Neck Pain- and Unsteadiness-Inducing Activities and their Relationship to the Presence, Intensity, Frequency, and Disability of Headaches

 , ,
, ,  ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
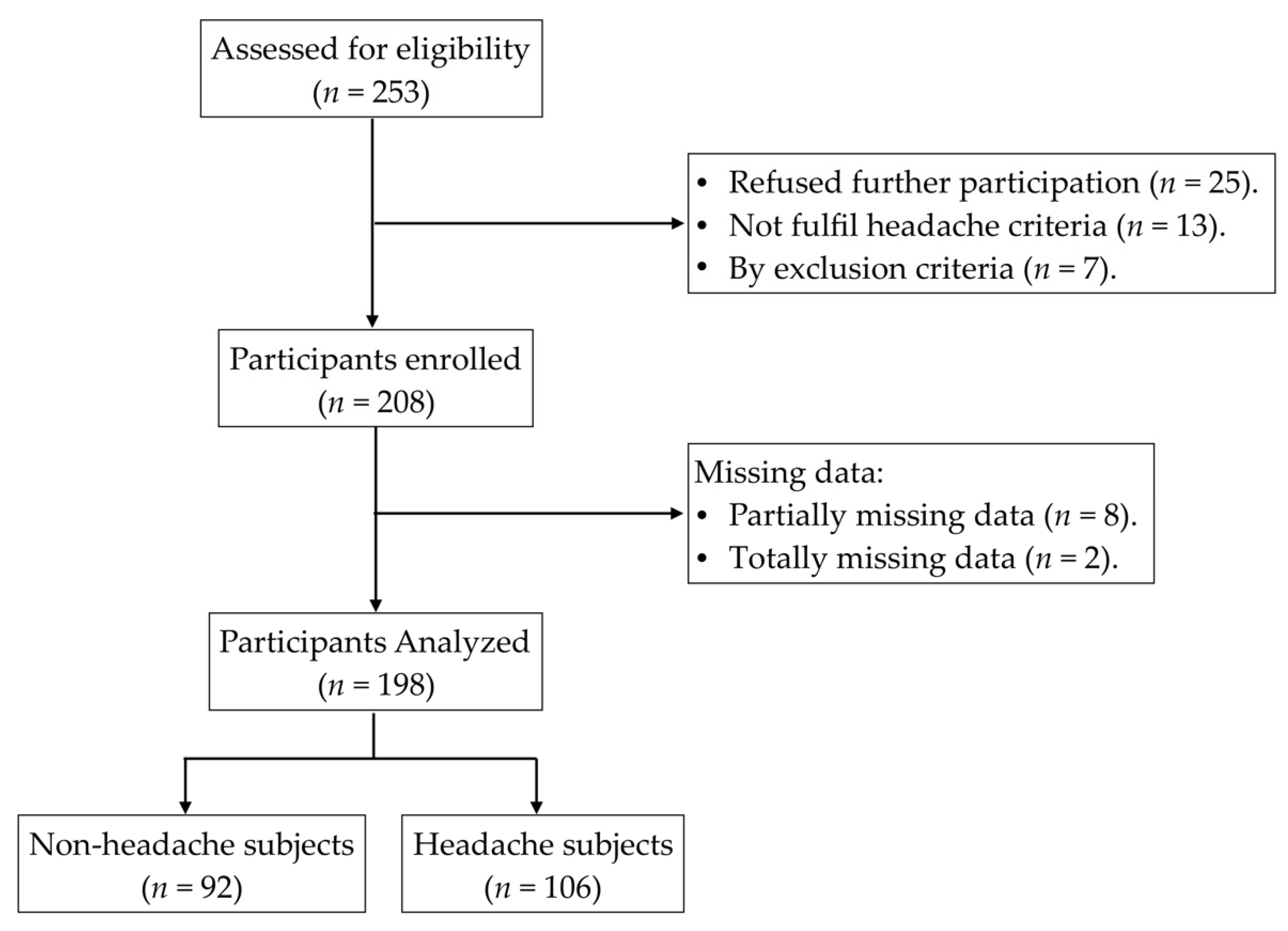
2.2. Participants
2.3. Measurements
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Woldeamanuel, Y.W.; Cowan, R.P. Migraine affects 1 in 10 people worldwide featuring recent rise: A systematic review and meta-analysis of community-based studies involving 6 million participants. J. Neurol. Sci. 2017, 372, 307–315. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef] [Green Version]
- Steiner, T.J.; Stovner, L.J.; Katsarava, Z.; Láinez, M.J.A.; Lampl, C.; Lantéri-Minet, M.; Rastenyte, D.; De La Torre, E.R.; Tassorelli, C.; Barre, J.; et al. The impact of headache in Europe: principal results of the Eurolight project. J. Headache Pain 2014, 15, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linde, M.; Gustavsson, A.; Stovner, L.J.; Steiner, T.J.; Barré, J.; Katsarava, Z.; Lainez, J.M.; Lampl, C.; Lantéri-Minet, M.; Rastenyte, D.; et al. The cost of headache disorders in Europe: The Eurolight project. Eur. J. Neurol. 2011, 19, 703–711. [Google Scholar] [CrossRef]
- Ashina, S.; Bendtsen, L.; Lyngberg, A.C.; Lipton, R.B.; Hajiyeva, N.; Jensen, R. Prevalence of neck pain in migraine and tension-type headache: A population study. Cephalalgia 2014, 35, 211–219. [Google Scholar] [CrossRef]
- Blaschek, A.; Milde-Busch, A.; Straube, A.; Schankin, C.; Langhagen, T.; Jahn, K.; Schröder, S.A.; Reiter, K.; Von Kries, R.; Heinen, F. Self-reported muscle pain in adolescents with migraine and tension-type headache. Cephalalgia 2012, 32, 241–249. [Google Scholar] [CrossRef] [Green Version]
- Uthaikhup, S.; Assapun, J.; Watcharasaksilp, K.; Jull, G.A. Effectiveness of physiotherapy for seniors with recurrent headaches associated with neck pain and dysfunction: A randomized controlled trial. Spine J. 2017, 17, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Bisdorff, A.; Andrée, C.; Vaillant, M.; Sándor, P.S. Headache-associated dizziness in a headache population: Prevalence and impact. Cephalalgia 2010, 30, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Anagnostou, E.; Gerakoulis, S.; Voskou, P.; Kararizou, E. Postural instability during attacks of migraine without aura. Eur. J. Neurol. 2018, 26, 319-e21. [Google Scholar] [CrossRef]
