
The Carotid Endarterectomy Cadaveric Investigation for Cranial Nerve Injuries: Anatomical Study

 , ,
, ,
Abstract
:1. Introduction
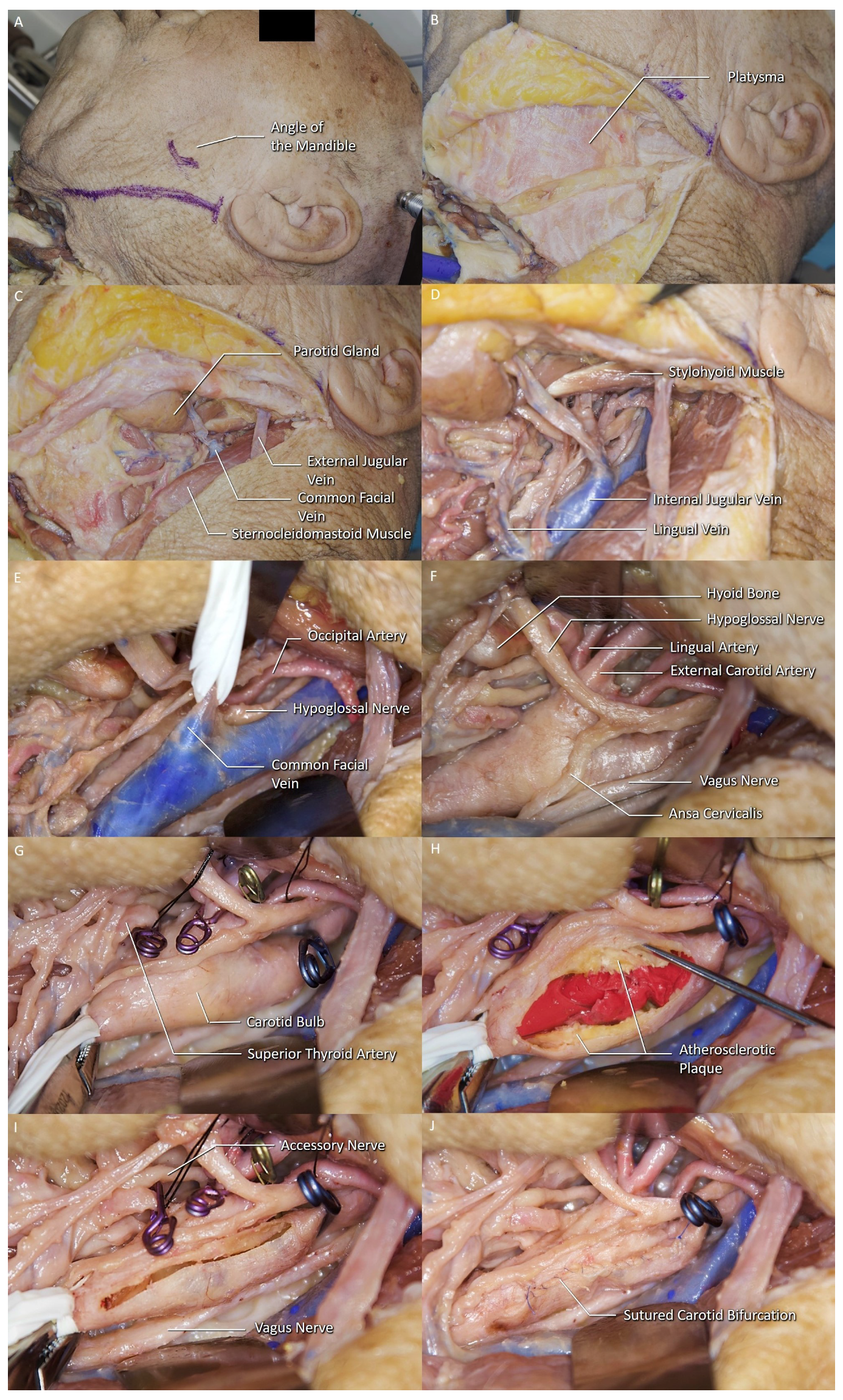
2. Materials and Methods
3. Results
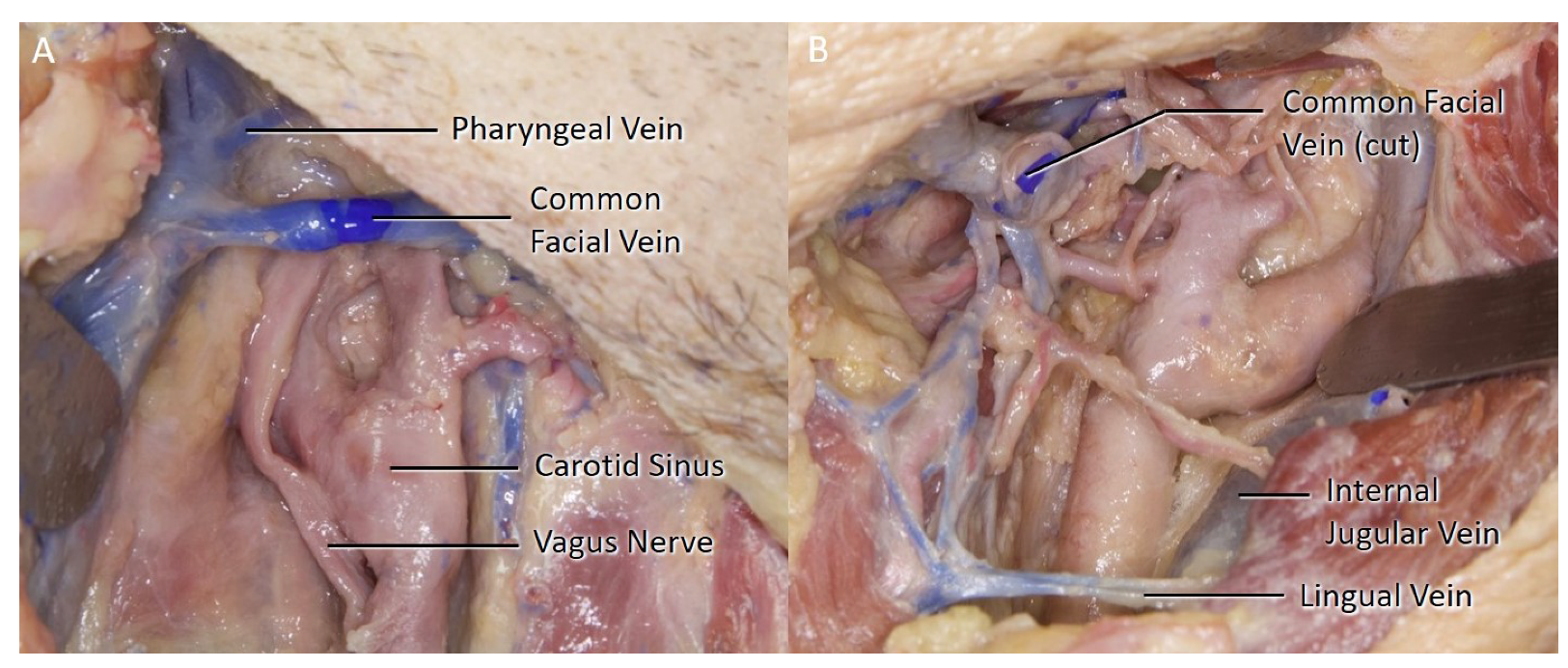
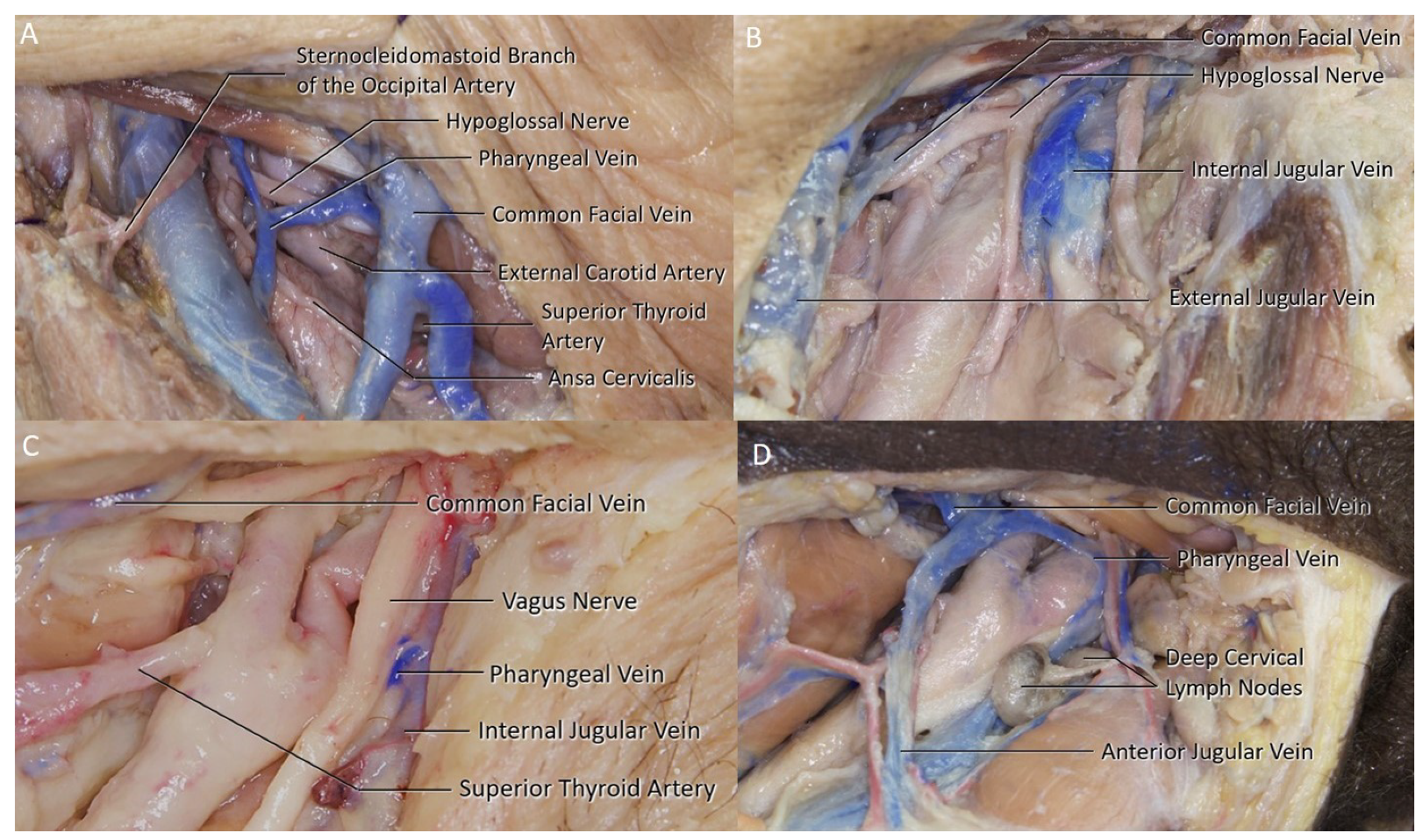
3.1. Common Facial Vein
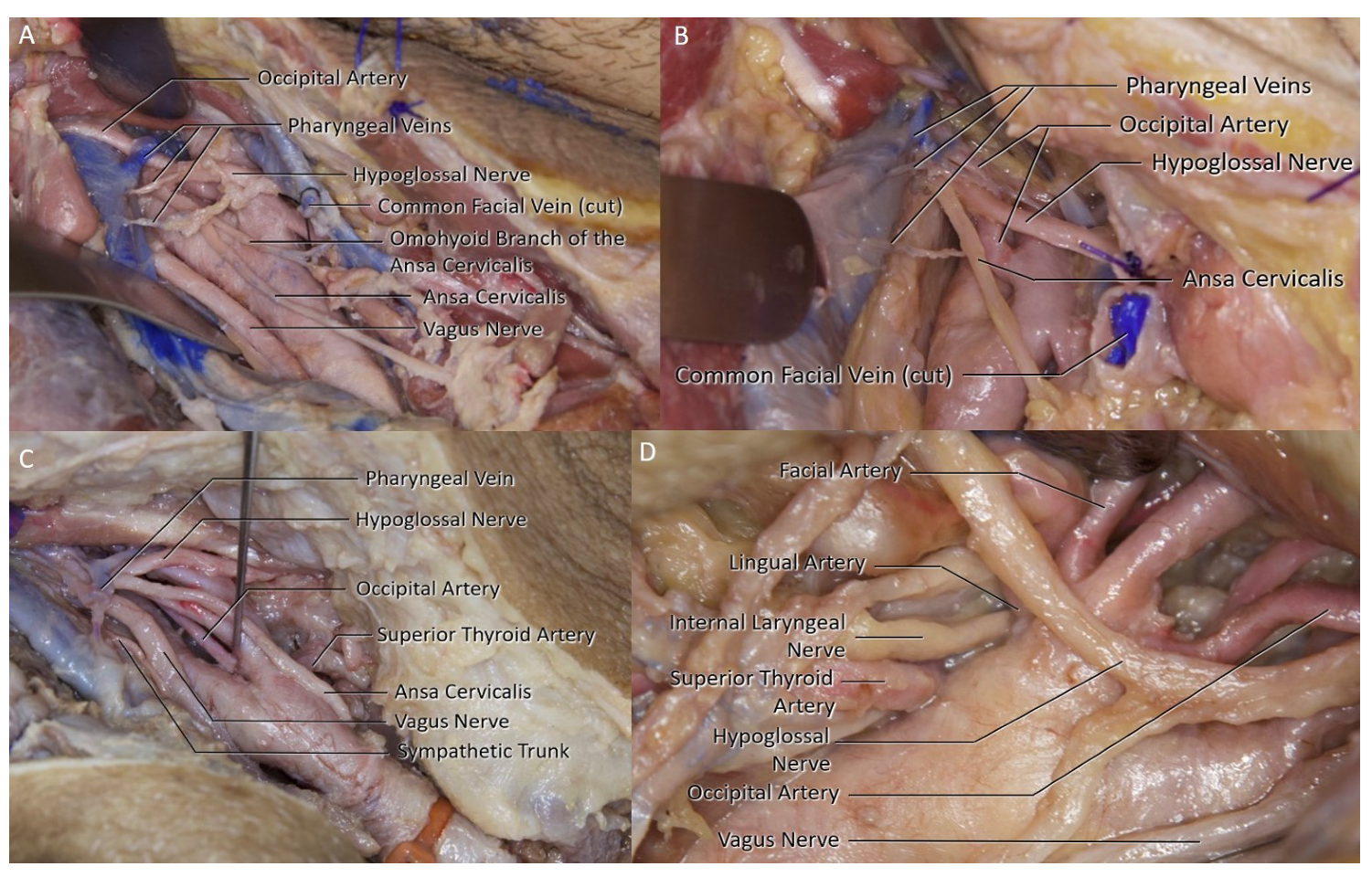
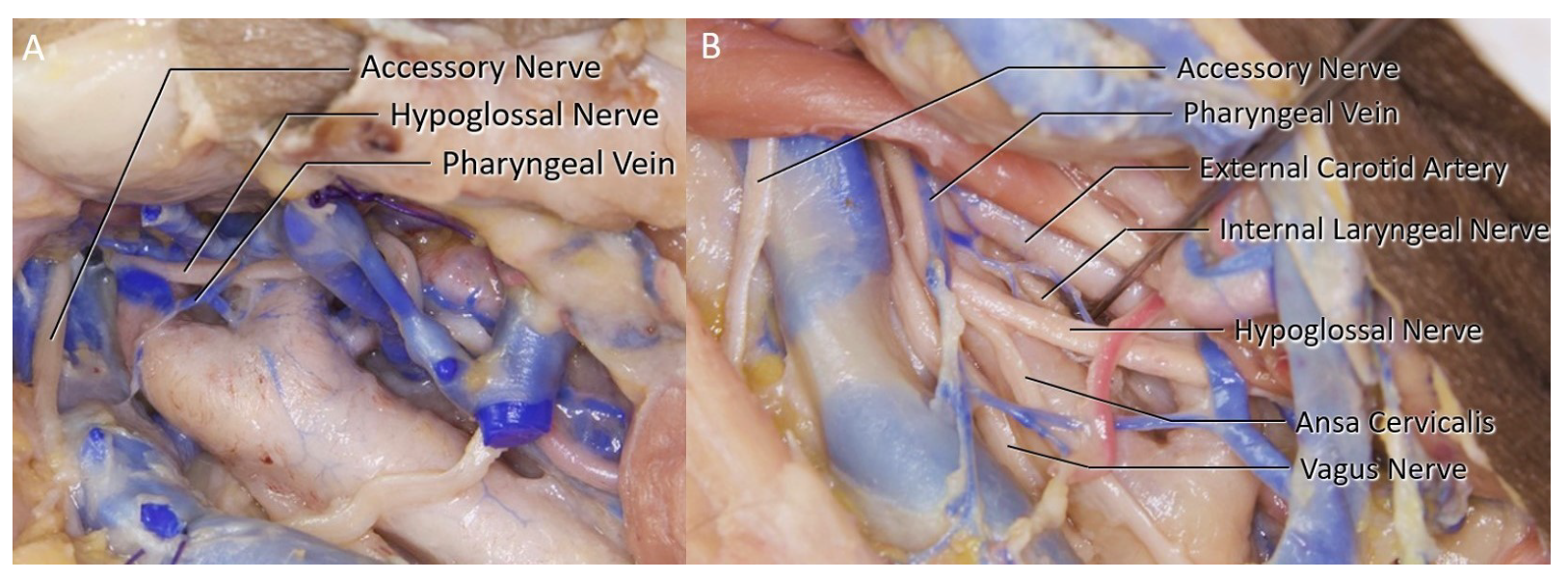
3.2. Pharyngeal Vein
3.3. Lingual Vein
3.4. Arterial Branches
3.5. Carotid Bifurcation
3.6. Hypoglossal Nerve
3.7. Side Variation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CEA | Carotid Endarterectomy |
| HN | Hypoglossal Nerve |
| CASE | Center for Advanced Simulation and Education |
| SCM | Sternocleidomastoid Muscle |
| IJV | Internal Jugular Vein |
| CCA | Common Carotid Artery |
| ICA | Internal Carotid Artery |
| ECA | External Carotid Artery |
| STA | Superior Thyroid Artery |
References
- Bonita, R. Epidemiology of stroke. Lancet 1992, 339, 342–344. [Google Scholar] [CrossRef]
