Regulation of Reactive Oxygen Species-Mediated Damage in the Pathogenesis of Schizophrenia

1
Independent Researcher, 1353 Tanaka Drive, San Jose, CA 95131, USA
2
Massachusetts Institute of Technology, 77 Massachusetts Ave, Cambridge, MA 02139, USA
*
Author to whom correspondence should be addressed.
Brain Sci. 2020, 10(10), 742; https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10100742
Submission received: 4 September 2020
/
Revised: 6 October 2020
/
Accepted: 15 October 2020
/
Published: 16 October 2020
{kind=link}
{kind=link}
Abstract
:The biochemical integrity of the brain is paramount to the function of the central nervous system, and oxidative stress is a key contributor to cerebral biochemical impairment. Oxidative stress, which occurs when an imbalance arises between the production of reactive oxygen species (ROS) and the efficacy of the antioxidant defense mechanism, is believed to play a role in the pathophysiology of various brain disorders. One such disorder, schizophrenia, not only causes lifelong disability but also induces severe emotional distress; however, because of its onset in early adolescence or adulthood and its progressive development, consuming natural antioxidant products may help regulate the pathogenesis of schizophrenia. Therefore, elucidating the functions of ROS and dietary antioxidants in the pathogenesis of schizophrenia could help formulate improved therapeutic strategies for its prevention and treatment. This review focuses specifically on the roles of ROS and oxidative damage in the pathophysiology of schizophrenia, as well as the effects of nutrition, antipsychotic use, cognitive therapies, and quality of life on patients with schizophrenia. By improving our understanding of the effects of various nutrients on schizophrenia, it may become possible to develop nutritional strategies and supplements to treat the disorder, alleviate its symptoms, and facilitate long-term recovery.
1. Introduction
As the most metabolically active part of the human body, the brain generates many reactive oxygen species (ROS), which can cause oxidative stress (OS) when excessively produced or inadequately removed [1,2,3]. This, in turn, can lead to neural cell damage [4,5]. Given that high oxidation activity must be balanced with antioxidant activity in the brain, it is an organ prone to oxidation-related damage [6,7,8]. Such OS is a potential factor in brain deterioration and loss of gray matter, which lead to issues with cognition and daily functioning [9,10,11,12]; furthermore, OS has been associated with a plethora of psychiatric disorders [13,14,15,16,17]. One such disorder, schizophrenia is characterized by emotional, cognitive, and behavioral disturbances, as well as inaccurate perceptions of reality and high mortality and morbidity [18,19,20,21,22]. Understanding the etiology and pathophysiology of schizophrenia is a prerequisite for developing more effective treatments. To date, the factors implicated in the development of schizophrenia include excessive free radicals and impaired antioxidant defense [5,23]. As such, a diet rich in antioxidants has been suggested as a promising strategy for slowing the progression of the disorder [24,25].
This review specifically focuses on the role of ROS-mediated oxidative damage in the pathophysiology of schizophrenia. In addition, current knowledge on treating schizophrenia with antioxidants is presented, along with information on how antioxidant levels in patients with schizophrenia may be regulated by nutritional, pharmacological, and lifestyle factors. Because schizophrenia is a progressive disorder from its onset in adolescence or early adulthood [10,26,27,28], the intake of natural antioxidants may help regulate its development [29].
2. Schizophrenia
Schizophrenia is a severe mental disorder characterized by frequent relapses, cognitive impairment [30,31,32], and emotional and functional disability [33,34,35]. Compared to healthy controls, patients with schizophrenia have lower total brain, gray matter, and white matter volumes and densities; on the other hand, schizophrenia patients have significantly higher third and lateral ventricle volumes [36,37]. Brain abnormalities in the amygdala, cerebellum, basal ganglia, corpus callosum, inferior parietal lobule, medial temporal lobe, superior temporal gyrus, prefrontal cortical areas, and thalamus have also been found in postmortem studies of individuals with the disorder [38,39]. The symptoms of schizophrenia are classified as positive, such as hallucinations and delusions, and negative, such as social withdrawal and flat affect [40,41,42,43,44,45]. Cognitive deficits, including the impairment of attention, memory, and executive function, are also hallmarks of schizophrenia; they present from the prodromal phase of the disorder before psychotic symptoms fully intensify [28,46,47]. Such cognitive decline can present at an early age among those with schizophrenia, eventually leading to self-care issues and impaired social and occupational function [28,48,49]. Moreover, patients with schizophrenia often report anxiety, depression, obsessive behavior, substance abuse, and suicidal ideation. Given these symptoms, schizophrenia has a high social impact [26].
3. Oxidative Stress
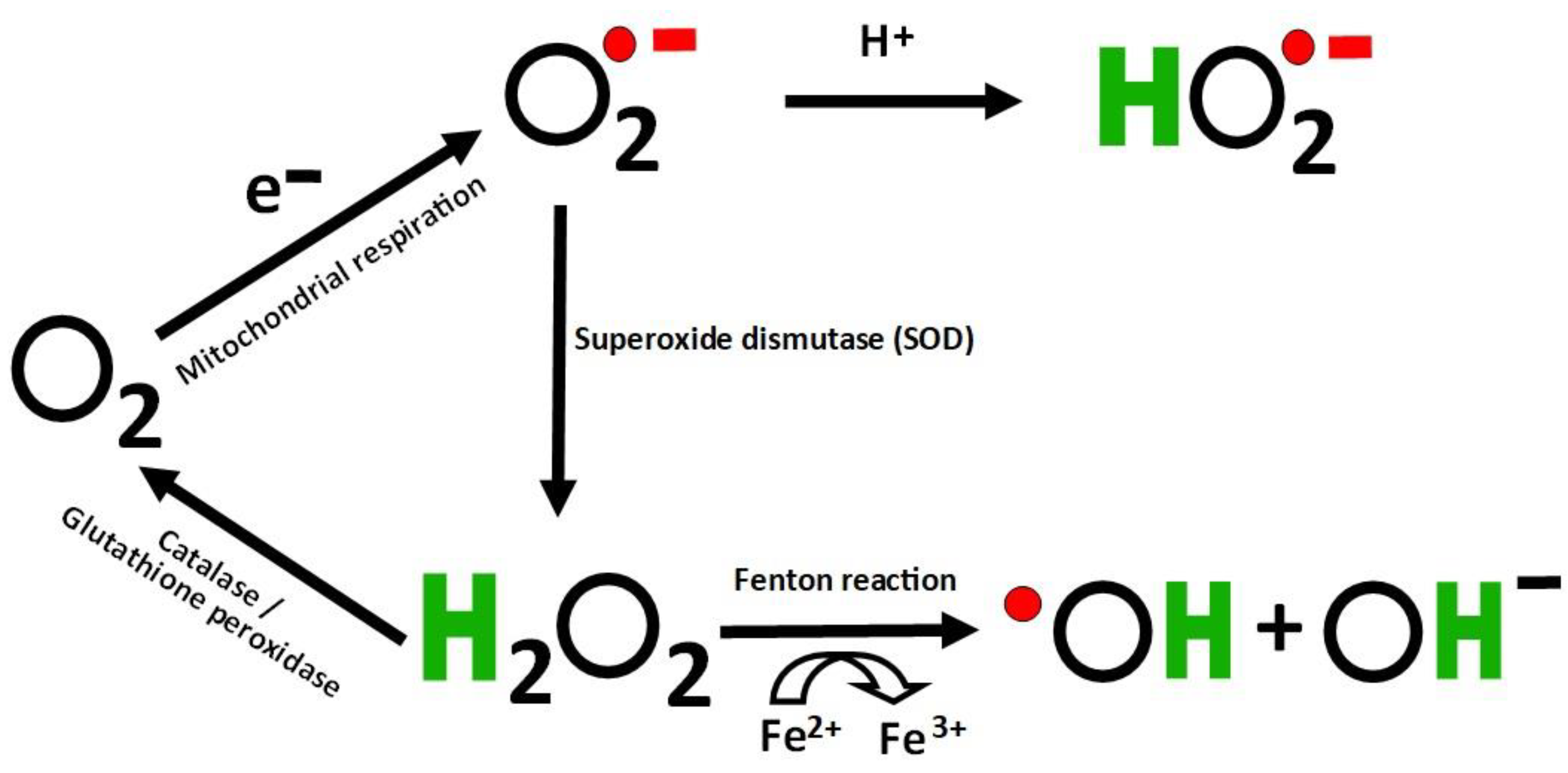
As the brain requires high levels of oxygen to function normally, it is known to be a major repository of free radicals and ROS as well as a high-risk area for neurodegeneration [15,50,51,52]. OS takes place when an imbalance arises between antioxidants and oxidants [53,54,55]. Free radicals display at least one unpaired electron and are intermediate in reducing oxygen to water [56]. Continuous reduction of oxygen causes the generation of ROS [15,57] (Figure 1). This imbalance may be attributable to a malfunctioning antioxidant system and/or high levels of ROS including superoxide anion radicals (O2•), hydroxyl radicals (HO•), peroxyl radicals (HOO•), hydrogen peroxide (H2O2), nitric oxide, and reactive nitrogen species [58,59,60,61].
O2− is central to the formation of ROS; superoxide dismutases (SOD) can transform O2− into the more stable H2O2 [62] (Figure 2). H2O2 can subsequently form highly reactive ·OH radicals through the Fenton reaction using Fe2+ as a catalyst [63]. These ·OH radicals are among the most cytotoxic and reactive ROS [64]. Conversely, H2O2 may be decomposed to water and O2 by catalase and peroxidases, such as glutathione peroxidase [65]. In the short-term, OS helps eradicate pathogens as part of the immune response [55]; however, severe OS caused by a major imbalance in antioxidants and oxidants causes cell damage [66,67,68]. ROS can be similarly beneficial, playing a role in modulating inflammation [2,69,70,71]; however, by modifying lipids, proteins, nucleic acids, and other molecules, excess ROS can also be damaging [61,72,73]. In particular, increased ROS may lead to lipid peroxidation, which damages cells and organelle membranes [74,75]. Furthermore, surplus ROS can also facilitate mutagenesis by causing purine oxidation, strand breaks in DNA, and cross-linking of proteins and DNA; it may also induce chromatin structure changes that can epigenetically modify gene expression [6,76,77].
4. Mitochondrial ROS Production
Mitochondria are responsible for cellular processes, such as energy production, cell death, and signaling [78]. They produce 90% of endogenous ROS due to leakage in electron transfer that continuously generates O2− [79,80]. Mitochondria maintain an efficient antioxidant system to control ROS levels [63]. These levels fluctuate rapidly in mitochondria and are involved in normal cellular signaling [81]. Thus, alterations in mitochondrial redox balance due to toxins, chronic ischemia, or mutation may cause disease due to oxidative stress [81]. Neurons are particularly vulnerable to OS from ROS overproduction and deficient antioxidant responses [81]. These cells are long-lived and do not undergo mitosis. Consequently, OS that leads to mitochondrial dysfunction and eventual cell death results in loss of neuronal function [82]. Mitochondria and ROS are significant in determining how cells respond to disruption in homeostasis by stressors such as infection and metabolic changes [83]. Mitochondrial dysfunction in schizophrenia alters redox balance and produces low-grade inflammation [6]. Genetic, biochemical, and anatomical studies all provide evidence that mitochondrial dysfunction plays a role in schizophrenia [84]. Such abnormalities vary with symptoms, treatment status, and treatment response [84].
5. Association between Oxidative Stress and Schizophrenia
An accumulation of evidence indicates that the pathophysiology of schizophrenia is partially attributable to heightened OS [85,86,87,88,89,90]. Evidence of higher lipid peroxidation levels, changes in plasma antioxidant levels, and alterations in antioxidant enzyme activity have also been found in schizophrenia patients [91]. The oxidative imbalance in schizophrenia patients has been demonstrated through protein carbonylation, lipid peroxidation, and higher 8-hydroxydeoxyguanosine levels indicating cell death and DNA damage [10,75,92,93]. Heightened OS in those with schizophrenia can occur through disruptions to the antioxidant enzymes catalase, superoxide dismutase (SOD), glutathione, and glutathione peroxidase (GPx), [94,95,96,97,98,99,100], as well as via increased levels of the lipid peroxidation products malondialdehyde (MDA) and thiobarbituric acid reactive substances [23,85,101], and lower antioxidant levels in the cerebrospinal fluid, red blood cells, serum, and plasma [102,103]. ROS generation can also increase with schizophrenia; this has been attributed to dopamine autooxidation, mitochondrial dysfunction, and the prooxidant effects of some antipsychotic medications [104,105,106]. Mitochondrial dysfunction, which is also associated with OS, has been linked to neurodegeneration in schizophrenia [107,108,109]. Indeed, neurons are particularly vulnerable to excess ROS because of their high metabolism, plentiful fatty acids (for peroxidation), decreased antioxidant levels, reduced regenerative capabilities, and high transition metal concentrations that catalyze hydroxyl radical formation [2,15,53,110]. Given this evidence, OS could function as a biomarker for schizophrenia, indicating the pathophysiology, etiology, symptomatology, and treatment response of the disorder, and could potentially predict the progression of symptoms towards psychosis [111,112,113].
Increased oxidant activity and decreased antioxidant activity have been reported in patients with schizophrenia [107]. In a meta-analysis, researchers evaluated the evidence of OS from peripheral measures during the various clinical phases of schizophrenia [114]. A cross-sectional study comprising of 42 healthy individuals and 42 schizophrenia cases measured the total antioxidant capacity and the prooxidant antioxidant balance (which combines the prooxidant load and antioxidant capacity within one measurement) in the serum of participants; the latter value was observed to be elevated in schizophrenia patients, which indicates the prevalence of OS in the progression of schizophrenia [102]. In addition, lower antioxidant capacity indicates that schizophrenia patients may be more vulnerable to OS damage [8,102]. In another study, the relationship between SOD activity and thiobarbituric acid reactive substances in the platelets of 36 schizophrenia patients (aged 18–36) was examined in comparison to 32 healthy controls; lower antioxidative processes were observed in schizophrenia patients as well as an imbalance between prooxidants and antioxidants [115]. Furthermore, SOD activity was significantly reduced in the platelets of the patients with schizophrenia compared with the healthy controls [115]. Along with impeded antioxidant enzyme activity, numerous studies have associated decreased plasma total antioxidant status with schizophrenia [116,117,118]. For example, in a study of 50 participants with schizophrenia (aged 18–60) and 50 controls matched for age and sex, blood samples were collected to determine SOD, MDA, glutathione, and GPx levels; schizophrenia patients had significantly lower levels of SOD and GPx, but higher levels of MDA than controls, indicating increased OS [119]. Overall, evidence suggests that OS occurs in schizophrenia with an imbalance in the antioxidant defense mechanism and antioxidant enzyme impairment [120,121].
