1. Introduction
Cerebral palsy (CP) is a motor syndrome that results from a permanent, non-progressive injury in the developing brain. The clinical picture is shaped according to the time of occurrence of the lesion, the location and severity of the neural alterations, life experience, and activity level of the subject. CP includes a broad number of movement and postural disorders. The severity, the type of motor impairment, and the associated deficiencies (e.g., communication, intellectual capacity, behavioral problems) are highly variable. Overall prevalence has remained stable over the past 40 years, despite progress in antenatal and perinatal care. In France, around 125,000 people are affected [
1].
Postural control is a prerequisite for activities of daily living (ADL). Generally, upholding a stable postural balance against gravity is challenging and requires a refined network organization, i.e., accurate connections between sensory inputs, central CNS integration, and muscle effector outputs. Dynamic postural control includes feedforward or anticipatory postural adjustments that predict disturbances and produce preprogrammed responses to maintain stability, and feedback or compensatory postural adjustments activated by sensory events following loss of postural balance. Both mechanisms are centrally driven to optimize postural balance [
2,
3]. Fine-tuning of postural muscle contraction during specific motor tasks is inefficient in most individuals with CP, since flawed co-activation of antagonist muscles as well as difficulties in temporal organization and amplitude modulation of the muscles are present [
4]. In patients with CP, one of the main clinical dysfunctions consists of the failure to activate the postural muscles in the right order and to fine-tune them [
5]. Other neurological issues limit the control of balance in patients with CP, such as spasticity, hyperactive stretch reflexes, and dyskinesia [
6].
Neurorehabilitation of postural balance in patients with CP is rather complex, as the clinical shapes among these patients are extremely heterogeneous. Generally speaking, unstable support surfaces induce increased activation of the trunk musculature and a constant muscle response to adjust the posture against instability. As a result, patients do not need to carry out complex exercise routines to benefit from trunk rehabilitation on these surfaces [
7,
8]. Hippotherapy can be considered an unstable support therapy that generates up to 100 three-dimensional smooth physical trunk and girdle micromovements per minute, mimicking the patient’s body during walking [
9]. Moreover, the therapy is released in a particularly appealing and friendly ecosystem where children are generally confident and highly motivated. This general panorama plays a key role in optimizing brain plasticity through a key enriched environment for the promotion of functional recovery of postural balance [
10].
From the effector point of view, when balance of a seated person is challenged, postural stability is restored via activation of the major trunk muscles. Even during quiet sitting, tonic muscle activity can be observed in all major trunk muscles, but tonic activity is not sufficient to resist perturbations. Additional phasic muscle activity, which is symmetrical across the body, is necessary to slow the movement of the trunk and bring it back to a vertical position. However, each trunk muscle responds to multiple, but not all, perturbation directions. In spite of the crucial role of those mechanisms for postural balance, the muscular response to seated perturbations and its characteristics are not fully understood or described in health or disease states [
11,
12].
Assessing postural control during functional tasks is important in order to understand balance adjustments adopted by CP individuals in their daily lives. Since hippotherapy might support the regularization of sitting postural balance [
10], we aimed to explore the role of the pelvic girdle in this regularization by choosing two key muscles above and below this main anatomical structure, namely, the rectus abdominis (RA) and the adductor magnus (AM). RA participates in sitting stability by controlling the backward–forward sway of the trunk [
13]. AM is both a dynamic stabilizer of the pelvis and femur as well as a prime mover of the femur into adduction and has the potential to affect postural control of the pelvis while sitting [
14,
15]. Since one of the main neurophysiological alterations of the CP neuromotor system is the activation and fine-tuning of the postural muscles, we focused on the recording of the electrical activity of these muscles by means of surface electromyography (EMG). We deliberately chose to analyze these two non-antagonistic postural muscle groups, nevertheless with opposite actions in pelvic positioning (retroversion and anteversion, respectively). Indeed, the complex multilayered arrangement of extensor muscles of the lumbar region (multifidus, longissimus thoracis, iliocostalis lumborum) makes the interpretation of muscle activation through surface EMG during postural tasks difficult [
16]. On the other hand, even if the individual hip adductor muscles are quite close together at the medial side of the proximal thigh (in particular adductor magnus, gracilis, and adductor longus), a good reliability of surface EMG can be demonstrated when recording the activity of the AM muscle [
17]. In addition, AM plays a role in hip extension, contributing to the stabilization of the pelvic girdle during riding. In fact, the hip extension moment arm length of AM changes with the hip angle and is a more effective hip extensor than either the hamstrings or gluteus maximus when the hip is flexed.
