Incidence of Autism Spectrum Disorder in Youths Affected by Gilles de la Tourette Syndrome Based on Data from a Large Single Italian Clinical Cohort

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Ethics and Procedures
- (i)
- To verify if patients met the inclusion/exclusion criteria, because sometimes, tics can be a symptom of another disease; with this in mind, we analyzed ceruloplasmin to exclude Wilson’s disease, thyroid hormones to exclude hyperthyroidism, amino acids to exclude metabolic disease, and a peripheral blood smear to exclude neuroacanthocytosis;
- (ii)
- All other levels (e.g., blood count, glycemia, azotemia, creatinine, prolactin, antistreptolysin o titre and throat swab, and transaminases) and urine samples were checked, and an ECG was performed, in order to gain a general picture of the patient’s state of health, which could be useful in case the patient needed pharmacological treatment.
2.3. Assessments
2.4. Statistical Analysis
3. Results
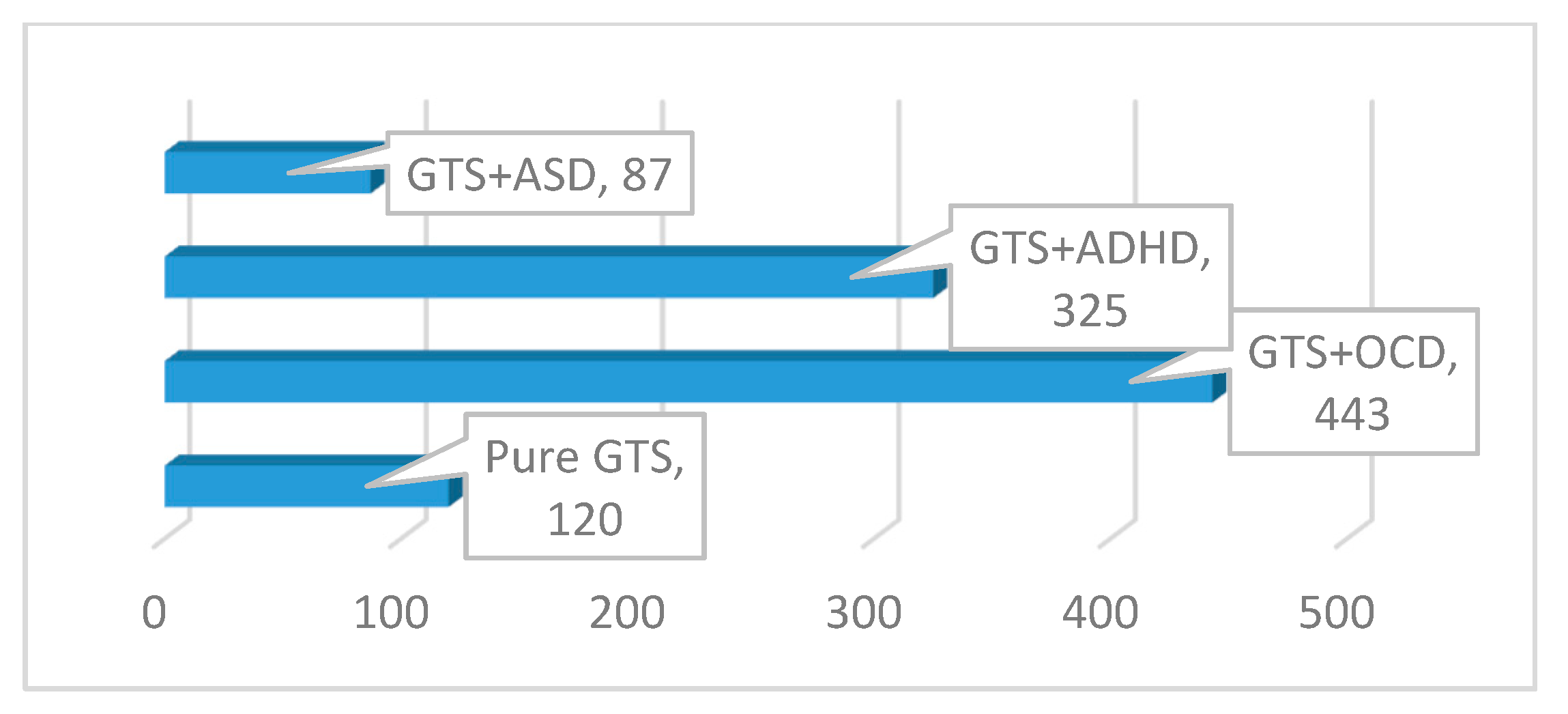
3.1. Sample Characteristics
3.2. Incidence of ASD in GTS
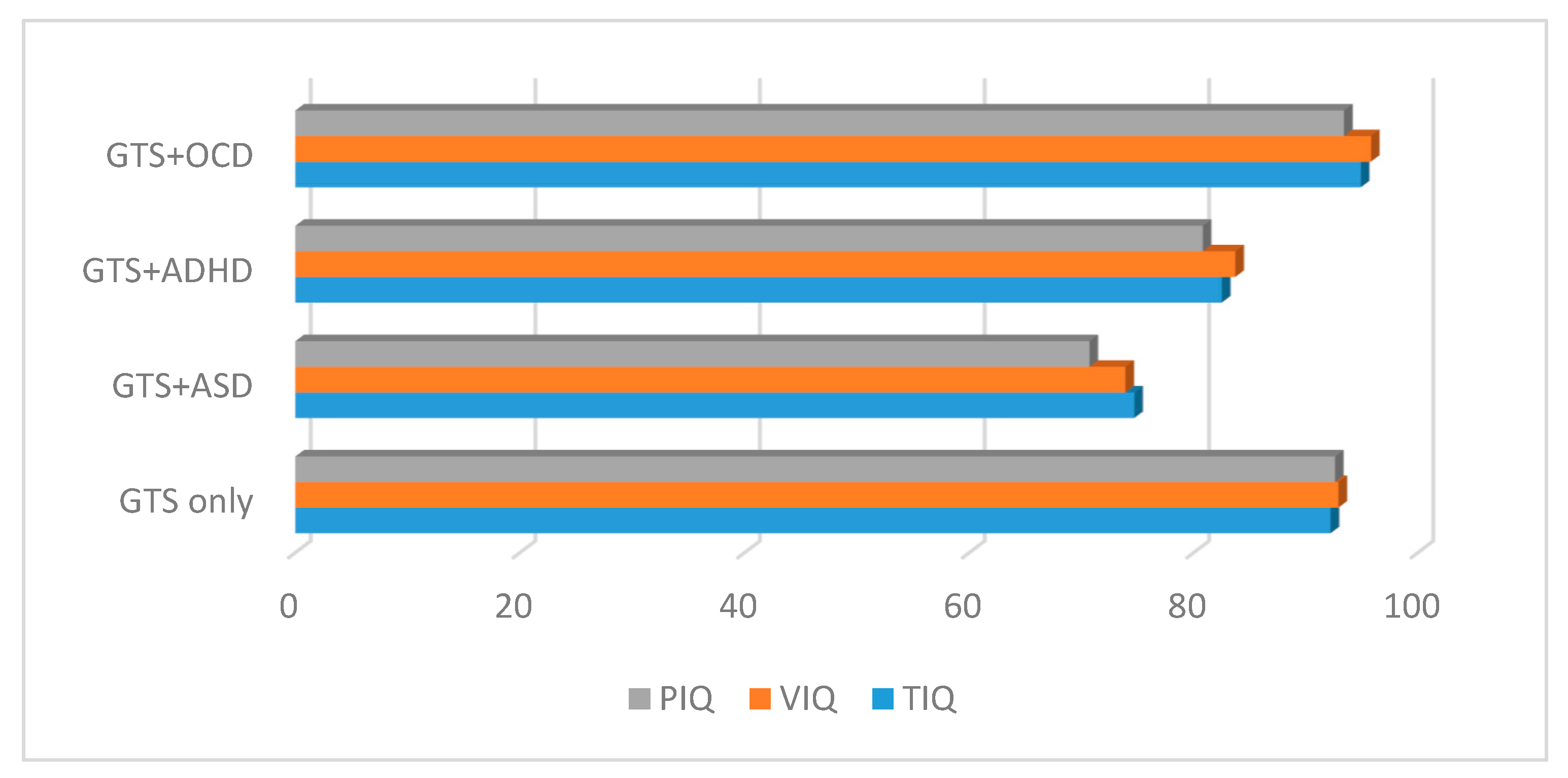
3.3. Neuropsychological Evaluation
4. Discussion
- (i)
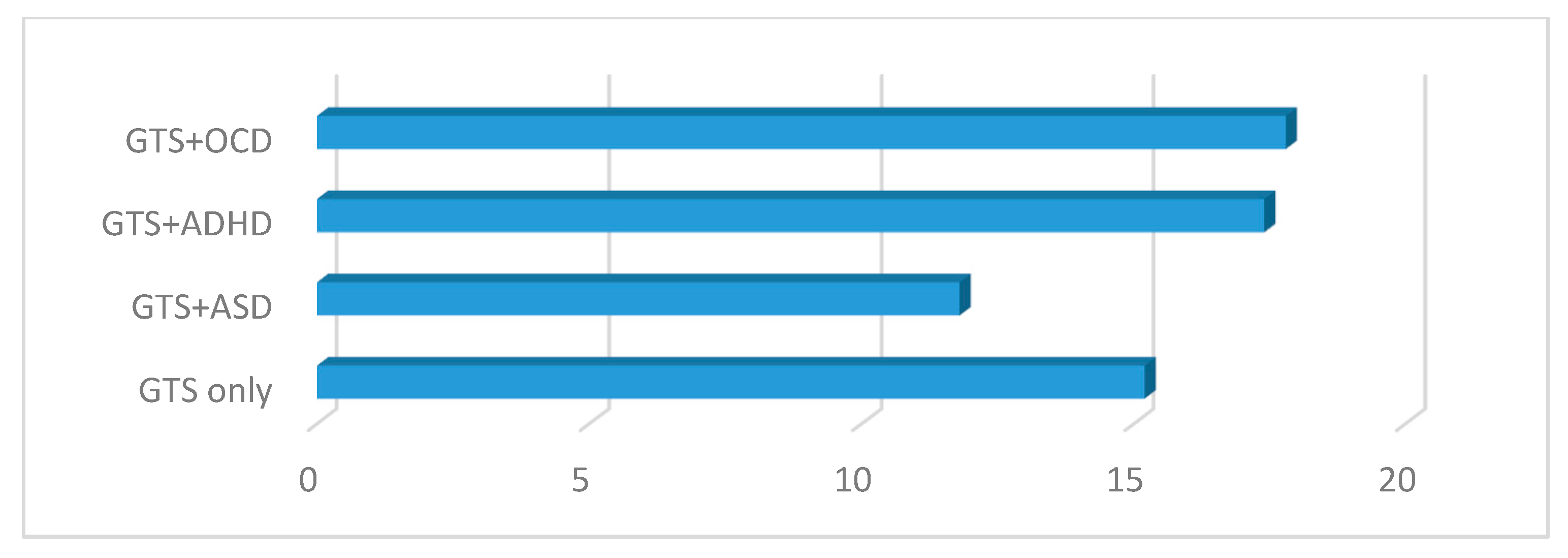
- The YGTSS scores are in line with previous studies [2,29] stating that high incidence of OCD and ADHD in GTS can cause poor quality of life and distress, and worsen symptoms the symptoms of GTS with higher YGTSS scores [30]. On the contrary, we did not find a higher YGTSS score in patients with GTS + ASD. This could be explained by the lower mean IQ, which could have resulted in a lower consciousness [31];
- (ii)
