Functional and Structural Connectome Features for Machine Learning Chemo-Brain Prediction in Women Treated for Breast Cancer with Chemotherapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Clinical Characteristics
2.2. MRI Acquisition
2.3. MRI Image Analysis
2.4. Graph Theoretical Analysis
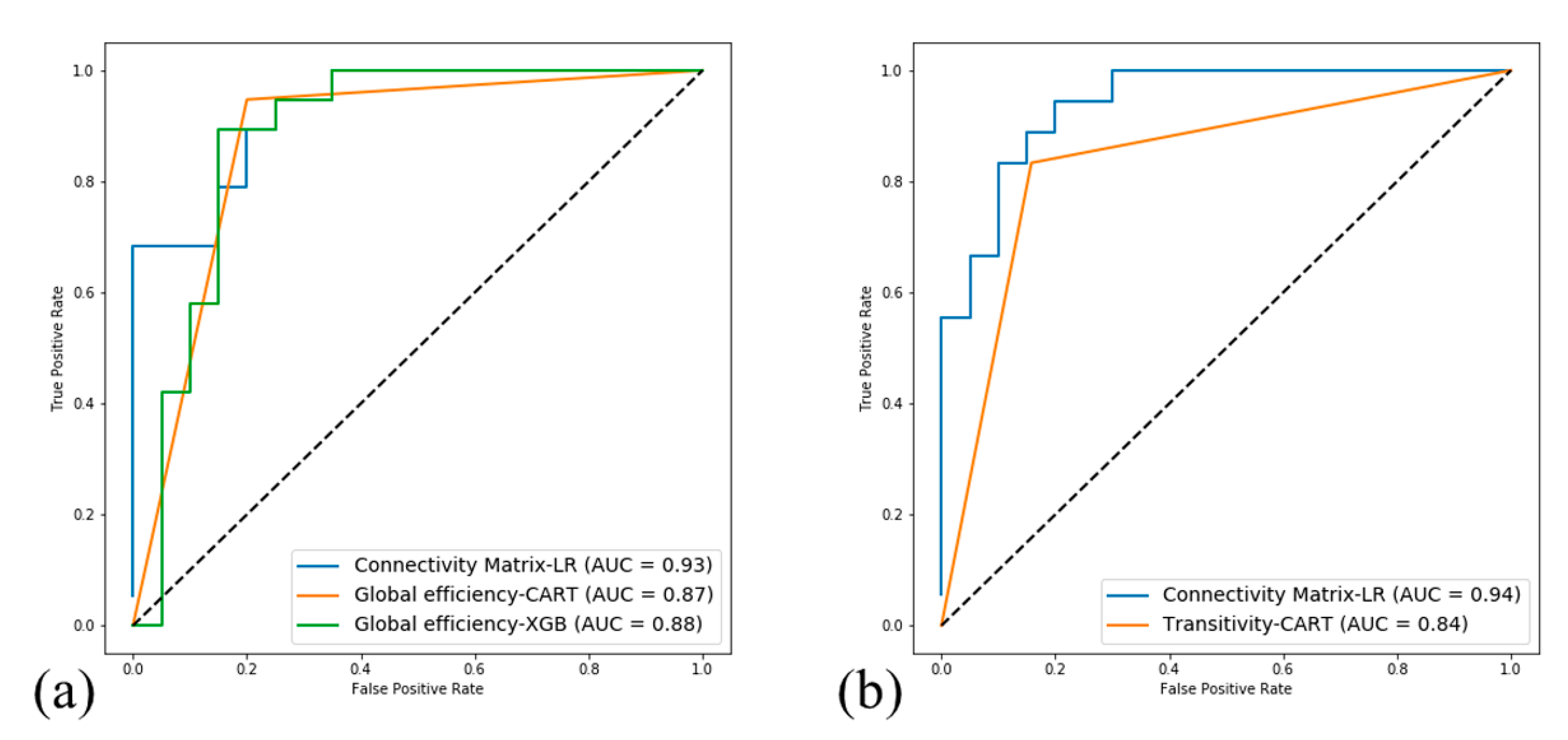
2.5. Machine Learning Algorithms
3. Results
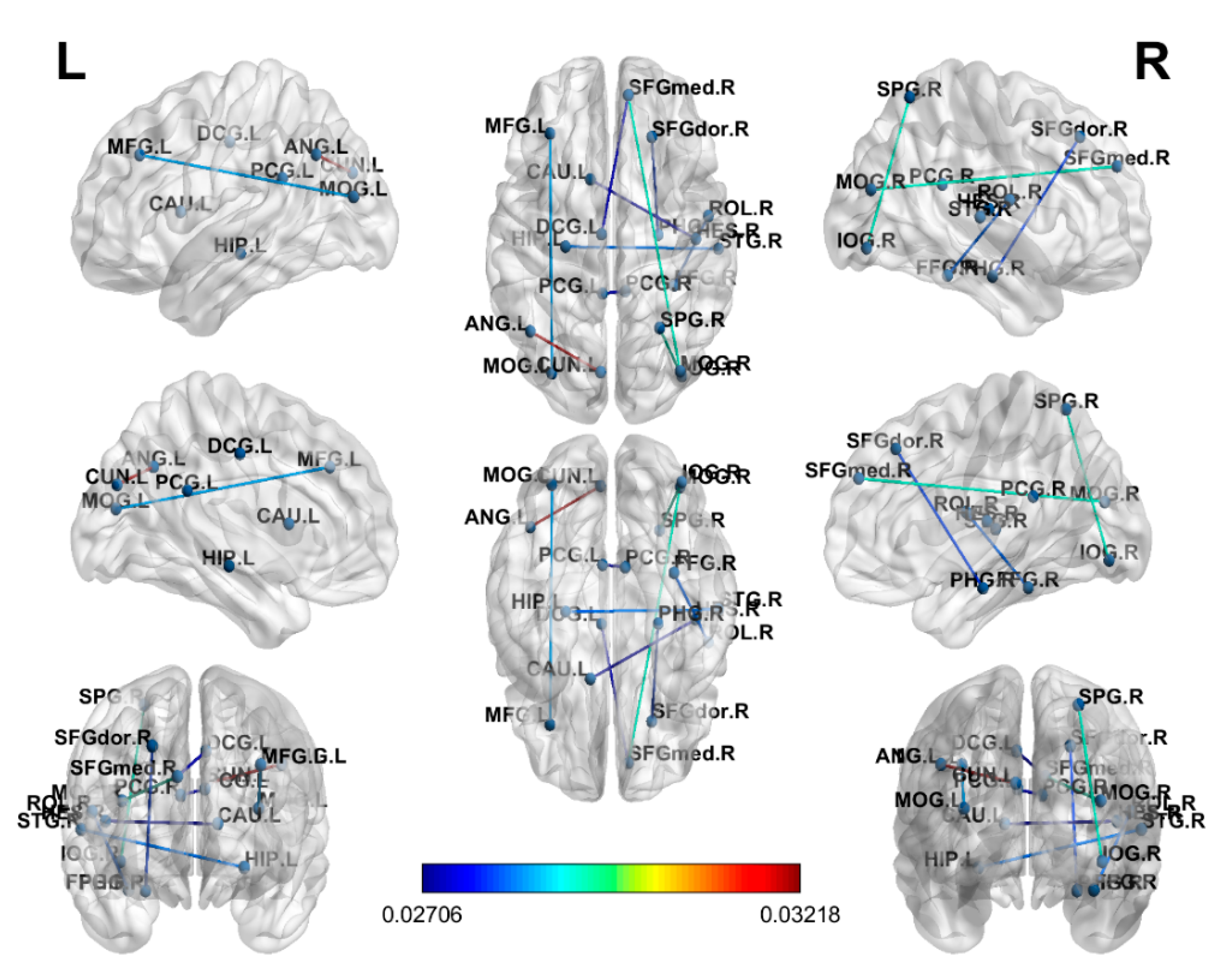
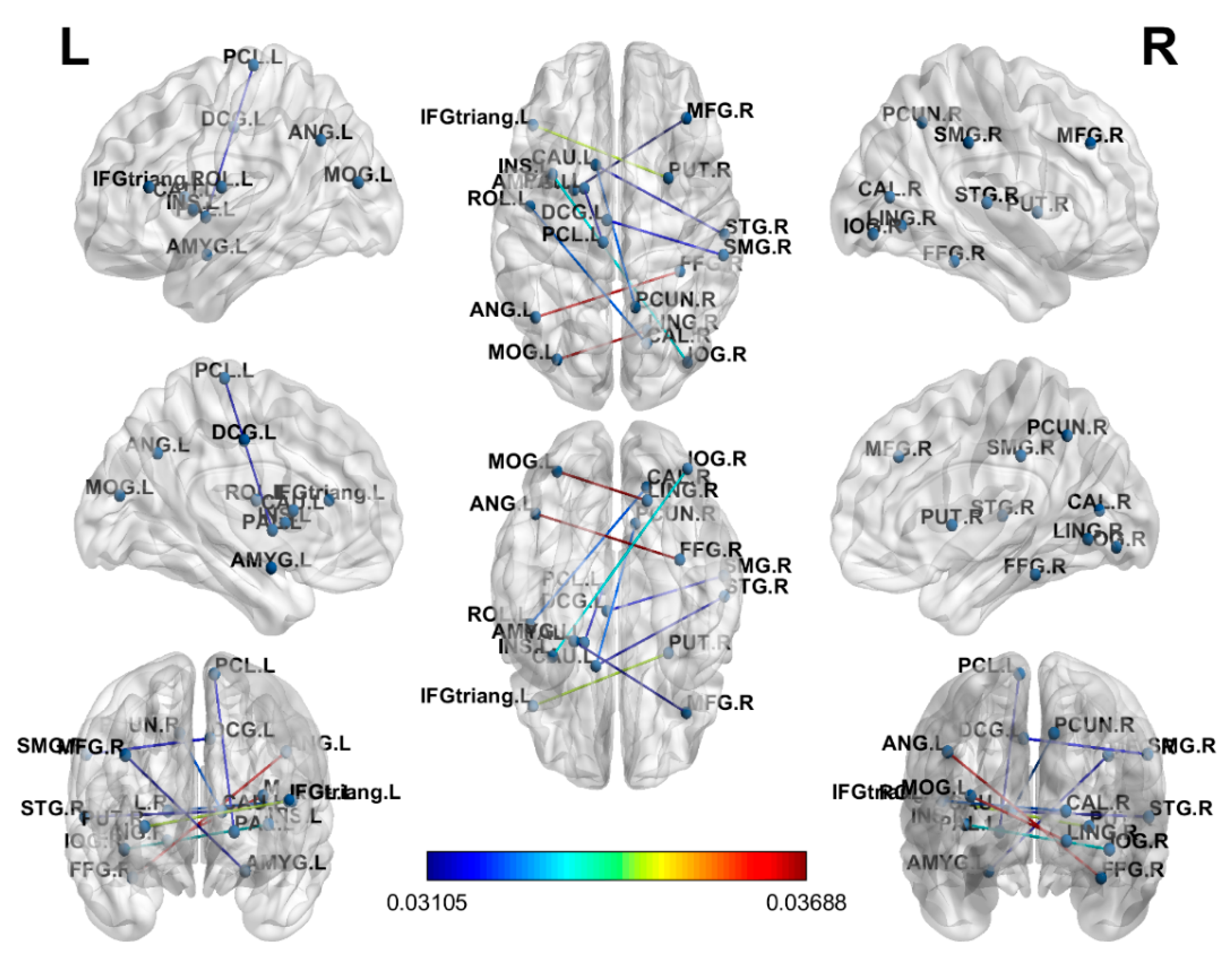
3.1. Connectome Analysis
3.2. Topological Coefficients Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AAL | automated anatomical labeling |
| ABIDE | Autism Brain Imaging Data Exchange |
| AUC | areas under curve |
| BC | breast cancer |
| C | mean clustering coefficient |
| C+ | breast cancer survivors |
| C− | nonchemotherapy-treated breast cancer survivors |
| CAMS-R | Cognitive and Affective Mindfulness Scale-Revised |
| CART | decision tree classifier |
| DL | deep learning |
| EEG | electroencephalogram |
| FACT | fiber assignment by continuous tracking |
| FACT-Cog | Functional Assessment of Cancer Therapy-Cognitive Function |
| GQI | generalized q-sampling imaging |
| HC | healthy control |
| IES-R | Impact of Event Scale–Revised |
| L | characteristic path length |
| LOOCV | leave-one-out cross-validation |
| LR | logistic regression |
| MDD | major depressive disorder |
| MMSE | Mini-Mental State Examination |
| MNI | Montreal Neurological Institute |
| NQA | normalized quantitative anisotropy |
| RF | random forest |
| ROI | region of interest |
| rs-fMRI | resting-state functional magnetic resonance imaging |
| SPM | Statistical Parametric Mapping |
| SVM | support vector machine |
| XGB | xgboost |
| γ | normalized clustering coefficient |
| λ | normalized characteristic path length |
| σ | small-worldness index |
References
- Hislop, J.O. Yes, Virginia, Chemo Brain is Real. Clin. Breast Cancer 2015, 15, 87–89. [Google Scholar] [CrossRef]
- Moore, H.C. An overview of chemotherapy-related cognitive dysfunction, or ‘chemobrain’. Oncology 2014, 28, 797–804. [Google Scholar] [PubMed]