In this pilot, our objective was to strengthen our previous hypothesis regarding the reinforcement of postural balance [
10] by drawing a general picture of the changes in the contractile properties of key postural muscles through hippotherapy. We characterized the initial EMG patterns in the time and frequency domains and their modification during a 12-week hippotherapy program for neurorehabilitation with the aim of paving the way for future clinical trials in the neurorehabilitation field.
4. Discussion
In the present study, we analyzed the behavior of two muscle groups contributing to the stabilization of the pelvis in a sitting position through control of anteversion and retroversion of the pelvic girdle, stabilization of the backward–forward sway of the trunk, and anchorage of the pelvis while sitting [
14,
15]. The level and duration of muscle activation throughout execution of a postural task was reflected in the myoelectric characteristics that were recorded and displayed by the use of electromyography. EMG signals, which are complex signals, are deeply influenced by the anatomical and physiological properties of muscles and their alteration, as noticed in patients with CP [
34,
35,
40]. EMG is a common tool often used to study muscle activity with regard to posture and movement, since motion shapes electromyographic recordings [
31]. However, very few studies investigating electrical muscle activity and hippotherapy have been published in the scientific literature to date, with even less focusing on patients with CP. The few available studies address the findings from a qualitative point of view, with none carrying out a quantitative analysis of EMG signals from either the time or the frequency domains [
18,
44,
45,
46,
47]. We focused here on the electrical activity of muscle measured during dynamic postural balance while sitting through surface EMG. We firstly verified the reliability of inter-day EMG measurements in order to validate the methodology, then we analyzed the myoelectrical activation patterns and their evolution with respect to treatment during (i) a short-term interval, i.e., comparing the beginning with the end of each session, and (ii) throughout the whole neurorehabilitation process, i.e., comparing the initial features and their variations after six and twelve weeks of treatment.
A first crucial feature of our results concerned the inter-day reliability of the EMG signal. We noticed that absolute submaximal surface EMG amplitudes obtained during sitting on an unstable support surface (horseback), without external aids, had a substantial inter-day reliability on both measured muscles, as shown by the intraclass correlation coefficient values [
48]. Each patient was expected to have some degree of variation in their movements between trials, with CP patients in particular showing significant alterations in muscle control. These data support the assertion that the intersession reliability of our model was sufficient to allow longitudinal analysis of postural muscle behavior in response to hippotherapy.
With this crucial issue verified, a second interesting feature of our results was the symmetry of the muscle action. Previous studies on patients with CP described that impaired muscle tone and, more precisely, spasticity is typically not uniformly spread throughout the trunk and limbs of affected patients. This was stated as a major cause of abnormal body asymmetry between homologous muscle groups, leading to significant postural balance impairment [
18,
44]. In the present study, some minimal differences were noticed in both the time and frequency domains between the right and the left RA and AM muscles. However, no particular trend emerged, and the differences observed were almost completely attenuated throughout the session, i.e., the left–right asymmetry noticed at the beginning of the treatment (left mRMS was 15% higher than right mRMS, but non-significant) faded at six and twelve weeks. It was conceivable from a physiological point of view that the dynamic smooth solicitation of the postural muscles during hippotherapy harmonized their contractile tempo, in accordance with the postural enhancement during sitting that we usually notice in our patients from a clinical point of view.
Two EMG-related neuromuscular characteristics are usually underlined in patients with CP and can be, to a certain extent, connected to the noticed changes of the present study, helping to explain some of our results. Firstly, excessive EMG intensity of antagonist muscle co-activation during voluntary movement, which was not foreseen here, results from a need to stabilize joints or body segments and seems to be a useful compensatory strategy in patients with CP. Secondly, high-frequency components of the EMG spectrum mainly correspond to high-frequency content of action potentials generated by the fast fiber types (type IIa and IIx fibers) [
40]. The higher mean power frequency values observed at the beginning of the hippotherapy treatment probably indicated that during postural balance activities, relatively more fast-twitch muscle fibers were activated.
