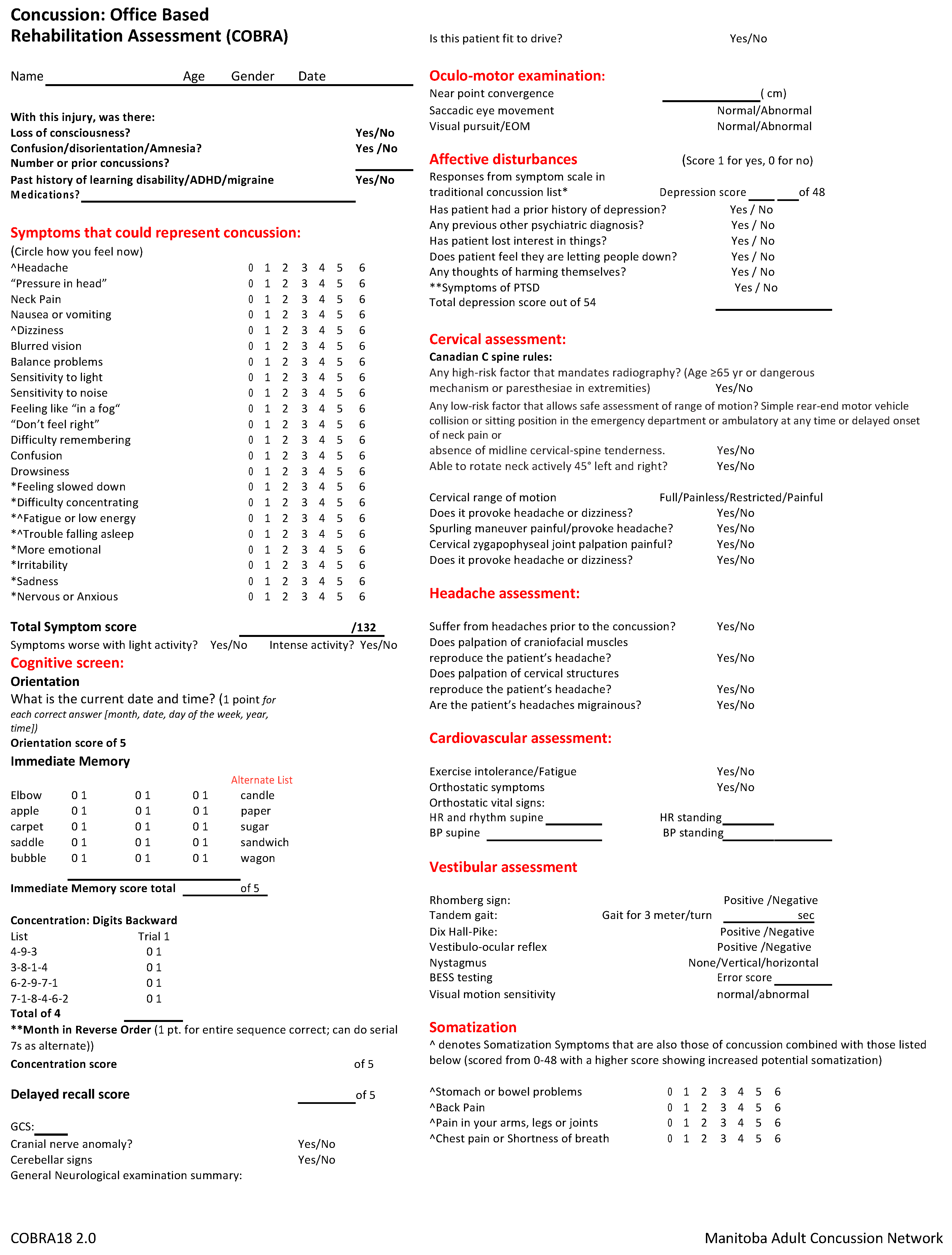
Concussion Office Based Rehabilitation Assessment: A Novel Clinical Tool for Concussion Assessment and Management



Abstract
:
{kind=link}
{kind=link}
1. Introduction
2. Discussion
3. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Ochiai, H.; Abe, T. Clinical features and early detection of sport-related concussion. Acute Med. Surg. 2019, 6, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.M. Canada, Veterans Affairs Canada, Research Directorate. In Persistent Symptoms Following Mild Traumatic Brain Injury (MTBI): A Resource for Clinicians and Staff; Veterans Affairs Canada Research Directorate: Ottawa, ON, Canada, 2011; Available online: https://www.deslibris.ca/ID/227128 (accessed on 5 July 2020).