- Rothwell, P.; Slattery, J.; Warlow, C. A systematic review of the risks of stroke and death due to endarterectomy for symptomatic carotid stenosis. Stroke 1996, 27, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajid, M.; Vijaynagar, B.; Singh, P.; Hamilton, G. Literature review of cranial nerve injuries during carotid endarterectomy. Acta Chir. Belg. 2007, 107, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Kakisis, J.; Antonopoulos, C.; Mantas, G.; Moulakakis, K.; Sfyroeras, G.; Geroulakos, G. Cranial nerve injury after carotid endarterectomy: Incidence, risk factors, and time trends. Eur. J. Vasc. Endovasc. Surg. 2017, 53, 320–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loukas, M.; Thorsell, A.; Tubbs, R.; Kapos, T.; Louis, R., Jr.; Vulis, M.; Hage, R.; Jordan, R. The ansa cervicalis revisited. Folia Morphol. 2007, 66, 120–125. [Google Scholar]
- Kikuta, S.; Jenkins, S.; Kusukawa, J.; Iwanaga, J.; Loukas, M.; Tubbs, R.S. Ansa cervicalis: A comprehensive review of its anatomy, variations, pathology, and surgical applications. Anat. Cell Biol. 2019, 52, 221. [Google Scholar] [CrossRef] [PubMed]