6. Oxidative Damage in Schizophrenia
Postmortem brains and peripheral tissues from patients with schizophrenia show evidence of OS [26], which is often the result of ROS-induced damage to macromolecules such as lipids, proteins, nucleic acids, and polysaccharides [122,123]. Studies of OS in schizophrenia have indicated the heightened oxidative damage caused by increased prooxidants and reduced antioxidants [5,124]. OS-induced damage to macromolecules ultimately affects cell damage, which is a likely factor in schizophrenia. In addition, patients with schizophrenia have been found to have weaker antioxidant defenses in their cerebrospinal fluid, peripheral blood [5,125], and postmortem brain tissue [28]. Evidence from genetic studies also suggests that these patients likely have a decreased capacity for staging a sufficient antioxidant defense response [28]. Furthermore, reports of abnormal plasma, serum, and red blood cell OS parameters also indicate that those with schizophrenia have a deficient antioxidant defense [114,126]. The inability of antioxidant defense mechanisms to combat free-radical production results in damage to cell membranes, has an adverse effect on neurotransmission [127,128], and contributes to the symptoms of schizophrenia [28,129]. Specifically, several studies have reported high nitric oxide and MDA levels, both important markers of OS, as well as reduced antioxidant glutathione levels in patients with schizophrenia [5,99,117,130]. The effects of increased cell damage and OS have also been implicated in the development of schizophrenia [131,132,133]. For example, in a study of 64 patients with schizophrenia and 80 healthy controls, in which 8-hydroxydeoxyguanosine levels, total antioxidant status, and total oxidant status were measured in plasma, OS was found to play a role in schizophrenia pathogenesis through disease damage [134]. Although reduced total antioxidant status has been observed in schizophrenia patients in several other studies, again indicating the link between the disorder and OS, similar differences have not been observed for oxidative damage of DNA [135].
7. Positive Effects of Nutraceuticals and Antioxidants on Schizophrenia
Given that OS-induced cell damage and the exacerbation schizophrenia symptoms can at least in part be attributed to the impairment of the antioxidant defense system [136,137], strengthening this system and scavenging free radicals by employing endogenous and exogenous antioxidants could potentially reduce the effects of OS [138,139,140]. Enzymes such as catalase, GPx, and SOD, along with vitamins E and C, are typically measured to quantify the antioxidant defense system in schizophrenia patients [115,124,130,141,142]; such antioxidants may also, therefore, have a therapeutic effect on schizophrenia [5,20,143]. Indeed, some antioxidants such as vitamins and essential polyunsaturated fatty acids have been shown to ameliorate the symptoms of schizophrenia [144,145,146]. Moreover, several studies have reported that schizophrenia can be treated with a combination of dietary supplementation, adjuvant antioxidant therapy, and antipsychotic medication [147,148].
8. Role of Vitamins in Schizophrenia Treatment
Adjuvant treatment including certain vitamins and minerals may have therapeutic benefits against psychiatric disorders [149,150], and there are viable biological mechanisms by which these molecules may produce their protective effects [151]. Given that quality of diet is considered a risk factor for some psychiatric disorders [152,153], it may also be possible to improve symptoms by addressing patients’ nutritional deficiencies [154]. In particular, schizophrenia patients are known to be more likely to maintain poor diets. Some preliminary evidence suggests that specific vitamin and mineral supplements could ameliorate the symptoms of schizophrenia [139].
8.1. Roles of Vitamin E and Vitamin C
Vitamins C and E are the most common antioxidants studied in relation to schizophrenia [124,155,156]. Schizophrenia patients have been shown to have lower plasma vitamin C and E levels compared to healthy controls [142]. Moreover, early intervention with these two vitamins, along with other antioxidants such as beta carotene, could potentially prevent oxidative damage and exacerbation of symptoms in schizophrenia, as shown by observations of lipid peroxidation and impaired antioxidant defense [157,158,159]. However, multiple studies, including 2-week to 2-year treatment periods, have failed to observe changes in Brief Psychiatric Rating Scale scores with daily doses of 600–1600 IU vitamin E [160]. Nevertheless, early studies suggest that vitamin E may help treat tardive dyskinesia, an occasional effect of long-term antipsychotic use [161]. Although a meta-analysis including 11 randomized clinical trials did not find any credible evidence for vitamin E alleviating tardive dyskinesia, some studies within the meta-analysis found that vitamin E supplementation helped prevent further deterioration of tardive dyskinesia [162]; therefore, there may be some benefit to adding vitamin E as a treatment strategy for schizophrenia [161].
Because vitamin E is lipid soluble, it has limited ability to prevent oxidative damage in the mitochondria, nucleus, and cytosolic proteins, which is where the majority of ROS are formed [163,164,165,166]. Thus, vitamin C, which is water soluble, has also been investigated as a beneficial supplement [167]. However, the adjunctive use of both vitamins in schizophrenia treatment necessitates caution since over-consumption can result in prooxidant rather than antioxidant effects [124]. The benefits of vitamin C include safeguarding neurons from OS, ensuring the proper regulation of neurotransmission, ameliorating inflation, and altering neuronal development and epigenetic function [168,169,170]. In addition to curtailing membrane phospholipid peroxidation, vitamin C can also enhance the regeneration of vitamin E [163]. Interestingly, the concentration of vitamin C in the brain is 10-fold higher than in serum; it can also be retained in the brain after crossing the blood brain barrier through GLUT1, a glucose transmitter [124]. Patients with schizophrenia have been shown to exhibit significantly reduced levels of SOD and vitamin C in comparison to healthy controls [171,172]. Therefore, supplementing with vitamin C is important: it helps maintain appropriate central nervous system (CNS) functioning, strengthens the antioxidant defense system of the brain [154], and safeguards neuronal differentiation and maturation, myelin formation, neurotransmission modulation, and catecholamine synthesis [173].
In a double-blind placebo-controlled study, 40 schizophrenia patients were split into groups receiving either vitamin C or a placebo for eight weeks, and both groups were also adjunctly treated with atypical antipsychotics [174]. While increased levels of serum MDA and reduced levels of plasma ascorbic acid were typically observed in schizophrenia patients, these levels were significantly reversed in the group treated with vitamin C relative to the placebo group. After eight weeks, there were also significantly greater improvements in the Brief Psychiatric Rating Scale (BPRS) scores of the vitamin C group compared to the placebo group [174]. Thus, oral vitamin C supplementation taken with atypical antipsychotics may lower OS, increase ascorbic acid levels, and enhance BPRS scores, signifying its potential as an adjunctive treatment for schizophrenia [174]. In another study, researchers observed that the intake of vitamin C, vitamin E, and omega-3 fatty acid supplements lowered BPRS and positive and negative syndrome scale (PANSS) scores in schizophrenia [143]. Studies involving combined treatment of vitamin E and C or vitamin C treatment alone have shown that these treatments significantly enhance BPRS scores and reduce total dyskinetic movement scores [124,174]. Both vitamins are nonenzymatic antioxidants; therefore, they likely reduce OS in schizophrenia by dismantling free-radical chain reactions [161].
Sources of Vitamin C and Vitamin E
Vitamin C is best obtained through certain fruits and vegetables including oranges, grapefruit, kiwis, potatoes, tomatoes, broccoli, green and red peppers, cabbage, cauliflower, strawberries, Brussels sprouts, and cantaloupe [175,176]. Dietary sources of vitamin E include nuts, such as almonds, peanuts, and hazelnuts; seeds, such as sunflower seeds; and vegetable oils, such as wheat germ oil, soybean oil, sunflower oil, and corn oil [175]. Vitamin E is also readily found in spinach, broccoli, mango, kiwi, tomato, and fortified cereals [176].
8.2. Role of Vitamin D
Schizophrenia patients are often deficient in vitamin D, which is known to function in neurodevelopment and neuroprotection [177,178,179,180,181,182]. The neuroprotective effects of vitamin D arise through modulation of neurotrophin production, calcium homeostasis, neuromediator synthesis, and prevention of oxidative damage [183,184,185]. A study on schizophrenia risk, which included 424 schizophrenia patients and 424 date of birth and gender matched controls, found that neonatal vitamin D levels (determined from serum 25-hydroxyvitamin (25(OH)) vitamin D3 levels in the participants’ dried blood spots gathered during the first year of their lives) influence the odds of developing schizophrenia; participants in the bottom two quintiles for vitamin D levels had a two-fold greater risk of schizophrenia compared to participants in all other quintiles [186]. In another study, in which 25(OH) vitamin D was measured in 20 recent onset schizophrenia patients and 20 matched controls, lower levels of vitamin D were linked to more severe symptoms and cognitive deficits in schizophrenia [187]. In a study of 60 patients with chronic schizophrenia, participants received either a placebo or a 50,000 IU dose of vitamin D3 once every two weeks in addition to daily consumption of probiotics (8 × 109 CFU) for 12 weeks; the combined treatment of vitamin D and probiotics had a beneficial impact not only on metabolic profiles but also on total and general PANSS scores [188].
Sources of Vitamin D
Few natural foods are good sources of vitamin D; however, fatty fish, such as tuna, salmon, and mackerel, as well as fish liver oils, are considered to be optimal sources [175]. Vitamin D is also available in limited quantities in egg yolks, cheese, and beef liver, primarily via vitamin D3 and 25(OH) D3 [189]. Some mushrooms offer D2, albeit in inconsistent quantities [190].
8.3. Role of Vitamin B
Several meta-analyses have shown that schizophrenia patients experience greater folate deficiencies than their healthy counterparts [191,192]. One study established that intake of fish fat was positively correlated with folate and vitamin B12 levels in patients with schizophrenia, suggesting that such patients can experience dietary deficits of key nutrients [193]. Further studies of schizophrenia patients have examined the potential effects of supplementation with vitamin B6 alone, folate alone, folic acid with vitamin B12, and folic acid combined with vitamins B12 and B6 [194]. An analysis of seven randomized-controlled trials that investigated vitamin B supplementation (including 297 individuals in total) found that it had a significant positive impact on total symptom scores [139]. Moreover, a 3-month supplementation with vitamin B (400 μg B12, 2 mg folic acid, and 25 mg B6) significantly lowered PANSS total scores for 42 schizophrenia patients with increased homocysteine levels [139]. In addition, the efficacy of vitamin B supplements had been shown to be significantly related to the duration of schizophrenia [145,195]: supplementation has a greater reductive effect on symptoms in the earlier stages of the disorder [139]. Overall, group B vitamin supplements, especially folate and vitamin B12, appear to improve the general symptoms of schizophrenia [196,197].
Sources of Vitamin B
Sources of folate include dark green leafy vegetables, nuts, fruits, peas, juices, beans, dairy, seafood, meat, eggs, grains, and poultry [175]. Specifically, folate can be found in foods such as spinach, rice, brussels sprouts, lettuce, mustard greens, green peas, wheat germ, crab, peanuts, papaya, yeast, cantaloupe, fish, ground beef, beef liver, black-eyed peas, asparagus, spaghetti, avocado, broccoli, bread, kidney beans, tomato juice, orange juice, oranges, bananas, eggs, baked beans, milk, and chicken breast [175]. Many foods are also known to be good sources of vitamin B6 including starchy vegetables, such as potatoes, non-citrus fruit, fish, fortified cereals, poultry, and organ meats such as beef liver. Natural sources of vitamin B12 include fish, milk and dairy, poultry, meat, and eggs [175,198,199]. Although plant-based diets are not adequate sources of vitamin B12, vegetarians can obtain this nutrient through fortified cereals. Vitamin B12 is also found in certain nutritional yeast products [175].
9. Role of Polyunsaturated Fatty Acids in Schizophrenia Treatment
The properties of docosahexaenoic acid (DHA) and omega-3 eicosapentaenoic acid (EPA) are significant for psychosis-related disorders as they are known to reduce OS by modulating mitochondria, decreasing microinflammation stress, and enhancing neurotransmission of serotonin and dopamine [191,200,201]. They can also protect against toxicity due to apoptosis and regulate gene expression of brain-derived neurotrophic factor [202]. Depletion of polyunsaturated fatty acids (PUFAs) has been linked to psychosis and cognitive deficits, and it may be associated with the heightened OS observed in schizophrenia [114,203,204]; on the other hand, similar to EPA and DHA, PUFA treatment can also prevent OS [160]. Disruption of PUFA metabolism and PUFA deficiencies in red blood cell (RBC) membranes are frequently observed in schizophrenia patients [161,205,206]. Similarly, postmortem brain studies have reported lower PUFA levels in schizophrenia patients, particularly arachidonic acid and DHA [203,207]. Seven randomized clinical trials have been conducted to compare EPA supplements against placebos in schizophrenia patients being treated with antipsychotics [207]. Among these, the positive effects of EPA on primary efficiency were reported in two studies [207]. According to one study, conducted over 12 weeks with 80 patients, EPA reduced the time until a response was observed in patients experiencing non-affective psychosis; moreover, the EPA treatment group showed a 20% reduction in antipsychotic medication use [208].
Omega-3 supplementation is known to substantially improve certain psychopathologies [209,210,211,212]. Importantly, combining omega-3 EPUFAs and antioxidants, especially during the nascent stages of illness when the human brain exhibits considerable neuroplasticity, is potentially more efficacious in improving long-term clinical outcomes [211]. In schizophrenia, omega-3 fatty acid supplements significantly alleviated symptoms in four out of seven randomized clinical trials [54,161,213]. This may be because omega-3 fatty acids contain generous amounts of EPA, which has antioxidant properties [214,215,216]. In a specific study of omega-3 supplements in schizophrenia, the nutrient significantly improved the symptoms of both schizophrenia and tardive dyskinesia [161]. Similarly, a combination of vitamin E, vitamin C, and omega-3 significantly reduced the severity of positive and negative symptoms, as well as RBC-SOD levels, in chronic schizophrenia patients over a four month period [212]. Such reduced RBC-SOD levels indicate that combining antioxidants with omega-3 PUFAs can alleviate many of the symptoms associated with OS; decreased RBC-SOD levels show that excess SOD production is no longer required to compensate for high ROS concentrations [212]. Correspondingly, in a placebo-controlled randomized clinical trial in which an n-3 PUFA intervention was tested over 26 weeks with 71 schizophrenia patients (aged 16–35), treatment reduced the severity of symptoms [217]. In another study, haloperidol treatment was supplemented with omega-3 fatty acids (1000 mg capsules, 180 mg EPA, 120 mg DHA; taken twice daily), vitamin E (400 IU taken twice daily), and vitamin C (1000 mg taken daily) in 17 patients with schizophrenia [212]. Over a period of four months, these patients were measured with the Scale for the Assessment of Negative Symptoms, Barnes Akathisia Rating Scale, Simpson Angus Scale, and BPRS; in all four assessments, scores in follow-up visits were significantly lower than baseline scores [212].