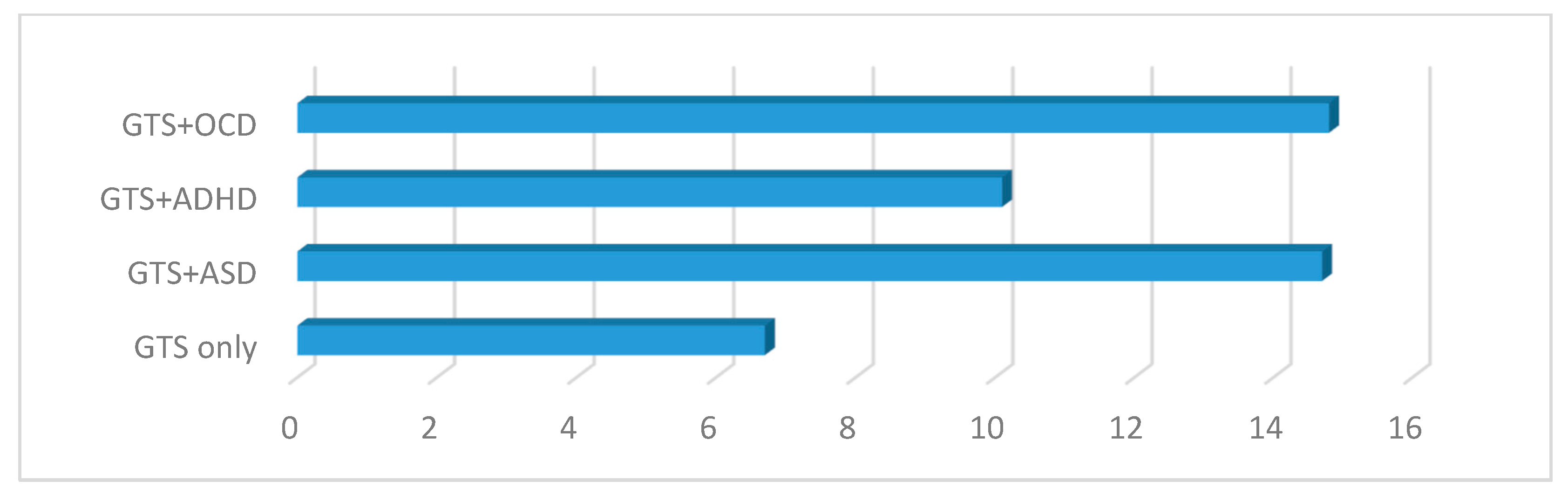
- The CY-BOCS scores showed statistically significant differences between all four GTS subgroups. Patients with GTS + OCD and GTS + ASD presented higher scores, but they were not statistically different compared to those of the GTS only and GTS + ADHD subgroups. These results are of interest, as repetitive behaviors are observed in as many as 65% of patients with GTS and can be classified as “tic-like” or OCD-like symptoms according to the clinical phenomenology [30]. Repetitive behaviors in ASD typically overlap with the phenomena in GTS; however, it may be challenging to distinguish the phenomenological characteristics of ASD from those of GTS. In clinical practice, medical professionals often find it difficult to define the disorder that best describes a child’s symptoms [31];
- (iii)
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Rizzo, R.; Gulisano, M.; Calì, P.V.; Curatolo, P. Long term clinical course of Tourette syndrome. Brain Dev. 2012, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, R.; Gulisano, M.; Pellico, A.; Calì, P.V.; Curatolo, P. Tourette syndrome and comorbid conditions: A spectrum of different severities and complexities. J. Child Neurol. 2014, 29, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Efron, D.; Dale, R.C. Tics and Tourette syndrome. J. Paediatr. Child Health 2018, 54, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, R.; Gulisano, M.; Martino, D.; Robertson, M.M. Gilles de la Tourette Syndrome, Depression, Depressive illness, and Correlates in a Child and adolescent Population. J. Child Adolesc. Psychopharmacol. 2017, 27, 243–249. [Google Scholar] [CrossRef]