- Aldoori, J.; Mahadevan, V.; Aldoori, M. The significance of the pharyngeal veins during carotid endarterectomy: Description of an anatomical triangle. Ann. R. Coll. Surg. Engl. 2018, 100, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Hertzer, N.; Feldman, B.; Beven, E.; Tucker, H. A prospective study of the incidence of injury to the cranial nerves during carotid endarterectomy. Surg. Gynecol. Obstet. 1980, 151, 781–784. [Google Scholar] [PubMed]
- Hertzer, N.R. Postoperative Management and Complications of Extra Cranial Carotid Reconstruction. In Vascular Surgery, 2nd ed.; WB Saunders Co.: Philadelphia, PA, USA, 2018. [Google Scholar]
- Fernando, D.; Lord, R.; Ozmen, J. The blood supply of the hypoglossal nerve and its relevance to carotid endarterectomy. Cardiovasc. Surg. 1999, 7, 287–291. [Google Scholar] [CrossRef]
- Charlesworth, D.; Greenhalgh, R. Vascular Surgical Techniques, “Carotid Endarterectomy”; Butterworths: London, UK, 1984. [Google Scholar]
- Deepak, C.A.; Sarvadnya, J.J.; Sabitha, K. Variant anatomy of internal jugular vein branching. Ann. Maxillofac. Surg. 2015, 5, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çırak, M.; Bozkurt, B.; Yağmurlu, K. Vagus Nerve Injury During Carotid Endarterectomy: A Cadaveric Study. Med. J. Bakirkoy 2020, 16, 33–39. [Google Scholar] [CrossRef]