- Malińska, M.; Bugajska, J. The Influence of Occupational and Non-Occupational Factors on the Prevalence of Musculoskeletal Complaints in Users of Portable Computers. Int. J. Occup. Saf. Ergon. 2010, 16, 337–343. [Google Scholar] [CrossRef]
- Hansraj, K.K. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg. Technol. Int. 2014, 25, 277–279. [Google Scholar] [PubMed]
- Xavier, M.K.; Pitangui, A.C.; Silva, G.R.; Oliveira, V.M.; Beltrao, N.B.; Araujo, R.C. Prevalence of headache in adolescents and association with use of computer and videogames. Cien Saude Colet 2015, 20, 3477–3486. [Google Scholar] [CrossRef] [Green Version]
- McDougall, J.J. Arthritis and Pain. Neurogenic origin of joint pain. Arthritis Res. Ther. 2006, 8, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodick, D.; Silberstein, S. Central Sensitization Theory of Migraine: Clinical Implications. Headache J. Head Face Pain 2006, 46, S182–S191. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.H.; Drummond, P.D. The Role of the Trigemino Cervical Complex in Chronic Whiplash Associated Headache: A Cross Sectional Study. Headache J. Head Face Pain 2016, 56, 961–975. [Google Scholar] [CrossRef]
- STROBE initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [Green Version]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- González, T.; Balsa, A.; De Murieta, J.S.; Zamorano, E.; González, I.; Martin-Mola, E. Spanish version of the Northwick Park Neck Pain Questionnaire: Reliability and validity. Clin. Exp. Rheumatol. 2001, 19, 41–46. [Google Scholar]
- Renaud, J.; Márquez, G.; Padrón, L.V.; Rentería, L.V. Síntomas de inestabilidad corporal y enfermedad vestibular. Rev. Med. Inst. Mex. Seguro Soc. 2003, 41, 373–378. [Google Scholar]
- Rodríguez-Almagro, D.; Achalandabaso-Ochoa, A.; Rus, A.; Obrero-Gaitán, E.; Zagalaz-Anula, N.; Lomas-Vega, R. Validation of the Spanish version of the migraine disability assessment questionnaire (MIDAS) in university students with migraine. BMC Neurol. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Concato, J.; Peduzzi, P.; Holford, T.R.; Feinstein, A.R. Importance of events per independent variable in proportional hazards analysis. I. Background, goals, and general strategy. J. Clin. Epidemiol. 1995, 48, 1495–1501. [Google Scholar] [CrossRef]