- Burd, L.; Li, Q.; Kerbeshian, J.; Klug, M.G.; Freeman, R.D. Tourette syndrome and comorbid pervasve developmental disorders. J. Child Neurol. 2009, 24, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Darrow, S.M.; Grados, M.; Sandor, P.; Hirschtritt, M.E.; Illmann, C.; Osiecki, L.; Dion, Y.; King, R.; Pauls, D.; Budman, C.L.; et al. Autism Spectrum Symptoms in a Tourette Syndrome Sample. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 610–617. [Google Scholar] [CrossRef] [Green Version]
- Ghanizadeh, A.; Mosallaei, S. Psychiatric disorder and behavioral problems in children and adolescents with Tourette Syndrome. Brain Dev. 2009, 31, 15–19. [Google Scholar] [CrossRef]
- Huisman-van Dijk, H.M.; Schoot, R.V.; Rijkeboer, M.M.; Mathews, C.A.; Cath, D.C. The relationship between tics, OC, ADHD and autism symptoms: A cross-disorder symptom analysis in Gilles de la Tourette syndrome patients and family-members. Psychiatry Res. 2016, 237, 138–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cravedi, E.; Deniau, E.; Giannitelli, M.; Xavier, J.; Hartmann, A.; Cohen, D. Tourette syndrome and other neurodevelopmental disorders: A comprehensive review. Child Adolesc. Psychiatry Ment. Health 2017, 11, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eapen, V.; Snedden, C.; Črnčec, R.; Pick, A.; Sachdev, P. Tourette syndrome, co-morbidities and quality of life. Aust. N. Z. J. Psychiatry 2016, 50, 82–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rydzewska, E.; Hughes-McCormack, L.A.; Gillberg, C.; Henderson, A.; MacIntyre, C.; Rintoul, J.; Cooper, S.A. Age at identification, prevalence and general health