
Perinatal Acetaminophen Exposure and Childhood Attention-Deficit/Hyperactivity Disorder (ADHD): Exploring the Role of Umbilical Cord Plasma Metabolites in Oxidative Stress Pathways

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Independent Variable: Childhood ADHD
2.3. Dependent Variables: Umbilical Cord and Maternal Plasma Analytes
2.4. Maternal and Child Covariates
2.5. Statistical Analyses
3. Results
3.1. Maternal and Child Characteristics
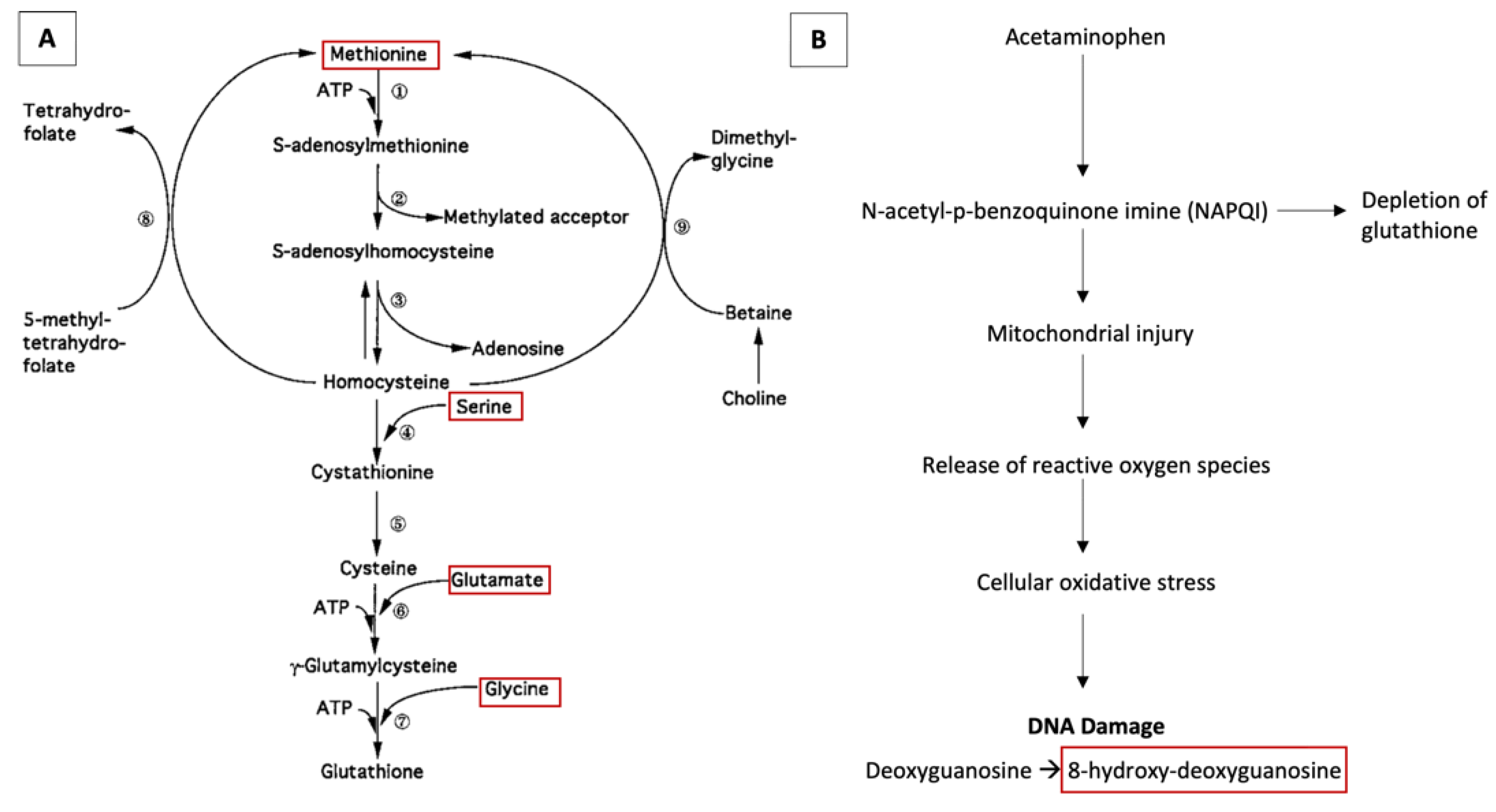
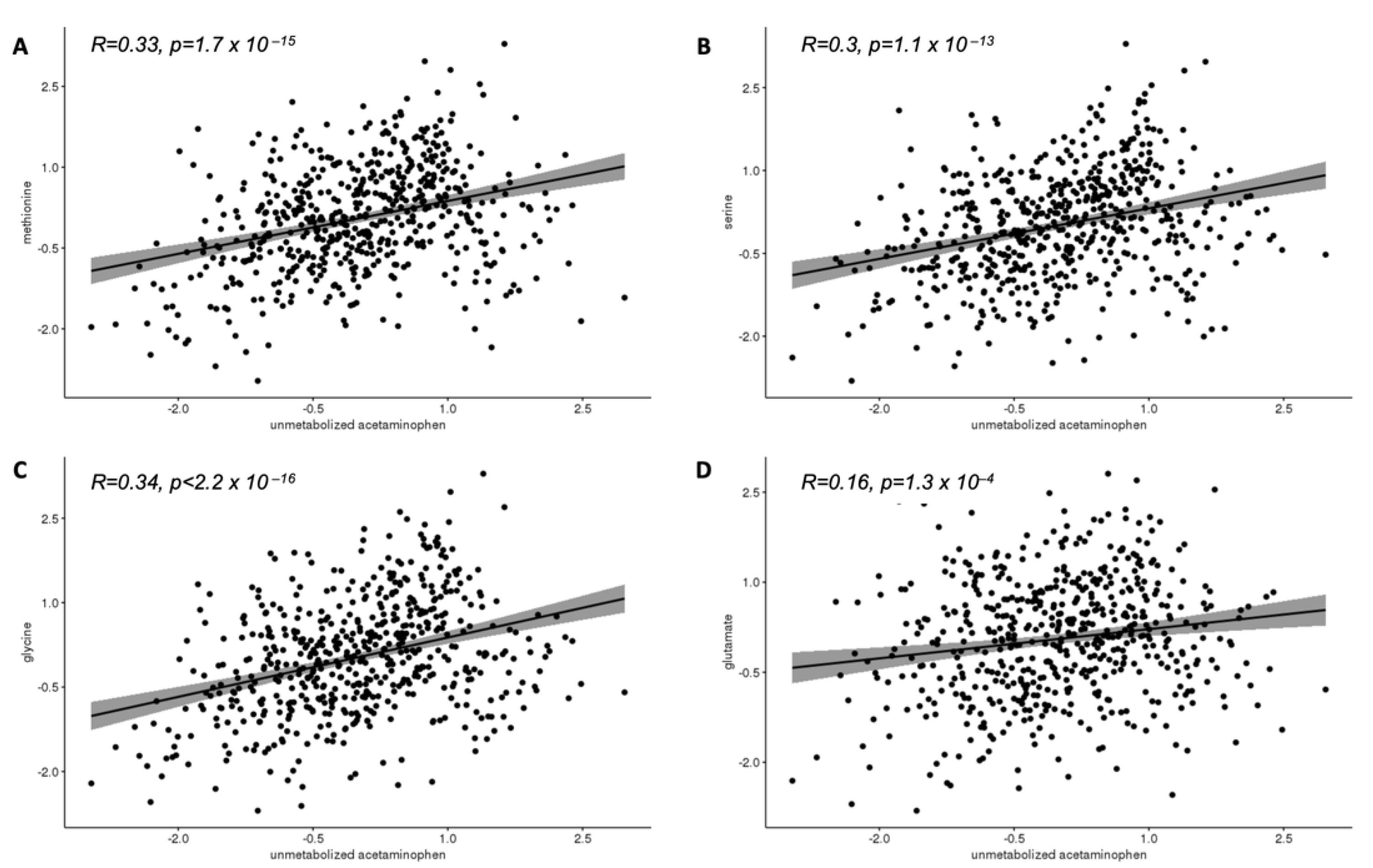
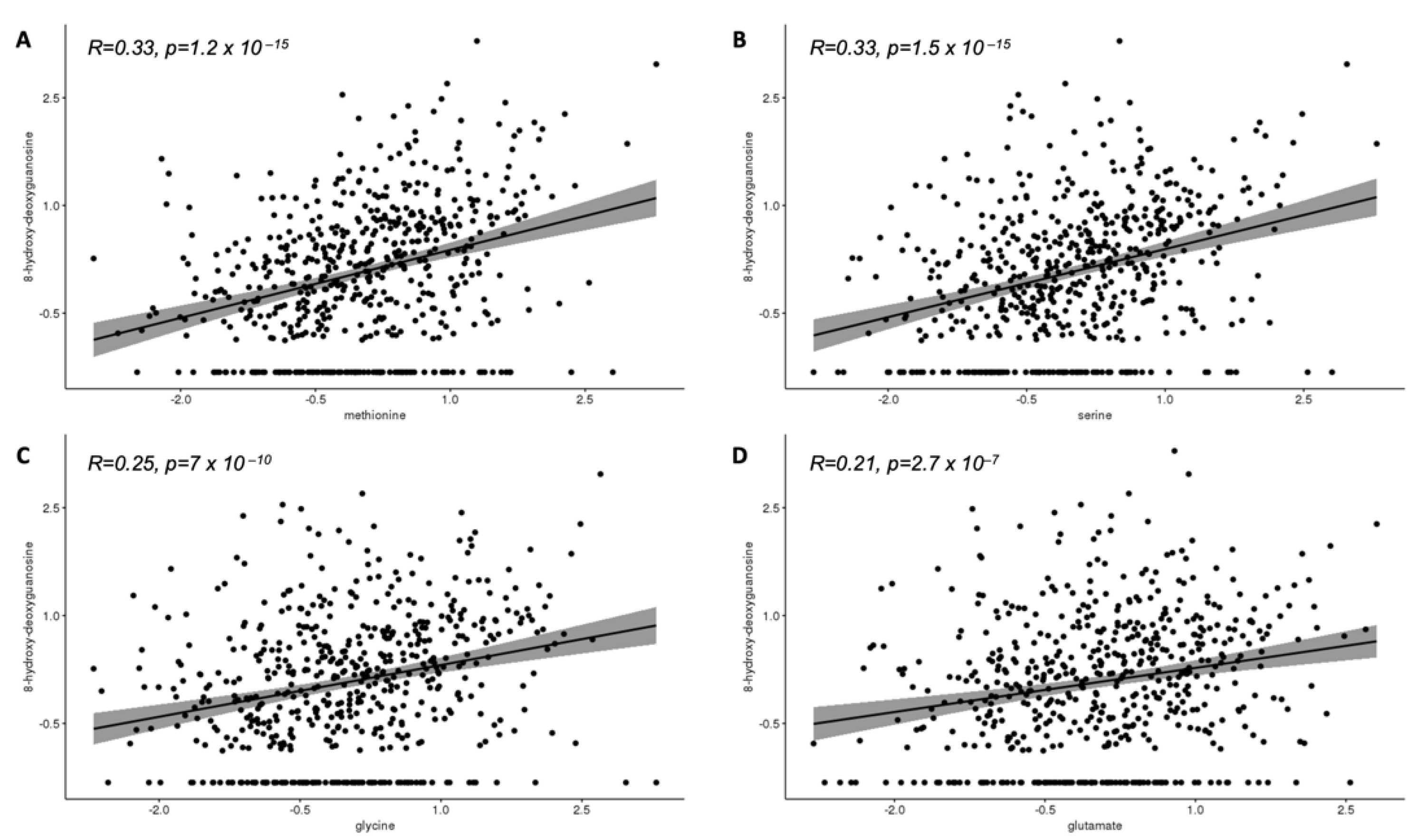
3.2. Correlations of Cord Plasma Methionine, Serine, Glycine, and Glutamate with Cord Plasma Unmetabolized Acetaminophen and 8-Hydroxy-Deoxyguanosine
3.3. Correlations of Cord Plasma Methionine, Serine, Glycine, and Glutamate with Cord Plasma Unmetabolized Acetaminophen and 8-Hydroxy-Deoxyguanosine
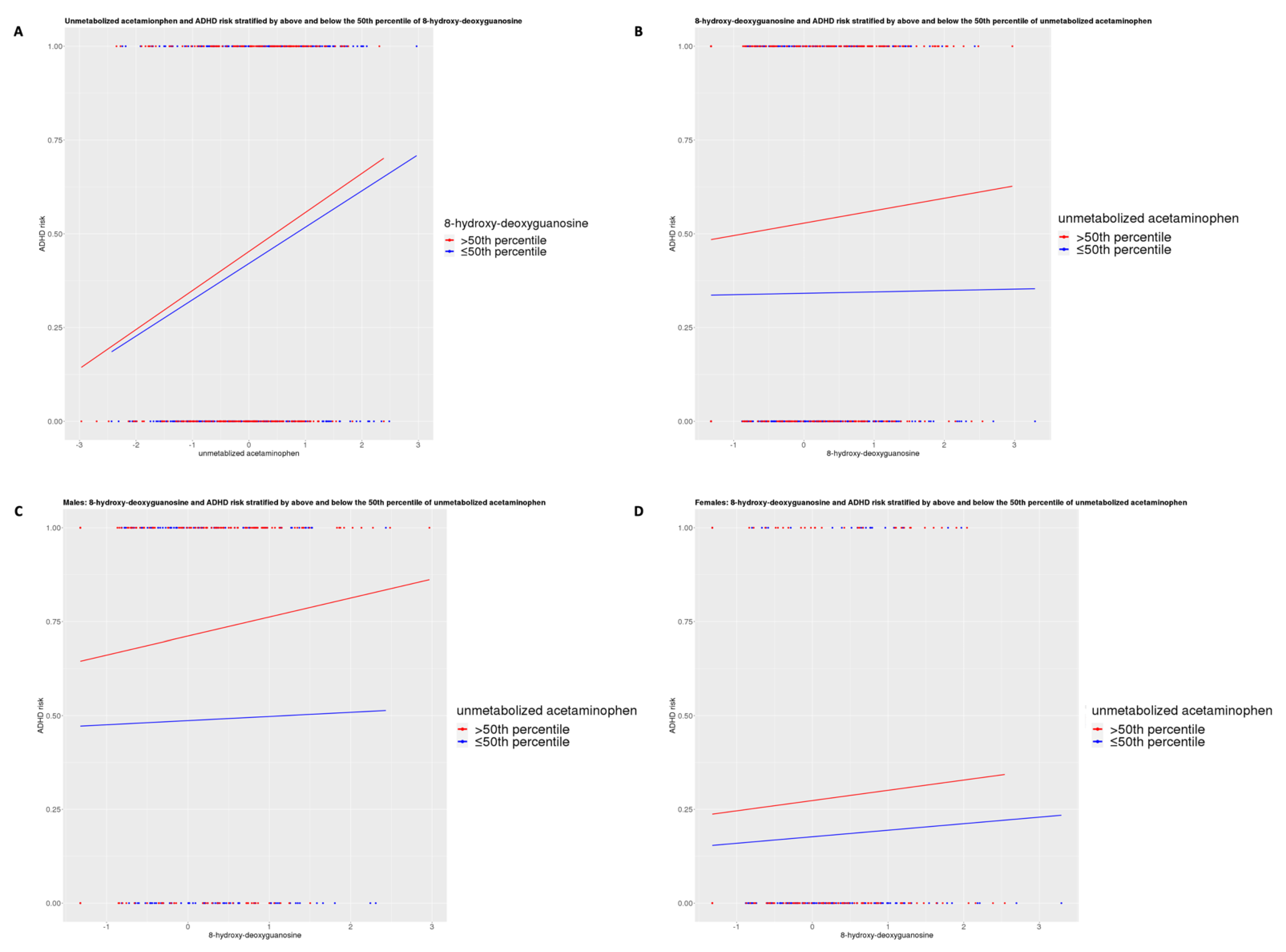
3.4. Logistic Regressions of Odds of ADHD and Cord Plasma Analytes
3.5. Cord Plasma Methionine and Glycine as Partial Mediators for the Association between Cord Plasma Unmetabolized Acetaminophen and Childhood ADHD
3.6. Correlations of Cord and Maternal Plasma Methionine and Glycine and Associations of Maternal Plasma Methionine and Glycine with Childhood ADHD
4. Discussion
4.1. Main Findings and Interpretation
4.2. Strengths, Limitations, and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kristensen, D.M.; Mazaud-Guittot, S.; Gaudriault, P.; Lesné, L.; Serrano, T.; Main, K.M.; Jegou, B. Analgesic use—Prevalence, biomonitoring and endocrine and reproductive effects. Nat. Rev. Endocrinol. 2016, 12, 381–393. [Google Scholar] [CrossRef]
- Werler, M.M.; the National Birth Defects Prevention Study; Mitchell, A.; Hernandez-Diaz, S.; Honein, M.A. Use of over-the-counter medications during pregnancy. Am. J. Obstet. Gynecol. 2005, 193, 771–777. [Google Scholar] [CrossRef]
- Brandlistuen, R.E.; Ystrom, E.; Nulman, I.; Koren, G.; Nordeng, H. Prenatal paracetamol exposure and child neurodevelopment: A sibling-controlled cohort study. Int. J. Epidemiol. 2013, 42, 1702–1713. [Google Scholar] [CrossRef] [Green Version]
- Liew, Z.; Ritz, B.; Rebordosa, C.; Lee, P.-C.; Olsen, J. Acetaminophen Use During Pregnancy, Behavioral Problems, and Hyperkinetic Disorders. JAMA Pediatr. 2014, 168, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, Y.; Riley, A.W.; Lee, L.-C.; Hong, X.; Wang, G.; Tsai, H.-J.; Mueller, N.T.; Pearson, C.; Thermitus, J.; Panjwani, A.; et al. Maternal Biomarkers of Acetaminophen Use and Offspring Attention Deficit Hyperactivity Disorder. Brain Sci. 2018, 8, 127. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Azuine, R.E.; Zhang, Y.; Hou, W.; Hong, X.; Wang, G.; Riley, A.; Pearson, C.; Zuckerman, B.; Wang, X. Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure With Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood. JAMA Psychiatry 2020, 77, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Liew, Z.; Ritz, B.; Virk, J.; Olsen, J. Maternal use of acetaminophen during pregnancy and risk of autism spectrum disorders in childhood: A Danish national birth cohort study. Autism Res. 2015, 9, 951–958. [Google Scholar] [CrossRef]
