Subcortical T1-Rho MRI Abnormalities in Juvenile-Onset Huntington’s Disease


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Acquisition
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
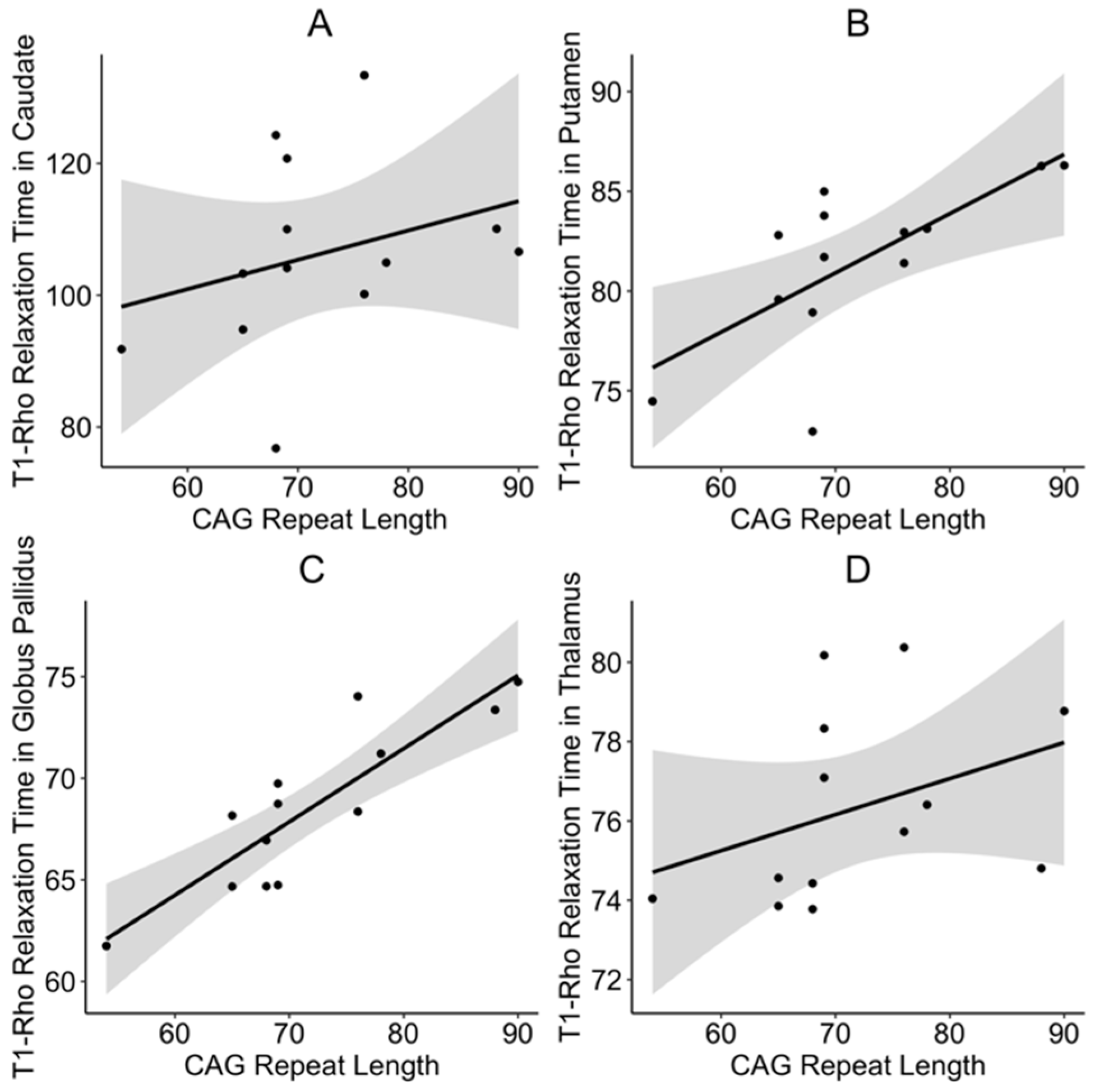
3.1. Primary Outcomes
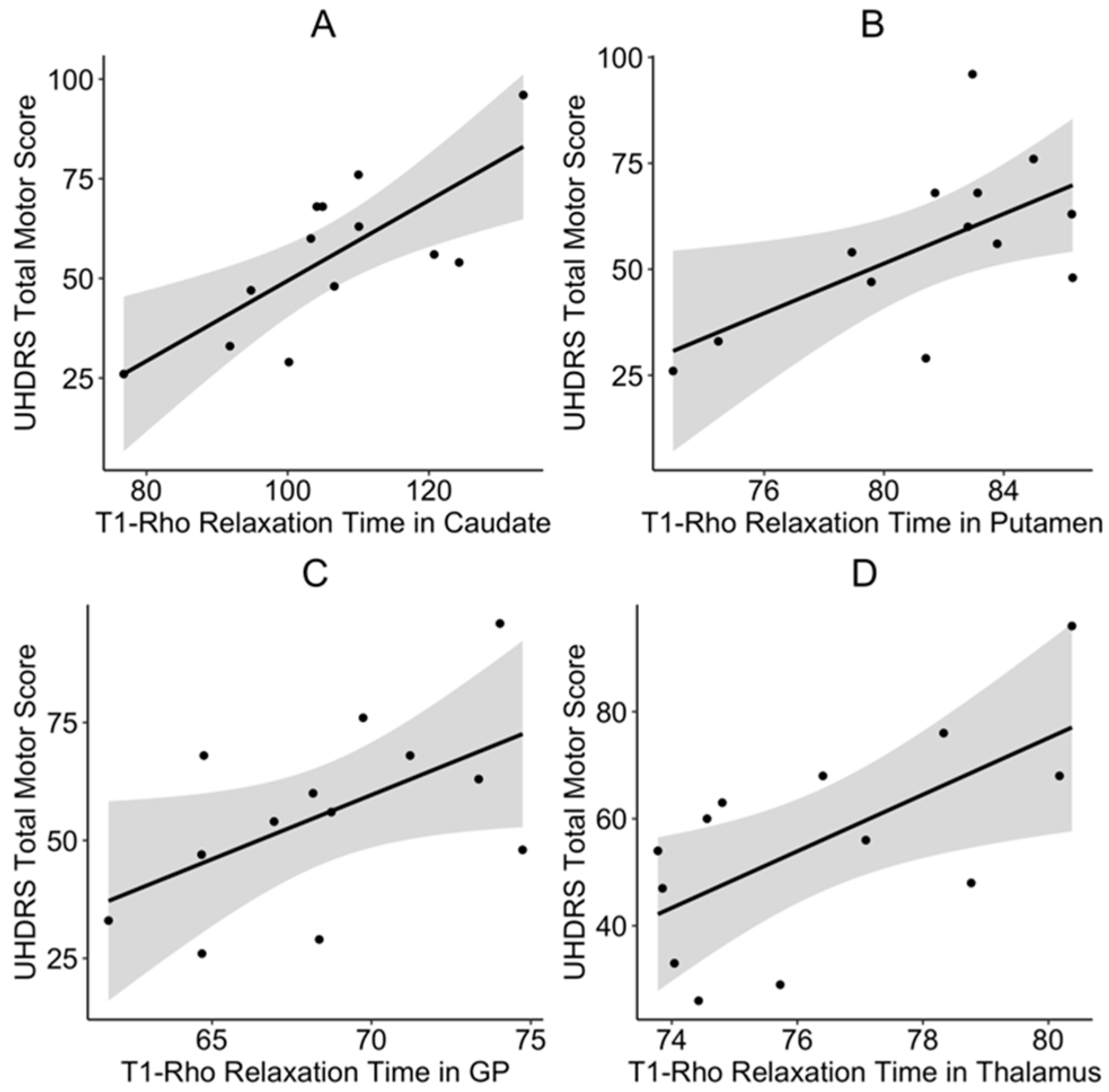
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nopoulos, P.C. Huntington disease: A single-gene degenerative disorder of the striatum. Dialogues Clin. Neurosci. 2016, 18, 91–98. [Google Scholar] [PubMed]
- Tereshchenko, A.; Magnotta, V.; Epping, E.; Mathews, K.; Espe-Pfeifer, P.; Martin, E.; Dawson, J.; Duan, W.; Nopoulos, P. Brain structure in juvenile-onset Huntington disease. Neurology 2019, 92, e1939–e1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nopoulos, P.C.; Aylward, E.H.; Ross, C.A.; Johnson, H.J.; Magnotta, V.A.; Juhl, A.R.; Pierson, R.K.; Mills, J.; Langbehn, D.R.; Paulsen, J.S.; et al. Cerebral cortex structure in prodromal Huntington disease. Neurobiol. Dis. 2010, 40, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haris, M.; Singh, A.; Cai, K.; Davatzikos, C.; Trojanowski, J.Q.; Melhem, E.R.; Clark, C.M.; Borthakur, A. T1rho (T1ρ) MR imaging in Alzheimer’s disease and Parkinson’s disease with and without dementia. J. Neurol. 2011, 258, 380–385. [Google Scholar] [CrossRef] [Green Version]
- Haris, M.; Yadav, S.K.; Rizwan, A.; Singh, A.; Cai, K.; Kaura, D.; Wang, E.; Davatzikos, C.; Trojanowski, J.Q.; Melhem, E.R.; et al. T1rho MRI and CSF biomarkers in diagnosis of Alzheimer’s disease. Neuroimage Clin. 2015, 7, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Haris, M.; McArdle, E.; Fenty, M.; Singh, A.; Davatzikos, C.; Trojanowski, J.Q.; Melhem, E.R.; Clark, C.M.; Borthakur, A. Early marker for Alzheimer’s disease: Hippocampus T1rho (T1ρ) estimation. J. Magn. Reson. Imaging 2009, 29, 1008–1012. [Google Scholar] [CrossRef] [Green Version]
- Borthakur, A.; Sochor, M.; Davatzikos, C.; Trojanowski, J.Q.; Clark, C.M. T1rho MRI of Alzheimer’s disease. Neuroimage 2008, 41, 1199–1205. [Google Scholar] [CrossRef] [Green Version]