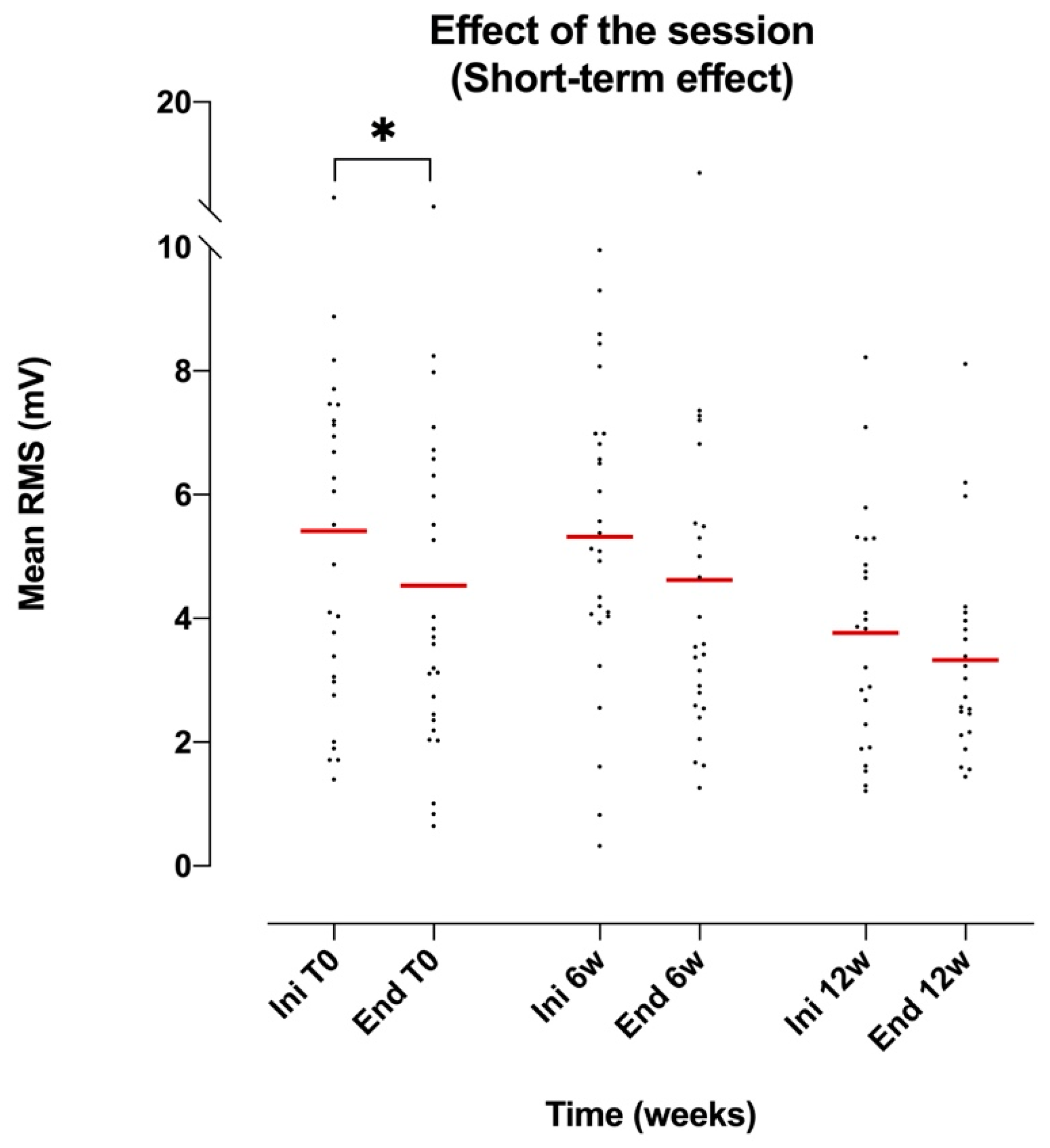
When analyzing muscle activation through mRMS, RA remained substantially equivalent (slight decline) during the session regardless of the time of treatment, i.e., at baseline and after six and twelve weeks of the beginning of the therapeutic protocol. The absence of a significant reduction in RMS during the 30-minute session was against the phenomenon of muscle fatigue. This was surprising when considering the relatively poor use of postural muscles in such patients with locomotion and sitting aids (e.g., wheelchairs, molded seats, back braces) and the potential low fatigue resistance of postural muscles in the context of an upper motor neuron lesion [
49,
50]. Nevertheless, when studying postural muscle activity, any possible change in muscle activation due to fatigue is unlikely to become apparent during recordings of short duration, i.e., 30 minutes. Indeed, the low levels of muscle activity reached in the postural tasks should result in a fatigue time of around several hours [
28].