- Liew, Z.; Bach, C.C.; Asarnow, R.F.; Ritz, B.; Olsen, J. Paracetamol use during pregnancy and attention and executive function in offspring at age 5 years. Int. J. Epidemiol. 2016, 45, 2009–2017. [Google Scholar] [CrossRef]
- Liew, Z.; Kioumourtzoglou, M.-A.; Roberts, A.L.; O’Reilly, J.; Ascherio, A.; Weisskopf, M.G. Use of Negative Control Exposure Analysis to Evaluate Confounding: An Example of Acetaminophen Exposure and Attention-Deficit/Hyperactivity Disorder in Nurses’ Health Study II. Am. J. Epidemiol. 2019, 188, 768–775. [Google Scholar] [CrossRef]
- Avella-Garcia, C.B.; Julvez, J.; Fortuny, J.; Rebordosa, C.; García-Esteban, R.; Riaño-Galan, I.; Tardon, A.; Rodríguez-Bernal, C.L.; Iñiguez, C.; Andiarena, A.; et al. Acetaminophen use in pregnancy and neurodevelopment: Attention function and autism spectrum symptoms. Int. J. Epidemiol. 2016, 45, 1987–1996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, B.H.; Lugo-Candelas, C.; Wu, H.; Laue, H.E.; Boivin, A.; Gillet, V.; Aw, N.; Rahman, T.; Lepage, J.-F.; Whittingstall, K.; et al. Association of Prenatal Acetaminophen Exposure Measured in Meconium With Risk of Attention-Deficit/Hyperactivity Disorder Mediated by Frontoparietal Network Brain Connectivity. JAMA Pediatr. 2020, 174, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.Z.; Kriebel, D. Prenatal and perinatal analgesic exposure and autism: An ecological link. Environ. Health 2013, 12, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.-H.; Pan, T.-L.; Wang, P.-W.; Hsu, J.-W.; Huang, K.-L.; Su, T.-P.; Li, C.-T.; Lin, W.-C.; Tsai, S.-J.; Chen, T.-J.; et al. Prenatal Exposure to Acetaminophen and the Risk of Attention-Deficit/Hyperactivity Disorder: A Nationwide Study in Taiwan. J. Clin. Psychiatry 2019, 80. [Google Scholar] [CrossRef] [PubMed]
- Rifas-Shiman, S.L.; Cardenas, A.; Hivert, M.; Tiemeier, H.; Bertoldi, A.D.; Oken, E. Associations of prenatal or infant exposure to acetaminophen or ibuprofen with mid-childhood executive function and behaviour. Paediatr. Périnat. Epidemiol. 2019, 34, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Stergiakouli, E.; Thapar, A.; Smith, G.D. Association of Acetaminophen Use During Pregnancy With Behavioral Problems in Childhood. JAMA Pediatry 2016, 170, 964–970. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.M.D.; Waldie, K.E.; Wall, C.; Murphy, R.; Mitchell, E.A. The ABC Study Group Associations between Acetaminophen Use during Pregnancy and ADHD Symptoms Measured at Ages 7 and 11 Years. PLoS ONE 2014, 9, e108210. [Google Scholar] [CrossRef] [Green Version]