Sources of PUFA
10. Role of Antipsychotics
Clinical trials show that antipsychotic medications significantly improve psychotic symptoms for patients with schizophrenia [221,222,223]. Atypical antipsychotics may partially normalize ROS metabolism and oxidative stress [75]. Commonly used antipsychotic drugs include aripiprazole, brexpiprazole, chlorpromazine, clozapine, lurasidone, and risperidone. At doses recommended for managing acute episodes, antipsychotic drugs can alter lipid peroxidation product (TBARS) levels in plasma [75,224].
10.1. Aripiprazole
Aripiprazole is an effective and well-tolerated atypical antipsychotic for patients with schizophrenia [225,226,227]. The drug acts as a dopamine D2 and serotonin 5-HT1A receptor agonist and as a serotonin 5-HT2A receptor antagonist [228,229]. Aripiprazole displays high affinity for serotonin 5-HT1A and 5-HT2A receptors and dopamine D2 and D3 receptors [223]. The drug is unlikely to cause weight gain, sedation, or other changes in metabolism [226,230,231,232]. A 52-week trial of 478 patients with schizophrenia found that intramuscular injections of aripiprazole every four weeks (fixed at either 441 mg or 882 mg) was well-tolerated, making it a suitable treatment for schizophrenia [233]. One study showed that aripiprazole did not affect levels of a plasma lipid peroxidation marker but did induce some insignificant prooxidative effects at low doses [75].
10.2. Brexpiprazole
Brexpiprazole is an oral atypical antipsychotic drug with clinical evidence for efficacy in the treatment of schizophrenia [234,235,236]. Like aripiprazole, the drug acts as an antagonist of serotonin 5-HT2A receptors and a partial agonist for serotonin 5-HT1A and dopamine D2 receptors [236,237,238,239,240]. Phase 3 clinical trials indicate that 2–4 mg of brexpiprazole per day is effective short-term in reducing PANSS scores and alleviating symptoms of acute schizophrenia [221,241,242]. An analysis of twelve clinical trials demonstrated that brexpiprazole was superior to placebo in improving PANSS scores in patients with schizophrenia at doses of 1 mg, 2 mg, and 4 mg over six weeks [243]. Brexpiprazole is well-tolerated and is administered daily [242,244].
10.3. Risperidone
Risperidone is an established treatment that alleviates both positive and negative symptoms of schizophrenia [245,246,247]. Fifty-four of 60 patients showed a decrease of 20% or more in PANSS score after two months of risperidone treatment; the remaining patients showed less reduction [245]. On average, participants gained 0.84 kg of weight during treatment [245]. Other studies found that risperidone treatment may reduce serum interleukin-6, testosterone, and estradiol levels [246,248]. Also, 30 patients with schizophrenia administered stable doses of risperidone displayed significantly reduced plasma total antioxidant capacity and increased TBARS levels compared to 30 healthy controls [249]. However, incubating control plasma with risperidone at doses commonly used in treatment produced no changes in lipid peroxidation [249].
10.4. Lurasidone
Lurasidone is an atypical antipsychotic with high affinity for dopamine D2 receptors, noradrenaline alpha-2C receptors, and serotonin 5-HT2A, 5-HT1A, and 5HT7 receptors [222,250,251]. A study of 2373 patients with acute schizophrenia found lurasidone was safe and effective, especially with a daily dose of 80 mg [251]. Lurasidone administered at 40 mg and 80 mg daily in adolescent patients with schizophrenia in another study found statistically and clinically significant improvement of symptoms at both doses [252]. Further, lurasidone treatment was linked to significant improvement in PANSS total scores [253]. Similarly, daily administration of 40–120 mg lurasidone for up to 24 months shows sustained improvement in PANSS total scores [254]. In general, lurasidone is well-tolerated with limited impact on weight gain and metabolism [252,253,255].
10.5. Clozapine
Clozapine may be a useful option for controlling symptoms in patients with first-episode schizophrenia who have not previously received treatment [256,257,258]. Clozapine is an antagonist of dopamine D2 and serotonin 5-HT2 receptors [259,260]. The drug was the first antipsychotic to show efficacy in treatment-resistant schizophrenia and shows the lowest risk of mortality [259,260,261]. A study of 36 patients indicated improved cognitive function after six months of clozapine treatment, particularly for verbal fluency and attention [262]. These effects on cognition suggest that clozapine may improve quality of life and vocational function in patients with schizophrenia [263]. Further, no significant increases were observed in plasma TBARS levels following clozapine use [264]. Finally, 100 patients with chronic schizophrenia received clozapine or risperidone as treatment [265]. Compared to risperidone, clozapine had significantly greater antioxidant effects via decreasing lipid peroxidation and increasing SOD and glutathione levels [265]. These antioxidant properties suggest that clozapine might be useful in managing negative symptoms [265,266].
10.6. Chlorpromazine
11. Role of Cognitive Therapies
Nutritional and pharmacological treatment alone may be insufficient for managing all symptoms of schizophrenia, particularly negative symptoms [273]. Cognitive behavioral therapy (CBT) for psychosis is recommended alongside antipsychotics for managing schizophrenia [274,275,276]. CBT shows efficacy for lessening positive and negative symptoms over a 9-month timeframe in patients with medication-resistant schizophrenia [274,275,276]. CBT was also found effective in a study of 90 patients with schizophrenia for reducing disorganized behavior that disrupts daily routine and function [277]. CBT for patients with schizophrenia additionally decreases violent behavior, substance abuse, and suicidal ideation, while promoting physical exercise, and participation in the community [274].
Cognitive Enhancement Therapy (CET) focuses on cognitive deficits in schizophrenia, through rehabilitating cognition [278]. A study of 58 early course patients with schizophrenia over two years found CET effective [279]. CET also improves retention of employment during the early phases of schizophrenia by promoting functional recovery [279].
12. Role of Quality of Life
People with schizophrenia typically exhibit a poor quality of life due to their dysfunctional psychological state and lifestyle circumstances [280]. Significant issues facing people with the condition include homelessness, lack of access to medical care, poor social skills, low socioeconomic status, and unemployment [274]. Patients with schizophrenia, starting from onset, generally have low-quality diets, and nutritional deficiencies [152,281]. A factor that might partially explain this observation is that people with low socioeconomic status are eight times more likely to develop schizophrenia than people with higher socioeconomic status [282]. Moreover, nutritional deficiencies are identified as risk factors for psychiatric disorders [283]. Patients were more likely to have an irregular eating schedule, eat instant meals, and drink more coffee than controls in a study of 194 subjects [284]. People with schizophrenia also smoke four more cigarettes per day on average than controls [284]. Finally, a study of 159 patients with schizophrenia found 41% did not eat fruit daily, 51% ate meals in less than fifteen minutes, and 63% did not consume fish [285]. Inadequacies in diet and exercise associated with schizophrenia may partially be due to the disorder’s impact on socioeconomic status as many patients with schizophrenia are unable to obtain and sustain employment [286].
13. Implications
Pharmaceutical treatment of schizophrenia is currently limited to only a few antipsychotic medications. Notwithstanding the proven efficacy of these antipsychotics, general outcomes in schizophrenia are far from optimal. As antipsychotic drug treatment has yet to provide suitable functional recovery, there remains a need to adopt complementary approaches to treating the disorder. Therefore, adjunctive treatment options that have proven useful in schizophrenia, such as antioxidant intake, are highly desirable. The current evidence on the effects of OS in schizophrenia pathophysiology support antioxidants as a potential therapeutic strategy for this disorder.
14. Conclusions
Schizophrenia is unquestionably an extremely distressing brain disorder. It leads to a number of behavioral and neurodevelopmental abnormalities, including deficiencies in social functioning, perception, and processing emotions. The evidence reviewed here suggests that OS is a key component of schizophrenia’s pathophysiology, likely as a result of an imbalance between prooxidant and antioxidant molecules within cells and tissues. Evidence also suggests this imbalance is not the result of antipsychotic drug use; in some cases, antipsychotic medications have been implicated to reduce oxidative stress. Moreover, cell damage and OS are most typically present in the early stages of schizophrenia; thus, preemptive treatment with specific diets and nutritional supplements could help arrest the progression and severity of the disorder. An important consideration to a nutraceutical approach is that many schizophrenia patients have poor dietary habits, in part due to socioeconomic factors such as homelessness or unemployment. While many antioxidant treatments have been reported as efficacious in improving the psychopathology of schizophrenia, vitamins B, C, D, and E, as well as omega-3 PUFA, have perhaps emerged as the most promising complementary schizophrenia treatment strategies.
Author Contributions
S.M. (Samskruthi Madireddy) and S.M. (Sahithi Madireddy) have contributed equally; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ben-Azu, B.; Aderibigbe, A.O.; Ajayi, A.M.; Iwalewa, E.O. Neuroprotective effects of the ethanol stem bark extracts of Terminalia ivorensis in ketamine–induced schizophrenia-like behaviors and oxidative damage in mice. Pharm. Biol. 2016, 54, 2871–2879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, W.; Silva, C.E.B.; Mohammadzai, I.U.; da Rocha, J.B.T.; Landeira-Fernandez, J. Association of oxidative stress to the genesis of anxiety: Implications for possible therapeutic interventions. Curr. Neuropharmacol. 2014, 12, 120–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taysi, S.; Tascan, A.S.; Ugur, M.G.; Demir, M. Radicals, oxidative/nitrosative stress and preeclampsia. Mini Rev. Med. Chem. 2019, 19, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Nagano, T.; Mizuno, M.; Morita, K.; Nawa, H. Pathological implications of oxidative stress in patients and animal models with schizophrenia: The role of epidermal growth factor receptor signaling. Curr. Top. Behav. Neurosci. 2016, 29, 429–446. [Google Scholar]
- Gonzalez-Liencres, C.; Tas, C.; Brown, E.C.; Erdin, S.; Onur, E.; Cubukcoglu, Z.; Aydemir, O.; Aysen Esen-Danaci, A.; Brüne, M. Oxidative stress in schizophrenia: A case–control study on the effects on social cognition and neurocognition. BMC Psychiatry 2014, 14, 268. [Google Scholar] [CrossRef] [Green Version]
- Bitanihirwe, B.K.Y.; Tsung-Ung, W.; Woo, T.W. Oxidative stress in schizophrenia: An integrated approach. Neurosci. Biobehav. Rev. 2011, 35, 878–893. [Google Scholar] [CrossRef] [Green Version]
- Ciobica, A.; Padurariu, M.; Dobrin, I.; Stefanescu, C.; Dobrin, R. Oxidative stress in schizophrenia—Focusing on the main markers. Psychiatr. Danub. 2011, 23, 237–245. [Google Scholar]
- Liu, Z.; Ren, Z.; Zhang, J.; Chuang, C.C.; Kandaswamy, E.; Zhou, T.; Zuo, L. Role of ROS and nutritional antioxidants in human diseases. Front. Physiol. 2018, 9, 477. [Google Scholar] [CrossRef] [Green Version]
- Dean, O.M.; van den Buuse, M.; Bush, A.I.; Copolov, D.L.; Ng, F.; Dodd, S.; Berk, M. A role for glutathione in the pathophysiology of bipolar disorder and schizophrenia? Animal models and relevance to clinical practice. Curr. Med. Chem. 2009, 16, 2965–2976. [Google Scholar] [CrossRef]
- Magalhães, P.V.S.; Dean, O.; Andreazza, A.C.; Berk, M.; Kapczinski, F. Antioxidant treatments for schizophrenia. Cochrane Database Syst. Rev. 2016, 2, CD008919. [Google Scholar] [CrossRef] [Green Version]
- Wadhwa, R.; Gupta, R.; Maurya, P.K. Oxidative stress and accelerated aging in neurodegenerative and neuropsychiatric disorder. Curr. Pharm. Des. 2018, 24, 4711–4725. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.J.; Yücel, M.; Pantelis, C.; Berk, M. Neurobiology of schizophrenia spectrum disorders: The role of oxidative stress. Ann. Acad. Med. 2009, 38, 396–401. [Google Scholar]