- Calvo, M.O.; Domínguez, A.C. Unconditioned logistic regression and sample size: A bibliographic review. Rev. Esp. Salud Pública 2002, 76, 85–93. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Jiang, S.; Land, K.C. Multicollinearity in hierarchical linear models. Soc. Sci. Res. 2015, 53, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Blake, P.; Burstein, R. Emerging evidence of occipital nerve compression in unremitting head and neck pain. J. Headache Pain 2019, 20, 76–77. [Google Scholar] [CrossRef]
- Cachinero-Torre, A.; Díaz-Pulido, B.; Asúnsolo, Á. Relationship of the Lateral Rectus Muscle, the Supraorbital Nerve, and Binocular Coordination with Episodic Tension-Type Headaches Frequently Associated with Visual Effort. Pain Med. 2017, 18, 969–979. [Google Scholar] [CrossRef]
- Kristjansson, E.; Treleaven, J. Sensorimotor Function and Dizziness in Neck Pain: Implications for Assessment and Management. J. Orthop. Sports Phys. Ther. 2009, 39, 364–377. [Google Scholar] [CrossRef] [Green Version]
- Buisseret-Delmas, C.; Compoint, C.; Delfini, C.; Buisseret, P. Organisation of reciprocal connections between trigeminal and vestibular nuclei in the rat. J. Comp. Neurol. 1999, 409, 153–168. [Google Scholar] [CrossRef]
- Marano, E.; Marcelli, V.; Di Stasio, E.; Bonuso, S.; Vacca, G.; Manganelli, F.; Marciano, E.; Perretti, A. Trigeminal Stimulation Elicits a Peripheral Vestibular Imbalance in Migraine Patients. Headache J. Head Face Pain 2005, 45, 325–331. [Google Scholar] [CrossRef]
- Lampl, C.; Rapoport, A.M.; Levin, M.; Bräutigam, E. Migraine and episodic Vertigo: A cohort survey study of their relationship. J. Headache Pain 2019, 20, 33–35. [Google Scholar] [CrossRef] [Green Version]
- Valenza, M.C.; Valenza, G.; González-Jiménez, E.; De-La-Llave-Rincón, A.I.; Arroyo-Morales, M.; Fernández-De-Las-Peñas, C. Alteration in Sleep Quality in Patients with Mechanical Insidious Neck Pain and Whiplash-Associated Neck Pain. Am. J. Phys. Med. Rehabil. 2012, 91, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Cigarán-Méndez, M.; Fernández-Muñoz, J.; Navarro-Pardo, E.; Jiménez-Antona, C.; Paras-Bravo, P.; Alburquerque-Sendín, F.; Fernández-De-Las-Peñas, C. Gender differences in variables associated with sleep quality in chronic tension type headache. Women Health 2017, 58, 1037–1049. [Google Scholar] [CrossRef] [PubMed]