- Tovo-Rodrigues, L.; Schneider, B.C.; Martins-Silva, T.; Del-Ponte, B.; De Mola, C.L.; Schuler-Faccini, L.; Vianna, F.S.L.; Munhoz, T.N.; Entiauspe, L.; Silveira, M.F.; et al. Is intrauterine exposure to acetaminophen associated with emotional and hyperactivity problems during childhood? Findings from the 2004 Pelotas birth cohort. BMC Psychiatry 2018, 18, 368. [Google Scholar] [CrossRef] [Green Version]
- Ystrom, E.; Gustavson, K.; Brandlistuen, R.E.; Knudsen, G.P.; Magnus, P.; Susser, E.; Smith, G.D.; Stoltenberg, C.; Surén, P.; Håberg, S.E.; et al. Prenatal Exposure to Acetaminophen and Risk of ADHD. Pediatrics 2017, 140, e20163840. [Google Scholar] [CrossRef] [Green Version]
- Gou, X.; Wang, Y.; Tang, Y.; Qu, Y.; Tang, J.; Shi, J.; Xiao, D.; Mu, D. Association of maternal prenatal acetaminophen use with the risk of attention deficit/hyperactivity disorder in offspring: A meta-analysis. Aust. N. Z. J. Psychiatry 2019, 53, 195–206. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, J.Y.; Lee, J.; Jeong, G.H.; Lee, E.; Lee, S.; Lee, K.H.; Kronbichler, A.; Stubbs, B.; Solmi, M.; et al. Environmental risk factors, protective factors, and peripheral biomarkers for ADHD: An umbrella review. Lancet Psychiatry 2020, 7, 955–970. [Google Scholar] [CrossRef]
- Masarwa, R.; Levine, H.; Gorelik, E.; Reif, S.; Perlman, A.; Matok, I. Prenatal Exposure to Acetaminophen and Risk for Attention Deficit Hyperactivity Disorder and Autistic Spectrum Disorder: A Systematic Review, Meta-Analysis, and Meta-Regression Analysis of Cohort Studies. Am. J. Epidemiol. 2018, 187, 1817–1827. [Google Scholar] [CrossRef]
- Alemany, S.; Avella-García, C.; Liew, Z.; García-Esteban, R.; Inoue, K.; Cadman, T.; López-Vicente, M.; González, L.; Galán, I.R.; Andiarena, A.; et al. Prenatal and postnatal exposure to acetaminophen in relation to autism spectrum and attention-deficit and hyperactivity symptoms in childhood: Meta-analysis in six European population-based cohorts. Eur. J. Epidemiol. 2021. [Google Scholar] [CrossRef]
- Liew, Z.; Ernst, A. Intrauterine Exposure to Acetaminophen and Adverse Developmental Outcomes: Epidemiological Findings and Methodological Issues. Curr. Environ. Health Rep. 2021, 8, 23–33. [Google Scholar] [CrossRef]
- Bauer, A.Z.; Kriebel, D.; Herbert, M.R.; Bornehag, C.-G.; Swan, S.H. Prenatal paracetamol exposure and child neurodevelopment: A review. Horm. Behav. 2018, 101, 125–147. [Google Scholar] [CrossRef]
- Ghanizadeh, A. Acetaminophen may mediate oxidative stress and neurotoxicity in autism. Med. Hypotheses 2012, 78, 351. [Google Scholar] [CrossRef] [PubMed]
- Parker, W.; Hornik, C.D.; Bilbo, S.; Holzknecht, Z.E.; Gentry, L.; Rao, R.; Lin, S.S.; Herbert, M.R.; Nevison, C.D. The role of oxidative stress, inflammation and acetaminophen exposure from birth to early childhood in the induction of autism. J. Int. Med. Res. 2017, 45, 407–438. [Google Scholar] [CrossRef] [PubMed]
- Lupattelli, A.; Spigset, O.; Twigg, M.; Zagorodnikova, K.; Mårdby, A.-C.; Moretti, M.E.; Drozd, M.; Panchaud, A.; Hameen-Anttila, K.; Rieutord, A.; et al. Medication use in pregnancy: A cross-sectional, multinational web-based study. BMJ Open 2014, 4, e004365. [Google Scholar] [CrossRef] [Green Version]
