
MEG Node Degree Differences in Patients with Focal Epilepsy vs. Controls—Influence of Experimental Conditions

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Controls
2.3. Patients
2.4. MRI Scan
2.5. MEG Recording
2.6. MEG Data Analysis
2.6.1. Pre-Processing
2.6.2. Source Analysis
2.6.3. Connectivity and Graph Analysis
2.6.4. Power Analysis
2.7. Statistics
3. Results
3.1. Eyes-Opened Compared to Eyes-Closed
3.2. Eyes-Closed before and after a Demanding Task
3.3. ICC Evaluation of Control Data
3.4. Healthy Controls Compared to Patients with Focal Epilepsy
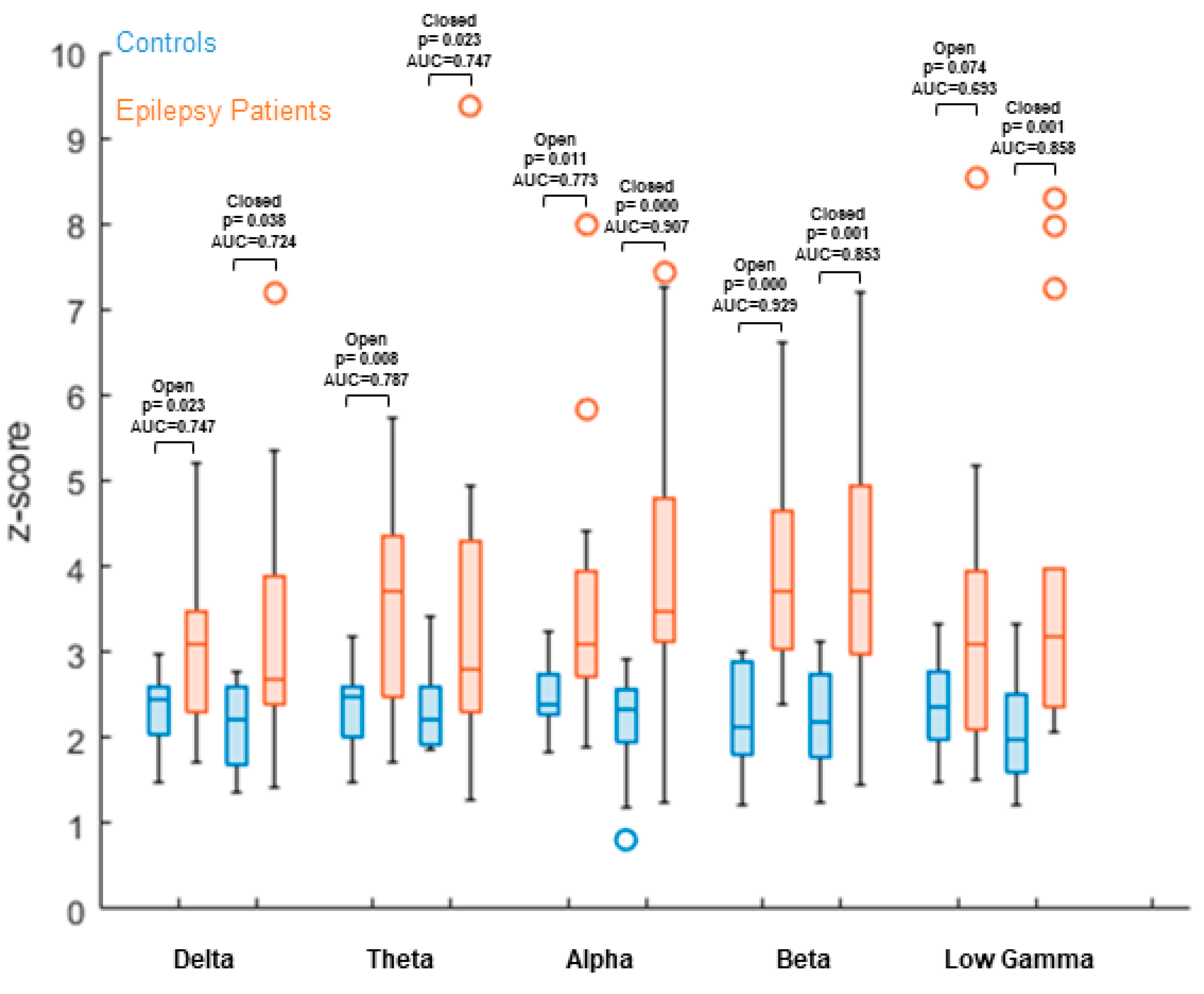
3.5. Node Degree Comparison between Healthy Controls at Different Experimental Conditions and Patients
3.6. Comparison of Power between Patients and Controls
3.7. Correlation of maxND and IED Rate
4. Discussion
4.1. Increased Node Degree as a Correlate of Epilepsy
4.2. Influence of Vigilance
4.3. Delta
4.4. Beta
4.5. Expected Alpha/Low Gamma Alterations in Open vs. Closed Eyes
4.6. Power Comparison
4.7. Limitations and Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pitkänen, A.; Löscher, W.; Vezzani, A.; Becker, A.J.; Simonato, M.; Lukasiuk, K.; Gröhn, O.; Bankstahl, J.P.; Friedman, A.; Aronica, E.; et al. Advances in the development of biomarkers for epilepsy. Lancet Neurol. 2016, 15, 843–856. [Google Scholar] [CrossRef]
- Sultana, B.; Panzini, M.-A.; Carpentier, A.V.; Comtois, J.; Rioux, B.; Gore, G.; Bauer, P.R.; Kwon, C.-S.; Jetté, N.; Josephson, C.B.; et al. Incidence and Prevalence of Drug-Resistant Epilepsy. Neurology 2021, 96, 805–817. [Google Scholar] [CrossRef]
- Fiest, K.M.; Sajobi, T.T.; Wiebe, S. Epilepsy surgery and meaningful improvements in quality of life: Results from a randomized controlled trial. Epilepsia 2014, 55, 886–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, J.; Liu, S.; Qin, H.; Li, B.; Zhang, X. Drug-Resistant Epilepsy and Surgery. Curr. Neuropharmacol. 2017, 16, 17–28. [Google Scholar] [CrossRef]
- Lee, S.K.; Lee, S.Y.; Kim, K.-K.; Hong, K.-S.; Lee, D.-S.; Chung, C.K. Surgical outcome and prognostic factors of cryptogenic neocortical epilepsy. Ann. Neurol. 2005, 58, 525–532. [Google Scholar] [CrossRef]
- Chapman, K.; Wyllie, E.; Najm, I.; Ruggieri, P.; Bingaman, W.; Lüders, J.; Kotagal, P.; Lachhwani, D.; Dinner, D.; Lüders, H.O. Seizure outcome after epilepsy surgery in patients with normal preoperative MRI. J. Neurol. Neurosurg. Psychiatry 2005, 76, 710–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noe, K.H.; Sulc, V.; Wong-Kisiel, L.; Wirrell, E.C.; Van Gompel, J.J.; Wetjen, N.M.; Britton, J.W.; So, E.; Cascino, G.D.; Marsh, W.R.; et al. Long-term Outcomes After Nonlesional Extratemporal Lobe Epilepsy Surgery. JAMA Neurol. 2013, 70, 1003–1008. [Google Scholar] [CrossRef]
