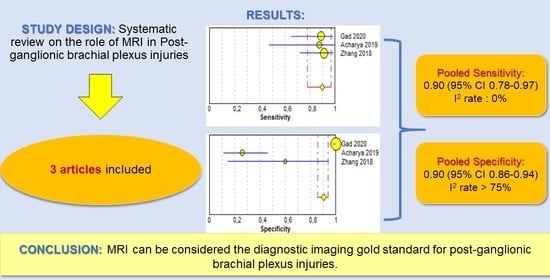
Diagnostic Accuracy of the Magnetic Resonance Imaging in Adult Post-Ganglionic Brachial Plexus Traumatic Injuries: A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , ,  , ,
, ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Database Search
2.3. Study Selection
2.4. Statistical Analysis
3. Results
3.1. Strategy Search
3.2. Methodological Quality Assessment
3.3. Synthesis of Results
- -
- nerve rupture: characterized by different degrees of nerve thickening caused by edema and inflammation with abnormal hyper intense signal in T2/short-tau inversion recovery (STIR) sequences;
- -
- neuroma formation, characterized by a focal thickening of the injured segment of the nerve [17].
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gilcrease-Garcia, B.M.; Deshmukh, S.D.; Parsons, M.S. Anatomy, Imaging, and Pathologic Conditions of the Brachial Plexus. Radio Graph. 2020, 40, 1686–1714. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J. Ultrasound of the Brachial Plexus. Semin. Musculoskelet. Radiol. 2018, 22, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Lutz, A.M.; Gold, G.; Beaulieu, C. MR Imaging of the Brachial Plexus. Neuroimaging Clin. N. Am. 2014, 24, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Wade, R.G.; Takwoingi, Y.; Wormald, J.C.; Ridgway, J.P.; Tanner, S.; Rankine, J.J.; Bourke, G. MRI for detecting root avulsions in traumatic adult brachial plexus injuries: A systematic review and meta-analysis of diagnostic accuracy. Radiology 2019, 193, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Yoshikawa, T.; Hayashi, N.; Yamamoto, S.; Tajiri, Y.; Yoshioka, N.; Masumoto, T.; Mori, H.; Abe, O.; Aoki, S.; Ohtomo, K. Brachial plexus injury: Clinical manifestations, conventional imaging findings, and the latest imaging techniques. Radiographics 2006, 26 (Suppl. 1), S133–S143. [Google Scholar] [CrossRef] [Green Version]
- Fox, I.K.; Mackinnon, S.E. Adult peripheral nerve disorders—Nerve entrapment, repair, transfer and brachial plexus disorders. Plast. Reconstr. Surg. 2011, 127. [Google Scholar] [CrossRef] [Green Version]
- Silbermann-Hoffman, O.; Teboul, F. Post-traumatic brachial plexus MRI in practice. Diagn. Interv. Imaging 2013, 94, 925–943. [Google Scholar] [CrossRef] [Green Version]
- Franzblau, L.E.; Shauver, M.J.; Chung, K.C. Patient satisfaction and self-reported outcomes after complete brachial plexus avulsion injury. J. Hand Surg. 2004, 39.5, 948–955. [Google Scholar] [CrossRef]
- Ochi, M.; Ikuta, Y.; Watanabe, M.; Kimori, K.; Itoh, K. The diagnostic value of MRI in traumatic brachial plexus injury. J. Hand Surg. 1994, 19, 55–59. [Google Scholar] [CrossRef]
- Bischoff, C.; Kollmer, J.; Schulte-Mattler, W. State-of-the-Art Diagnosis of Peripheral Nerve Trauma: Clinical Examination, Electrodiagnostic, and Imaging. In Modern Concepts of Peripheral Nerve Repair; Springer: Cham, Germany, 2017; pp. 11–25. [Google Scholar]
- Balakrishna, S. A Pictorial essay of MRI findings–obstetric brachial plexopathy. Eur. Congr. Radiol. 2019, 2019. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med Res. Methodol. 2006, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Gad, D.M.; Hussein, M.T.; Omar, N.N.M.; Kotb, M.M.; Abdel-Tawab, M.; Yousef, H.A.Z. Role of MRI in the diagnosis of adult traumatic and obstetric brachial plexus injury compared to intraoperative findings. Egypt. J. Radiol. Nucl. Med. 2020, 51, 1–7. [Google Scholar] [CrossRef]
- Acharya, A.M.; Cherian, B.S.; Bhat, A.K. Diagnostic accuracy of MRI for traumatic adult brachial plexus injury: A comparison study with surgical findings. J. Orthop. 2020, 17, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xiao, T.; Yu, Q.; Li, Y.; Shen, F.; Li, W. Clinical value and diagnostic accuracy of 3.0 T multi-parameter magnetic resonance imaging in traumatic brachial plexus injury. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 7199. [Google Scholar]