- Hermelink, K. Chemotherapy and Cognitive Function in Breast Cancer Patients: The So-Called Chemo Brain. J. Natl. Cancer Inst. Monogr. 2015, 2015, 67–69. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, L.J.; McCreath, G.A.; Komeylian, Z.; Rich, J.B. Cognitive impairment in breast cancer survivors treated with chemotherapy depends on control group type and cognitive domains assessed: A multilevel meta-analysis. Neurosci. Biobehav. Rev. 2017, 83, 417–428. [Google Scholar] [CrossRef]
- Asher, A. Cognitive dysfunction among cancer survivors. Am. J. Phys. Med. Rehabil. 2011, 90 (Suppl. S1), S16–S26. [Google Scholar] [CrossRef]
- Reuter-Lorenz, P.A.; Cimprich, B. Cognitive function and breast cancer: Promise and potential insights from functional brain imaging. Breast Cancer Res. Treat. 2013, 137, 33–43. [Google Scholar] [CrossRef]
- Słowik, A.J.; Jabłoński, M.J.; Michałowska-Kaczmarczyk, A.M.; Jach, R. Evaluation of quality of life in women with breast cancer, with particular emphasis on sexual satisfaction, future perspectives and body image, depending on the method of surgery. Psychiatr. Pol. 2017, 51, 871–888. [Google Scholar] [CrossRef]
- Horowitz, T.S.; Suls, J.; Trevino, M. A Call for a Neuroscience Approach to Cancer-Related Cognitive Impairment. Trends Neurosci. 2018, 41, 493–496. [Google Scholar] [CrossRef]
- Chen, V.C.H.; Lin, T.Y.; Yeh, D.C.; Chai, J.W.; Weng, J.C. Predicting chemo-brain in breast cancer survivors using multiple MRI features and machine-learning. Magn. Reson. Med. 2019, 81, 3304–3313. [Google Scholar] [CrossRef]
- Yeh, F.C.; Wedeen, V.J.; Tseng, W.Y. Generalized q-sampling imaging. IEEE Trans. Med. Imaging 2010, 29, 1626–1635. [Google Scholar]
- Wise, T.; Radua, J.; Nortje, G.; Cleare, A.J.; Young, A.H.; Arnone, D. Voxel-Based Meta-Analytical Evidence of Structural Disconnectivity in Major Depression and Bipolar Disorder. Biol. Psychiatry 2016, 79, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, S.; Bhatia, M.S.; Bhargava, S.K.; Kumari, R.; Chandra, S. A Diffusion Tensor Imaging Study Using a Voxel-Based Analysis, Region-of-Interest Method to Analyze White Matter Abnormalities in First-Episode, Treatment-Naive Major Depressive Disorder. J. Neuropsychiatry Clin. Neurosci. 2016, 28, 131–137. [Google Scholar] [CrossRef]