- Blumcke, I.; Spreafico, R.; Haaker, G.; Coras, R.; Kobow, K.; Bien, C.G.; Pfäfflin, M.; Elger, C.; Widman, G.; Schramm, J.; et al. Histopathological Findings in Brain Tissue Obtained during Epilepsy Surgery. N. Engl. J. Med. 2017, 377, 1648–1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, M.; Keller, S.; Nicolson, A.; Biswas, S.; Smith, D.; Farah, J.O.; Eldridge, P.; Wieshmann, U. The long-term outcomes of epilepsy surgery. PLoS ONE 2018, 13, e0196274. [Google Scholar] [CrossRef] [Green Version]
- De Tisi, J.; Bell, G.S.; Peacock, J.L.; McEvoy, A.W.; Harkness, W.F.; Sander, J.; Duncan, J.S. The long-term outcome of adult epilepsy surgery, patterns of seizure remission, and relapse: A cohort study. Lancet 2011, 378, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Gelžinienė, G.; Endzinienė, M.; Vaičienė, N.; Magistris, M.R.; Seeck, M. Presurgical evaluation of epilepsy patients. Medicina 2008, 44, 585–592. [Google Scholar] [CrossRef] [Green Version]
- Rathore, C.; Radhakrishnan, K. Concept of epilepsy surgery and presurgical evaluation. Epileptic Disord 2015, 17, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Sommer, B.; Roessler, K.; Rampp, S.; Hamer, H.M.; Blumcke, I.; Stefan, H.; Buchfelder, M. Magnetoencephalography-guided surgery in frontal lobe epilepsy using neuronavigation and intraoperative MR imaging. Epilepsy Res. 2016, 126, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, B.; Fu, L.; Cui, Z. Use of interictal 18F-fluorodeoxyglucose (FDG)-PET and magnetoencephalography (MEG) to localize epileptogenic foci in non-lesional epilepsy in a cohort of 16 patients. J. Neurol. Sci. 2015, 355, 120–124. [Google Scholar] [CrossRef]
- Sutherling, W.W.; Mamelak, A.N.; Thyerlei, D.; Maleeva, T.; Minazad, Y.; Philpott, L.; Lopez, N. Influence of magnetic source imaging for planning intracranial EEG in epilepsy. Neurology 2008, 71, 990–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rampp, S.; Stefan, H.; Wu, X.; Kaltenhäuser, M.; Maess, B.; Schmitt, F.C.; Wolters, C.H.; Hamer, H.; Kasper, B.S.; Schwab, S.; et al. Magnetoencephalography for epileptic focus localization in a series of 1000 cases. Brain 2019, 142, 3059–3071. [Google Scholar] [CrossRef] [PubMed]
- Englot, D.J.; Hinkley, L.B.; Kort, N.S.; Imber, B.S.; Mizuiri, D.; Honma, S.M.; Findlay, A.M.; Garrett, C.; Cheung, P.L.; Mantle, M.; et al. Global and regional functional connectivity maps of neural oscillations in focal epilepsy. Brain 2015, 138, 2249–2262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knake, S.; Halgren, E.; Shiraishi, H.; Hara, K.; Hamer, H.; Grant, P.; Carr, V.; Foxe, D.; Camposano, S.; Busa, E.; et al. The value of multichannel MEG and EEG in the presurgical evaluation of 70 epilepsy patients. Epilepsy Res. 2006, 69, 80–86. [Google Scholar] [CrossRef] [PubMed]