- Mccrory, P.; Meeuwisse, W.H.; Dvorak, J.; Aubry, M.; Bailes, J.E.; Broglio, S.P.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport-the 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef] [Green Version]
- Harmon, K.G.; Drezner, J.A.; Gammons, M.; Guskiewicz, K.M.; Halstead, M.; Herring, S.A.; Kutcher, J.S.; Pana, A.; Putukian, M.; Roberts, W.O. American Medical Society for Sports Medicine position statement on concussion in sport. Br. J. Sports Med. 2019, 53, 213–225. [Google Scholar] [CrossRef]
- Ventura, R.E.; Balcer, L.J.; Galetta, S.L.; Rucker, J.C. Ocular motor assessment in concussion: Current status and future directions. J. Neurol. Sci. 2016, 361, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Skandsen, T.; Einarsen, C.E.; Normann, I.; Bjoralt, S.; Karlsen, R.H.; Mcdonagh, D.; Nilsen, T.I.L.; Akslen, A.N.; Haberg, A.; Vik, A. The epidemiology of mild traumatic brain injury: The Trondheim MTBI follow-up study. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leslie, O.; Craton, N. Concussion: Purely a Brain Injury? Clin. J. Sport Med. 2013, 23, 331–332. [Google Scholar] [CrossRef] [PubMed]
- Craton, N.; Ali, H.; Lenoski, S. COACH CV: The Seven Clinical Phenotypes of Concussion. Brain Sci. 2017, 7, 119. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.J.; Leddy, J.J.; Willer, B. Physiological, vestibulo-ocular and cervicogenic post-concussion disorders: An evidence-based classification system with directions for treatment. Brain Inj. 2015, 29, 238–248. [Google Scholar] [CrossRef]
- Leddy, J.; Baker, J.G.; Haider, M.N.; Hinds, A.; Willer, B. A Physiological Approach to Prolonged Recovery from Sport-Related Concussion. J. Athl. Train. 2017, 52, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, K.A.; Kaye, S.; Blaine, H.; Edmed, S.L.; Meares, S.; Rossa, K.R.; Haden, C. Psychological approaches for the management of persistent postconcussion symptoms after mild traumatic brain injury: A systematic review. Disabil. Rehabil. 2019, 1–9. [Google Scholar] [CrossRef]
- Mucha, A.; Collins, M.W.; Elbin, R.J.; Furman, J.M.; Troutmanenseki, C.; Dewolf, R.; Marchetti, G.; Kontos, A.P. A Brief Vestibular/Ocular Motor Screening (VOMS) Assessment to Evaluate Concussions. Am. J. Sports Med. 2014, 42, 2479–2486. [Google Scholar] [CrossRef] [PubMed]
- Sufrinko, A.; McAllister-Deitrick, J.; Womble, M.; Kontos, A. Do Sideline Concussion Assessments Predict Subsequent Neurocognitive Impairment After Sport-Related Concussion? J. Athl. Train. 2017, 52, 676–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumbabrown, A.; Teramoto, M.; Bloom, O.J.; Brody, D.L.; Chesnutt, J.C.; Clugston, J.R.; Collins, M.W.; Gioia, G.A.; Kontos, A.P.; Lal, A.; et al. Concussion Guidelines Step 2: Evidence for Subtype Classification. Neurosurgery 2020, 86, 2–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, M.; Madathil, R. Evaluation of Cognitive Symptoms Following Concussion. Curr. Pain Headache Rep. 2015, 19, 45. [Google Scholar] [CrossRef] [PubMed]
- Pearce, K.L.; Sufrinko, A.; Lau, B.C.; Henry, L.; Collins, M.W.; Kontos, A.P. Near Point of Convergence After a Sport-Related Concussion: Measurement Reliability and Relationship to Neurocognitive Impairment and Symptoms. Am. J. Sports Med. 2015, 43, 3055–3061. [Google Scholar] [CrossRef] [Green Version]
- Halstead, M.E.; Mcavoy, K.; Devore, C.D.; Carl, R.L.; Lee, M. Returning to Learning Following a Concussion. Pediatrics 2013, 132, 948–957. [Google Scholar] [CrossRef] [Green Version]
- Matuszak, J.M.; McVige, J.; McPherson, J.; Willer, B.; Leddy, J. A Practical Concussion Physical Examination Toolbox. Sports Health 2016, 8, 260–269. [Google Scholar] [CrossRef] [Green Version]