- Mangia, S.; Svatkova, A.; Mascali, D.; Nissi, M.J.; Burton, P.C.; Bednarik, P.; Auerbach, E.J.; Giove, F.; Eberly, L.E.; Howell, M.J.; et al. Multi-modal Brain MRI in Subjects with PD and iRBD. Front. Neurosci. 2017, 11, 709. [Google Scholar] [CrossRef]
- Nestrasil, I.; Michaeli, S.; Liimatainen, T.; Rydeen, C.E.; Kotz, C.M.; Nixon, J.P.; Hanson, T.; Tuite, P.J. T1rho and T2rho MRI in the evaluation of Parkinson’s disease. J. Neurol. 2010, 257, 964–968. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.P.; Follmer, R.L.; Oguz, I.; Warren, L.A.; Christensen, G.E.; Fiedorowicz, J.G.; Magnotta, V.A.; Wemmie, J.A. Brain abnormalities in bipolar disorder detected by quantitative T1rho mapping. Mol. Psychiatry 2015, 20, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Mangia, S.; Carpenter, A.F.; Tyan, A.E.; Eberly, L.E.; Garwood, M.; Michaeli, S. Magnetization transfer and adiabatic T1rho MRI reveal abnormalities in normal-appearing white matter of subjects with multiple sclerosis. Mult. Scler. 2014, 20, 1066–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wassef, S.N.; Wemmie, J.; Johnson, C.P.; Johnson, H.; Paulsen, J.S.; Long, J.D.; Magnotta, V.A. T1rho imaging in premanifest Huntington disease reveals changes associated with disease progression. Mov. Disord. 2015, 30, 1107–1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moser, A.D.; Epping, E.; Espe-Pfeifer, P.; Martin, E.; Zhorne, L.; Mathews, K.; Nance, M.; Hudgell, D.; Quarrell, O.; Nopoulos, P. A survey-based study identifies common but unrecognized symptoms in a large series of juvenile Huntington’s disease. Neurodegener. Dis. Manag. 2017, 7, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tereshchenko, A.; McHugh, M.; Lee, J.K.; Gonzalez-Alegre, P.; Crane, K.; Dawson, J.; Nopoulos, P. Abnormal Weight and Body Mass Index in Children with Juvenile Huntington’s Disease. J. Huntingt. Dis. 2015, 4, 231–238. [Google Scholar] [CrossRef] [Green Version]
- van der Plas, E.; Langbehn, D.R.; Conrad, A.L.; Koscik, T.R.; Tereshchenko, A.; Epping, E.A.; Magnotta, V.A.; Nopoulos, P.C. Abnormal brain development in child and adolescent carriers of mutant huntingtin. Neurology 2019, 93, e1021–e1030. [Google Scholar] [CrossRef]
- Huntington Study Group. Unified Huntington’s Disease Rating Scale: Reliability and consistency. Mov. Disord. 1996, 11, 136–142. [Google Scholar] [CrossRef]