- Beaulieu, C. The basis of anisotropic water diffusion in the nervous system—A technical review. NMR Biomed. 2002, 15, 435–455. [Google Scholar] [CrossRef]
- Roine, T.; Jeurissen, B.; Perrone, D.; Aelterman, J.; Leemans, A.; Philips, W.; Sijbers, J. Isotropic non-white matter partial volume effects in constrained spherical deconvolution. Front. Neuroinform. 2014, 8, 28. [Google Scholar] [CrossRef]
- Roine, T.; Jeurissen, B.; Perrone, D.; Aelterman, J.; Philips, W.; Leemans, A.; Sijbers, J. Informed constrained spherical deconvolution (iCSD). Med. Image Anal. 2015, 24, 269–281. [Google Scholar] [CrossRef]
- Vos, S.B.; Jones, D.K.; Viergever, M.A.; Leemans, A. Partial volume effect as a hidden covariate in DTI analyses. NeuroImage 2011, 55, 1566–1576. [Google Scholar] [CrossRef]
- Kesler, S.R.; Watson, C.L.; Blayney, D.W. Brain network alterations and vulnerability to simulated neurodegeneration in breast cancer. Neurobiol. Aging 2015, 36, 2429–2442. [Google Scholar] [CrossRef] [Green Version]
- Bassett, D.S.; Bullmore, E. Small-World Brain Networks. Neuroscientist 2006, 12, 512–523. [Google Scholar] [CrossRef]
- Kesler, S.R.; Wefel, J.S.; Hosseini, S.M.H.; Cheung, M.; Watson, C.L.; Hoeft, F. Default mode network connectivity distinguishes chemotherapy-treated breast cancer survivors from controls. Proc. Natl. Acad. Sci. USA 2013, 110, 11600–11605. [Google Scholar] [CrossRef] [Green Version]
- Saccà, V.; Sarica, A.; Novellino, F.; Barone, S.; Tallarico, T.; Filippelli, E.; Granata, A.; Chiriaco, C.; Bossio, R.B.; Valentino, P.; et al. Evaluation of machine learning algorithms performance for the prediction of early multiple sclerosis from resting-state FMRI connectivity data. Brain Imaging Behav. 2019, 13, 1103–1114. [Google Scholar] [CrossRef]
- Brown, C.J.; Miller, S.P.; Booth, B.G.; Zwicker, J.G.; Grunau, R.E.; Synnes, A.R.; Chau, V.; Hamarneh, G. Predictive connectome subnetwork extraction with anatomical and connectivity priors. Comput. Med. Imaging Graph. 2019, 71, 67–78. [Google Scholar] [CrossRef]