- Martínez, Y.; Li, X.; Liu, G.; Bin, P.; Yan, W.; Más, D.; Valdivié, M.; Hu, C.-A.A.; Ren, W.; Yin, Y. The role of methionine on metabolism, oxidative stress, and diseases. Amino Acids 2017, 49, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.C. Regulation of hepatic glutathione synthesis: Current concepts and controversies. FASEB J. 1999, 13, 1169–1183. [Google Scholar] [CrossRef] [Green Version]
- Perrone, S.; Laschi, E.; Buonocore, G. Biomarkers of oxidative stress in the fetus and in the newborn. Free. Radic. Biol. Med. 2019, 142, 23–31. [Google Scholar] [CrossRef]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, C. 8-hydroxy-2′-deoxyguanosine (8-OHdG): A Critical Biomarker of Oxidative Stress and Carcinogenesis. J. Environ. Sci. Health Part C 2009, 27, 120–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, C.L.; Kosyk, O.; Ross, P.K.; Schoonhoven, R.; Boysen, G.; Swenberg, J.A.; Heinloth, A.N.; Boorman, G.A.; Cunningham, M.L.; Paules, R.S.; et al. Phenotypic Anchoring of Acetaminophen-Induced Oxidative Stress with Gene Expression Profiles in Rat Liver. Toxicol. Sci. 2006, 93, 213–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghavan, R.; Selhub, J.; Paul, L.; Ji, Y.; Wang, G.; Hong, X.; Zuckerman, B.; Fallin, M.D.; Wang, X. A prospective birth cohort study on cord blood folate subtypes and risk of autism spectrum disorder. Am. J. Clin. Nutr. 2020, 112, 1304–1317. [Google Scholar] [CrossRef]
- Wang, X. Maternal Cigarette Smoking, Metabolic Gene Polymorphism, and Infant Birth Weight. JAMA 2002, 287, 195–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.; Divall, S.; Radovick, S.; Paige, D.; Ning, Y.; Chen, Z.; Ji, Y.; Hong, X.; Walker, S.O.; Caruso, D.; et al. Preterm Birth and Random Plasma Insulin Levels at Birth and in Early Childhood. JAMA 2014, 311, 587–596. [Google Scholar] [CrossRef]
- Hong, X.; Liang, L.; Sun, Q.; Keet, C.A.; Tsai, H.-J.; Ji, Y.; Wang, G.; Ji, H.; Clish, C.; Pearson, C.; et al. Maternal triacylglycerol signature and risk of food allergy in offspring. J. Allergy Clin. Immunol. 2019, 144, 729–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steen, J.; Loeys, T.; Moerkerke, B.; Vansteelandt, S. Medflex: An R Package for Flexible Mediation Analysis using Natural Effect Models. J. Stat. Softw. 2017, 76, 1–46. [Google Scholar] [CrossRef] [Green Version]
- Thapar, A.; Cooper, M.; Jefferies, R.; Stergiakouli, E. What causes attention deficit hyperactivity disorder? Arch. Dis. Child. 2011, 97, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Gustafsson, P.; Källén, K. Perinatal, maternal, and fetal characteristics of children diagnosed with attention-deficit-hyperactivity disorder: Results from a population-based study utilizing the Swedish Medical Birth Register. Dev. Med. Child Neurol. 2010, 53, 263–268. [Google Scholar] [CrossRef]