- Horton, M.C.; Nopoulos, P.; Nance, M.; Landwehrmyer, G.B.; Barker, R.A.; Squitieri, F.; REGISTRY Investigators of the European Huntington’s Disease Network; Burgunder, J.M.; Quarrell, O. Assessment of the Performance of a Modified Motor Scale as Applied to Juvenile Onset Huntington’s Disease. J. Huntingt. Dis. 2019, 8, 181–193. [Google Scholar] [CrossRef]
- Tabrizi, S.J.; Langbehn, D.R.; Leavitt, B.R.; Roos, R.A.; Durr, A.; Craufurd, D.; Kennard, C.; Hicks, S.L.; Fox, N.C.; Scahill, R.I.; et al. Biological and clinical manifestations of Huntington’s disease in the longitudinal TRACK-HD study: Cross-sectional analysis of baseline data. Lancet Neurol. 2009, 8, 791–801. [Google Scholar] [CrossRef] [Green Version]
- Pierson, R.; Johnson, H.; Harris, G.; Keefe, H.; Paulsen, J.S.; Andreasen, N.C.; Magnotta, V.A. Fully automated analysis using BRAINS: AutoWorkup. Neuroimage 2011, 54, 328–336. [Google Scholar] [CrossRef] [Green Version]
- Powell, S.; Magnotta, V.A.; Johnson, H.; Jammalamadaka, V.K.; Pierson, R.; Andreasen, N.C. Registration and machine learning-based automated segmentation of subcortical and cerebellar brain structures. Neuroimage 2008, 39, 238–247. [Google Scholar] [CrossRef] [Green Version]
- Tustison, N.J.; Cook, P.A.; Klein, A.; Song, G.; Das, S.R.; Duda, J.T.; Kandel, B.M.; van Strien, N.; Stone, J.R.; Gee, J.C.; et al. Large-scale evaluation of ANTs and FreeSurfer cortical thickness measurements. Neuroimage 2014, 99, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T.S.; Metaxas, D.N. Open science--combining open data and open source software: Medical image analysis with the Insight Toolkit. Med. Image Anal. 2005, 9, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Bigler, D.; Meadowcraft, M.; Sun, X.; Vesek, J.; Dresner, A.; Smith, M.; Yang, Q. MR Parameter Map Suite: ITK Classes for Calculating Magnetic Resonance T2 and T1 Parameter Maps. Insight J. 2008, 2008, 237. [Google Scholar]
- Tereshchenko, A.V.; Schultz, J.L.; Bruss, J.E.; Magnotta, V.A.; Epping, E.A.; Nopoulos, P.C. Abnormal development of cerebellar-striatal circuitry in Huntington disease. Neurology 2020, 94, e1908–e1915. [Google Scholar] [CrossRef]