- De Tiège, X.; Lundqvist, D.; Beniczky, S.; Seri, S.; Paetau, R. Current clinical magnetoencephalography practice across Europe: Are we closer to use MEG as an established clinical tool? Seizure 2017, 50, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, B.; Vlachos, I.; Wang, Z.; Mosher, J.; Najm, I.; Burgess, R.; Iasemidis, L.; Alexopoulos, A. Epileptic focus localization based on resting state interictal MEG recordings is feasible irrespective of the presence or absence of spikes. Clin. Neurophysiol. 2015, 126, 667–674. [Google Scholar] [CrossRef]
- Hegner, Y.L.; Marquetand, J.; Elshahabi, A.; Klamer, S.; Lerche, H.; Braun, C.; Focke, N.K. Increased Functional MEG Connectivity as a Hallmark of MRI-Negative Focal and Generalized Epilepsy. Brain Topogr. 2018, 31, 863–874. [Google Scholar] [CrossRef]
- Van Mierlo, P.; Höller, Y.; Focke, N.K.; Vulliemoz, S. Network Perspectives on Epilepsy Using EEG/MEG Source Connectivity. Front. Neurol. 2019, 10, 721. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.A.; Cash, S.S. Epilepsy as a Disorder of Cortical Network Organization. Neuroscience 2012, 18, 360–372. [Google Scholar] [CrossRef] [PubMed]
- Friston, K.J. Functional and Effective Connectivity: A Review. Brain Connect. 2011, 1, 13–36. [Google Scholar] [CrossRef] [PubMed]
- Jiruska, P.; de Curtis, M.; Jefferys, J.; Schevon, C.A.; Schiff, S.J.; Schindler, K. Synchronization and desynchronization in epilepsy: Controversies and hypotheses. J. Physiol. 2013, 591, 787–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De, R.N.J. Epilepsy and the Functional Anatomy of the Human Brain. Neurology 1954, 4, 483. [Google Scholar] [CrossRef]
- Boccaletti, S.; Latora, V.; Moreno, Y.; Chavez, M.; Hwang, D.-U. Complex networks: Structure and dynamics. Phys. Rep. 2006, 424, 175–308. [Google Scholar] [CrossRef]
- Bettus, G.; Wendling, F.; Guye, M.; Valton, L.; Régis, J.; Chauvel, P.; Bartolomei, F. Enhanced EEG functional connectivity in mesial temporal lobe epilepsy. Epilepsy Res. 2008, 81, 58–68. [Google Scholar] [CrossRef]
- Wu, T.; Ge, S.; Zhang, R.; Liu, H.; Chen, Q.; Zhao, R.; Yin, Y.; Lv, X.; Jiang, T. Neuromagnetic coherence of epileptic activity: An MEG study. Seizure 2014, 23, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Elshahabi, A.; Klamer, S.; Sahib, A.K.; Lerche, H.; Braun, C.; Focke, N.K. Magnetoencephalography Reveals a Widespread Increase in Network Connectivity in Idiopathic/Genetic Generalized Epilepsy. PLoS ONE 2015, 10, e0138119. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.T.; Falahpour, M. Vigilance Effects in Resting-State fMRI. Front. Neurosci. 2020, 14, 321. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Ramírez, J.; Freedman, S.; Mateos, D.; Pérez-Velázquez, J.L.; Valiante, T. Eyes Closed or Eyes Open? Exploring the Alpha Desynchronization Hypothesis in Resting State Functional Connectivity Networks with Intracranial EEG. bioRxiv 2017, 118174. [Google Scholar] [CrossRef] [Green Version]