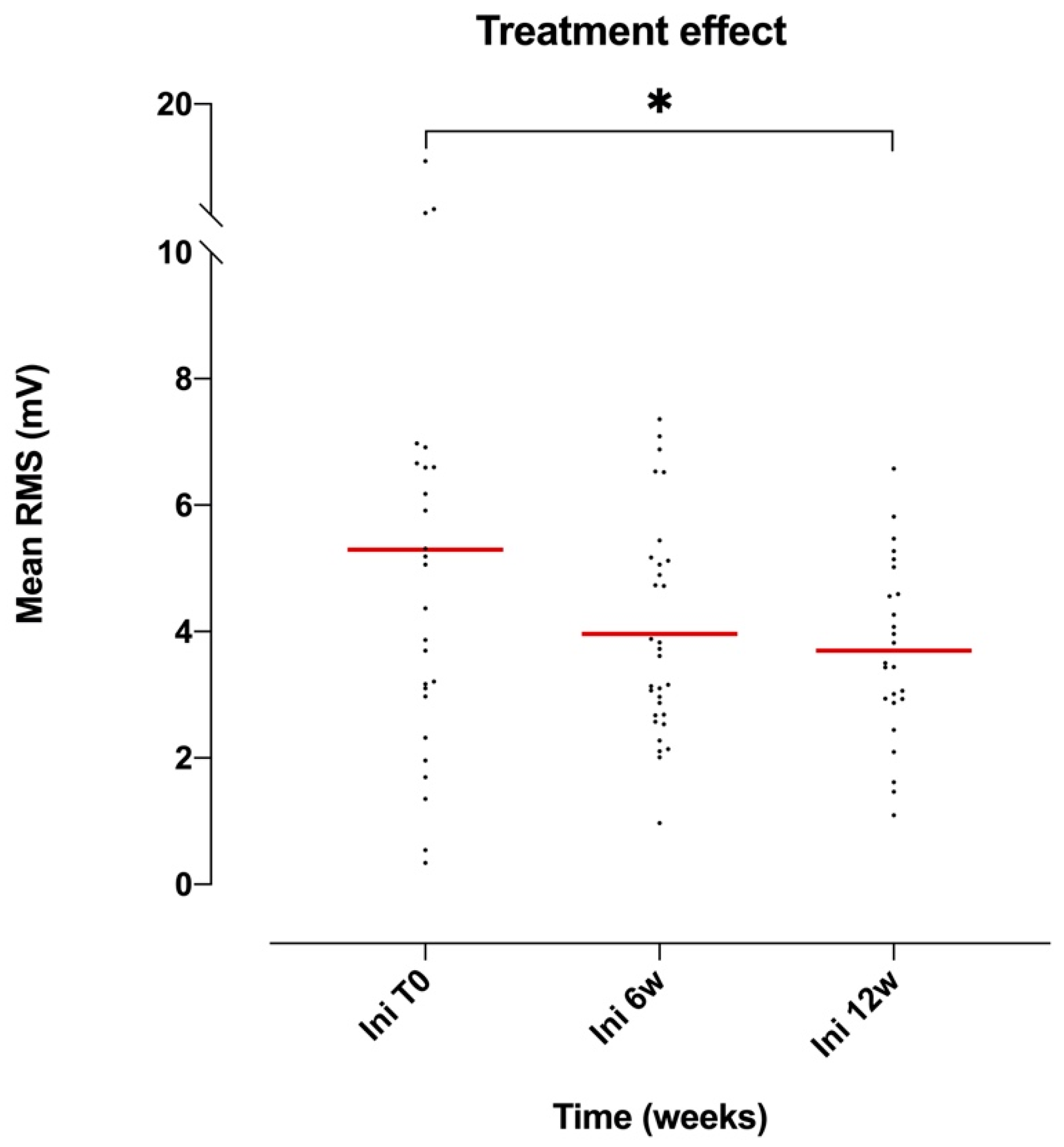
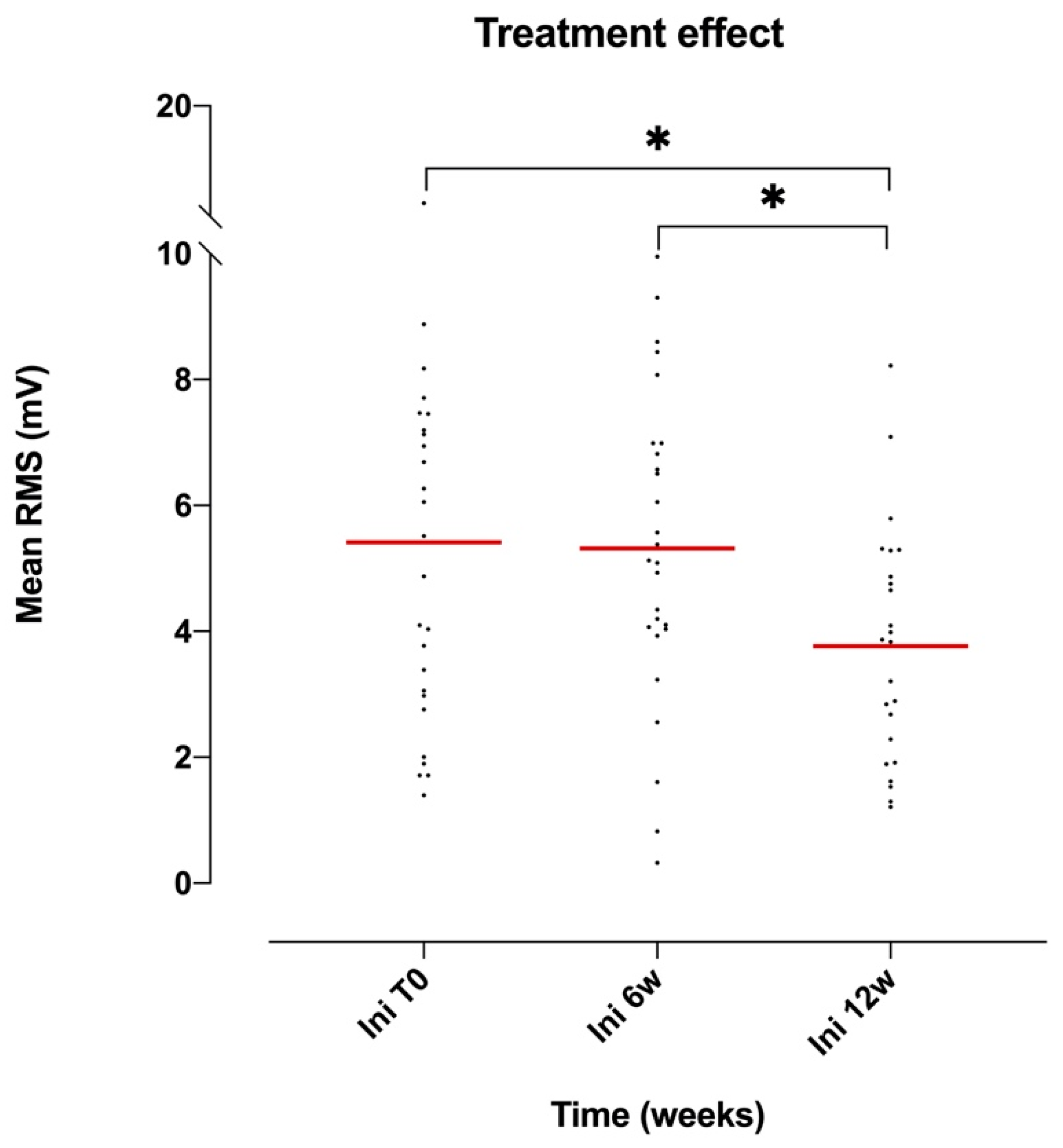
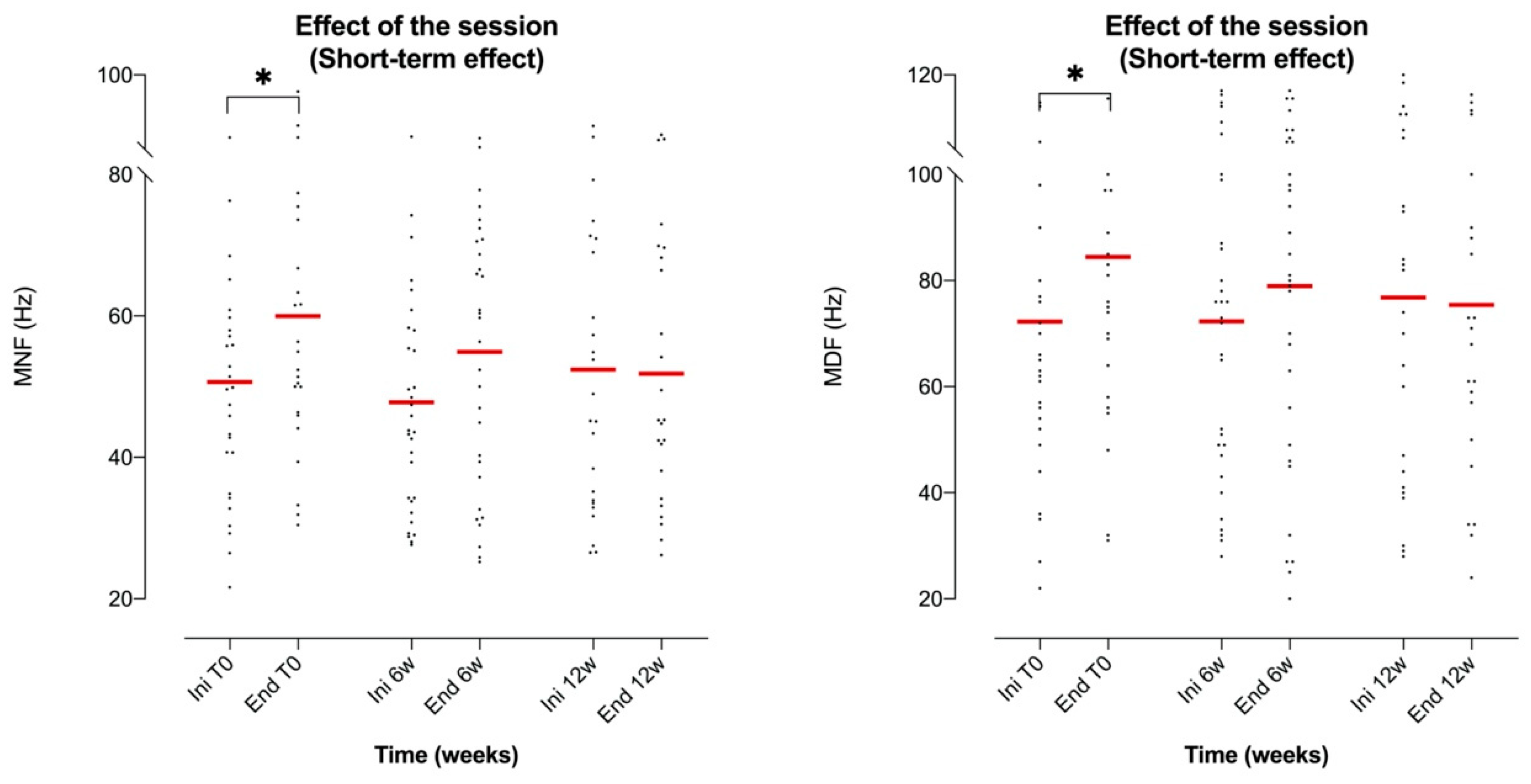
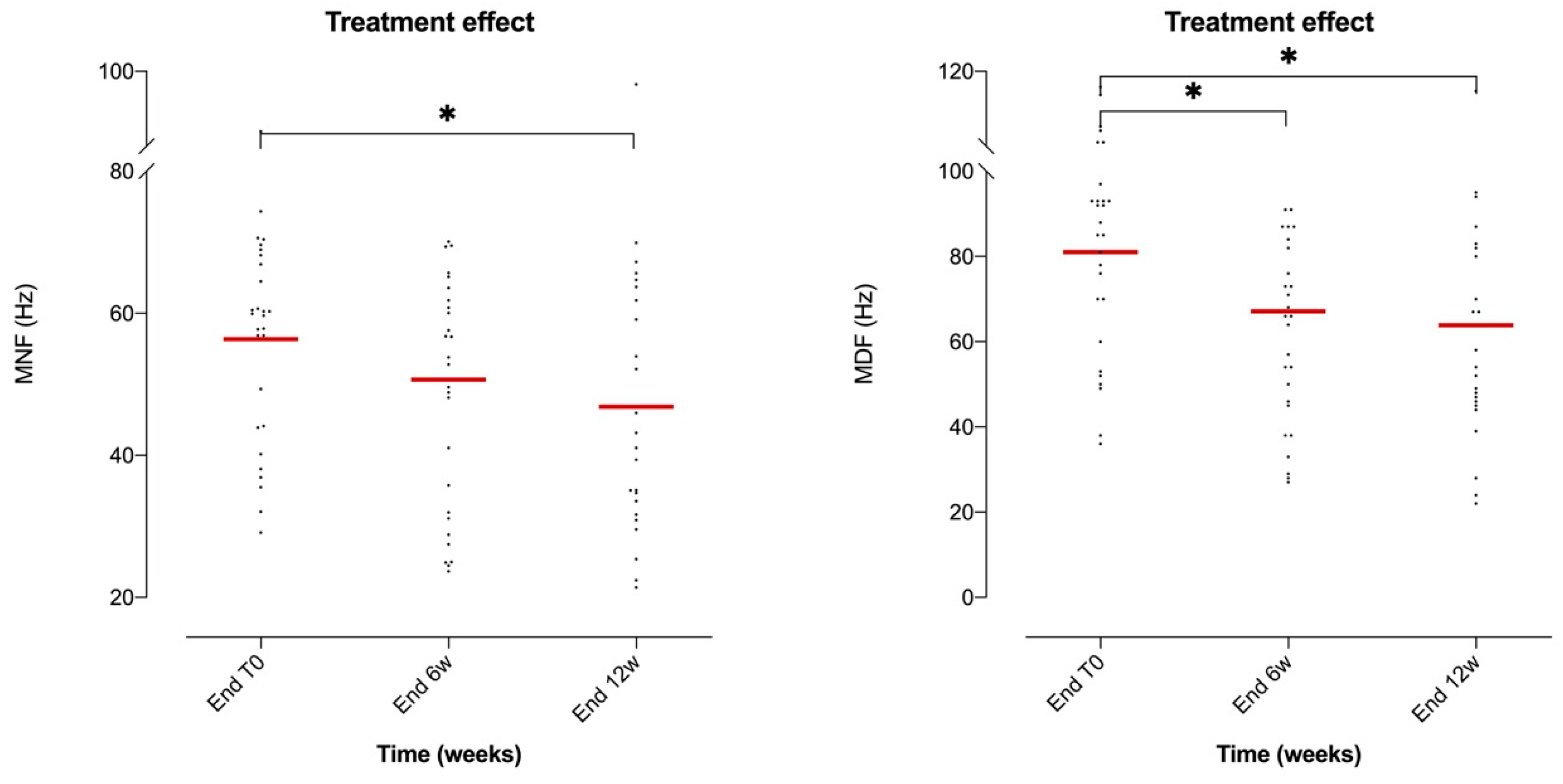
Interestingly, the RMS decreased continuously at six weeks (25%) and twelve weeks (30%) with respect to the initial mRMS values. This was coherent with a morphophysiological transformation of the muscle toward a less powerful but more fatigue-resistant muscle following the treatment protocol. Indeed, prolonged endurance training elicits several metabolic and morphological changes, including fast-to-slow fiber-type transformation [
51]. This hypothesis was coherent with the behavior of MNF and MDF, whose end-session values decreased gradually in relation to the time of treatment, consolidating the possibility of morphophysiological transformation of postural muscles through hippotherapy. However, it must be noted that after upper motor neuron damage there is marked atrophy and a pronounced shift in the contractile and histochemical profiles from slow-twitch to fast-twitch muscle fibers, with a reduction in oxidative potential and an increase in the fatigability of the affected muscles [
52].
