 11 | 0.503 | 3.869 | 94.054 | |||
| 12 | 0.416 | 3.201 | 97.254 | |||
| 13 | 0.357 | 2.746 | 100.00 | |||
| Component | Weekdays | Weekends | ||
|---|---|---|---|---|
| Item (Question) Number | Coefficient | Item (Question) Number | Coefficient | |
| 1 | 10 | 0.814 | 4 | 0.716 |
| 5 | −0.666 | 13 | 0.689 | |
| 7 | 0.638 | 3 | 0.550 | |
| 15 | 0.499 | 15 | 0.451 | |
| 2 | 9 | 0.782 | 10 | 0.766 |
| 8 | 0.663 | 9 | 0.677 | |
| - | - | 11 | 0.618 | |
| 3 | 3 | 0.860 | 12 | 0.749 |
| 13 | 0.634 | 6 | 0.735 | |
| 4 | 12 | 0.783 | 5 | −0.669 |
| 11 | 0.757 | 14 | 0.637 | |
| 5 | 6 | 0.791 | 7 | 0.864 |
| 14 | 0.655 | 8 | −0.645 | |
| 6 | 4 | 0.906 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hazzaa, H.M.; Alothman, S.A.; Albawardi, N.M.; Alghannam, A.F.; Almasud, A.A. An Arabic Sedentary Behaviors Questionnaire (ASBQ): Development, Content Validation, and Pre-Testing Findings. Behav. Sci. 2022, 12, 183. https://0-doi-org.brum.beds.ac.uk/10.3390/bs12060183
Al-Hazzaa HM, Alothman SA, Albawardi NM, Alghannam AF, Almasud AA. An Arabic Sedentary Behaviors Questionnaire (ASBQ): Development, Content Validation, and Pre-Testing Findings. Behavioral Sciences. 2022; 12(6):183. https://0-doi-org.brum.beds.ac.uk/10.3390/bs12060183
Chicago/Turabian StyleAl-Hazzaa, Hazzaa M., Shaima A. Alothman, Nada M. Albawardi, Abdullah F. Alghannam, and Alaa A. Almasud. 2022. "An Arabic Sedentary Behaviors Questionnaire (ASBQ): Development, Content Validation, and Pre-Testing Findings" Behavioral Sciences 12, no. 6: 183. https://0-doi-org.brum.beds.ac.uk/10.3390/bs12060183