- Colclough, G.; Woolrich, M.; Tewarie, P.; Brookes, M.; Quinn, A.; Smith, S. How reliable are MEG resting-state connectivity metrics? NeuroImage 2016, 138, 284–293. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Seeck, M.; Beniczky, S. Accuracy of Interictal and Ictal Electric and Magnetic Source Imaging: A Systematic Review and Meta-Analysis. Front. Neurol. 2019, 10, 1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquetand, J.; Vannoni, S.; Carboni, M.; Hegner, Y.L.; Stier, C.; Braun, C.; Focke, N.K. Reliability of Magnetoencephalography and High-Density Electroencephalography Resting-State Functional Connectivity Metrics. Brain Connect. 2019, 9, 539–553. [Google Scholar] [CrossRef] [PubMed]
- Coquelet, N.; De Tiège, X.; Destoky, F.; Roshchupkina, L.; Bourguignon, M.; Goldman, S.; Peigneux, P.; Wens, V. Comparing MEG and high-density EEG for intrinsic functional connectivity mapping. NeuroImage 2020, 210, 116556. [Google Scholar] [CrossRef] [PubMed]
- Aydin, Ü.; Vorwerk, J.; Dümpelmann, M.; Küpper, P.; Kugel, H.; Heers, M.; Wellmer, J.; Kellinghaus, C.; Haueisen, J.; Rampp, S.; et al. Combined EEG/MEG Can Outperform Single Modality EEG or MEG Source Reconstruction in Presurgical Epilepsy Diagnosis. PLoS ONE 2015, 10, e0118753. [Google Scholar] [CrossRef] [Green Version]
- Kwan, P.; Arzimanoglou, A.; Berg, A.T.; Brodie, M.J.; Allen Hauser, W.; Mathern, G.; Moshé, S.L.; Perucca, E.; Wiebe, S.; French, J. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2010, 51, 1069–1077. [Google Scholar] [CrossRef]
- Nolte, G. The magnetic lead field theorem in the quasi-static approximation and its use for magnetoencephalography forward calculation in realistic volume conductors. Phys. Med. Biol. 2003, 48, 3637–3652. [Google Scholar] [CrossRef]
- Jung, T.-P.; Makeig, S.; Bell, A.J.; Sejnowski, T.J. Independent Component Analysis of Electroencephalographic and Event-Related Potential Data. In Central Auditory Processing and Neural Modeling; Springer: Singapore, 1998; pp. 189–197. [Google Scholar]
- Tzoutio-Mazoyera, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Tzourio-Mazoyer, B.; Joliot, M. Automated Anatomical Labeling of Activations in SPM Using a Macroscopic Anatomical Parcellation of the MNI MRI Single-Subject Brain. NeuroImage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Chen, G.; Taylor, P.A.; Haller, S.P.; Kircanski, K.; Stoddard, J.; Pine, D.S.; Leibenluft, E.; Brotman, M.A.; Cox, R.W. Intraclass correlation: Improved modeling approaches and applications for neuroimaging. Hum. Brain Mapp. 2018, 39, 1187–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maris, E.; Oostenveld, R. Nonparametric statistical testing of EEG- and MEG-data. J. Neurosci. Methods 2007, 164, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niso, G.; Carrasco, S.; Gudín, M.; Maestú, F.; Del-Pozo, F.; Pereda, E. What graph theory actually tells us about resting state interictal MEG epileptic activity. NeuroImage Clin. 2015, 8, 503–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, C.