- Caporrino, F.A.; Moreira, L.; Moraes, V.Y.; Belloti, J.C.; Gomes dos Santos, J.B.; Faloppa, F. Brachial plexus injuries: Diagnosis performance and reliability of everyday tools. Hand Surg. 2014, 19, 7–11. [Google Scholar] [CrossRef]
- Ahlawat, S.; Belzberg, A.J.; Montgomery, E.A.; Fayad, L.M. MRI features of peripheral traumatic neuromas. Eur. Radiol. 2016, 26, 1204–1212. [Google Scholar] [CrossRef]
- Van Es, H.W.; Bollen, T.L.; van Heesewijk, H.P.M. MRI of the brachial plexus: A pictorial review. Eur. J. Radiol. 2010, 74, 391–402. [Google Scholar] [CrossRef]
- Mazal, A.T.; Faramarzalian, A.; Samet, J.D.; Gill, K.; Cheng, J.; Chhabra, A. MR neurography of the brachial plexus in adult and pediatric age groups: Evolution, recent advances, and future directions. Expert Rev. Med. Devices 2020, 17, 111–122. [Google Scholar] [CrossRef]
- Upadhyaya, V.; Upadhyaya, D.N.; Kumar, A.; Gujral, R.B. MR neurography in traumatic brachial plexopathy. Eur. J. Radiol. 2015, 84, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Stilwill, S.E.; Mills, M.K.; Hansford, B.G.; Allen, H.; Mahan, M.; Moore, K.R.; Hanrahan, C.J. Practical Approach and Review of Brachial Plexus Pathology With Operative Correlation: What the Radiologist Needs to Know. Semin. Roentgenol. 2019, 54, 92–112. [Google Scholar] [CrossRef]
- Fuzari, H.K.; de Andrade, A.D.; Vilar, C.F.; Sayão, L.B.; Diniz, P.R.; Souza, F.H.; de Oliveira, D.A. Diagnostic accuracy of magnetic resonance imaging in post-traumatic brachial plexus injuries: A systematic review. Clin. Neurol. Neurosurg. 2018, 164, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Tagliafico, A.; Succio, G.; Serafini, G.; Martinoli, C. Diagnostic accuracy of MRI in adults with suspect brachial plexus lesions: A multicentre retrospective study with surgical findings and clinical follow-up as reference standard. Eur. J. Radiol. 2012, 81, 2666–2672. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.G.; Yang, J.T.; Yang, Y.; Wang, H.G.; Fu, G.; Gu, L.Q.; Li, P.; Zhu, Q.Y.; Liu, X.L.; Zhu, J.K. Diagnostic value and surgical implications of the 3D DW-SSFP MRI on the management of patients with brachial plexus injuries. Sci. Rep. 2016, 6, 35999. [Google Scholar] [CrossRef] [PubMed]
- Kwee, R.M.; Chhabra, A.; Wang, K.C.; Marker, D.R.; Carrino, J.A. Accuracy of MRI in diagnosing peripheral nerve disease: A systematic review of the literature. Am. J. Roentgenol. 2014, 203, 1303–1309. [Google Scholar] [CrossRef]
- Noguerol, T.M.; Barousse, R.; Socolovsky, M.; Luna, A. Quantitative magnetic resonance (MR) neurography for evaluation of peripheral nerves and plexus injuries. Quant. Imaging Med. Surg. 2017, 7, 398. [Google Scholar] [CrossRef] [Green Version]
- Mathes, T.; Oliver, K. A comparison of methods for meta-analysis of a small number of studies with binary outcomes. Res. Synth. Methods 2018, 9, 366–381. [Google Scholar] [CrossRef]
- Lee, Y.H. An overview of meta-analysis for clinicians. Korean J. Intern. Med. 2018, 33, 277. [Google Scholar] [CrossRef] [Green Version]
- Vargas, M.I. Three-dimensional MR imaging of the brachial plexus. In Seminars in Musculoskeletal Radiology; Thieme Medical Publishers: New York, NY, USA, 2015; Volume 19. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Study Design | Subject Features | Postganglionic Lesions | Age | MRI Field Intensity | MRI Sequences Employed | MRI Timing | Standard of Reference | Level of Evidence | Main Conclusion | |
|---|---|---|---|---|---|---|---|---|---|---|