- Cevoli, S.; Giannini, G.; Favoni, V.; Pierangeli, G.; Cortelli, P. Migraine and sleep disorders. Neurol. Sci. 2012, 33, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.; Pavlović, J.M. Sleep Disorders and Migraine: Review of Literature and Potential Pathophysiology Mechanisms. Headache J. Head Face Pain 2018, 58, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Taylor, F.R. Tobacco, Nicotine, and Headache. Headache J. Head Face Pain 2015, 55, 1028–1044. [Google Scholar] [CrossRef]
- Rozen, T.D. Cluster Headache Clinical Phenotypes: Tobacco Nonexposed (Never Smoker and No Parental Secondary Smoke Exposure as a Child) versus Tobacco-Exposed: Results from the United States Cluster Headache Survey. Headache 2018, 58, 688–699. [Google Scholar] [CrossRef]
- Jiménez-Trujillo, I.; López-De-Andrés, A.; Del Barrio, J.L.; Hernández-Barrera, V.; Valero-De-Bernabé, M.; Jiménez-García, R. Gender Differences in the Prevalence and Characteristics of Pain in Spain: Report from a Population-Based Study. Pain Med. 2019, 20, 2349–2359. [Google Scholar] [CrossRef]
- Palacios-Cena, D.; Alonso-Blanco, C.; Hernandez-Barrera, V.; Carrasco-Garrido, P.; Jimenez-Garcia, R.; Fernandez-de-las-Penas, C. Prevalence of neck and low back pain in community-dwelling adults in Spain: An updated population-based national study (2009/10-2011/12). Eur. Spine J. 2015, 24, 482–492. [Google Scholar] [CrossRef]
- Whitehouse, W.; Agrawal, S. Management of children and young people with headache. Arch. Dis. Child. Educ. Pract. Ed. 2016, 102, 58–65. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Headache (n = 106) | Non-Headache (n = 92) | Total (n = 198) | |||||
|---|---|---|---|---|---|---|---|
| Categorical | F | % | F | % | F | % | |
| Gender | Male | 27 | 25.5 | 54 | 58.7 | 81 | 40.9 |
| Female | 79 | 74.5 | 38 | 41.3 | 117 | 59.1 | |
| Course | First course | 36 | 34.0 | 25 | 27.2 | 61 | 30.8 |
| Second course | 37 | 34.9 | 31 | 33.7 | 68 | 34.3 | |
| Third course | 9 | 8.5 | 16 | 17.4 | 25 | 12.6 | |
| Fourth course | 12 | 11.3 | 6 | 6.5 | 18 | 9.1 | |
| Master | 12 | 11.3 | 14 | 15.2 | 26 | 13.1 | |
| Continuous | Mean | SD | Mean | SD | Mean | SD | |
| Age (years) | 21.20 | 2.80 | 21.69 | 3.32 | 21.43 | 3.05 | |
| Height (cm) | 168.08 | 8.08 | 172.38 | 9.51 | 170.08 | 9.01 | |
| Weight (kg) | 64.04 | 11.22 | 69.88 | 13.92 | 66.75 | 12.85 | |