-Y.Z.; He, Y.; Lin, C.-P. Graph theoretical analysis of human brain structural networks. Rev. Neurosci. 2011, 22, 551–563. [Google Scholar] [CrossRef]
- He, Y.; Evans, A. Graph theoretical modeling of brain connectivity. Curr. Opin. Neurol. 2010, 23, 341–350. [Google Scholar] [CrossRef] [Green Version]
- Rampp, S.; Rössler, K.; Hamer, H.; Illek, M.; Buchfelder, M.; Doerfler, A.; Pieper, T.; Hartlieb, T.; Kudernatsch, M.; Koelble, K.; et al. Dysmorphic neurons as cellular source for phase-amplitude coupling in Focal Cortical Dysplasia Type II. Clin. Neurophysiol. 2021, 132, 782–792. [Google Scholar] [CrossRef]
- Noh, B.H.; Berg, A.T.; Nordli, D.R. Concordance of MRI lesions and EEG focal slowing in children with nonsyndromic epilepsy. Epilepsia 2013, 54, 455–460. [Google Scholar] [CrossRef]
- Di Gennaro, G.; Quarato, P.P.; Sebastiano, F.; Esposito, V.; Onorati, P.; Mascia, A.; Romanelli, P.; Grammaldo, L.G.; Falco, C.; Scoppetta, C.; et al. Postoperative EEG and seizure outcome in temporal lobe epilepsy surgery. Clin. Neurophysiol. 2004, 115, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Van Dellen, E.; Douw, L.; Hillebrand, A.; Ris-Hilgersom, I.H.M.; Schoonheim, M.; Baayen, J.C.; Hamer, P.D.W.; Velis, D.N.; Klein, M.; Heimans, J.J.; et al. MEG Network Differences between Low- and High-Grade Glioma Related to Epilepsy and Cognition. PLoS ONE 2012, 7, e50122. [Google Scholar] [CrossRef]
- Jin, S.-H.; Jeong, W.; Chung, C.K. Focal cortical dysplasia alters electrophysiological cortical hubs in the resting-state. Clin. Neurophysiol. 2014, 126, 1482–1492. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.; Jin, S.-H.; Kim, M.; Kim, J.S.; Chung, C.K. Abnormal functional brain network in epilepsy patients with focal cortical dysplasia. Epilepsy Res. 2014, 108, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Nolte, G.; Bai, O.; Wheaton, L.; Mari, Z.; Vorbach, S.; Hallett, M. Identifying true brain interaction from EEG data using the imaginary part of coherency. Clin. Neurophysiol. 2004, 115, 2292–2307. [Google Scholar] [CrossRef]
- Demirakca, T.; Cardinale, V.; Dehn, S.; Ruf, M.; Ende, G. The Exercising Brain: Changes in Functional Connectivity Induced by an Integrated Multimodal Cognitive and Whole-Body Coordination Training. Neural Plast. 2016, 2016, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Román, F.J.; Medina, Y.I.; Martínez, K.; Karama, S.; Burgaleta, M.; Evans, A.C.; Jaeggi, S.M.; Colom, R. Enhanced structural connectivity within a brain sub-network supporting working memory and engagement processes after cognitive training. Neurobiol. Learn. Mem. 2017, 141, 33–43. [Google Scholar] [CrossRef]