- Assadian, A.; Senekowitsch, C.; Pfaffelmeyer, N.; Assadian, O.; Ptakovsky, H.; Hagmüller, G. Incidence of cranial nerve injuries after carotid eversion endarterectomy with a transverse skin incision under regional anaesthesia. Eur. J. Vasc. Endovasc. Surg. 2004, 28, 421–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schummer, W.; Schummer, C.; Fröber, R. Persistent left superior vena cava and central venous catheter position: Clinical impact illustrated by four cases. Surg. Radiol. Anat. 2003, 25, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, Z.; Govsa, F.; Celik, S.; Ozgur, T. Clinically relevant variations of the superior thyroid artery: An anatomic guide for surgical neck dissection. Surg. Radiol. Anat. 2009, 31, 151. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.; Oehley, M.; Bartlett, A.; Adams, D.; Blyth, P.; Al-Ali, S. Anatomical variations of the common carotid artery bifurcation. ANZ J. Surg. 2006, 76, 970–972. [Google Scholar] [CrossRef] [PubMed]
- Steele, R.J. Gray’s Anatomy. The Anatomical Basis of Clinical Practice; Standring, S., Ed.; Churchill Livingstone Elsevier: London, UK, 2008; ISBN 978 0 8089 2371 8. [Google Scholar]