- Verlaet, A.A.J.; Breynaert, A.; Ceulemans, B.; De Bruyne, T.; Fransen, E.; Pieters, L.; Savelkoul, H.F.J.; Hermans, N. Oxidative stress and immune aberrancies in attention-deficit/hyperactivity disorder (ADHD): A case–control comparison. Eur. Child Adolesc. Psychiatry 2018, 28, 719–729. [Google Scholar] [CrossRef]
- Oztop, D.; Altun, H.; Baskol, G.; Ozsoy, S. Oxidative stress in children with attention deficit hyperactivity disorder. Clin. Biochem. 2012, 45, 745–748. [Google Scholar] [CrossRef]
- Levine, R.L.; Moskovitz, J.; Stadtman, E.R. Oxidation of Methionine in Proteins: Roles in Antioxidant Defense and Cellular Regulation. IUBMB Life 2001, 50, 301–307. [Google Scholar] [CrossRef]
- Buckley, N.A.; Dawson, A.; Isbister, G.K. Treatments for paracetamol poisoning. BMJ 2016, 353, i2579. [Google Scholar] [CrossRef]
- Buckley, N.; Eddleston, M. Paracetamol (acetaminophen) poisoning. BMJ Clin. Evid. 2007, 2101. [Google Scholar]
- Gao, J.; Cahill, C.M.; Huang, X.; Roffman, J.L.; Lamon-Fava, S.; Fava, M.; Mischoulon, D.; Rogers, J.T. S-Adenosyl Methionine and Transmethylation Pathways in Neuropsychiatric Diseases Throughout Life. Neurotherapeutics 2018, 15, 156–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; as Work Group of the American Psychiatric Association Council on Research; Gerbarg, P.; Bottiglieri, T.; Massoumi, L.; Carpenter, L.L.; Lavretsky, H.; Muskin, P.R.; Brown, R.P.; Mischoulon, D. S-Adenosylmethionine (SAMe) for Neuropsychiatric Disorders. J. Clin. Psychiatry 2017, 78, e656–e667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shekim, W.O.; Antun, F.; Hanna, G.; McCracken, J.T.; Hess, E.B. S-adenosyl-L-methionine (SAM) in adults with ADHD, RS: Preliminary results from an open trial. Psychopharmacol. Bull. 1990, 26, 249–253. [Google Scholar]
- Green, T.; Steingart, L.; Frisch, A.; Zarchi, O.; Weizman, A.; Gothelf, R. The feasibility and safety of S-adenosyl-l-methionine (SAMe) for the treatment of neuropsychiatric symptoms in 22q11.2 deletion syndrome: A double-blind placebo-controlled trial. J. Neural Transm. 2012, 119, 1417–1423. [Google Scholar] [CrossRef]
- Terneus, M.V.; Brown, J.M.; Carpenter, A.B.; Valentovic, M.A. Comparison of S-adenosyl-l-methionine (SAMe) and N-acetylcysteine (NAC) protective effects on hepatic damage when administered after acetaminophen overdose. Toxicology 2008, 244, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.M.; Ball, J.G.; Wright, M.S.; Van Meter, S.; Valentovic, M.A. Novel protective mechanisms for S-adenosyl-l-methionine against acetaminophen hepatotoxicity: Improvement of key antioxidant enzymatic function. Toxicol. Lett. 2012, 212, 320–328. [Google Scholar] [CrossRef] [Green Version]
- Rees, W.D.; Wilson, F.A.; Maloney, C. Sulfur Amino Acid Metabolism in Pregnancy: The Impact of Methionine in the Maternal Diet. J. Nutr. 2006, 136, 1701S–1705S. [Google Scholar] [CrossRef]