of children with autism: Observational study of a whole country population. BMJ Open 2019, 9, e025904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirschtritt, M.E.; Lee, P.C.; Pauls, D.L.; Dion, Y.; Grados, M.A.; Illmann, C.C.; King, R.A.; Sandor, P.; McMahon, W.M.; Lyon, G.J.; et al. Tourette Syndrome Association International Consortium for Genetics: Tourette Syndrome Association International Consortium for Genetics Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry 2015, 72, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Melchior, L.; Bertelsen, B.; Debes, N.M.; Groth, C.; Skov, L.; Mikkelsen, J.D.; Brøndum-Nielsen, K.; Tümer, Z. Microduplication of 15q13.3 and Xq21.31 in a family with Tourette syndrome and comorbidities. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2013, 162, 825–831. [Google Scholar] [CrossRef]
- Nickel, K.; Tebartz van Elst, L.; Domschke, K.; Gläser, B.; Stock, F.; Endres, D.; Maier, S.; Riedel, A. Heterozygous deletion of SCN2A and SCN3A in a patient with autism spectrum disorder and Tourette syndrome: A case report. BMC Psychiatry 2018, 2, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poot, M. Connecting the CNTNAP2 Networks with Neurodevelopmental Disorders. Mol. Syndr. 2015, 6, 7–22. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Liu, Y.; Zarrei, M.; Tong, W.; Dong, R.; Wang, Y.; Zhang, H.; Yang, X.; MacDonald, J.R.; Uddin, M.; et al. Association of IMMP2L deletions with autism spectrum disorder: A trio family study and meta-analysis. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2017, 177, 93–100. [Google Scholar] [CrossRef]