- Bahceci, B.; Kokacya, M.H.; Copoglu, U.S.; Bahceci, I.; Sahin, K.; Bagcioglu, E.; Dokuyucu, R. Elevated nucleosome level and oxidative stress in schizophrenia patients. Bratisl Lek Listy 2015, 116, 587–590. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.; Peng, C.; Sun, L.; Li, J.; Qing, Y.; Hu, X.; Yang, X.; Li, Y.; Xu, C.; Zhang, J.; et al. Leukocyte proteomic profiling in first–episode schizophrenia patients: Does oxidative stress play central roles in the pathophysiology network of schizophrenia? Antioxid. Redox Sign. 2019, 31, 579–588. [Google Scholar] [CrossRef]
- Madireddy, S.; Madireddy, S. Protection from the pathogenesis of neurodegenerative disorders, including alzheimer’s disease, amyotrophic lateral sclerosis, Huntington’s disease, and Parkinson’s diseases, through the mitigation of reactive oxygen species. J. Neurosci. Neurol. Disord. 2019, 3, 148–161. [Google Scholar] [CrossRef] [Green Version]
- Ng, F.; Berk, M.; Dean, O.; Bush, A.I. Oxidative stress in psychiatric disorders: Evidence base and therapeutic implications. Int. J. Neuropsychopharmacol. 2008, 11, 851–876. [Google Scholar] [CrossRef] [Green Version]
- Porokhovnik, L.N.; Passekov, V.P.; Gorbachevskaya, N.L.; Sorokin, A.B.; Veiko, N.N.; Lyapunova, N.A. Active ribosomal genes, translational homeostasis and oxidative stress in the pathogenesis of schizophrenia and autism. Psychiatr. Genet. 2015, 25, 79–87. [Google Scholar] [CrossRef]
- Alhadidi, M.M.; Abdullah, K.L.; Yoong, T.L.; Hadid, L.A.; Danaee, M. A systematic review of randomized controlled trials of psychoeducation interventions for patients diagnosed with schizophrenia. Int. J. Soc. Psychiatry 2020, 66, 542–552. [Google Scholar] [CrossRef]
- Bošković, M.; Grabnar, I.; Terzič, T.; Plesničar, B.K.; Vovk, T. Oxidative stress in schizophrenia patients treated with long–acting haloperidol decanoate. Psychiatry Res. 2013, 210, 761–768. [Google Scholar] [CrossRef]
- Huang, D.; Liu, S. Oxidative stress and schizophrenia. J. Psychiatry Brain Sci. 2017, 2, 4. [Google Scholar]
- Rodríguez, B.; Nani, J.V.; Almeida, P.G.C.; Brietzke, E.; Lee, R.S.; Hayashi, M.A.F. Neuropeptides and oligopeptidases in schizophrenia. Neurosci. Biobehav. Rev. 2020, 108, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.K.; Keshavan, M.S. Antioxidants, redox signaling, and pathophysiology in schizophrenia: An integrative view. Antioxid. Redox Sign. 2011, 15, 2011–2035. [Google Scholar] [CrossRef] [PubMed]
- Güneş, M.; Camkurt, M.A.; Bulut, M.; Demir, S.; İbiloğlu, A.O.; Kaya, M.C.; Atl, A.; Kaplan, I.; Sir, A. Evaluation of paraoxonase, arylesterase and malondialdehyde levels in schizophrenia patients taking typical, atypical and combined antipsychotic treatment. Clin. Psychopharma. Neurosci. 2016, 14, 345–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collin, F.; Cheignon, C.; Hureau, C. Oxidative stress as a biomarker for alzheimer’s disease. Biomark. Med. 2018, 12, 201–203. [Google Scholar] [CrossRef]
- Firth, J.; Teasdale, S.B.; Allott, K.; Siskind, D.; Marx, W.; Cotter, J.; Veronese, N.; Schuch, F.; Smith, L.; Solmi, M.; et al. The efficacy and safety of nutrient supplements in the treatment of mental disorders: A meta–review of meta–analyses of randomized controlled trials. World Psychiatry 2019, 18, 308–324. [Google Scholar] [CrossRef] [Green Version]
- Do, K.Q.; Conus, P.; Cuenod, M. Redox dysregulation and oxidative stress in schizophrenia: Nutrigenetics as a challenge in psychiatric disease prevention. In Personalized Nutrition; Simopoulos, A.P., Milner, J.A., Eds.; Karger: Basel, Switzerland, 2010; Volume 101, pp. 131–153. [Google Scholar]
- Jaaro-Peled, H.; Sawa, A. Neurodevelopmental factors in schizophrenia. Psychiatr. Clin. 2020, 43, 263–274. [Google Scholar] [CrossRef]
- Lin, C.-H.; Lane, H.-Y. Early identification and intervention of schizophrenia: Insight from hypotheses of glutamate dysfunction and oxidative stress. Front. Psychiatry 2019, 10, 93. [Google Scholar] [CrossRef]
- Panahi, Y.; Rajaee, S.M.; Johnston, T.P.; Sahebkar, A. Neuroprotective effects of antioxidants in the management of neurodegenerative disorders: A literature review. J. Cell. Biochem. 2019, 120, 2742–2748. [Google Scholar] [CrossRef]
- Do, K.Q.; Cuenod, M.; Hensch, T.K. Targeting Oxidative stress and aberrant critical period plasticity in the developmental trajectory to schizophrenia. Schizophr. Bull. 2015, 41, 835–846. [Google Scholar] [CrossRef]
- Harvey, P.D.; Isner, E.C. Cognition, social cognition, and functional capacity in early—Onset schizophrenia. Child Adolesc. Psychiatr. Clin. 2020, 29, 171–182. [Google Scholar] [CrossRef]
- Zanelli, J.; Mollon, J.; Sandin, S.; Morgan, C.; Dazzan, P.; Pilecka, I.; Marques, T.R.; David, A.; Morgan, K.D.; Fearon, P.; et al. Cognitive change in schizophrenia and other psychoses in the decade following the first episode. Am. J. Psychiatry 2019, 176, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Chowdari, K.V.; Bamne, M.N.; Nimgaonkar, V.L. Genetic association studies of antioxidant pathway genes and schizophrenia. Antioxid. Redox Sign. 2011, 15, 2037–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, E.K.; Drago, A. A molecular pathway analysis stresses the role of inflammation and oxidative stress towards cognition in schizophrenia. J. Neural Transm. 2017, 124, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Zugno, A.I.; Canever, L.; Heylmann, A.S.; Wessler, P.G.; Steckert, A.; Mastella, G.A.; de Oliveira, M.B.; Damázio, L.S.; Pachec, F.D.; Calixto, O.P.; et al. Effect of folic acid on oxidative stress and behavioral changes in the animal model of schizophrenia induced by ketamine. J. Psychiatr. Res. 2016, 81, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Hamazaki, K.; Maekawa, M.; Toyota, T.; Dean, B.; Hamazaki, T.; Yoshikawa, T. Fatty acid composition of the postmortem corpus callosum of patients with schizophrenia, bipolar disorder, or major depressive disorder. Eur. Psychiatry 2017, 39, 51–56. [Google Scholar] [CrossRef] [PubMed]
- van Erp, T.G.; Hibar, D.P.; Rasmussen, J.M.; Glahn, D.C.; Pearlson, G.D.; Andreassen, O.A.; Agartz, I.; Westlye, L.T.; Haukvik, U.K.; Dale, A.M.; et al. Subcortical brain volume abnormalities in 2028 individuals with schizophrenia and 2540 healthy controls via the ENIGMA consortium. Mol. Psychiatry 2016, 21, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Gourion, D.; Gourevitch, R.; Leprovost, J.B.; Olié, H.; Lôo, J.P.; Krebs, M.O. Neurodevelopmental hypothesis in schizophrenia. Encephale 2004, 30, 109–118. [Google Scholar] [CrossRef]
- Guessoum, S.B.; Le Strat, Y.; Dubertret, C.; Mallet, J. A transnosographic approach of negative symptoms pathophysiology in schizophrenia and depressive disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 99, 109862. [Google Scholar] [CrossRef]
- Bulbul, F.; Virit, O.; Alpak, G.; Unal, A.; Bulut, M.; Kaya, M.C.; Altindag, A.; Celik, H.; Savas, H.A. Are oxidative stress markers useful to distinguish schizoaffective disorder from schizophrenia and bipolar disorder? Acta Neuropsychiatr. 2014, 26, 120–124. [Google Scholar] [CrossRef]
- Gainsford, K.; Fitzgibbon, B.; Fitzgerald, P.B.; Hoy, K.E. Transforming treatments for schizophrenia: Virtual reality, brain stimulation and social cognition. Psychiatry Res. 2020, 288, 112974. [Google Scholar] [CrossRef]
- Humpston, C.S.; Broome, M.R. Thinking, believing, and hallucinating self in schizophrenia. Lancet Psychiatry 2020, 7, 638–646. [Google Scholar] [CrossRef]
- Khandaker, G.M.; Dantzer, R. Is there a role for immune–to–brain communication in schizophrenia? Psychopharmacology 2016, 233, 1559–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khavari, B.; Cairns, M.J. Epigenomic dysregulation in schizophrenia: In search of disease etiology and biomarkers. Cells 2020, 9, 1837. [Google Scholar] [CrossRef] [PubMed]
- Smeland, O.B.; Frei, O.; Dale, A.M.; Andreassen, O.A. The polygenic architecture of schizophrenia—Rethinking pathogenesis and nosology. Nat. Rev. Neurol. 2020, 16, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Schooler, N.R. Negative symptoms in schizophrenia: A review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [Green Version]
- Krug, A.; Stein, F.; Kircher, T. Cognitive disorders in schizophrenia. Nervenarzt 2020, 91, 2–9. [Google Scholar] [CrossRef]
- Pu, S.; Nakagome, K.; Itakura, M.; Iwata, M.; Nagata, I.; Kaneko, K. The association between cognitive deficits and prefrontal hemodynamic responses during performance of working memory task in patients with schizophrenia. Schizophr. Res. 2016, 172, 114–122. [Google Scholar] [CrossRef]
- Wright, S.; Kochunov, P.; Chiappelli, J.; McMahon, R.; Muellerklein, F.; Wijtenburg, S.A.; White, M.G.; Rowland, L.M.; Hong, E. Accelerated white matter aging in schizophrenia: Role of white matter blood perfusion. Neurobiol. Aging 2014, 35, 2411–2418. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.H.; Kim, J.E.; Rhie, S.J.; Yoon, S. The role of oxidative stress in neurodegenerative diseases. Exp. Neurobiol. 2015, 24, 325–340. [Google Scholar] [CrossRef]
- Salim, S. Oxidative stress and the central nervous system. J. Pharmacol. Exp. Ther. 2017, 360, 201–205. [Google Scholar] [CrossRef]
- Sbodio, J.I.; Snyder, S.H.; Paul, B.D. Redox mechanisms in neurodegeneration: From disease outcomes to therapeutic opportunities. Antioxid. Redox Sign. 2019, 30, 1450–1499. [Google Scholar] [CrossRef] [PubMed]
- Newsholme, P.; Cruzat, V.F.; Keane, K.N.; Carlessi, R.; de Bittencourt, P.I.H. Molecular mechanisms of ROS production and oxidative stress in diabetes. Biochem. J. 2016, 473, 4527–4550. [Google Scholar] [CrossRef] [PubMed]
- Okusaga, O.O. Accelerated aging in schizophrenia patients: The potential role of oxidative stress. Aging Dis. 2014, 5, 256–262. [Google Scholar] [PubMed]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative stress: Harms and benefits for human health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Wang, Z.; Cao, J.; Chen, Y.; Dong, Y. A novel and compact review on the role of oxidative stress in female reproduction. Reprod. Biol. Endocrinol. 2018, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- Nita, M.; Grzybowski, A. The role of the reactive oxygen species and oxidative stress in the pathomechanism of the age-related ocular diseases and other pathologies of the anterior and posterior eye segments in adults. Oxid. Med. Cell. Longev. 2016, 2016, 3164734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collin, F. Chemical basis of reactive oxygen species reactivity and involvement in neurodegenerative diseases. Int. J. Mol. Sci. 2019, 20, 2407. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, T.; Muraoka, I. Exercise–induced oxidative stress and the effects of antioxidant intake from a physiological viewpoint. Antioxidants 2018, 7, 119. [Google Scholar] [CrossRef] [Green Version]
- Rahal, A.; Kumar, A.; Singh, V.; Yadav, B.; Tiwari, R.; Chakraborty, S.; Chakraborty, S.; Dhama, K. Oxidative stress, prooxidants, and antioxidants: The interplay. BioMed Res. Int. 2014, 2014, 761264. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Kukreti, R.; Saso, L.; Kukreti, S. Oxidative stress: A key modulator in neurodegenerative diseases. Molecules 2019, 24, 1583. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Branicky, R.; Noë, A.; Hekimi, S. Superoxide dismutases: Dual roles in controlling ROS damage and regulating ROS signaling. J. Cell. Biol. 2018, 217, 1915–1928. [Google Scholar] [CrossRef] [PubMed]
- Zorov, D.B.; Juhaszova, M.; Sollott, S.J. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiol. Rev. 2014, 94, 909–950. [Google Scholar] [CrossRef] [Green Version]
- Bolisetty, S.; Jaimes, E.A. Mitochondria and reactive oxygen species: Physiology and pathophysiology. Int. J. Mol. Sci. 2013, 14, 6306–6344. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Roychoudhury, A. Reactive oxygen species (ROS) and response of antioxidants as ROS-scavengers during environmental stress in plants. Front. Environ. Sci. 2014, 2, 53. [Google Scholar] [CrossRef] [Green Version]