- Brown, J.M.; Ball, J.G.; Hogsett, A.; Williams, T.; Valentovic, M. Temporal study of acetaminophen (APAP) and S-adenosyl-l-methionine (SAMe) effects on subcellular hepatic SAMe levels and methionine adenosyltransferase (MAT) expression and activity. Toxicol. Appl. Pharmacol. 2010, 247, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Thomas, B.; Gruca, L.L.; Bennett, C.; Parimi, P.S.; Hanson, R.W.; Kalhan, S. Metabolism of Methionine in the Newborn Infant: Response to the Parenteral and Enteral Administration of Nutrients. Pediatr. Res. 2008, 64, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Hernandes, M.S.; Troncone, L.R.P. Glycine as a neurotransmitter in the forebrain: A short review. J. Neural Transm. 2009, 116, 1551–1560. [Google Scholar] [CrossRef]
- Javitt, D.C.; Sershen, H.; Hashim, A.; Lajtha, A. Inhibition of striatal dopamine release by glycine and glycyldodecylamide. Brain Res. Bull. 2000, 52, 213–216. [Google Scholar] [CrossRef]
- Tripp, G.; Wickens, J. Neurobiology of ADHD. Neuropharmacology 2009, 57, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.P.-C.; Lane, H.-Y.; Tsai, G. Attention Deficit Hyperactivity Disorder and N-methyl-D-aspartate (NMDA) Dysregulation. Curr. Pharm. Des. 2014, 20, 5180–5185. [Google Scholar] [CrossRef] [PubMed]
- Kon, K.; Ikejima, K.; Okumura, K.; Aoyama, T.; Arai, K.; Takei, Y.; Lemasters, J.J.; Sato, N. Role of apoptosis in acetaminophen hepatotoxicity. J. Gastroenterol. Hepatol. 2007, 22, S49–S52. [Google Scholar] [CrossRef]
- Parashar, A. Pharmacological screening of glycine amino acid prodrug of acetaminophen. Indian J. Pharmacol. 2015, 47, 202–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppert, B.; Havdahl, A.; Riglin, L.; Jones, H.J.; Zheng, J.; Smith, G.D.; Tilling, K.; Thapar, A.; Reichborn-Kjennerud, T.; Stergiakouli, E. Association of Maternal Neurodevelopmental Risk Alleles With Early-Life Exposures. JAMA Psychiatry 2019, 76, 834–842. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.Z.; Swan, S.H.; Kriebel, D.; Liew, Z.; Taylor, H.S.; Bornehag, C.-G.; Andrade, A.M.; Olsen, J.; Jensen, R.H.; Mitchell, R.T.; et al. Paracetamol use during pregnancy—A call for precautionary action. Nat. Rev. Endocrinol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T.; Song, M. ADHD and Early Experience: Revisiting the Case of Low Birth Weight. Pediatrics 2017, 141, e20173488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momany, A.M.; Kamradt, J.M.; Nikolas, M.A. A Meta-Analysis of the Association Between Birth Weight and Attention Deficit Hyperactivity Disorder. J. Abnorm. Child Psychol. 2017, 46, 1409–1426. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, E.; Sjölander, A.; Almqvist, C.; Anckarsäter, H.; D’Onofrio, B.M.; Lichtenstein, P.; Larsson, H. Birth weight as an independent predictor of ADHD symptoms: A within-twin pair analysis. J. Child Psychol. Psychiatry 2014, 56, 453–459. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Cord Acetaminophen ≤50th Percentile | Cord Acetaminophen >50th Percentile | p-Value b | % Missing c |