- Shen, C.-Y.; Chen, V.C.-H.; Yeh, D.-C.; Huang, S.-L.; Zhang, X.-R.; Chai, J.-W.; Huang, Y.-H.; Chou, M.-C.; Weng, J.-C. Association of functional dorsal attention network alterations with breast cancer and chemotherapy. Sci. Rep. 2019, 9, 104. [Google Scholar] [CrossRef]
- Li, T.-Y.; Chen, V.C.-H.; Yeh, D.-C.; Huang, S.-L.; Chen, C.-N.; Chai, J.-W.; Chen, C.C.-C.; Weng, J.-C. Investigation of chemotherapy-induced brain structural alterations in breast cancer patients with generalized q-sampling MRI and graph theoretical analysis. BMC Cancer 2018, 18, 1211. [Google Scholar] [CrossRef]
- Huang, H.-H.; Dai, J.-G.; Liang, Y. Clinical Drug Response Prediction by Using a Lq Penalized Network-Constrained Logistic Regression Method. Cell. Physiol. Biochem. 2018, 51, 2073–2084. [Google Scholar] [CrossRef]
- Iyama, Y.; Nakaura, T.; Katahira, K.; Nagayama, Y.; Oda, S.; Utsunomiya, D.; Yamashita, Y. Development and validation of a logistic regression model to distinguish transition zone cancers from benign prostatic hyperplasia on multi-parametric prostate MRI. Eur. Radiol. 2017, 27, 3600–3608. [Google Scholar] [CrossRef]
- Murphy, R.F.; Plumblee, L.; Barfield, W.B.; Murphy, J.S.; Fuerstenau, N.; Spence, D.D.; Kelly, D.M.; Dow, M.A.; Mooney, J.F. Septic Arthritis of the Hip—Risk Factors Associated With Secondary Surgery. J. Am. Acad. Orthop. Surg. 2019, 27, 321–326. [Google Scholar] [CrossRef]
- Sankari, E.S.; Manimegalai, D. Predicting membrane protein types using various decision tree classifiers based on various modes of general PseAAC for imbalanced datasets. J. Theor. Biol. 2017, 435, 208–217. [Google Scholar] [CrossRef]
- Dong, F.; Li, Q.; Xu, D.; Xiu, W.; Zeng, Q.; Zhu, X.; Xu, F.; Jiang, B.; Zhang, M. Differentiation between pilocytic astrocytoma and glioblastoma: A decision tree model using contrast-enhanced magnetic resonance imaging-derived quantitative radiomic features. Eur. Radiol. 2018, 29, 3968–3975. [Google Scholar] [CrossRef]
- Hyun, C.M.; Kim, H.P.; Lee, S.M.; Lee, S.; Seo, J.K. Deep learning for undersampled MRI reconstruction. Phys. Med. Biol. 2018, 63, 135007. [Google Scholar] [CrossRef]