- The Brainstorm Consortium. Analysis of shared heritability in common disorder of the brain. Science 2018, 22, 360. [Google Scholar]
- McHugh, M. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Intelligence Scale for Children; The Psychological Corporation: New York, NY, USA, 1949. [Google Scholar]
- Sparrow, S.; Balla, D.; Cicchetti, D. Vineland Adaptive Behavior Scales; Giunti OS: Firenze, Italy, 2003. [Google Scholar]
- Robertson, M.; Eapen, V. The National Hospital Interview Schedule for the assessment of Gilles de la Tourette Syndrome. Int. J. Methods Psychiatr. Res. 1996, 6, 203–226. [Google Scholar] [CrossRef]
- Leckman, J.F.; Riddle, M.A.; Hardin, M.T.; Ort, S.I.; Swartz, K.L.; Stevenson, J.; Cohen, D.J. The Yale Global Tic Severity Scale: Initial testing of a clinician-rated scale of tic severity. J. Am. Acad. Child Adolesc. Psychiatry 1989, 28, 566–573. [Google Scholar] [CrossRef]
- Scahill, L.; Riddle, M.A.; McSwiggin-Hardin, M.; Ort, S.I.; King, R.A.; Goodman, W.K.; Cicchetti, D.; Leckman, J.F. Children’s Yale-Brown Obsessive Compulsive Scale: Reliability and validity. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 844–852. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Lecavalier, L.; Snow, A.V.; Norris, M. Autism spectrum disorders and intellectual disability. In International Handbook of Autism and Pervasive Developmental Disorders; Matson, J.L., Sturmey, P., Eds.; Springer: New York, NY, USA, 2011; pp. 37–51. [Google Scholar]
- Rizzo, R.; Curatolo, P.; Gulisano, M.; Virzì, M.; Arpino, C.; Robertson, M.M. Disentangling the effects of Tourette syndrome and attention deficit hyperactivity disorder on cognitive and behavioral phenotypes. Brain Dev. 2007, 29, 413–420. [Google Scholar] [CrossRef]