- Cross, N.; Paquola, C.; Pomares, F.B.; Perrault, A.A.; Jegou, A.; Nguyen, A.; Aydin, U.; Bernhardt, B.C.; Grova, C.; Dang-Vu, T.T. Cortical gradients of functional connectivity are robust to state-dependent changes following sleep deprivation. NeuroImage 2021, 226, 117547. [Google Scholar] [CrossRef]
- Chengyang, L.; Daqing, H.; Jianlin, Q.; Haisheng, C.; Qingqing, M.; Jin, W.; Jiajia, L.; Enmao, Y.; Yongcong, S.; Xi, Z. Short-term memory deficits correlate with hippocampal-thalamic functional connectivity alterations following acute sleep restriction. Brain Imaging Behav. 2017, 11, 954–963. [Google Scholar] [CrossRef]
- Shao, Y.; Wang, L.; Ye, E.; Jin, X.; Ni, W.; Yang, Y.; Wen, B.; Hu, D.; Yang, Z. Decreased Thalamocortical Functional Connectivity after 36 Hours of Total Sleep Deprivation: Evidence from Resting State fMRI. PLoS ONE 2013, 8, e78830. [Google Scholar] [CrossRef]
- Schönherr, M.; Stefan, H.; Hamer, H.M.; Rössler, K.; Buchfelder, M.; Rampp, S. The delta between postoperative seizure freedom and persistence: Automatically detected focal slow waves after epilepsy surgery. NeuroImage Clin. 2017, 13, 256–263. [Google Scholar] [CrossRef]
- Kaltenhäuser, M.; Scheler, G.; Rampp, S.; Paulini, A.; Stefan, H. Spatial intralobar correlation of spike and slow wave activity localisations in focal epilepsies: A MEG analysis. NeuroImage 2007, 34, 1466–1472. [Google Scholar] [CrossRef]
- Hooshmand, H.; Morganroth, R.; Corredor, C. Significance of Focal and Lateralized Beta Activity in the EEG. Clin. Electroencephalogr. 1980, 11, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Heers, M.; Hirschmann, J.; Jacobs, J.; Dümpelmann, M.; Butz, M.; von Lehe, M.; Elger, C.E.; Schnitzler, A.; Wellmer, J. Frequency domain beamforming of magnetoencephalographic beta band activity in epilepsy patients with focal cortical dysplasia. Epilepsy Res. 2014, 108, 1195–1203. [Google Scholar] [CrossRef]
- Wang, B.; Meng, L. Functional brain network alterations in epilepsy: A magnetoencephalography study. Epilepsy Res. 2016, 126, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Marcuse, L.V.; Fields, M.C.; Yoo, J. The normal adult EEG. In Rowan’s Primer of EEG.; Elsevier BV: Amsterdam, The Netherlands, 2016; pp. 39–66. [Google Scholar]
- Park, S.-P.; Kwon, O.-Y. Increased EEG Current-Source Density in the High Beta Frequency Band Induced by Levetiracetam Adjunctive Therapy in Refractory Partial Epilepsy. J. Clin. Neurol. 2009, 5, 178–185. [Google Scholar] [CrossRef]
- Berger, H. Über Das Elektrenkephalogramm Des Menschen. Available online: https://www.scirp.org/(S(i43dyn45teexjx455qlt3d2q))/reference/ReferencesPapers.aspx?ReferenceID=6553 (accessed on 5 July 2021).