| BMI | 22.55 | 2.97 | 23.30 | 3.16 | 22.90 | 3.07 | |
| MIDAS | 5.01 | 9.05 | 0.80 | 2.43 | 3.06 | 7.13 | |
| Headache frequency a | 5.79 | 6.84 | 0.79 | 1.35 | 3.47 | 5.66 | |
| Headache intensity (0/10) a | 4.10 | 2.26 | 1.60 | 2.10 | 2.94 | 2.51 | |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | OR | 95% C.I. | p | OR | 95% C.I. | p | ||
| Inferior | Superior | Inferior | Superior | |||||
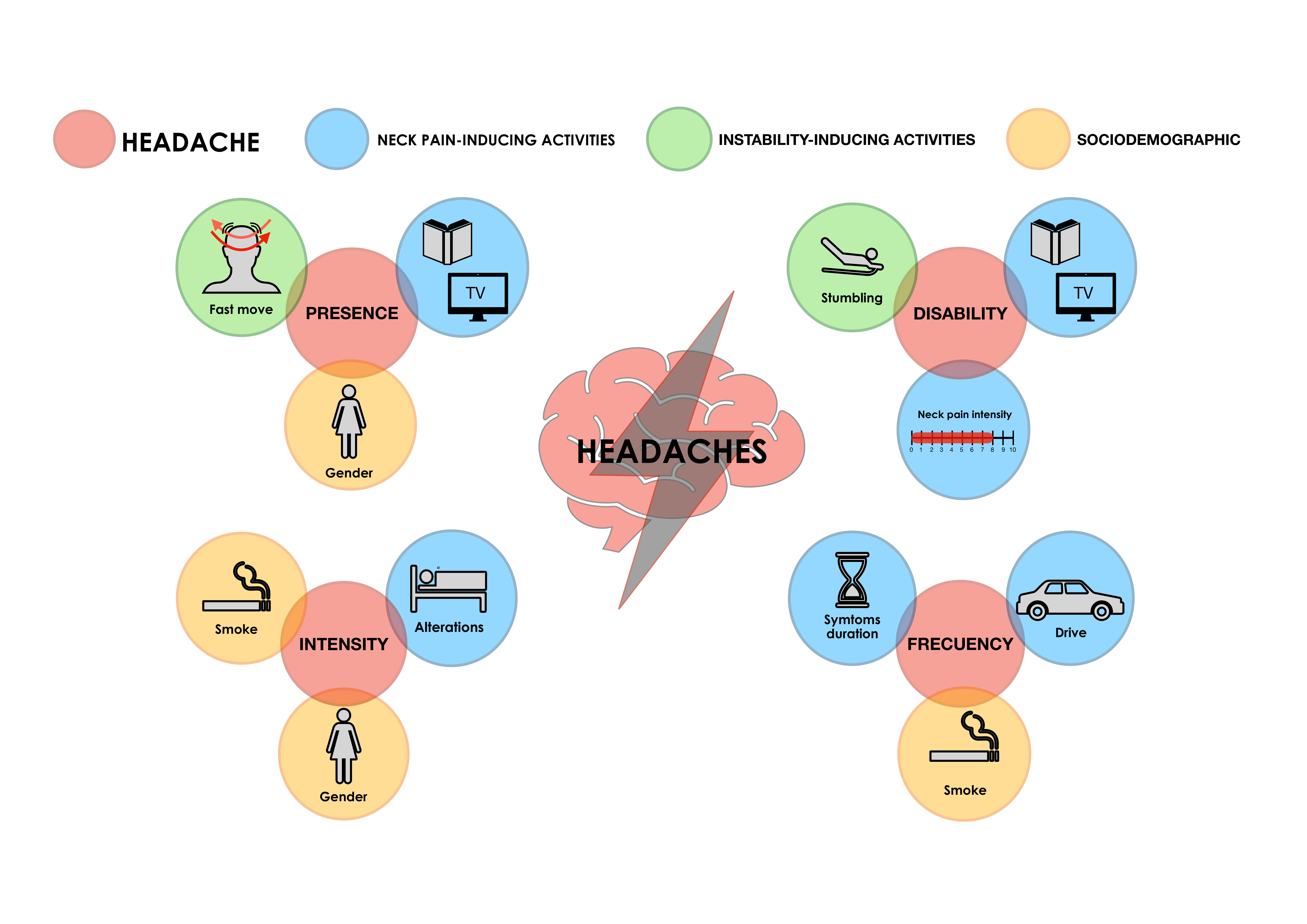
| Gender | 4.158 | 2.276 | 7.596 | <0.001 | 3.029 | 1.597 | 5.746 | 0.001 |
| Height (cm) | 0.946 | 0.915 | 0.978 | 0.001 | NS | NS | NS | NS |
| Neck pain intensity | 2.782 | 1.517 | 5.102 | 0.001 | NS | NS | NS | NS |
| Neck pain-associated symptoms duration | 3.148 | 1.515 | 6.540 | 0.002 | NS | NS | NS | NS |
| Neck pain when reading or watching TV | 2.582 | 1.454 | 4.586 | 0.001 | 2.042 | 1.100 | 3.792 | 0.024 |
| Unsteadiness when moving the head | 3.640 | 1.998 | 6.631 | <0.001 | 2.544 | 1.335 | 4.851 | 0.005 |
| Unsteadiness during fast position changes | 2.533 | 1.407 | 4.560 | 0.002 | NS | NS | NS | NS |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | B | 95% C.I. | p | B | 95% C.I. | p | ||
| Inferior | Superior | Inferior | Superior | |||||
| Neck pain intensity | 3.709 | 1.952 | 5.466 | <0.001 | 3.308 | 1.671 | 4.945 | <0.001 |
| Neck pain-related sleep disturbances | 3.607 | 1.306 | 5.908 | 0.002 | NS | NS | NS | NS |
| Duration of neck pain-associated symptoms | 2.819 | 1.136 | 4.502 | 0.001 | NS | NS | NS | NS |
| Neck pain when lifting weights | 4.878 | 0.900 | 8.856 | 0.017 | NS | NS | NS | NS |
| Neck pain when reading or watching TV | 2.652 | 0.704 | 4.601 | 0.008 | 1.895 | 0.158 | 3.632 | 0.033 |
| Neck pain at work | 4.751 | 1.467 | 8.034 | 0.005 | NS | NS | NS | NS |
| Neck pain at driving | 4.873 | 0.829 | 8.917 | 0.019 | NS | NS | NS | NS |
| Stumbling | 3.654 | 1.838 | 5.471 | <0.001 | 3.672 | 2.034 | 5.310 | <0.001 |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | B | 95% C.I. | p | B | 95% C.I. | p | ||
| Inferior | Superior | Inferior | Superior | |||||
| Smoking | 6.926 | 3.154 | 10.705 | <0.001 | 5.445 | 1.729 | 9.16 | 0.004 |
| Neck pain intensity | 2.279 | 0.913 | 3.645 | 0.001 | NS | NS | NS | NS |
| Duration of neck pain-associated symptoms | 2.534 | 1.289 | 3.779 | <0.001 | 1.399 | 0.016 | 2.781 | 0.047 |