- Masuda, T.; Nakaura, T.; Funama, Y.; Okimoto, T.; Sato, T.; Higaki, T.; Noda, N.; Imada, N.; Baba, Y.; Awai, K. Machine-learning integration of CT histogram analysis to evaluate the composition of atherosclerotic plaques: Validation with IB-IVUS. J. Cardiovasc. Comput. Tomogr. 2019, 13, 163–169. [Google Scholar] [CrossRef]
- Maeta, K.; Nishiyama, Y.; Fujibayashi, K.; Gunji, T.; Sasabe, N.; Iijima, K.; Naito, T.; Lopez, B.; Bian, J.; Billis, A.; et al. Prediction of Glucose Metabolism Disorder Risk Using a Machine Learning Algorithm: Pilot Study. JMIR Diabetes 2018, 3, e10212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, B.; Liu, P.; Lin, J.; Deng, L.; Hu, K.; Zheng, H. Predicting Invasive Disease-Free Survival for Early Stage Breast Cancer Patients Using Follow-Up Clinical Data. IEEE Trans. Biomed. Eng. 2019, 66, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Collins, D.L.; Neelin, P.; Peters, T.M.; Evans, A.C. Automatic 3D Intersubject Registration of MR Volumetric Data in Standardized Talairach Space. J. Comput. Assist. Tomogr. 1994, 18, 192–205. [Google Scholar] [CrossRef] [PubMed]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A Functional Connectivity Toolbox for Correlated and Anticorrelated Brain Networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef] [Green Version]
- Behzadi, Y.; Restom, K.; Liau, J.; Liu, T.T. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage 2007, 37, 90–101. [Google Scholar] [CrossRef] [Green Version]
- Bullmore, E.T.; Bassett, D.S. Brain graphs: Graphical models of the human brain connectome. Annu. Rev. Clin. Psychol. 2011, 7, 113–140. [Google Scholar] [CrossRef] [Green Version]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. NeuroImage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Van Wijk, B.C.M.; Stam, C.J.; Daffertshofer, A. Comparing Brain Networks of Different Size and Connectivity Density Using Graph Theory. PLoS ONE 2010, 5, e13701. [Google Scholar] [CrossRef]