- Adrian, E.D.; Matthews, B.H.C. The Berger Rhythm: Potential Changes from the Occipital Lobes in Man. Brain 1934, 57, 355–385. [Google Scholar] [CrossRef]
- Smith, J.R. The Electroencephalogram during Normal Infancy and Childhood: II. The Nature of the Growth of the Alpha Waves. Pedagog. Semin. J. Genet. Psychol. 1938, 53, 455–469. [Google Scholar] [CrossRef]
- Agcaoglu, O.; Wilson, T.W.; Wang, Y.; Stephen, J.; Calhoun, V.D. Resting state connectivity differences in eyes open versus eyes closed conditions. Hum. Brain Mapp. 2019, 40, 2488–2498. [Google Scholar] [CrossRef] [Green Version]
- Bastos, A.M.; Schoffelen, J.-M. A Tutorial Review of Functional Connectivity Analysis Methods and Their Interpretational Pitfalls. Front. Syst. Neurosci. 2016, 9, 175. [Google Scholar] [CrossRef] [Green Version]
- Clemens, B.; Szigeti, G.; Barta, Z. EEG frequency profiles of idiopathic generalised epilepsy syndromes. Epilepsy Res. 2000, 42, 105–115. [Google Scholar] [CrossRef]
- Clemens, B. Valproate decreases EEG synchronization in a use-dependent manner in idiopathic generalized epilepsy. Seizure 2008, 17, 224–233. [Google Scholar] [CrossRef] [Green Version]
- Arzy, S.; Allali, G.; Brunet, D.; Michel, C.M.; Kaplan, P.W.; Seeck, M. Antiepileptic drugs modify power of high EEG frequencies and their neural generators. Eur. J. Neurol. 2010, 17, 1308–1312. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.W.J. Investigating Causal Relations by Econometric Models and Cross-spectral Methods. Econometrica 1969, 37, 424. [Google Scholar] [CrossRef]
- Coito, A.; Biethahn, S.; Tepperberg, J.; Carboni, M.; Roelcke, U.; Seeck, M.; Van Mierlo, P.; Gschwind, M.; Vulliémoz, S. Interictal epileptogenic zone localization in patients with focal epilepsy using electric source imaging and directed functional connectivity from low-density EEG. Epilepsia Open 2019, 4, 281–292. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Age | Sex | Years with Epilepsy | Localization of Epilepsy | Spikes/ 40 min rec. | Etiology |
|---|---|---|---|---|---|---|
| 1 | 34 | f | 35 | left fronto-temporal lobe | 32 | lesional |
| 2 | 44 | f | 11 | right temporal lobe | 9 | lesional |
| 3 | 25 | f | 16 | right fronto-parietal lobe | 0 | non-lesional |
| 4 | 46 | f | 35 | left parieto-occipital lobe | 149 | non-lesional |
| 5 | 60 | f | 48 | left temporal lobe | 14 | non-lesional |
| 6 | 29 | m | 3 | left temporal lobe | 10 | non-lesional |
| 7 | 23 | m | 23 | right centro-cingular | >300 | lesional |
| 8 | 31 | f | 20 | right frontal lobe | 24 | non-lesional |
| 9 | 38 | f | 29 | left hemisphere | 0 | non-lesional |