- Bai, Z.; Li, X.; Chen, G.; Du, Y.; Wei, Z.; Chen, X.; Zheng, G.; Deng, W.; Cheng, Y. Serum oxidative stress marker levels in unmedicated and medicated patients with schizophrenia. J. Mol. Neurosci. 2018, 66, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Chittiprol, S.; Venkatasubramanian, G.; Neelakantachar, N.; Babu, S.V.; Reddy, N.A.; Shetty, K.T.; Gangadhar, B.N. Oxidative stress and neopterin abnormalities in schizophrenia: A longitudinal study. J. Psychiatr. Res. 2010, 44, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Sarandol, A.; Kirli, S.; Akkaya, C.; Altin, A.; Demirci, M.; Sarandol, E. Oxidative–antioxidative systems and their relation with serum S100 B levels in patients with schizophrenia: Effects of short term antipsychotic treatment. Prog. Neuro–Psychopharmacol. Biol. Psychiatry 2007, 31, 1164–1169. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Arellano, L.; González-García, N.; Salazar-García, M.; Corona, J.C. Antioxidants as a potential target against inflammation and oxidative stress in attention-deficit/hyperactivity disorder. Antioxidants 2020, 9, 176. [Google Scholar] [CrossRef] [Green Version]
- Leza, J.C.; García–Bueno, B.; Bioque, M.; Arango, C.; Parellada, M.; Do, K.; O’Donnell, P.; Bernardo, M. Inflammation in schizophrenia: A question of balance. Neurosci. Biobehav. Rev. 2015, 55, 612–626. [Google Scholar] [CrossRef]
- Muller, N. Inflammation in schizophrenia: Pathogenetic aspects and therapeutic considerations. Schizophr. Bull. 2018, 44, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Mehta, V.; Desai, N.; Perwez, A.; Nemade, D.; Dawoodi, S.; Zaman, S.B. ACE alzheimer’s: The role of vitamin A, C and E (ACE) in oxidative stress induced alzheimer’s disease. J. Med. Res. Innov. 2018, 2. [Google Scholar] [CrossRef]
- Sharma, P.; Jha, A.B.; Dubey, R.S.; Pessarakli, M. Reactive oxygen species, oxidative damage, and antioxidative defense mechanism in plants under stressful conditions. J. Bot. 2012, 2012, 217037. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; You, Y.; Yu, L.; Yao, L.; Lu, H.; Zhou, X.; Wu, S.; Chen, L.; Chen, Y.; Zhao, X. Uric acid levels in subjects with schizophrenia: A systematic review and meta-analysis. Psychiatry Res. 2020, 292, 113305. [Google Scholar] [CrossRef]
- Dietrich-Muszalska, A.; Kolińska-Łukaszuk, J. Comparative effects of aripiprazole and selected antipsychotic drugs on lipid peroxidation in plasma. Psychiatry Clin. Neurosci. 2018, 72, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Forni, C.; Facchiano, F.; Bartoli, M.; Pieretti, S.; Facchiano, A.; D’Arcangelo, D.; Norelli, S.; Valle, G.; Nisini, R.; Beninati, S.; et al. Beneficial role of phytochemicals on oxidative stress and age-related diseases. BioMed Res. Int. 2019, 2019, 8748253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jha, S.K.; Jha, N.K.; Kumar, D.; Ambasta, R.K.; Kumar, P. Linking mitochondrial dysfunction, metabolic syndrome and stress signaling in neurodegeneration. Mol. Basis Dis. 2017, 1863, 1132–1146. [Google Scholar] [CrossRef] [PubMed]
- Chandel, N.S. Mitochondria as signaling organelles. BMC Biol. 2014, 12, 34. [Google Scholar] [CrossRef]
- Wang, X.; Wang, W.; Lia, L.; Perry, G.; Lee, H.; Zhu, X. Oxidative stress and mitochondrial dysfunction in Alzheimer’s disease. Biochim. Biophys. Acta 2014, 1842, 1240–1247. [Google Scholar] [CrossRef] [Green Version]
- Idelchik, M.P.S.; Begley, U.; Begley, T.J.; Melendez, J.A. Mitochondrial ROS control of cancer. Semin. Cancer Biol. 2017, 47, 57–66. [Google Scholar] [CrossRef]
- Angelova, P.R.; Abramov, A.Y. Role of mitochondrial ROS in the brain: From physiology to neurodegeneration. FEBS Lett. 2018, 592, 692–702. [Google Scholar] [CrossRef]
- Akbar, M.; Essa, M.M.; Daradkeh, G.; Abdelmegeeda, M.A.; Choia, Y.; Mahmoodd, L.; Song, B. Mitochondrial dysfunction and cell death in neurodegenerative diseases through nitroxidative stress. Brain Res. 2016, 1637, 34–55. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.D.; Alvarez, L.A.; Zhang, X.; Soldati, T. Reactive oxygen species and mitochondria: A nexus of cellular homeostasis. Redox Biol. 2015, 6, 472–485. [Google Scholar] [CrossRef]
- Roberts, R.C. Postmortem studies on mitochondria in schizophrenia. Schizophr. Res. 2017, 187, 17–25. [Google Scholar] [CrossRef]
- An, H.; Du, X.; Huang, X.; Qi, L.; Jia, Q.; Yin, G.; Xiao, C.; Huang, X.; Ning, Y.; Cassidy, R.M.; et al. Obesity, altered oxidative stress, and clinical correlates in chronic schizophrenia patients. Transl. Psychiatry 2018, 8, 258. [Google Scholar] [CrossRef]
- Boll, K.M.; Noto, C.; Bonifácio, K.L.; Bortolasci, C.C.; Gadelha, A.; Bressan, R.A.; Barbosa, D.S.; Maes, M.; Moreira, E.G. Oxidative and nitrosative stress biomarkers in chronic schizophrenia. Psychiatry Res. 2017, 253, 43–48. [Google Scholar] [CrossRef]
- Fraguas, D.; Diaz-Caneja, C.M.; Ayora, M.; Hernandez-Alvarez, F.; Rodriguez-Quiroga, A.; Recio, S.; Leza, J.C.; Arango, C. Oxidative stress and inflammation in first–episode psychosis: A systematic review and meta-analysis. Schizophr. Bull. 2019, 45, 742–751. [Google Scholar] [CrossRef]
- Jordan, W.; Dobrowolny, H.; Bahn, S.; Bernstein, H.G.; Brigadski, T.; Frodl, T.; Isermann, B.; Lessmann, V.; Pilz, J.; Rodenbeck, A.; et al. Oxidative stress in drug–naïve first episode patients with schizophrenia and major depression: Effects of disease acuity and potential confounders. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Magaji, M.G.; Iniaghe, L.O.; Abolarin, M.; Abdullahi, O.I.; Magaji, R.A. Neurobehavioural evaluation of resveratrol in murine models of anxiety and schizophrenia. Metab. Brain Dis. 2017, 32, 437–442. [Google Scholar] [CrossRef]
- Steullet, P.; Cabungcal, J.; Coyle, J.; Didriksen, M.; Gill, K.; Grace, A.A.; Hensch, T.K.; LaMantia, A.-S.; Lindemann, L.; Maynard, T.M.; et al. Oxidative stress–driven parvalbumin interneuron impairment as a common mechanism in models of schizophrenia. Mol. Psychiatry 2017, 22, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.Q.; Kosten, T.R.; Zhang, X.Y. Free radicals, antioxidant defense systems, and schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 46, 200–206. [Google Scholar] [CrossRef]
- Mueller, T.M.; Meador-Woodruff, J.H. Post-translational protein modifications in schizophrenia. NPJ Schizophr. 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Conn, K.A.; Burne, T.H.J.; Kesby, J.P. Subcortical dopamine and cognition in schizophrenia: Looking beyond psychosis in preclinical models. Front. Neurosci. 2020, 14, 542. [Google Scholar] [CrossRef] [PubMed]
- González-Blanco, L.; García-Portilla, M.P.; García-Álvarez, L.; de la Fuente-Tomás, L.; García, C.I.; Sáiz, P.A. Oxidative stress biomarkers and clinical dimensions in first 10 years of schizophrenia. Rev. Psiquiatr. Salud Ment. 2018, 11, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Miljević, Č.D.; Nikolić-Kokić, A.; Blagojević, D.; Milovanović, M.; Munjiza, A.; Jukić, M.M.; Pešić, V.; Lečić-Toševski, D.; Spasić, M.B. Association between neurological soft signs and antioxidant enzyme activity in schizophrenic patients. Psychiatry Res. 2018, 269, 746–752. [Google Scholar] [CrossRef]
- Morera-Fumero, A.L.; Diaz-Mesa, E.; Abreu-Gonzalez, P.; Fernandez-Lopez, L.; Cejas-Mendez, M.D. Low levels of serum total antioxidant capacity and presence at admission and absence at discharge of a day/night change as a marker of acute paranoid schizophrenia relapse. Psychiatry Res. 2017, 249, 200–205. [Google Scholar] [CrossRef]
- Nucifora, L.G.; Tanaka, T.; Hayes, L.N.; Kim, M.; Lee, B.J.; Matsuda, T.; Nucifora, F.C.; Sedlak, T.; Mojtabai, R.; Eaton, W.; et al. Reduction of plasma glutathione in psychosis associated with schizophrenia and bipolar disorder in translational psychiatry. Transl. Psychiatry 2017, 7, e1215. [Google Scholar] [CrossRef] [Green Version]
- Tunçel, Ö.K.; Sarısoy, G.; Bilgici, B.; Pazvantoglu, O.; Çetin, E.; Ünverdi, E.; Avcı, B.; Böke, O. Oxidative stress in bipolar and schizophrenia patients. Psychiatry Res. 2015, 228, 688–694. [Google Scholar] [CrossRef]
- Zhang, Y.; Catts, V.S. Shannon Weickert, C. Lower antioxidant capacity in the prefrontal cortex of individuals with schizophrenia. Aust. N. Z. J. Psychiatry 2018, 52, 690–698. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Chen, D.-C.; Tan, Y.-L.; Tan, S.-P.; Wang, Z.-R.; Yang, F.-D.; Okusaga, O.O.; Zunta-Soares, G.B.; Soares, J.C. The interplay between BDNF and oxidative stress in chronic schizophrenia. Psychoneuroendocrinology 2015, 51, 201–208. [Google Scholar] [CrossRef]
- Devanarayanan, S.; Nandeesha, H.; Kattimani, S.; Sarkar, S. Relationship between matrix metalloproteinase–9 and oxidative stress in drug–free male schizophrenia: A case control study. Clin. Chem. Lab. Med. 2016, 54, 447–452. [Google Scholar] [CrossRef]
- Avval, F.Z.; Mahmoudi, N.; Tirkani, A.N.; Jarahi, L.; Alamdari, D.H.; Sadjadi, S.A. Determining pro–oxidant antioxidant balance (PAB) and total antioxidant capacity (TAC) in patients with schizophrenia. Iran. J. Psychiatry 2018, 13, 223–227. [Google Scholar]
- Zhang, M.; Zhao, Z.M.; He, L.; Wan, C. A meta–analysis of oxidative stress markers in schizophrenia. Sci. China Life Sci. 2010, 53, 112–124. [Google Scholar] [CrossRef]
- Martins-de-Souza, D.; Harris, L.W.; Guest, P.C.; Bahn, S. The role of energy metabolism dysfunction and oxidative stress in schizophrenia revealed by proteomics. Antioxid. Redox Sign. 2011, 15, 2067–2079. [Google Scholar] [CrossRef] [PubMed]
- Vidal, P.M.; Pacheco, R. The cross-talk between the dopaminergic and the immune system involved in schizophrenia. Front. Pharmacol. 2020, 11, 394. [Google Scholar] [CrossRef] [PubMed]
- Vidovic, B.; Milovanovi, S.; Dordevic, B.; Kotur-Stevuljevi, J.; Stefanovic, A.; Ivaniševic, J.; Miljković, M.; Spasić, S.; Stojanović, D.; Pantović, M. Effect of alpha-lipoic acid supplementation on oxidative stress markers and antioxidative defense in patients with schizophrenia. Psychiat. Danub. 2014, 26, 205–213. [Google Scholar]
- Kim, Y.; Na, K. Neuroprotection in schizophrenia and its therapeutic implications. Psychiatry Investig. 2017, 14, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Rajasekaran, A.; Venkatasubramanian, G.; Berk, M.; Debnath, M. Mitochondrial dysfunction in schizophrenia: Pathways, mechanisms and implications. Neurosci. Biobehav. Rev. 2015, 48, 10–21. [Google Scholar] [CrossRef]
- Marazziti, D.; Baroni, S.; Picchetti, M.; Landi, P.; Silvestri, S.; Vatteroni, E.; Dell’Osso, M.C. Psychiatric disorders and mitochondrial dysfunctions. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 270–275. [Google Scholar]
- Johri, A.; Beal, M.F. Antioxidants in Huntington’s disease. Biochim. Biophys. Acta 2012, 1822, 664–674. [Google Scholar] [CrossRef] [Green Version]
- Conus, P.; Seidman, L.J.; Fournier, M.; Xin, L.; Cleusix, M.; Baumann, P.S.; Ferrari, C.; Cousins, A.; Alameda, L.; Gholam-Rezaee, M.; et al. N-acetylcysteine in a double-blind randomized placebo-controlled trial: Toward biomarker-guided treatment in early psychosis. Schizophr. Bull. 2018, 44, 317–327. [Google Scholar] [CrossRef] [Green Version]
- Perkins, D.O.; Jeffries, C.D.; Addington, J.; Bearden, C.E.; Cadenhead, K.S.; Cannon, T.D.; Cornblatt, B.A.; Mathalon, D.H.; McGlashan, T.H.; Seidman, L.J.; et al. Toward a psychosis risk blood diagnostic for persons experiencing high–risk symptoms: Preliminary results from the NAPLS project. Schizophr. Bull. 2015, 41, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.Q.; Chen, D.C.; Tan, Y.L.; Tan, S.; Wang, Z.; Yang, F.; Soares, J.C.; Zhang, X.Y. Association of altered CuZn superoxide dismutase and cognitive impairment in schizophrenia patients with tardive dyskinesia. J. Psychiatr. Res. 2014, 58, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Flatow, J.; Buckley, P.; Miller, B.J. Meta-analysis of oxidative stress in schizophrenia. Biol. Psychiatry 2013, 74, 400–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich-Muszalska, A.; Olas, B.; Rabe-Jablonska, J. Oxidative stress in blood platelets from schizophrenic patients. Platelets 2005, 16, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Raffa, M.; Atig, F.; Mhalla, A.; Kerkeni, A.; Mechri, A. Decreased glutathione levels and impaired antioxidant enzyme activities in drug–naïve first–episode schizophrenic patients. BMC Psychiatry 2011, 11, 124. [Google Scholar] [CrossRef] [Green Version]
- Raffa, M.; Barhoumi, S.; Atig, F.; Fendri, C.; Kerkeni, A.; Mechri, A. Reduced antioxidant defense systems in schizophrenia and bipolar I disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 39, 371–375. [Google Scholar] [CrossRef]
- Yao, J.K.; Reddy, R. Oxidative Stress in Schizophrenia: Pathogenetic and Therapeutic Implications. Antioxid. Redox Sign. 2011, 15, 1999–2002. [Google Scholar] [CrossRef] [Green Version]
- Dadheech, G.; Mishra, S.; Gautam, S.; Sharma, P. Evaluation of antioxidant deficit in schizophrenia. Indian J. Psychiatry 2008, 50, 16–20. [Google Scholar]