| Acharya, 2019 [16] | Prospective | 35 patients with traumatic brachial plexus injuries | Eight surgically demonstrated postganglionic lesions | Patients under the age of 60 | 1.5 T | T1-T2-T2 weighted 3D neurography-T2 spin echo- short-tau inversion recovery (STIR) | At least 3 weeks after injury | Surgery | 2b | Magnetic resonance imaging (MRI) is a useful tool in the diagnosis of brachial plexus injuries. |
| Zhang, 2018 [17] | Prospective | 28 patients with traumatic brachial plexus injuries | 23 surgically demonstrated postganglionic lesions, in 12 patients | Mean age: 27.2 | 3 T | T1-T2-STIR- balance FFE- diffusion-weighted imaging with background signal suppression (DWIBS) | Not reported | Surgery | 2b | MRI is a valuable diagnostic tool for brachial plexus lesions, especially if balance-FFE, STIR, and DWIBS sequences are performed. |
| Caporrino, 2014 [18] | Prospective | 34 patients with traumatic plexus injuries | Not reported | Mean age: 29.8 | 1.5 T | Not reported | 2–3 months after injury | Surgery | 2b | MRI showed poor diagnostic performance in identifying brachial plexus lesions compared to physical examination. Notwithstanding, it is reasonable to think that the combination of physical examination and MRI could provide the best diagnostic accuracy. |
| Gad, 2020 [15] | Prospective | 22 patients with traumatic brachial plexus injuries | 18 surgically demonstrated postganglionic lesions | Mean age: 26.3 | 1.5 T | T1, STIR, T2, T2-STIR, and DWIBS | Not reported | Surgery | 2b | “MRI is the imaging modality of choice in the examination of traumatic and obstetric brachial plexus injuries; it is safe and non-invasive, having the multiplanar capability and better soft tissue characterization”. |
| Patient Selection | Index Test | Reference Standard | Flow and Timing | |
|---|---|---|---|---|
| Acharya, 2019 [16] | + | + | + | + |
| Zhang, 2018 [17] | ? | + | ? | ? |
| Caporrino, 2014 [18] | + | ? | + | ? |
| Gad, 2020 [15] | + | + | + | ? |
| Study | TP | FP | FN | TN | Sensitivity (95% CI) | Specificity (95% CI) | Forrest Plots |
|---|---|---|---|---|---|---|---|
| Gad 2020 [15] | 16 | 0 | 2 | 198 | 0.89 (0.65–0.99) | 1.00 (0.98–1.00) |   |
| Acharya 2019 [16] | 7 | 20 | 1 | 7 | 0.88 (0.47–1.00) | 0.26 (0.11–0.46) | |
| Zhang 2018 [17] | 21 | 2 | 2 | 3 | 0.91 (0.72–0.99) | 0.60 (0.15–0.95) |
| TP | FP | FN | TN | Pooled Sensitivity | Pooled Specificity | Pooled LR+ | Pooled LR− | Pooled DOR | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Value (95% CI) | I2 | Value (95% CI) | I2 | Value (95% CI) | I2 | Value (95% CI) | I2 | Value (95%CI) | I2 | ||||
| 44 | 22 | 5 | 208 | 0.90 (0.78–0.97) | 0.0% | 0.90 (0.86–0.94) | 98.1% | 7.70 (0.28–214.76) | 96.5% | 0.17 (0.07–0.39) | 0.0% | 40.71 (0.99–1666.3) | 84.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leigheb, M.; Tricca, S.; Percivale, I.; Licandro, D.; Paladini, A.; Barini, M.; Guzzardi, G.; Grassi, F.A.; Stecco, A.; Carriero, A. Diagnostic Accuracy of the Magnetic Resonance Imaging in Adult Post-Ganglionic Brachial Plexus Traumatic Injuries: A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 173. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020173
Leigheb M, Tricca S, Percivale I, Licandro D, Paladini A, Barini M, Guzzardi G, Grassi FA, Stecco A, Carriero A. Diagnostic Accuracy of the Magnetic Resonance Imaging in Adult Post-Ganglionic Brachial Plexus Traumatic Injuries: A Systematic Review and Meta-Analysis. Brain Sciences. 2021; 11(2):173. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020173
Chicago/Turabian StyleLeigheb, Massimiliano, Stefano Tricca, Ilaria Percivale, Davide Licandro, Andrea Paladini, Michela Barini, Giuseppe Guzzardi, Federico A. Grassi, Alessandro Stecco, and Alessandro Carriero. 2021. "Diagnostic Accuracy of the Magnetic Resonance Imaging in Adult Post-Ganglionic Brachial Plexus Traumatic Injuries: A Systematic Review and Meta-Analysis" Brain Sciences 11, no. 2: 173. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020173