- Hosseini, S.M.H.; Hoeft, F.; Kesler, S.R. GAT: A Graph-Theoretical Analysis Toolbox for Analyzing Between-Group Differences in Large-Scale Structural and Functional Brain Networks. PLoS ONE 2012, 7, e40709. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Hunter, J.D. Matplotlib: A 2D Graphics Environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Xia, M.; Wang, J.; He, Y. BrainNet Viewer: A Network Visualization Tool for Human Brain Connectomics. PLoS ONE 2013, 8, e68910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; He, X.; Tao, L.; Cheng, H.; Li, J.; Zhang, J.; Qiu, B.; Yu, Y.; Wang, K. The attention network changes in breast cancer patients receiving neoadjuvant chemotherapy: Evidence from an arterial spin labeling perfusion study. Sci. Rep. 2017, 7, 42684. [Google Scholar] [PubMed] [Green Version]
- McDonald, B.C.; Conroy, S.K.; Ahles, T.A.; West, J.D.; Saykin, A.J. Alterations in Brain Activation During Working Memory Processing Associated With Breast Cancer and Treatment: A Prospective Functional Magnetic Resonance Imaging Study. J. Clin. Oncol. 2012, 30, 2500–2508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deprez, S.; Amant, F.; Yigit, R.; Porke, K.; Verhoeven, J.; Stock, J.V.D.; Smeets, A.; Christiaens, M.-R.; Leemans, A.; Van Hecke, W.; et al. Chemotherapy-induced structural changes in cerebral white matter and its correlation with impaired cognitive functioning in breast cancer patients. Hum. Brain Mapp. 2011, 32, 480–493. [Google Scholar] [CrossRef] [PubMed]
- Van Der Burgh, H.K.; Schmidt, R.; Westeneng, H.-J.; De Reus, M.A.; Berg, L.H.V.D.; Heuvel, M.P.V.D. Deep learning predictions of survival based on MRI in amyotrophic lateral sclerosis. NeuroImage Clin. 2017, 13, 361–369. [Google Scholar]
- Su, S.; Yu, D.; Cheng, J.; Chen, Y.; Zhang, X.; Guan, Y.; Li, Y.; Bi, Y.; Xue, T.; Lu, X.; et al. Decreased Global Network Efficiency in Young Male Smoker: An EEG Study during the Resting State. Front. Psychol. 2017, 8, 1605. [Google Scholar] [CrossRef] [Green Version]