Plasticity of skeletal muscle in response to metabolic and functional demands after injury or rehabilitation is driven by metabolic, biochemical, and mechanical properties depending on fiber type. Among the different properties, the myosin heavy chain isoform expression is the most frequently used classification criteria for fiber type [
53]. Due to its abundance and contractile significance, qualitative and quantitative changes in myosin and its isoforms exert significant effects on muscle strength and endurance. Human muscles contain three isoforms of myosin heavy chain, called type I, type IIa, and type IIx. A fiber can express a single myosin heavy chain isoform (a pure fiber) or co-express multiple isoforms (a hybrid fiber) [
54]. Type I fibers are slow-twitch fibers because of their slow speed of contraction and have a predominantly oxidative metabolism. Type IIx fibers are fast-twitch fibers because of their fast speed of contraction and mainly metabolize glucose via the glycolytic pathway. Type IIa fibers are intermediate fibers with fast contraction speed, but mixed (glycolytic/oxidative) metabolism [
55]. Exercise and disuse are the prime determinants of muscle fiber type transition, with the presence of hybrid fibers relating to a high degree of muscle plasticity [
56,
57]. Alterations in muscle fiber types affect the contractile, metabolic, and biochemical properties of the muscle. The diverse population of muscle fibers in a given muscle allows for various types of tasks, ranging from prolonged, low-intensity contractions (e.g., to maintain posture) to fast and strong maximal contractions. While the fiber type composition of a muscle is genetically determined, muscle plasticity is high and can be stimulated in response to environmental cues, such as targeted functional solicitation [
58].
The response to long-lasting physical submaximal exercise, e.g., during a twelve-week hippotherapy cycle, occurs within a very short time and may be linked to changes in concentrations of cellular metabolites which occur after chronic stimulation of skeletal muscle [
59]. Mitochondrial biogenesis (whereby mitochondria produce the energy currency of the cell and regulate cellular metabolism) coupled with improved functional parameters of mitochondria play a key role and are a typical response of endurance efforts [
60,
61]. For instance, it was shown that after only six weeks of training, exercise increases muscle mitochondrial content up to 50%–100% [
62]. Among the human muscle fiber types, the mitochondrial content is highest in type I fibers, followed by type IIa and type IIx fibers [
63,
64]. Mitochondrial changes are intensity-specific, since lower intensity exercise predominantly increases the mitochondrial volume in type I muscle fibers, while recruitment of mitochondria in type II fibers requires much higher intensity exercise [
65]. Altogether, endurance exercise positively modulates the overall process as part of muscle adaptation response toward enhanced metabolic and contractile capacity over a very short period of time. The muscle’s oxidative and regenerative potential is thus modulated by increasing the proportion of slow myosin and mitochondria of the muscle fibers [
62].
With respect to AM, most cases (11 out of 18 patients) exhibited a bilateral increase in muscle tone, revealed by a spasticity quoted as 2/2+ according to the modified Ashworth scale prior to the start of the protocol. Clinical manifestations corresponded to signs of stiffness as a result of stretch (for example, when adopting the sitting position on the horse). In such patients, the electromyographic activity was not only present during the dynamic phase of stretching, reflecting an archetypal stretch reflex, but persisted during the static phase. In our CP patients, locomotor impairment left the related muscles immobilized in a shortened position leading to muscle contracture, which is a cause of intrinsic hypertonia. Furthermore, muscle immobilization hampers the pivotal mechanism responsible for the development of spasticity, namely, reduction of post-activation depression [
66]. Hippotherapy has a direct effect on spasticity [
67], providing regular and individualized soft and slow-moving stretching movements along with the correct positioning of limbs. Consequently, a decrease in muscle activation (reflected by mRMS decline) was consistent with decreased muscle tension instead of the appearance of muscle fatigue, where a frequency shift resulted in lower frequencies. This was coherent with the concomitant decrease of MNF and MDF from six weeks after the beginning of the treatment. Nevertheless, the attenuation of muscle spasticity through hippotherapy in our patients was not the only phenomenon that explained the long-term decrease in mRMS and consequently muscle activation. Indeed, one could hypothesize that the significant decrease in mRMS at week 12 was partly the effect of decreased muscle tone and partly fast-to-slow fiber-type transformation consistent with the noticed EMG frequency domain characteristics (MNF and MDF), even if the latter could not be confirmed through our methodology and was beyond the scope of the study.
Taken together, the variations highlighted in the evolution of the myoelectric signal of the selected muscles as a result of the hippotherapy rehabilitation program can be explained in part by two main phenomena: on the one hand, a lesser need for activation of fast-twitch muscle fiber populations in order to stabilize posture and, on the other hand, the stimulation, to some extent, of muscle plasticity mechanisms, leading to a partial oxidative-like reconfiguration of the evaluated muscles.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}