- Dadheech, G.; Sharma, P.; Gautam, S. Oxidative stress–induced response of some endogenous antioxidants in schizophrenia. Indian J. Clin. Biochem. 2012, 27, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Perkins, D.O.; Jeffries, C.D.; Do, K.Q. Potential roles of redox dysregulation in the development of schizophrenia. Biol. Psychiatry 2020, 88, 326–336. [Google Scholar] [CrossRef]
- Federico, A.; Cardaioli, E.; da Pozzo, P.; Formichi, P.; Gallus, G.N.; Radi, E. Mitochondria, oxidative stress and neurodegeneration. J. Neurol. Sci. 2012, 322, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Zou, M.H. Roles of reactive oxygen species in physiology and pathology. In Atherosclerosis: Risks, Mechanisms, and Therapies; Wang, H., Patterson, C., Eds.; John Wiley & Sons Inc: Hoboken, NJ, USA, 2015; pp. 379–392. [Google Scholar] [CrossRef]
- Boskovic, M.; Vovk, T.; Plesnicar, B.K.; Grabnar, I. Oxidative stress in schizophrenia. Curr. Neuropharmacol. 2011, 9, 301–312. [Google Scholar] [PubMed] [Green Version]
- Upthegrove, R.; Khandaker, G.M. Cytokines, oxidative stress and cellular markers of inflammation in schizophrenia. Curr. Top. Behav. Neurosci. 2020, 44, 49–66. [Google Scholar] [PubMed]
- Barron, H.; Hafizi, S.; Andreazza, A.C.; Mizrahi, R. Neuroinflammation and oxidative stress in psychosis and psychosis risk. Int. J. Mol. Sci. 2017, 18, 651. [Google Scholar] [CrossRef] [Green Version]
- Carocci, A.; Catalano, A.; Sinicropi, M.S.; Genchi, G. Oxidative stress and neurodegeneration: The involvement of iron. BioMetals 2018, 31, 715–735. [Google Scholar] [CrossRef]
- Tan, S.H.; Karri, V.; Tay, N.W.R.; Chang, K.H.; Ah, H.Y.; Ng, P.Q.; Ho, H.S.; Keh, H.W.; Candasamy, M. Emerging pathways to neurodegeneration: Dissecting the critical molecular mechanisms in alzheimer’s disease, Parkinson’s disease. Biomed. Pharmacother. 2019, 111, 765–777. [Google Scholar] [CrossRef]
- Yao, J.K.; Leonard, S.; Reddy, R.D. Increased nitric oxide radicals in postmortem brain from patients with schizophrenia. Schizophr. Bull. 2004, 30, 923–934. [Google Scholar] [CrossRef] [Green Version]
- Dadheech, G.; Mishra, S.; Gautam, S.; Sharma, P. Oxidative stress, α-tocopherol, ascorbic acid and reduced glutathione status in schizophrenics. Indian J. Clin. Biochem. 2006, 21, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Maas, D.A.; Vallès, A.; Martens, G.J.M. Oxidative stress, prefrontal cortex hypomyelination and cognitive symptoms in schizophrenia. Transl. Psychiatry 2017, 7, e1171. [Google Scholar] [CrossRef] [Green Version]
- Mhillaj, E.; Morgese, M.G.; Trabace, L. Early life and oxidative stress in psychiatric disorders: What can we learn from animal models? Curr. Pharm. Des. 2015, 21, 396–403. [Google Scholar] [CrossRef]
- Young, J.; McKinney, S.B.; Ross, B.M.; Wahle, K.W.; Boyle, S.P. Biomarkers of oxidative stress in schizophrenic and control subjects. Prostaglandins Leukot. Essent. Fatty Acids 2007, 76, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Sertan Copoglu, U.; Virit, O.; Hanifi Kokacya, M.; Orkmez, M.; Bulbul, F.; Binnur Erbagci, A.; Semiz, M.; Alpak, G.; Unal, A.; Ari, M.; et al. Increased oxidative stress and oxidative DNA damage in non–remission schizophrenia patients. Psychiatry Res. 2015, 229, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Kilic, O.H.T.; Aksoy, I.; Elboga, G.C.; Bulbul, F. Oxidative parameters, oxidative DNA damage, and urotensin–II in schizoaffective disorder patients. Psychiatry Clin. Psychopharmacol. 2019, 29, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Li, H.C.; Chen, Q.Z.; Ma, Y.; Zhou, J. Imbalanced free radicals and antioxidant defense systems in schizophrenia: A comparative study. J. Zhejiang Univ. Sci. B 2006, 7, 981–986. [Google Scholar]
- Virit, O.; Altindag, A.; Yumru, M.; Dalkilic, A.; Savas, H.A.; Selek, S.; Erel, O.; Herken, H. A defect in the antioxidant defense system in schizophrenia. Neuropsychobiology 2009, 60, 87–93. [Google Scholar] [CrossRef]
- Bjorklund, G.; Chirumbolo, S. Role of oxidative stress and antioxidants in daily nutrition and human health. Nutrition 2017, 33, 311–321. [Google Scholar] [CrossRef]
- Firth, J.; Stubbs, B.; Sarris, J.; Rosenbaum, S.; Teasdale, S.; Berk, M.; Yung, A.R. The effects of vitamin and mineral supplementation on symptoms of schizophrenia: A systematic review and meta-analysis. Psychol. Med. 2017, 47, 1515–1527. [Google Scholar] [CrossRef] [Green Version]
- Visioli, F.; Burgos-Ramos, E. Selected micronutrients in cognitive decline prevention and therapy. Mol. Neurobiol. 2016, 53, 4083–4093. [Google Scholar] [CrossRef]
- Tsai, M.C.; Liou, C.W.; Lin, T.K.; Lin, I.M.; Huang, T.L. Changes in oxidative stress markers in patients with schizophrenia: The effect of antipsychotic drugs. Psychiatry Res. 2013, 209, 284–290. [Google Scholar] [CrossRef]
- D’Souza, B.; D’Souza, V. Oxidative injury and antioxidant vitamins E and C in schizophrenia. Indian J. Clin. Biochem. 2003, 18, 87–90. [Google Scholar] [CrossRef] [Green Version]
- Arvindakshan, M.; Ghate, M.; Ranjekar, P.K.; Evans, D.R.; Mahadik, S.P. Supplementation with a combination of omega 3 fatty acids and antioxidants (vitamin E and C) improves the outcome of schizophrenia. Schizophr. Res. 2003, 62, 195–204. [Google Scholar] [CrossRef]
- Albayrak, Y.; Ünsal, C.; Beyazyüz, M.; Ünal, A.; Kuloğlu, M. Reduced total antioxidant level and increased oxidative stress in patients with deficit schizophrenia: A preliminary study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 45, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Natarajan, R.; Ziedonis, D.; Fan, X. Antioxidant and anti–inflammatory nutrient status, supplementation, and mechanisms in patients with schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 78, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Solberg, D.K.; Refsum, H.; Andreassen, O.A.; Bentsen, H. A five-year follow-up study of antioxidants, oxidative stress and polyunsaturated fatty acids in schizophrenia. Acta Neuropsychiatr. 2019, 31, 202–212. [Google Scholar] [CrossRef]
- Fond, G.; Lançon, C.; Korchia, T.; Auquier, P.; Boyer, L. The role of inflammation in the treatment of schizophrenia. Front. Psychiatry 2020, 11, 160. [Google Scholar] [CrossRef] [Green Version]
- Reyazuddin, M.; Azmi, S.A.; Islam, N.; Rizvi, A. Oxidative stress and level of antioxidant enzymes in drug-naive schizophrenics. Indian J. Psychiatry 2014, 56, 344–349. [Google Scholar]
- Kaplan, B.J.; Rucklidge, J.J.; Romijn, A.; McLeod, K. The emerging field of nutritional mental health inflammation, the microbiome, oxidative stress, and mitochondrial function. Clin. Psychol. Sci. 2015, 3, 964–980. [Google Scholar] [CrossRef] [Green Version]
- Rucklidge, J.J.; Kaplan, B.J. Broad-spectrum micronutrient formulas for the treatment of psychiatric symptoms: A systematic review. Expert Rev. Neurother. 2013, 13, 49–73. [Google Scholar] [CrossRef]
- Basambombo, L.L.; Carmichael, P.H.; Cote, S.; Laurin, D. Use of vitamin E and C supplements for the prevention of cognitive decline. Ann. Pharmacother. 2017, 51, 118–124. [Google Scholar] [CrossRef]
- Dipasquale, S.; Pariante, C.M.; Dazzan, P.; Aguglia, E.; McGuire, P.; Mondelli, V. The dietary pattern of patients with schizophrenia: A systematic review. J. Psychiatr. Res. 2013, 47, 197–207. [Google Scholar] [CrossRef] [Green Version]
- Heald, A.; Sein, K.; Anderson, S.; Pendlebury, J.; Guy, M.; Narayan, V.; Gibson, M.; Haddad, P.; Livingston, M. Diet, exercise and the metabolic syndrome in schizophrenia: A cross–sectional study. Schizophr. Res. 2015, 169, 494–495. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J.; Murphy, J.; Mischoulon, D.; Papakostas, G.I.; Fava, M.; Berk, M.; Ng, C.H. Adjunctive nutraceuticals for depression: A systematic review and meta–analyses. Am. J. Psychiatry 2016, 173, 575–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghodake, S.R.; Suryakar, A.N.; Padalkar, R.K. The possible role of oxidants and antioxidant imbalance in pathophysiology of schizophrenia. Int. J. Med. Res. Health Sci. 2012, 2, 19–35. [Google Scholar]
- Reddy, R.; Reddy, R. Antioxidant therapeutics for schizophrenia. Antioxid. Redox Sign. 2011, 15, 2047–2055. [Google Scholar] [CrossRef]
- Taghizadeh, M.; Tamtaji, O.R.; Dadgostar, E.; Kakhaki, R.D.; Bahmani, F.; Abolhassani, J.; Aarabi, M.H.; Kouchaki, E.; Memarzadeh, M.R.; Asemi, Z. The effects of omega-3 fatty acids and vitamin E co-supplementation on clinical and metabolic status in patients with Parkinson’s disease: A randomized, double-blind, placebo-controlled trial. Neurochem. Int. 2017, 108, 183–189. [Google Scholar] [CrossRef]
- Trotta, E.; Bortolotti, S.; Fugazzotto, G.; Gellera, C.; Montagnese, S.; Amodio, P. Familial vitamin E deficiency: Multiorgan complications support the adverse role of oxidative stress. Nutrition 2019, 63–64, 57–60. [Google Scholar] [CrossRef]
- Ulatowski, L.M.; Manor, D. Vitamin E and neurodegeneration. Neurobiol. Dis. 2015, 84, 78–83. [Google Scholar] [CrossRef]
- Koga, M.; Serritella, A.V.; Sawa, A.; Sedlak, T.W. Implications for reactive oxygen species in schizophrenia pathogenesis. Schizophr. Res. 2016, 176, 52–71. [Google Scholar] [CrossRef]
- Arroll, M.A.; Wilder, L.; Neil, J. Nutritional interventions for the adjunctive treatment of schizophrenia: A brief review. Nutr. J. 2014, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Soares-Weiser, K.; Maayan, N.; McGrath, J. Vitamin E for neuroleptic-induced tardive dyskinesia. Cochrane Database Syst. Rev. 2011, 2, CD000209. [Google Scholar] [CrossRef] [Green Version]
- Bošković, M.; Vovk, T.; Koprivšek, J.; Plesnicar, B.K.; Grabnar, I. Vitamin E and essential polyunsaturated fatty acids supplementation in schizophrenia patients treated with haloperidol. Nutr. Neurosci. 2016, 19. [Google Scholar] [CrossRef] [PubMed]
- Eckert, G.P. The role of vitamin E in aging and alzheimer’s disease. In Vitamin E in Human Health; Weber, P., Birringer, M., Blumberg, J., Eggersdorfer, M., Frank, J., Eds.; Nutrition and Health. Humana Press: Cham, Switzerland, 2019; pp. 325–344. [Google Scholar]
- Grimm, M.O.W.; Mett, J.; Hartmann, T. The impact of vitamin E and other fat-soluble vitamins on alzheimer’s disease. Int. J. Mol. Sci. 2016, 17, 1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schirinzi, T.; Martella, G.; Imbriani, P.; Lazzaro, G.D.; Franco, D.; Colona, V.L.; Alwardat, M.; Salimei, P.S.; Mercuri, N.B.; Pierantozzi, M.; et al. Dietary vitamin E as a protective factor for Parkinson’s disease: Clinical and experimental evidence. Front. Neurol. 2019, 10, 148. [Google Scholar] [CrossRef] [Green Version]
- Kocot, J.; Luchowska-Kocot, D.; Kiełczykowska, M.; Musik, I.; Kurzepa, J. Does vitamin C influence neurodegenerative diseases and psychiatric disorders? Nutrients 2017, 9, 659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Q.-Q.; Shen, T.-T.; Wang, F.; Wu, P.-F.; Chen, J.-G. Preventive and therapeutic potential of vitamin C in mental disorders. Curr. Med. Sci. 2018, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Harrison, F.E. A critical review of vitamin C for the prevention of age-related cognitive decline and alzheimer’s disease. J. Alzheimer’s Dis. 2012, 29, 711–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popovic, L.M.; Mitic, N.R.; Miric, D.; Bisevac, B.; Miric, M.; Popovic, B. Influence of vitamin C supplementation on oxidative stress and neutrophil inflammatory response in acute and regular exercise. Oxid. Med. Cell. Longev. 2015, 2015, 295497. [Google Scholar] [CrossRef]
- Dasgupta, J.; Dasgupta, S.; Rajni; Singh, R.K. Role of free radicals and antioxidants in schizophernia. Int. J. Pharm. Chem. Biol. Sci. 2014, 4, 825–828. [Google Scholar]
- Heiser, P.; Sommer, O.; Schmidt, A.J.; Clement, H.W.; Hoinkes, A.; Hopt, U.T.; Schulz, E.; Krieg, J.C.; Dobschütz, E. Effects of antipsychotics and vitamin C on the formation of reactive oxygen species. J. Psychopharmacol. 2010, 24, 1499–1504. [Google Scholar] [CrossRef]
- Travica, N.; Ried, K.; Sali, A.; Scholey, A.; Hudson, I.; Pipingas, A. Vitamin C status and cognitive function: A systematic review. Nutrients 2017, 9, 960. [Google Scholar] [CrossRef]
- Dakhale, G.N.; Khanzode, S.D.; Khanzode, S.S.; Saoji, A. Supplementation of vitamin C with atypical antipsychotics reduces oxidative stress and improves the outcome of schizophrenia. Psychopharmacology 2005, 182, 494–498. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture, Agricultural Research Service. Available online: https://fdc.nal.usda.gov/ (accessed on 24 April 2020).