- Eddy, C.M.; Cavanna, A.E.; Gulisano, M.; Calì, P.; Robertson, M.M.; Rizzo, R. The effects of comorbid obsessive-compulsive disorder and attention-deficit hyperactivity disorder on quality of life in tourette syndrome. J. Neuropsychiatry Clin. Neurosci. 2012, 24, 458–462. [Google Scholar] [CrossRef]
- Toichi, M.; Kamio, Y.; Okada, T.; Sakihama, M.; Youngstrom, E.A.; Findling, R.L.; Yamamoto, K. A lack of self-consciousness in autism. Am. J. Psychiatry 2002, 159, 1422–1424. [Google Scholar] [CrossRef]
- Kadesjö, B.; Gillberg, C. Tourette’s disorder: Epidemiology and comorbidity in primary school children. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 548–555. [Google Scholar] [CrossRef]
- Khalifa, N.; von Knorring, A.L. Psychopathology in a Swedish population of school children with tic disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1346–1353. [Google Scholar] [CrossRef]
- Cederlund, M. Autism Mental Status Examination (AMSE): A valid instrument in the evaluation of pre-school children with suspected autism spectrum aisorders? J. Autism Dev. Disord. 2019, 49, 2965–2979. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Wu, H.; Lee, P.H.; Tsetsos, F.; Davis, L.K.; Yu, D.; Lee, S.H.; Dalsgaard, S.; Haavik, J.; Barta, C.; et al. Cross-disorder GWAS meta-analysis for Attention Deficit/Hyperactivity Disorder, Autism Spectrum Disorder, Obsessive Compulsive Disorder, and Tourette Syndrome. bioRxiv 2019, 770222. [Google Scholar] [CrossRef] [Green Version]