- Cronin, T.; Rosser, A.; Massey, T. Clinical Presentation and Features of Juvenile-Onset Huntington’s Disease: A Systematic Review. J. Huntingt. Dis. 2019, 8, 171–179. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| JOHD Group | Controls | p-Value | |
|---|---|---|---|
| N (Visits) | 11 (13) | 38 (39) | NA |
| Male, % (n) | 36.4 (4) | 39.5 (15) | 1 |
| Age (yrs), Mean ± SD | 15.39 ± 5.1 | 15.56 ± 3.82 | 0.905 |
| CAG Repeats, Mean ± SD | 72.82 ± 10.31 | 19.5 ± 3.85 | <0.001 |
| Disease Burden Score, Mean ± SD | 540.99 ± 148.11 | NA | NA |
| Disease Duration (yrs), Mean ± SD | 3.1 ± 2.61 | NA | NA |
| UHDRS, Mean ± SD | 55.27 ± 21.54 | NA | NA |
| JOHDRS, Mean ± SD | 14.91 ± 6.71 | NA | NA |
| Region | Control T1ρ (ms) | JOHD T1ρ (ms) | Beta-Coefficient | p-Value |
|---|---|---|---|---|
| Caudate, mean ± SD | 78.34 ± 6.35 | 106.42 ± 14.21 | 27.9 | <0.001 |
| Putamen, mean ± SD | 71.25 ± 2.56 | 81.79 ± 3.53 | 10.37 | <0.001 |
| Globus pallidus, mean ± SD | 64.13 ± 2.79 | 68.52 ± 4.05 | 4.62 | <0.001 |
| Thalamus, mean ± SD | 73.86 ± 2.46 | 76.38 ± 2.37 | 2.53 | <0.001 |
| Hippocampus, mean ± SD | 86.12 ± 8.5 | 87.65 ± 3.49 | 1.76 | 0.484 |
| Anterior Cerebellum mean ± SD | 92.12 ± 18.81 | 94.13 ± 11.55 | 1.94 | 0.732 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tereshchenko, A.V.; Schultz, J.L.; Kunnath, A.J.; Bruss, J.E.; Epping, E.A.; Magnotta, V.A.; Nopoulos, P.C. Subcortical T1-Rho MRI Abnormalities in Juvenile-Onset Huntington’s Disease. Brain Sci. 2020, 10, 533. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10080533
Tereshchenko AV, Schultz JL, Kunnath AJ, Bruss JE, Epping EA, Magnotta VA, Nopoulos PC. Subcortical T1-Rho MRI Abnormalities in Juvenile-Onset Huntington’s Disease. Brain Sciences. 2020; 10(8):533. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10080533
Chicago/Turabian StyleTereshchenko, Alexander V., Jordan L. Schultz, Ansley J. Kunnath, Joel E. Bruss, Eric A. Epping, Vincent A. Magnotta, and Peg C. Nopoulos. 2020. "Subcortical T1-Rho MRI Abnormalities in Juvenile-Onset Huntington’s Disease" Brain Sciences 10, no. 8: 533. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10080533