- Madireddy, S.; Madireddy, S. The role of diet in maintaining strong brain health by taking the advantage of the gut–brain axis. J. Food Nutr. Res. 2019, 7, 41–50. [Google Scholar] [CrossRef]
- Cieslak, K.; Feingold, J.; Antonius, D. Low Vitamin D levels predict clinical features of schizophrenia. Schizophr. Res. 2014, 159, 543–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krivoy, A.; Onn, R.; Vilner, Y.; Hochman, E.; Weizman, S.; Paz, A.; Hess, S.; Sagy, R.; Kimhi-Nesher, S.; Kalter, E.; et al. Vitamin D supplementation in chronic schizophrenia patients treated with clozapine: A randomized, double-blind, placebo-controlled clinical trial. EBioMedicine 2017, 26, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Lally, J.; Gaughran, F. Vitamin D in schizophrenia and depression: A clinical review. BJPsych Adv. 2019, 25, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Samoes, B.; Silveira, C. The role of vitamin D in the pathophysiology of schizophrenia. Neuropsychiatry 2017, 7, 362–369. [Google Scholar] [CrossRef]
- Sheikhmoonesi, F.; Zarghami, M.; Mamashli, S.; Charati, J.Y.; Hamzehpour, R.; Fattahi, S.; Azadbakht, R.; Kashi, Z.; Ala, S.; Moshayedi, M.; et al. Effectiveness of vitamin D supplement therapy in chronic stable schizophrenic male patients: A randomized controlled trial. Iran. J. Pharm. Res. 2016, 15, 941–950. [Google Scholar]
- Zhu, J.L.; Luo, W.W.; Cheng, X.; Li, Y.; Zhang, Q.Z.; Peng, W.X. Vitamin D deficiency and schizophrenia in adults: A systematic review and meta–analysis of observational studies. Psychiatry Res. 2020, 288, 112959. [Google Scholar] [CrossRef]
- Soliman, R.H.; Oraby, M.I.; Hussein, M.; El-Shafy, S.A.; Mostafa, S. Could vitamin D deficiency have an impact on motor and cognitive function in Parkinson’s disease? Egypt. J. Neurol. Psychiatry Neurosurg. 2019, 55, 34. [Google Scholar] [CrossRef]
- Wrzosek, M.; Łukaszkiewicz, J.; Wrzosek, M.; Jakubczyk, A.; Matsumoto, H.; Piątkiewicz, P.; Radziwoń-Zaleska, M.; Wojnar, M.; Nowicka, G. Vitamin D and the central nervous system. Pharmacol. Rep. 2013, 65, 271–278. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhou, R.; Zhang, Z.; Li, K. The association between vitamin D status, vitamin D supplementation, sunlight exposure, and Parkinson’s disease: A systematic review and meta–analysis. Med. Sci. Monit. 2019, 25, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Chiang, M.; Natarajan, R.; Fan, X. Vitamin D in schizophrenia: A clinical review. Evid. Based Ment. Health 2016, 19, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Graham, K.A.; Keefe, R.S.; Lieberman, J.A.; Calikoglu, A.S.; Lansing, K.M.; Perkins, D.O. Relationship of low vitamin D status with positive, negative and cognitive symptom domains in people with first-episode schizophrenia. Early Interv. Psychiatry 2015, 9, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, A.; Banafshe, H.R.; Mirhosseini, N.; Moradi, M.; Karimi, M.; Mehrzad, F.; Bahmani, F.; Asemi, Z. Clinical and metabolic response to vitamin D plus probiotic in schizophrenia patients. BMC Psychiatry 2019, 19, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ovesen, L.; Brot, C.; Jakobsen, J. Food contents and biological activity of 25-hydroxyvitamin D: A vitamin D metabolite to be reckoned with? Ann. Nutr. Metab. 2003, 47, 107–113. [Google Scholar] [CrossRef]
- Calvo, M.S.; Whiting, S.J.; Barton, C.N. Vitamin D fortification in the United States and Canada: Current status and data needs. Am. J. Clin. Nutr. 2004, 80, 1710S–1716S. [Google Scholar] [CrossRef] [Green Version]
- Balanza-Martinez, V. Nutritional supplements in psychotic disorders. Actas Esp. Psiquiatr. 2017, 45, 16–25. [Google Scholar]
- Wang, D.; Zhai, J.X.; Liu, D.W. Serum folate levels in schizophrenia: A meta-analysis. Psychiatry Res. 2016, 235, 83–89. [Google Scholar] [CrossRef]
- van de Lagemaat, E.E.; de Groot, L.C.P.G.M.; van den Heuvel, E.G.H.M. Vitamin B12 in relation to oxidative stress: A systematic review. Nutrients 2019, 11, 482. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, E.S.; Conus, N.; Kaput, J. B vitamin polymorphisms and behavior: Evidence of associations with neurodevelopment, depression, schizophrenia, bipolar disorder and cognitive decline. Neurosci. Biobehav. Rev. 2014, 47, 307–320. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Hodgson, N.W.; Trivedi, M.S.; Abdolmaleky, H.M.; Fournier, M.; Cuenod, M.; Do, K.Q.; Deth, R.C. Decreased Brain Levels of Vitamin B12 in Aging, Autism and Schizophrenia. PLoS ONE 2016, 11, e0146797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, H.E.; Roffman, J.L. Vitamin Supplementation in the Treatment of Schizophrenia. CNS Drugs 2014, 28, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L.; Rich, S.; Rosenberg, I.; Jacques, P.; Dallal, G.; Wilson, W.F.; Selhub, J. Plasma vitamin B12 concentrations relate to intake source in the Framingham offspring study. Am. J. Clin. Nutr. 2000, 71, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, F.; Bito, T. Vitamin B12 sources and microbial interaction. Exp. Biol. Med. 2018, 243, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Fedosov, S.N.; Nexo, E.; Heegaard, C.W. Vitamin B12 and its binding proteins in milk from cow and buffalo in relation to bioavailability of B12. J. Dairy Sci. 2019, 102, 4891–4905. [Google Scholar] [CrossRef]
- Munusamy, U.; Abdullah, S.N.A. Vitamin E: Phytochemistry and molecular aspects. Plant. Hum. Health 2019, 2, 345–360. [Google Scholar] [CrossRef]
- de Lau, L.M.L.; Bornebroek, M.; Witteman, J.C.M.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M.B. Dietary fatty acids and the risk of Parkinson disease: The rotterdam study. Neurology 2005, 64, 2040–2045. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Fries, G.R.; Colpo, G.D.; Silveira, P.P.; Portella, A.K.; Tabarés-Seisdedos, R.; Kapczinski, F. The therapeutic use of omega-3 fatty acids in bipolar disorder. Exp. Rev. Neurother. 2011, 11, 1029–1047. [Google Scholar] [CrossRef]
- Satogami, K.; Takahashi, S.; Yamada, S.; Ukai, S.; Shinosaki, K. Omega-3 fatty acids related to cognitive impairment in patients with schizophrenia. Schizophr. Res. Cogn. 2017, 9, 8–12. [Google Scholar] [CrossRef]
- Hsu, M.-C.; Huang, Y.-S.; Ouyang, W.-C. Beneficial effects of omega-3 fatty acid supplementation in schizophrenia: Possible mechanisms. Lipids Health Dis. 2020, 19, 159. [Google Scholar] [CrossRef]
- Crump, C.; Winkleby, M.A.; Sundquist, K.; Sundquist, J. Comorbidities and mortality in persons with schizophrenia: A Swedish national cohort study. Am. J. Psychiatry 2013, 170, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Tessier, C.; Sweers, K.; Frajerman, A.; Bergaoui, H.; Ferreri, F.; Delva, C.; Lapidus, N.; Lamaziere, A.; Roiser, J.P.; De Hert, M.; et al. Membrane lipidomics in schizophrenia patients: A correlational study with clinical and cognitive manifestations. Transl. Psychiatry 2016, 6, e906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawełczyk, T.; Grancow, M.; Kotlicka-Antczak, M.; Trafalska, E.; Gębski, P.; Szemraj, J.; Żurner, N.; Pawełczyk, A. Omega-3 fatty acids in first–episode schizophrenia—A randomized controlled study of efficacy and relapse prevention (OFFER): Rationale, design, and methods. BMC Psychiatry 2015, 15, 97. [Google Scholar] [CrossRef] [Green Version]
- Berger, G.E.; Proffitt, T.; McConchie, M.; Yuen, H.; Wood, S.J.; Amminger, G.P.; Brewer, W.; McGorry, P.D. Ethyl-eicosapentaenoic acid in first-episode psychosis: A randomized, placebo-controlled trial. J. Clin. Psychiatry 2007, 68, 1867–1875. [Google Scholar] [CrossRef]
- Agostoni, C.; Nobile, M.; Ciappolino, V.; Delvecchio, G.; Tesei, A.; Turolo, S.; Crippa, A.; Mazzocchi, A.; Altamura, C.A.; Brambilla, P. The role of omega-3 fatty acids in developmental psychopathology: A systematic review on early psychosis, autism, and ADHD. Int. J. Mol. Sci. 2017, 18, 2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzatello, P.; Brignolo, E.; De Grandi, E.; Bellino, S. Supplementation with omega-3 fatty acids in psychiatric disorders: A review of literature data. J. Clin. Med. 2016, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- Mahadik, S.P.; Pillai, A.; Joshi, S.; Foster, A. Prevention of oxidative stress-mediated neuropathology and improved clinical outcome by adjunctive use of a combination of antioxidants and omega-3 fatty acids in schizophrenia. Int. Rev. Psychiatry 2006, 18, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Sivrioglu, E.Y.; Kirli, S.; Sipahioglu, D.; Gursoy, B.; Sarandöl, E. The impact of omega-3 fatty acids, vitamins E and C supplementation on treatment outcome and side effects in schizophrenia patients treated with haloperidol: An open–label pilot study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 1493–1499. [Google Scholar] [CrossRef]
- Torrey, E.F.; Davis, J.M. Adjunct treatments for schizophrenia and bipolar disorder: What to try when you are out of ideas. Clin. Schizophr. Relat. Psychoses 2012, 5, 208–216. [Google Scholar] [CrossRef]
- Palaniswamy, K.S.; Vishwanadha, V.P.; Singaravelu, S.R. Fish oil rich in eicosapentaenoic acid protects against oxidative stress-related renal dysfunction induced by TCDD in Wistar rats. Cell Stress Chaperones 2014, 19, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Meital, L.T.; Windsor, M.T.; Perissiou, M.; Schulze, K.; Magee, R.; Kuballa, A.; Golledge, J.; Bailey, T.G.; Askew, C.D.; Russell, F.D. Omega-3 fatty acids decrease oxidative stress and inflammation in macrophages from patients with small abdominal aortic aneurysm. Sci. Rep. 2019, 9, 12978. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Samee, L.D.; El-Wardany, I.; Abdel-Fattah, S.A.; Abd El-Azeem, N.A.; Elsharkawy, M.S. Dietary omega-3 and antioxidants improve long-chain omega-3 and lipid oxidation of broiler meat. Bull. Natl. Res. Cent. 2019, 43, 45. [Google Scholar] [CrossRef] [Green Version]
- Pawełczyk, T.; Grancow-Grabka, M.; Trafalska, E.; Szemraj, J.; Pawełczyk, A. Oxidative stress reduction related to the efficacy of n–3 polyunsaturated fatty acids in first episode schizophrenia: Secondary outcome analysis of the OFFER randomized trial. Prostaglandins Leukot. Essent. Fatty Acids 2017, 121, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Sanguansri, L.; Augustin, M.A.; Lockett, T.J.; Abeywardena, M.Y.; Royle, P.J.; Mano, M.T.; Patten, G.S. Bioequivalence of n-3 fatty acids from microencapsulated fish oil formulations in human subjects. Br. J. Nutr. 2015, 113, 822–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vannice, G.; Rasmussen, H. Position of the academy of nutrition and dietetics: Dietary fatty acids for healthy adults. J. Acad. Nutr. Diet. 2014, 114, 136–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simopoulos, A.P. Evolutionary aspects of diet: The omega-6/omega-3 ratio and the brain. Mol. Neurobiol. 2011, 44, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.; Lane, H.; Lin, C. Brexpiprazole for the treatment of schizophrenia. Expert Opin. Pharmacother. 2017, 18, 217–223. [Google Scholar] [CrossRef]
- Bruijnzeel, D.; Yazdanpanah, M.; Suryadevara, U.; Tandon, R. Lurasidone in the treatment of schizophrenia: A critical evaluation. Expert Opin. Pharmacother. 2015, 16, 1559–1565. [Google Scholar] [CrossRef]
- Biagi, E.; Capuzzi, E.; Colmegna, F.; Mascarini, A.; Brambilla, G.; Ornaghi, A.; Santambrogio, J.; Clerici, M. Long-acting injectable antipsychotics in schizophrenia: Literature review and practical rerspective, with a focus on aripiprazole once-monthly. Adv. Ther. 2017, 34, 1036–1048. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.Y.; Tan, Y.L.; Cao, L.Y.; Wu, G.Y.; Xu, Q.; Shen, Y.; Zhou, D.F. Antioxidant enzymes and lipid peroxidation in different forms of schizophrenia treated with typical and atypical antipsychotics. Schizophr. Res. 2006, 81, 291–300. [Google Scholar] [CrossRef]
- Correll, C.U.; Kohegyi, E.; Zhao, C.; Baker, R.A.; McQuade, R.; Salzman, P.M.; Sanchez, R.; Nyilas, M.; Carson, W. Oral aripiprazole as maintenance treatment in adolescent schizophrenia: Results from a 52-week, randomized, placebo-controlled withdrawal study. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Croxtall, J.D. Aripiprazole: A review of its use in the management of schizophrenia in adults. CNS Drugs 2012, 26, 155–183. [Google Scholar] [CrossRef] [PubMed]
- Rapinesi, C.; Kotzalidis, G.D.; Mazzarini, L.; Brugnoli, R.; Ferracuti, S.; De Filippis, S.; Cuomo, I.; Giordano, G.; Del Casale, A.; Angeletti, G.; et al. Long-acting injectable (LAI) aripiprazole formulations in the Treatment of schizophrenia and bipolar disorder: A systematic review. Clin. Drug Investig. 2019, 39, 713–735. [Google Scholar] [CrossRef]
- de Bartolomeis, A.; Latte, G.; Tomasetti, C.; Iasevoli, F. Glutamatergic postsynaptic density protein dysfunctions in synaptic plasticity and dendritic spines morphology: Relevance to schizophrenia and other behavioral disorders pathophysiology, and implications for novel therapeutic approaches. Mol. Neurobiol. 2014, 49, 484–511. [Google Scholar] [CrossRef] [PubMed]
- Tuplin, E.W.; Holahan, M.R. Aripiprazole, a drug that displays partial agonism and functional selectivity. Curr. Neuropharmacol. 2017, 15, 1192–1207. [Google Scholar] [CrossRef] [Green Version]
- Kane, J.M.; Zhao, C.; Johnson, B.R.; Baker, R.A.; Eramo, A.; McQuade, R.D.; Duca, A.R.; Sanchez, R.; Peters-Strickland, T. Hospitalization rates in patients switched from oral anti-psychotics to aripiprazole once-monthly: Final efficacy analysis. J. Med. Econ. 2015, 18, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Naber, D.; Hansen, K.; Forray, C.; Baker, R.A.; Sapin, C.; Beillat, M.; Peters-Strickland, T.; Nylander, A.; Hertel, P.; Andersen, H.S.; et al. Qualify: A randomized head-to-head study of aripiprazole once-monthly and paliperidone palmitate in the treatment of schizophrenia. Schizophr. Res. 2015, 168, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, E.L.A.R.; de Mendonça Lima, T.; Vieira, M.E.B.; Storpirtis, S.; Aguiar, P.M. Efficacy and safety of aripiprazole for the treatment of schizophrenia: An overview of systematic reviews. Eur. J. Clin. Pharmacol. 2018, 74, 1215–1233. [Google Scholar] [CrossRef]