- Rapanelli, M.; Frick, L.R.; Pittenger, C. The Role of Interneurons in Autism and Tourette Syndrome. Trends Neurosci. 2017, 40, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Gulisano, M.; Barone, R.; Alaimo, S.; Ferro, A.; Pulvirenti, A.; Cirnigliaro, L.; Di Silvestre, S.; Martellino, S.; Maugeri, N.; Milana, M.C.; et al. Disentangling Restrictive and Repetitive Behaviors and Social Impairments in Children and Adolescents with Gilles de la Tourette Syndrome and Autism Spectrum Disorder. Brain Sci. 2020, 10, 308. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GTS (n = 975) | |
|---|---|
| Male (M)/female (F) | 813:162 |
| Age of onset (tic) | 6.4 ± 2.4 |
| Mean age | 12.4 ± 6.4 |
| Clinical subgroups (%) | |
| Pure GTS | 12.3 (n = 120) |
| GTS + ASD | 8.9 (n = 87) |
| GTS + OCD | 45.5 (n = 443) |
| GTS + ADHD | 33.3 (n = 325) |
| Measures | GTS Only | GTS + ASD | GTS + ADHD | GTS + OCD |
|---|---|---|---|---|
| IQ | ||||
| TIQ | 92.2 (17.8) | 74.7 (14.8) | 82.5 (9.2) | 94.9 (17.6) |
| VIQ | 92.9 (18.6) | 73.9 (12.5) | 83.7 (10.7) | 95.8 (18.5) |
| PIQ | 92.6 (7.5) | 70.73 (9.4) | 80.8 (8.7) | 93.4 (19.1) |
| YGTSS | 15.2 (7.6) | 11.8 (2.3) | 17.4 (6.9) | 17.8 (6.5) |
| CY-BOCS | 6.7 (6.1) | 14.7 (9.8) | 10.1 (6.8) | 14.8 (7.1) |
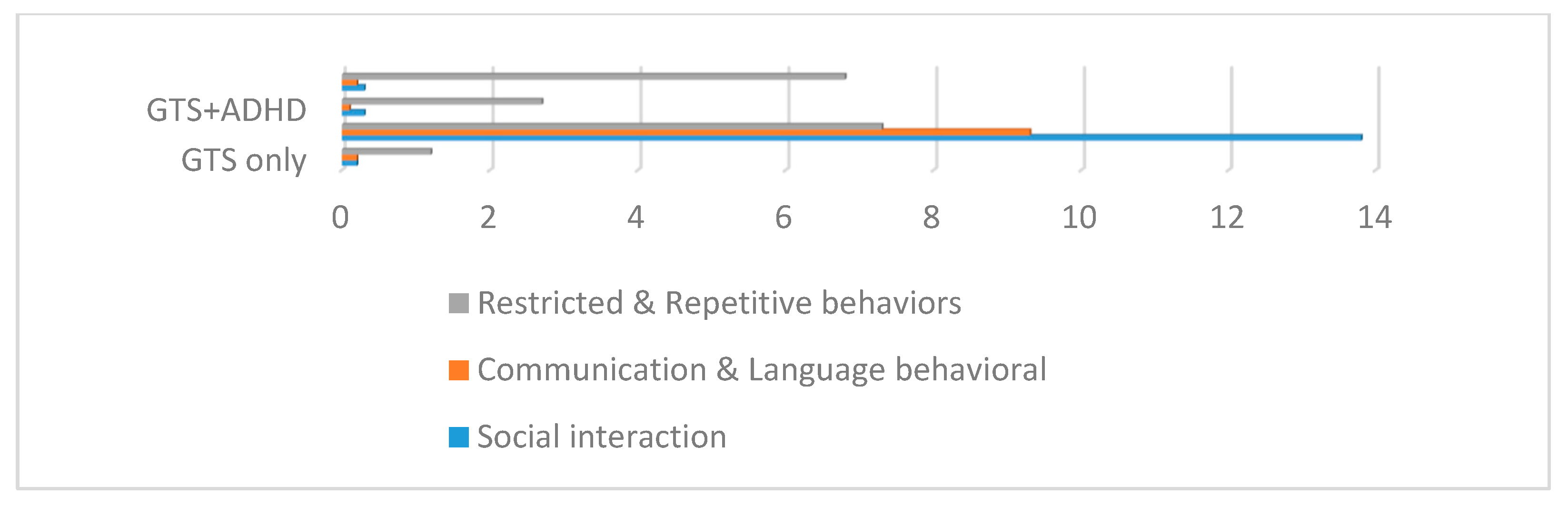
| ADI-R | ||||
| Social interaction | 0.2 (0.9) | 13.8 (6.8) | 0.3 (0.8) | 0.3 (0.9) |
| Communication and language behavioral | 0.2 (0.6) | 9.3 (5.1) | 0.1 (0.2) | 0.2 (0.6) |
| Restricted and repetitive behaviors | 1.2 (2.2) | 7.3 (3.6) | 2.7 (3.7) | 6.8 (3.1) |
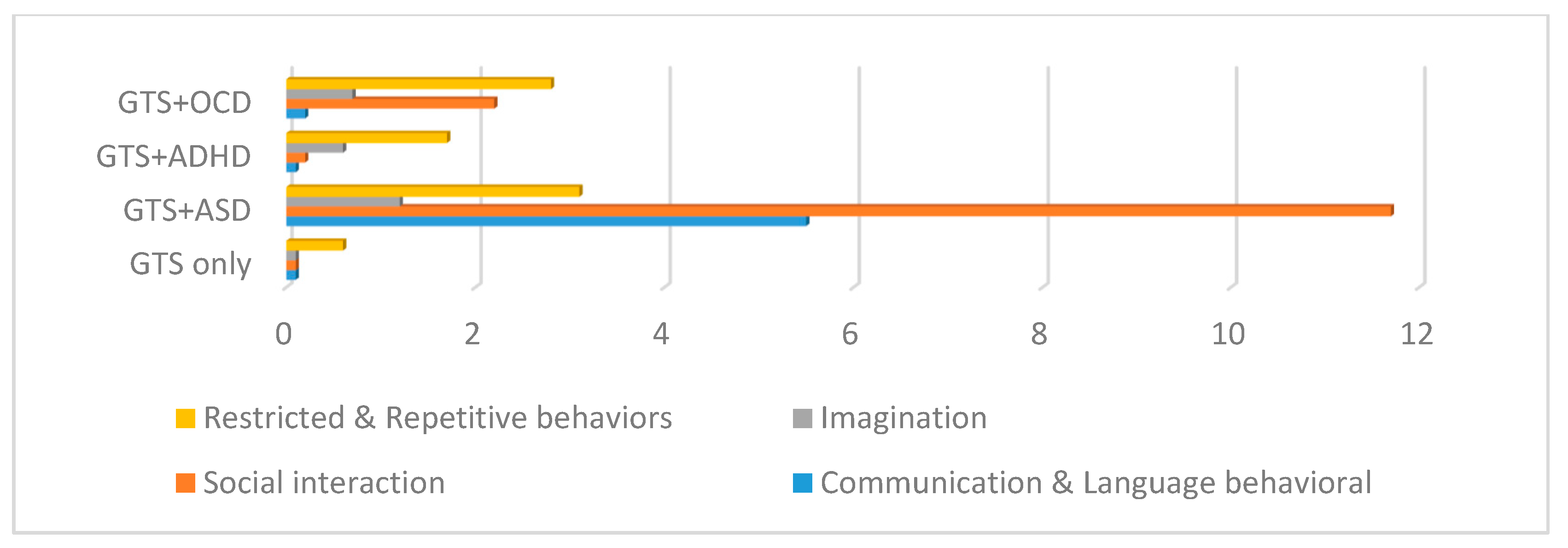
| ADOS | ||||
| Communication and language behavioral | 0.1 (0.3) | 5.5 (1.2) | 0.1 (0.2) | 0.2 (0.4) |