- Klosek, S.K.; Rungruang, T. Topography of carotid bifurcation: Considerations for neck examination. Surg. Radiol. Anat. 2008, 30, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Anangwe, D.; Saidi, H.; Ogeng’o, J.; Awori, K. Anatomical variations of the carotid arteries in adult Kenyans. East Afr. Med. J. 2008, 85, 244–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Attribute | Right | Left | Total |
|---|---|---|---|
| Total Specimens Available | 22 | 22 | 44 |
| No IJV Branch | 2 | 2 | 4 |
| Facial Vein | 20 | 18 | 38 |
| Pharyngeal Vein | 15 | 7 | 22 |
| Lingual Vein | 1 | 3 | 4 |
| Single Facial Vein | 4 | 12 | 16 |
| Single Pharyngeal Vein | 0 | 2 | 2 |
| Pharyngeal + Facial Veins | 15 | 3 | 18 |
| Facial + Lingual Veins | 1 | 1 | 2 |
| All 3 Branches | 0 | 2 | 2 |
| Multiple Pharyngeal Veins | 2 | 0 | 2 |
| Total Sides | Right | Left | p Value | |
|---|---|---|---|---|
| Phayngeal Vein over the Bifurcation | 12 (27.3%) | 9 | 3 | 0.0833 |
| PV and HN Intersection | 18 (40.9%) | 13 | 5 | 0.0593 |
| Both Variations Present | 10 (22.8%) | 9 | 1 | 0.0114 |
| Bifurcation Level | Number of Sides | HN in Close Proximity | Rate |