- Nasrallah, H.A.; Aquila, R.; Du, Y.; Stanford, A.D.; Claxton, A.; Weiden, P.J. Long-term safety and tolerability of aripiprazole lauroxil in patients with schizophrenia. CNS Spectr. 2019, 24, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Diefenderfer, L.A.; Iuppa, C. Brexpiprazole: A review of a new treatment option for schizophrenia and major depressive disorder. Ment. Health Clin. 2018, 7, 207–212. [Google Scholar] [CrossRef]
- Frampton, J.E. Brexpiprazole: A review in schizophrenia. Drugs 2019, 79, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.; Citrome, L. Brexpiprazole for the maintenance treatment of adults with schizophrenia: An evidence-based review and place in therapy. Neuropsychiatr. Dis. Treat. 2019, 15, 247–257. [Google Scholar] [CrossRef] [Green Version]
- Correll, C.U.; Skuban, A.; Hobart, M.; Ouyang, J.; Weiller, E.; Weiss, C.; Kane, J.M. Efficacy of brexpiprazole in patients with acute schizophrenia: Review of three randomized, double-blind, placebo-controlled studies. Schizophr. Res. 2017, 190, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Barnwal, P.; Winston, B.A.; Mondal, S.; Saha, I. Brexpiprazole: So far so good. Ther. Adv. Psychopharmacol. 2016, 6, 39–54. [Google Scholar] [CrossRef] [Green Version]
- McEvoy, J.; Citrome, L. Brexpiprazole for the treatment of schizophrenia: A Review of this novel serotonin-dopamine activity modulator. Clin. Schizophr. Relat. Psychoses 2016, 9, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Scarff, J.R. Brexpiprazole: A new treatment option for schizophrenia. Innov. Clin. Neurosci. 2016, 13, 26–29. [Google Scholar] [PubMed]
- Garnock-Jones, K.P. Brexpiprazole: A review in schizophrenia. CNS Drugs 2016, 30, 335–342. [Google Scholar] [CrossRef]
- Markovic, M.; Gallipani, A.; Patel, K.H.; Maroney, M. Brexpiprazole. Ann. Pharmacother. 2017, 51, 315–322. [Google Scholar] [CrossRef]
- Yee, A. Brexpiprazole for the treatment of schizophrenia. Expert Rev. Neurother. 2016, 16, 109–122. [Google Scholar] [CrossRef]
- Marder, S.R.; Hakala, M.J.; Josiassen, M.K.; Zhang, P.; Ouyang, J.; Weiller, E.; Weiss, C.; Hobart, M. Brexpiprazole in patients with schizophrenia: Overview of short- and long-term phase 3 controlled studies. Acta Neuropsychiatr. 2017, 29, 278–290. [Google Scholar] [CrossRef]
- Bravo-Mehmedbasic, A. Risperidone in the treatment of schizophrenia. Med. Arh. 2011, 65, 345–347. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Zhang, Y.; You, X.; Zhang, W.; Ma, Y.; Long, Q.; Liu, Z.; Hao, W.; Zeng, Y.; Teng, Z. Effects of risperidone on blood levels of interleukin-6 in schizophrenia: A meta-analysis. Medicine 2020, 99, e19694. [Google Scholar] [CrossRef] [PubMed]
- Rattehalli, R.D.; Zhao, S.; Li, B.G.; Jayaram, M.B.; Xia, J.; Sampson, S. Risperidone versus placebo for schizophrenia. Cochrane Database Syst. Rev. 2016, 12, CD006918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Wu, F.; Zhang, J.; Shi, L.; Hu, J.; Zhu, H.; Xiao, B.; Lin, W.; Wen, Y.; Shang, D. Effects of risperidone and aripiprazole on serum levels of prolactin, testosterone and estradiol in female patients with schizophrenia. Drug Res. 2018, 68, 410–414. [Google Scholar] [CrossRef]
- Dietrich-Muszalska, A.; Kontek, B. Lipid peroxidation in patients with schizophrenia. Psychiatry Clin. Neurosci. 2010, 64, 469–475. [Google Scholar] [CrossRef]
- Javed, A.; Arthur, H.; Curtis, L.; Hansen, L.; Pappa, S. Practical guidance on the use of lurasidone for the treatment of adults with schizophrenia. Neurol. Ther. 2019, 8, 215–230. [Google Scholar] [CrossRef] [Green Version]
- Zheng, W.; Cai, D.; Yang, X.; Li, L.; Zhang, Q.; Ng, C.H.; Ungvari, G.S.; Li, X.; Ning, Y.; Xiang, Y. Short-term efficacy and tolerability of lurasidone in the treatment of acute schizophrenia: A meta-analysis of randomized controlled trials. J. Psychiatr. Res. 2018, 103, 244–251. [Google Scholar] [CrossRef]
- Goldman, R.; Loebel, A.; Cucchiaro, J.; Deng, L.; Findling, R.L. Efficacy and safety of lurasidone in adolescents with schizophrenia: A 6-week, randomized placebo-controlled study. J. Child Adolesc. Psychopharmacol. 2017, 27, 516–525. [Google Scholar] [CrossRef] [Green Version]
- Higuchi, T.; Ishigooka, J.; Iyo, M.; Yeh, C.; Ebenezer, E.G.; Liang, K.Y.; Lee, J.K.; Lee, S.Y.; Lin, S.K.; Yoon, B.; et al. Lurasidone in the treatment of schizophrenia: Results of a double-blind, placebo-controlled trial in Asian patients. Asia Pac. Psychiatry 2019, 11, e12352. [Google Scholar] [CrossRef]
- Correll, C.U.; Cucchiaro, J.; Silva, R.; Hsu, J.; Pikalov, A.; Loebel, A. Long-term safety and effectiveness of lurasidone in schizophrenia: A 22-month, open-label extension study. CNS Spectr. 2016, 21, 393–402. [Google Scholar] [CrossRef] [Green Version]
- Lincoln, J.; Tripathi, A. Lurasidone for schizophrenia. Drug Ther. Bull. 2015, 53, 30–32. [Google Scholar]
- Khokhar, J.Y.; Henricks, A.M.; Kirk, E.; Green, A.I. Unique effects of clozapine: A pharmacological perspective. Adv. Pharmacol. 2018, 82, 137–162. [Google Scholar] [PubMed]
- Sahni, S.; Chavan, B.S.; Sidana, A.; Kalra, P.; Kaur, G. Comparative study of clozapine versus risperidone in treatment-naive, first-episode schizophrenia: A pilot study. Indian J. Med. Res. 2016, 144, 697–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siskind, D.J.; Lee, M.; Ravindran, A.; Zhang, Q.; Ma, E.; Motamarri, B.; Kisely, S. Augmentation strategies for clozapine refractory schizophrenia: A systematic review and meta-analysis. Aust. N. Z. J. Psychiatry 2018, 52, 751–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakra, E.; Azorin, J. Clozapine for the treatment of schizophrenia. Expert Opin. Pharmacother. 2012, 13, 1923–1935. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Uchida, H.; Watanabe, K.; Kashima, H. Factors associated with response to clozapine in schizophrenia: A review. Psychopharmacol. Bull. 2011, 44, 32–60. [Google Scholar]
- Vermeulen, J.M.; van Rooijen, G.; van de Kerkhof, M.P.J.; Sutterland, A.L.; Correll, C.U.; de Haan, L. Clozapine and long-term mortality risk in patients with schizophrenia: A systematic review and meta-analysis of studies lasting 1.1–12.5 years. Schizophr. Bull. 2019, 45, 315–329. [Google Scholar] [CrossRef]
- Lee, M.A.; Thompson, P.A.; Meltzer, H.Y. Effects of clozapine on cognitive function in schizophrenia. J. Clin. Psychiatry 1994, 55 (Suppl. B), 82–87. [Google Scholar]
- Andrade, C. Antipsychotic drugs in schizophrenia: Relative effects in patients with and without treatment resistance. J. Clin. Psychiatry 2016, 77, e1656–e1660. [Google Scholar] [CrossRef] [Green Version]
- Dietrich-Muszalska, A.; Kopka, J.; Kwiatkowska, A. The effects of ziprasidone, clozapine and haloperidol on lipid peroxidation in human plasma (in vitro): Comparison. Neurochem. Res. 2013, 38, 1490–1495. [Google Scholar] [CrossRef]
- Hendouei, N.; Farnia, S.; Mohseni, F.; Salehi, A.; Bagheri, M.; Shadfar, F.; Barzegar, F.; Hoseini, S.D.; Charati, J.Y.; Shaki, F. Alterations in oxidative stress markers and its correlation with clinical findings in schizophrenic patients consuming perphenazine, clozapine and risperidone. Biomed. Pharmacother. 2018, 103, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Siskind, D.; McCartney, L.; Goldschlager, R.; Kisely, S. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: Systematic review and meta-analysis. Br. J. Psychiatry 2016, 209, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, C.E.; Awad, G.A.; Rathbone, J.; Thornley, B.; Soares-Weiser, K. Chlorpromazine versus placebo for schizophrenia. Cochrane Database Syst. Rev. 2014, CD000284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, C.E.; Rathbone, J.; Thornley, B.; Clarke, M.; Borrill, J.; Wahlbeck, K.; Awad, G.A. Chlorpromazine for schizophrenia: A Cochrane systematic review of 50 years of randomised controlled trials. BMC Med. 2005, 3, 15. [Google Scholar] [CrossRef] [Green Version]
- Dudley, K.; Liu, X.; De Haan, S. Chlorpromazine dose for people with schizophrenia. Cochrane Database Syst. Rev. 2017, 4, CD007778. [Google Scholar] [CrossRef]
- Saha, K.B.; Bo, L.; Zhao, S.; Xia, J.; Sampson, S.; Zaman, R.U. Chlorpromazine versus atypical antipsychotic drugs for schizophrenia. Cochrane Database Syst. Rev. 2016, CD010631. [Google Scholar] [CrossRef]
- Ficarra, S.; Russo, A.; Barreca, D.; Giunta, E.; Galtieri, A.; Tellone, E. Short-term effects of chlorpromazine on oxidative stress in erythrocyte functionality: Activation of metabolism and membrane perturbation. Oxid. Med. Cell. Longev. 2016, 2016, 2394130. [Google Scholar] [CrossRef] [Green Version]
- Muhieddine, D.; Moughnié, M.; Abdel-Razzak, Z. Short communication: Chlorpromazine causes a time-dependent decrease of lipids in Saccharomyces cerevisiae. Interdiscip. Toxicol. 2019, 12, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Gangadhar, N.; Varambally, S. Yoga therapy for schizophrenia. Int. J. Yoga 2012, 5, 85–91. [Google Scholar]
- Ganguly, P.; Soliman, A.; Moustafa1, A.A. Holistic management of schizophrenia symptoms using pharmacological and non-pharmacological treatment. Front. Public Health 2018, 6, 166. [Google Scholar] [CrossRef]
- Health Quality Ontario. Cognitive behavioral therapy for psychosis: A health technology assessment. Ont. Health Technol. Assess. Ser. 2018, 18, 1–141. [Google Scholar]
- Jones, C.; Hacker, D.; Meaden, A.; Cormac, I.; Irving, C.B.; Xia, J.; Zhao, S.; Shi, C.; Chen, J. Cognitive behavioural therapy plus standard care versus standard care plus other psychosocial treatments for people with schizophrenia. Cochrane Database Syst. Rev. 2018, CD008712. [Google Scholar] [CrossRef]
- Sensky, T.; Turkington, D.; Kingdon, D.; Scott, J.L.; Scott, J.; Siddle, R.O.; O’Carroll, M.; Barnes, T.R.E. A randomized controlled trial of cognitive–behavioural therapy for persistent symptoms in schizophrenia resistant to medication. Arch. Gen. Psychiatry 2000, 57, 165–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogarty, G.E.; Greenwald, D.P.; Eack, S.M. Durability and mechanism of effects of Cognitive Enhancement Therapy. Psychiatr. Serv. 2006, 57, 1751–1757. [Google Scholar] [CrossRef] [Green Version]
- Eack, S.M.; Hogarty, G.E.; Greenwald, D.P.; Hogarty, S.S.; Keshavan, M.S. Effects of cognitive enhancement therapy on employment outcomes in early schizophrenia: Results from a two-year randomized trial. Res. Soc. Work Pract. 2011, 21, 32–42. [Google Scholar] [CrossRef] [Green Version]
- Costa, R.; Bastos, T.; Probst, M.; Seabra, A.; Abreu, S.; Vilhena, E.; Rosenbaum, S.; Ward, P.B.; Corredeira, R. Association of lifestyle-related factors and psychological factors on quality of life in people with schizophrenia. Psychiatry Res. 2018, 267, 382–393. [Google Scholar] [CrossRef]
- Firth, J.; Carney, R.; Stubbs, B.; Teasdale, S.; Vancampfort, D.; Ward, P.; Berk, M.; Sarris, J. Nutritional deficiencies and clinical correlates in first-episode psychosis: A systematic review and meta-analysis. Schizophr. Bull. 2017, 44, 1275–1292. [Google Scholar] [CrossRef]
- Funk, M.; Drew, N.; Knapp, M. Mental health, poverty and development. J. Public Ment. Health 2012, 11, 166–185. [Google Scholar] [CrossRef] [Green Version]
- Sarris, J.; Logan, A.C.; Akbaraly, T.N.; Amminger, G.P.; Balanzá-Martínez, V.; Freeman, M.P.; Hibbeln, J.; Matsuoka, Y.; Mischoulon, D.; Mizoue, T.; et al. Nutritional medicine as mainstream in psychiatry. Lancet Psychiatry 2015, 2, 271–274. [Google Scholar] [CrossRef]
- Adamowicz, K.; Kucharska-Mazur, J. Dietary behaviors and metabolic syndrome in schizophrenia patients. J. Clin. Med. 2020, 9, 537. [Google Scholar] [CrossRef] [Green Version]
- Simonelli-Muñoz, A.J.; Fortea, M.I.; Salorio, P.; Gallego-Gomez, J.I.; Sánchez-Bautista, S.; Balanza, S. Dietary habits of patients with schizophrenia: A self-reported questionnaire survey. Int. J. Ment. Health Nurs. 2012, 21, 220–228. [Google Scholar] [CrossRef]
- Heald, A.; Pendlebury, J.; Anderson, S.; Narayan, V.; Guy, M.; Gibson, M.; Haddad, P.; Livingston, M. Lifestyle factors and the metabolic syndrome in schizophrenia: A cross-sectional study. Ann. Gen. Psychiatry 2017, 16, 12. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Reactive oxygen species (ROS). The continuous reduction of oxygen through adding electrons generates ROS including superoxide anion radicals (O2•), hydroxyl radicals (HO•), peroxyl radicals (HOO•), and hydrogen peroxide (H2O2). The red circle indicates an unpaired electron.
Figure 1.
Reactive oxygen species (ROS). The continuous reduction of oxygen through adding electrons generates ROS including superoxide anion radicals (O2•), hydroxyl radicals (HO•), peroxyl radicals (HOO•), and hydrogen peroxide (H2O2). The red circle indicates an unpaired electron.

Figure 2.
ROS generation. The superoxide is generated from oxygen in the mitochondrial respiration chain, which can be further converted into hydrogen peroxide via superoxide dismutase. The hydrogen peroxide can be transformed to hydroxyl radicals and hydroxyl anions.
Figure 2.
ROS generation. The superoxide is generated from oxygen in the mitochondrial respiration chain, which can be further converted into hydrogen peroxide via superoxide dismutase. The hydrogen peroxide can be transformed to hydroxyl radicals and hydroxyl anions.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Madireddy, S.; Madireddy, S. Regulation of Reactive Oxygen Species-Mediated Damage in the Pathogenesis of Schizophrenia. Brain Sci. 2020, 10, 742. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10100742
AMA Style
Madireddy S, Madireddy S. Regulation of Reactive Oxygen Species-Mediated Damage in the Pathogenesis of Schizophrenia. Brain Sciences. 2020; 10(10):742. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10100742
Chicago/Turabian StyleMadireddy, Samskruthi, and Sahithi Madireddy. 2020. "Regulation of Reactive Oxygen Species-Mediated Damage in the Pathogenesis of Schizophrenia" Brain Sciences 10, no. 10: 742. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10100742
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.