- Chen, V.C.-H.; Shen, C.-Y.; Liang, S.H.-Y.; Li, Z.-H.; Hsieh, M.-H.; Tyan, Y.-S.; Lu, M.-L.; Lee, Y.; McIntyre, R.S.; Weng, J.-C. Assessment of brain functional connectome alternations and correlation with depression and anxiety in major depressive disorders. PeerJ 2017, 5, 3147. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep Learning for Brain MRI Segmentation: State of the Art and Future Directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [Green Version]
- Gong, E.; Pauly, J.M.; Wintermark, M.; Zaharchuk, G. Deep learning enables reduced gadolinium dose for contrast-enhanced brain MRI. J. Magn. Reson. Imaging 2018, 48, 330–340. [Google Scholar] [CrossRef]
- Tezcan, K.C.; Baumgartner, C.F.; Luechinger, R.; Pruessmann, K.P.; Konukoglu, E. MR Image Reconstruction Using Deep Density Priors. IEEE Trans. Med Imaging 2018, 38, 1633–1642. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Jang, H.; Kijowski, R.; Bradshaw, T.; McMillan, A.B. Deep Learning MR Imaging–based Attenuation Correction for PET/MR Imaging. Radiology 2018, 286, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-H.; Chen, V.C.-H.; Hsieh, C.-C.; Weng, Y.-P.; Hsu, Y.-T.; Hsiao, H.-P.; Wang, W.-K.; Chen, H.-M.; Weng, J.-C.; Wu, S.-I.; et al. Subjective and objective cognitive functioning among patients with breast cancer: Effects of chemotherapy and mood symptoms. Breast Cancer 2020. [Google Scholar] [CrossRef]
- Nugent, B.D.; Ren, D.; Bender, C.M.; Rosenzweig, M. The Impact of Age and Adjuvant Chemotherapy Modifications on Survival Among Black Women With Breast Cancer. Clin. Breast Cancer 2019, 19, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Scherling, C.S.; Collins, B.; MacKenzie, J.; Bielajew, C.; Smith, A.M. Pre-Chemotherapy Differences in Visuospatial Working Memory in Breast Cancer Patients Compared to Controls: An fMRI Study. Front. Hum. Neurosci. 2011, 5, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Breast Cancer Patients after Chemotherapy (n = 19) | Healthy Controls (n = 20) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min | Max | Mean | SD | Min | Max | p-Value | Effect Sizes | |
| Age (years) | 44.84 | 6.56 | 32 | 55 | 49.95 | 2.61 | 43 | 55 | 0.004 | −1.03 |
| Education (years) | 14.00 | 2.61 | 9 | 16 | 13.2 | 2.26 | 9 | 16 | 0.274 | 0.33 |