| Social interaction | 0.1 (0.6) | 11.7 (5.6) | 0.2 (0.2) | 2.2 (0.7) |
| Imagination | 0.1 (0.1) | 1.2 (1.9) | 0.6 (0.2) | 0.7 (0.4) |
| Restricted and repetitive behaviors | 0.6 (1.1) | 3.1 (2.2) | 1.7 (1.5) | 2.8(1.3) |
| p-Value | t-Value | |
|---|---|---|
| GTS + ASD vs. GTS only | 0.000 | 7.221 |
| GTS + ASD vs. GTS + ADHD | 0.000 | 5.061 |
| GTS + ASD vs. GTS + OCD | 0.910 | 0.112 |
| GTS only vs. GTS + ADHD | 0.000 | 4.808 |
| GTS only vs. GTS + OCD | 0.000 | 11.407 |
| GTS + OCD vs. GTS + ADHD | 0.000 | 9.226 |
| p-Value | t-Value | |
|---|---|---|
| ADOS | 0.085 | 1.723 |
| ADI-R | 0.181 | 1.337 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulisano, M.; Barone, R.; Mosa, M.R.; Milana, M.C.; Saia, F.; Scerbo, M.; Rizzo, R. Incidence of Autism Spectrum Disorder in Youths Affected by Gilles de la Tourette Syndrome Based on Data from a Large Single Italian Clinical Cohort. Brain Sci. 2020, 10, 812. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110812
Gulisano M, Barone R, Mosa MR, Milana MC, Saia F, Scerbo M, Rizzo R. Incidence of Autism Spectrum Disorder in Youths Affected by Gilles de la Tourette Syndrome Based on Data from a Large Single Italian Clinical Cohort. Brain Sciences. 2020; 10(11):812. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110812
Chicago/Turabian StyleGulisano, Mariangela, Rita Barone, Maria Rita Mosa, Maria Chiara Milana, Federica Saia, Miriam Scerbo, and Renata Rizzo. 2020. "Incidence of Autism Spectrum Disorder in Youths Affected by Gilles de la Tourette Syndrome Based on Data from a Large Single Italian Clinical Cohort" Brain Sciences 10, no. 11: 812. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110812