|---|---|---|---|
| C2 | 8 | 4 | 50% |
| C3 | 28 | 12 | 42.9% |
| C4 | 8 | 0 | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cevik, O.M.; Usseli, M.I.; Babur, M.; Unal, C.; Eksi, M.S.; Guduk, M.; Ovalioglu, T.C.; Aksoy, M.E.; Pamir, M.N.; Bozkurt, B. The Carotid Endarterectomy Cadaveric Investigation for Cranial Nerve Injuries: Anatomical Study. Brain Sci. 2021, 11, 211. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020211
Cevik OM, Usseli MI, Babur M, Unal C, Eksi MS, Guduk M, Ovalioglu TC, Aksoy ME, Pamir MN, Bozkurt B. The Carotid Endarterectomy Cadaveric Investigation for Cranial Nerve Injuries: Anatomical Study. Brain Sciences. 2021; 11(2):211. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020211
Chicago/Turabian StyleCevik, Orhun Mete, Murat Imre Usseli, Mert Babur, Cansu Unal, Murat Sakir Eksi, Mustafa Guduk, Talat Cem Ovalioglu, Mehmet Emin Aksoy, M. Necmettin Pamir, and Baran Bozkurt. 2021. "The Carotid Endarterectomy Cadaveric Investigation for Cranial Nerve Injuries: Anatomical Study" Brain Sciences 11, no. 2: 211. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020211