| MMSE | 28.11 | 1.29 | 26 | 30 | 28.35 | 1.46 | 25 | 30 | 0.583 | −0.17 |
| CAMS-R | 33.63 | 4.91 | 24 | 42 | 33.85 | 3.94 | 27 | 40 | 0.879 | −0.05 |
| IES-R | 14.26 | 23.91 | 0 | 64 | 8.60 | 12.57 | 0 | 38 | 0.366 | 0.30 |
| FACT-Cog | ||||||||||
| Perceived cognitive impairments | 53.26 | 10.49 | 34 | 67 | 59.45 | 6.88 | 47 | 70 | 0.035 | −0.70 |
| Comments from others | 14.00 | 2.47 | 7 | 16 | 14.30 | 1.84 | 11 | 16 | 0.669 | −0.14 |
| Perceived cognitive abilities | 17.21 | 5.78 | 2 | 26 | 18.00 | 5.49 | 0 | 24 | 0.664 | −0.14 |
| Impact on quality of life | 11.63 | 3.52 | 4 | 16 | 14.10 | 2.05 | 10 | 16 | 0.010 | −0.86 |
| Total score | 102.37 | 19.24 | 53 | 131 | 112.50 | 12.31 | 90 | 134 | 0.056 | −0.63 |
| Breast cancer stage | n | % | n | % | ||||||
| 0 | 0 | 0 | N/A | N/A | ||||||
| I | 2 | 10.53 | N/A | N/A | ||||||
| II | 14 | 73.68 | N/A | N/A | ||||||
| III | 3 | 15.79 | N/A | N/A | ||||||
| IV | 0 | 0 | N/A | N/A | ||||||
| Chemotherapeutic drugs (Taxotere and Epirubicin) | 19 | 100.00 | N/A | N/A | ||||||
| Radiation therapy | 4 | 21.05 | N/A | N/A | ||||||
| Hormonal treatment | 1 | 5.26 | N/A | N/A | ||||||
| Menopausal | 5 | 26.32 | 5 | 25.00 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, V.C.-H.; Lin, T.-Y.; Yeh, D.-C.; Chai, J.-W.; Weng, J.-C. Functional and Structural Connectome Features for Machine Learning Chemo-Brain Prediction in Women Treated for Breast Cancer with Chemotherapy. Brain Sci. 2020, 10, 851. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110851
Chen VC-H, Lin T-Y, Yeh D-C, Chai J-W, Weng J-C. Functional and Structural Connectome Features for Machine Learning Chemo-Brain Prediction in Women Treated for Breast Cancer with Chemotherapy. Brain Sciences. 2020; 10(11):851. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110851
Chicago/Turabian StyleChen, Vincent Chin-Hung, Tung-Yeh Lin, Dah-Cherng Yeh, Jyh-Wen Chai, and Jun-Cheng Weng. 2020. "Functional and Structural Connectome Features for Machine Learning Chemo-Brain Prediction in Women Treated for Breast Cancer with Chemotherapy" Brain Sciences 10, no. 11: 851. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110851