| 10 | 50 | m | 15 | temporal bilateral | 16 | non-lesional |
| 11 | 24 | m | 15 | left hemisphere | 18 | non-lesional |
| 12 | 24 | m | 6 | right temporal lobe | 3 | non-lesional |
| 13 | 25 | m | 16 | right temporal lobe | 23 | non-lesional |
| 14 | 34 | f | 17 | left temporal lobe | 0 | non-lesional |
| 15 | 23 | f | 7 | right hemisphere | 22 | non-lesional |
| Frequency Bands | Controls Open/Closed | Controls Start/End |
|---|---|---|
| Delta | 0.53 | 0.36 |
| Theta | 0.08 | 0.15 |
| Alpha | 0.29 | 0.13 |
| Beta | −0.21 | 0.13 |
| Low Gamma | 0.48 | −0.39 |
| Frequency Band | Delta | Theta | Alpha | Beta | Low Gamma |
|---|---|---|---|---|---|
| Start | p = 0.023; AUC=0.747 | p = 0.023; AUC = 0.747 | p = 0.000; AUC = 0.907 | p = 0.001; AUC=0.853 | p = 0.001; AUC = 0.858 |
| End | p = 0.038; AUC = 0.724 | p = 0.001; AUC = 0.844 | p = 0.010; AUC = 0.778 | p = 0.005; AUC = 0.800 | p = 0.038; AUC = 0.724 |
| Frequency Band | Delta | Theta | Alpha | Beta | Low Gamma |
|---|---|---|---|---|---|
| Open Eyes | p = 0.038; AUC = 0.724 | p = 0.008; AUC = 0.787 | p = 0.011; AUC = 0.773 | p = 0.000; AUC = 0.929 | p = 0.074; AUC = 0.693 |
| Closed Eyes | p = 0.023; AUC = 0.747 | p = 0.023; AUC = 0.747 | p = 0.000; AUC = 0.907 | p = 0.001; AUC = 0.853 | p = 0.001; AUC = 0.858 |
| Frequency Band | Delta | Theta | Alpha | Beta | Low Gamma |
|---|---|---|---|---|---|
| EC Power/AUC | p = 0.074; AUC = 0.307 | p = 0.014; AUC = 0.236 | p = 0.481; AUC = 0.422 | p = 0.171; AUC = 0.351 | p = 0.407; AUC = 0.591 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vogel, S.; Kaltenhäuser, M.; Kim, C.; Müller-Voggel, N.; Rössler, K.; Dörfler, A.; Schwab, S.; Hamer, H.; Buchfelder, M.; Rampp, S. MEG Node Degree Differences in Patients with Focal Epilepsy vs. Controls—Influence of Experimental Conditions. Brain Sci. 2021, 11, 1590. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121590
Vogel S, Kaltenhäuser M, Kim C, Müller-Voggel N, Rössler K, Dörfler A, Schwab S, Hamer H, Buchfelder M, Rampp S. MEG Node Degree Differences in Patients with Focal Epilepsy vs. Controls—Influence of Experimental Conditions. Brain Sciences. 2021; 11(12):1590. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121590
Chicago/Turabian StyleVogel, Stephan, Martin Kaltenhäuser, Cora Kim, Nadia Müller-Voggel, Karl Rössler, Arnd Dörfler, Stefan Schwab, Hajo Hamer, Michael Buchfelder, and Stefan Rampp. 2021. "MEG Node Degree Differences in Patients with Focal Epilepsy vs. Controls—Influence of Experimental Conditions" Brain Sciences 11, no. 12: 1590. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121590