| Neck pain when lifting weights | 4.454 | 1.485 | 7.424 | 0.004 | NS | NS | NS | NS |
| Neck pain when reading or watching TV | 1.815 | 0.332 | 3.298 | 0.017 | NS | NS | NS | NS |
| Neck pain at work | 4.061 | 1.605 | 6.517 | 0.001 | NS | NS | NS | NS |
| Neck pain when driving | 5.062 | 2.078 | 8.045 | 0.001 | 3.284 | 0.162 | 6.407 | 0.039 |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | B | 95% C.I. | p | B | 95% C.I. | p | ||
| Inferior | Superior | Inferior | Superior | |||||
| Gender | 1.481 | 0.520 | 2.442 | 0.003 | 1.471 | 0.558 | 2.385 | 0.002 |
| Smoking | 1.763 | 0.485 | 3.042 | 0.007 | 1.505 | 0.318 | 2.692 | 0.013 |
| Neck pain intensity | 0.497 | 0.033 | 0.961 | 0.036 | NS | NS | NS | NS |
| Neck pain-related sleep disturbances | 0.741 | 0.130 | 1.299 | 0.017 | 0.640 | 0.088 | 1.192 | 0.024 |
| Duration of neck pain-associated symptoms | 0.651 | 0.228 | 1.075 | 0.003 | NS | NS | NS | NS |
| Neck pain when reading or watching TV | 0.580 | 0.089 | 1.070 | 0.021 | NS | NS | NS | NS |
| Neck pain at work | 0.959 | 0.128 | 1.790 | 0.024 | NS | NS | NS | NS |
| Unsteadiness when moving head | 1.072 | 0.087 | 2.057 | 0.033 | NS | NS | NS | NS |
| Dizziness | 1.000 | 0.128 | 1.872 | 0.025 | NS | NS | NS | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Almagro, D.; Achalandabaso-Ochoa, A.; Molina-Ortega, F.J.; Obrero-Gaitán, E.; Ibáñez-Vera, A.J.; Lomas-Vega, R. Neck Pain- and Unsteadiness-Inducing Activities and their Relationship to the Presence, Intensity, Frequency, and Disability of Headaches. Brain Sci. 2020, 10, 425. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10070425
Rodríguez-Almagro D, Achalandabaso-Ochoa A, Molina-Ortega FJ, Obrero-Gaitán E, Ibáñez-Vera AJ, Lomas-Vega R. Neck Pain- and Unsteadiness-Inducing Activities and their Relationship to the Presence, Intensity, Frequency, and Disability of Headaches. Brain Sciences. 2020; 10(7):425. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10070425
Chicago/Turabian StyleRodríguez-Almagro, Daniel, Alexander Achalandabaso-Ochoa, Francisco Javier Molina-Ortega, Esteban Obrero-Gaitán, Alfonso Javier Ibáñez-Vera, and Rafael Lomas-Vega. 2020. "Neck Pain- and Unsteadiness-Inducing Activities and their Relationship to the Presence, Intensity, Frequency, and Disability of Headaches" Brain Sciences 10, no. 7: 425. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10070425