- Schneider, K.J.; Meeuwisse, W.H.; Nettelaguirre, A.; Barlow, K.M.; Boyd, L.A.; Kang, J.; Emery, C.A. Cervicovestibular rehabilitation in sport-related concussion: A randomised controlled trial. Br. J. Sports Med. 2014, 48, 1294–1298. [Google Scholar] [CrossRef]
- Eckner, J.T.; Seifert, T.; Pescovitz, A.; Zeiger, M.; Kutcher, J.S. Is Migraine Headache Associated with Concussion in Athletes? A Case–Control Study. Clin. J. Sport Med. 2017, 27, 266–270. [Google Scholar] [CrossRef] [Green Version]
- Seifert, T. Post-Traumatic Headache Therapy in the Athlete. Curr. Pain Headache Rep. 2016, 20, 41. [Google Scholar] [CrossRef]
- Anzalone, A.J.; Blueitt, D.; Case, T.; Mcguffin, T.; Pollard, K.; Garrison, J.C.; Jones, M.T.; Pavur, R.; Turner, S.M.; Oliver, J.M. A Positive Vestibular/Ocular Motor Screening (VOMS) Is Associated with Increased Recovery Time after Sports-Related Concussion in Youth and Adolescent Athletes. Am. J. Sports Med. 2017, 45, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Gall, B.; Parkhouse, W.; Goodman, D. Heart Rate Variability of Recently Concussed Athletes at Rest and Exercise. Med. Sci. Sports Exerc. 2004, 36, 1269–1274. [Google Scholar] [CrossRef]
- Orthostatic Intolerance and Autonomic Dysfunction in Youth, W: Clinical Journal of Sport Medicine. Available online: https://journals-lww-com.uml.idm.oclc.org/cjsportsmed/Fulltext/2016/01000/Orthostatic_Intolerance_and_Autonomic_Dysfunction.6.aspx (accessed on 5 July 2020).
- Corwin, D.J.; Wiebe, D.J.; Zonfrillo, M.R.; Grady, M.F.; Robinson, R.L.; Goodman, A.; Master, C.L. Vestibular Deficits following Youth Concussion. J. Pediatr. 2015, 166, 1221–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, L.D.; Tarima, S.; Laroche, A.A.; Hammeke, T.A.; Barr, W.B.; Guskiewicz, K.M.; Randolph, C.; Mccrea, M. Preinjury somatization symptoms contribute to clinical recovery after sport-related concussion. Neurology 2016, 86, 1856–1863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mccrory, P.; Meeuwisse, W.H.; Johnston, K.M.; Dvorak, J.; Aubry, M.; Molloy, M.G.; Cantu, R.C. Consensus Statement on Concussion in Sport 3rd International Conference on Concussion in Sport Held in Zurich, November 2008. Clin. J. Sport Med. 2009, 19, 185–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrine, K.; Gibaldi, J.C. Somatization in Post-Concussion Syndrome: A Retrospective Study. Cureus 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- Echemendia, R.J.; Meeuwisse, W.; McCrory, P.; Davis, G.A.; Putukian, M.; Leddy, J.; Makdissi, M.; Sullivan, S.J.; Broglio, S.P.; Raftery, M. The Sport Concussion Assessment Tool 5th Edition (SCAT5): Background and rationale. Br. J. Sports Med. 2017, 1–8. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katz, M.; Lenoski, S.; Ali, H.; Craton, N. Concussion Office Based Rehabilitation Assessment: A Novel Clinical Tool for Concussion Assessment and Management. Brain Sci. 2020, 10, 593. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10090593
Katz M, Lenoski S, Ali H, Craton N. Concussion Office Based Rehabilitation Assessment: A Novel Clinical Tool for Concussion Assessment and Management. Brain Sciences. 2020; 10(9):593. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10090593
Chicago/Turabian StyleKatz, Matthew, Stephane Lenoski, Haitham Ali, and Neil Craton. 2020. "Concussion Office Based Rehabilitation Assessment: A Novel Clinical Tool for Concussion Assessment and Management" Brain Sciences 10, no. 9: 593. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10090593