|---|---|---|---|---|---|
| n | 568 | 284 | 284 | ||
| Childhood ADHD diagnosis, n (%) | 248 | 97 (34.2%) | 151 (53.2%) | <0.001 * | |
| Maternal age (years), mean (SD) | 28.0 (6.6) | 28.0 (6.4) | 28.0 (6.8) | 0.973 | |
| Nulliparous, n (%) | 243 | 112 (39.4%) | 131 (46.1%) | 0.107 | |
| Maternal Race or ethnicity, n (%) | 0.111 | ||||
| Black | 276 | 190 (66.9%) | 186 (65.5%) | ||
| White | 32 | 12 (4.2%) | 20 (7.0%) | ||
| Hispanic | 118 | 55 (19.4%) | 63 (22.2%) | ||
| Other | 42 | 27 (9.5%) | 15 (5.3%) | ||
| Maternal Education, n (%) | 0.855 | 0.53% | |||
| Below College Degree | 396 | 199 (70.1%) | 197 (69.4%) | ||
| College Degree or Above | 172 | 85 (29.9%) | 97 (30.6%) | ||
| Maternal BMI (kg/m2), mean (SD) | 26.4 (6.1) | 26.0 (6.2) | 26.7 (5.9) | 0.170 | 5.46% |
| Maternal smoking,n (%) | 0.005 * | 1.23% | |||
| Never | 484 | 255 (89.8%) | 229 (80.6%) | ||
| Quit | 33 | 14 (4.9%) | 19 (6.7%) | ||
| Continuous | 51 | 15 (5.3%) | 36 (12.7%) | ||
| Maternal alcohol use before or during pregnancy, n (%) | 0.107 | 4.05% | |||
| No | 535 | 272 (85.8%) | 263 (92.6%) | ||
| Yes | 33 | 12 (4.2%) | 21 (7.4%) | ||
| Marital Status, n (%) | 0.181 | 0.88% | |||
| Not Married | 381 | 183 (64.4%) | 198 (69.7%) | ||
| Married | 187 | 101 (35.6%) | 86 (30.3%) | ||
| Child age in years by last visit, mean (SD) | 9.3 (3.5) | 9.6 (3.5) | 9.1 (3.4) | 0.129 | |
| Child Sex, n (%) | 0.205 | ||||
| Male | 315 | 150 (52.8%) | 165 (58.1%) | ||
| Female | 253 | 134 (47.2%) | 119 (41.9%) | ||
| Delivery type, n (%) | 0.857 | 0.53% | |||
| Cesarean | 180 | 91 (32.0%) | 89 (31.3%) | ||
| Vaginal | 388 | 193 (68.0%) | 195 (68.7%) | ||
| Preterm, n (%) | 0.051 | ||||
| No | 490 | 253 (89.1%) | 237 (83.5%) | ||
| Yes | 78 | 31 (10.9%) | 47 (16.5%) | ||
| Low Birthweight, n (%) | 0.002 c,* | 0.18% | |||
| No | 482 | 254 (89.4%) | 228 (80.3%) | ||
| Yes | 86 | 30 (10.6%) | 56 (19.7%) | ||
| Stress During Pregnancy, n (%) | 0.444 | 0.88% | |||
| Mild | 219 | 116 (40.8%) | 103 (36.3%) | ||
| Average | 246 | 121 (42.6%) | 125 (44.0%) | ||
| Severe | 103 | 47 (16.5%) | 56 (19.7%) | ||
| Maternal Fever During Pregnancy, n (%) | 0.844 | 5.11% | |||
| No | 541 | 271 (95.4%) | 270 (95.1%) | ||
| Yes | 27 | 13 (4.6%) | 14 (4.9%) | ||
| Cord methionine a (mean, SD) | 0.04 (0.99) | −0.28 (0.93) | 0.37 (0.94) | <0.001 * | |
| Cord serine a (mean, SD) | 0.01 (0.98) | −0.31 (0.90) | 0.33 (0.96) | <0.001 * | |
| Cord glycine a (mean, SD) | 0.03 (1.01) | −0.33 (0.91) | 0.39 (0.98) | <0.001 * | |
| Cord glutamate a (mean, SD) | 0.06 (1.00) | −0.13 (1.01) | 0.24 (0.95) | <0.001 * | |
| Cord 8-hydroxy-deoxyguanosine a (mean, SD) | 0.08 (0.95) | 0.06 (0.93) | 0.10 (0.98) | 0.604 |
| Unadjusted Logistic | Adjusted Logistic d | |||||||
|---|---|---|---|---|---|---|---|---|
| n | Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | ||
| ADHD only a | 568 | |||||||
| regressions for individual metabolites b | ||||||||
| acetaminophen >50th percentilec | 2.23 | (1.59, 3.13) | <0.001 * | 2.10 | (1.43, 3.11) | <0.001 * | ||
| methionine | 1.34 | (1.13, 1.60) | 0.001 * | 1.43 | (1.17, 1.77) | 0.001 * | ||
| glycine | 1.33 | (1.12, 1.57) | 0.001 * | 1.38 | (1.14, 1.68) | 0.001 * | ||
| serine | 1.26 | (1.07, 1.50) | 0.008 * | 1.31 | (1.07, 1.61) | 0.008 * | ||
| glutamate | 1.23 | (1.04, 1.45) | 0.018 * | 1.21 | (0.99, 1.47) | 0.058 | ||
| 8-hydroxy-deoxyguanosine | 1.09 | (0.92, 1.30) | 0.328 | 1.24 | (1.01, 1.52) | 0.039 * | ||
| regression with both acetaminophen and methionine b | ||||||||
| acetaminophen >50th percentile c | 1.98 | (1.39, 2.84) | <0.001 * | 1.79 | (1.19, 2.71) | 0.005 * | ||
| methionine | 1.20 | (1.00, 1.45) | 0.050 | 1.30 | (1.05, 1.62) | 0.018 * | ||
| regression with both acetaminophen and serine b | ||||||||
| acetaminophen >50th percentile c | 2.07 | (1.45, 2.97) | <0.001 * | 1.89 | (1.26, 2.87) | 0.002 * | ||
| serine | 1.12 | (0.93, 1.35) | 0.217 | 1.18 | (0.95, 1.46) | 0.128 | ||
| regression with both acetaminophen and glycine b | ||||||||
| acetaminophen >50th percentile c | 1.99 | (1.39, 2.85) | <0.001 * | 1.80 | (1.19, 2.73) | 0.005 * | ||
| glycine | 1.18 | (0.99, 1.42) | 0.071 | 1.26 | (1.02, 1.54) | 0.030 * | ||
| regression with both acetaminophen and glutamate b | ||||||||
| acetaminophen >50th percentile c | 2.12 | (1.50, 3.00) | <0.001 * | 2.01 | (1.35, 2.99) | 0.001 * | ||
| serine | 1.15 | (0.96, 1.37) | 0.126 | 1.13 | (0.93, 1.39) | 0.219 | ||
| regression with both acetaminophen and 8-hydroxy-deoxyguanosine b | ||||||||
| acetaminophen >50th percentile c | 2.22 | (1.58, 3.13) | <0.001 * | 2.08 | (1.41, 3.09) | <0.001 * | ||
| 8-hydroxy-deoxyguanosine | 1.08 | (0.91, 1.29) | 0.380 | 1.23 | (1.00, 1.51) | 0.051 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anand, N.S.; Raghavan, R.; Wang, G.; Hong, X.; Azuine, R.E.; Pearson, C.; Zuckerman, B.; Xie, H.; Wang, X. Perinatal Acetaminophen Exposure and Childhood Attention-Deficit/Hyperactivity Disorder (ADHD): Exploring the Role of Umbilical Cord Plasma Metabolites in Oxidative Stress Pathways. Brain Sci. 2021, 11, 1302. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101302
Anand NS, Raghavan R, Wang G, Hong X, Azuine RE, Pearson C, Zuckerman B, Xie H, Wang X. Perinatal Acetaminophen Exposure and Childhood Attention-Deficit/Hyperactivity Disorder (ADHD): Exploring the Role of Umbilical Cord Plasma Metabolites in Oxidative Stress Pathways. Brain Sciences. 2021; 11(10):1302. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101302
Chicago/Turabian StyleAnand, Neha S., Ramkripa Raghavan, Guoying Wang, Xiumei Hong, Romuladus E. Azuine, Colleen Pearson, Barry Zuckerman, Hehuang Xie, and Xiaobin Wang. 2021. "Perinatal Acetaminophen Exposure and Childhood Attention-Deficit/Hyperactivity Disorder (ADHD): Exploring the Role of Umbilical Cord Plasma Metabolites in Oxidative Stress Pathways" Brain Sciences 11, no. 10: 1302. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101302