
Differential Susceptibility to the Impact of the COVID-19 Pandemic on Working Memory, Empathy, and Perceived Stress: The Role of Cortisol and Resilience
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
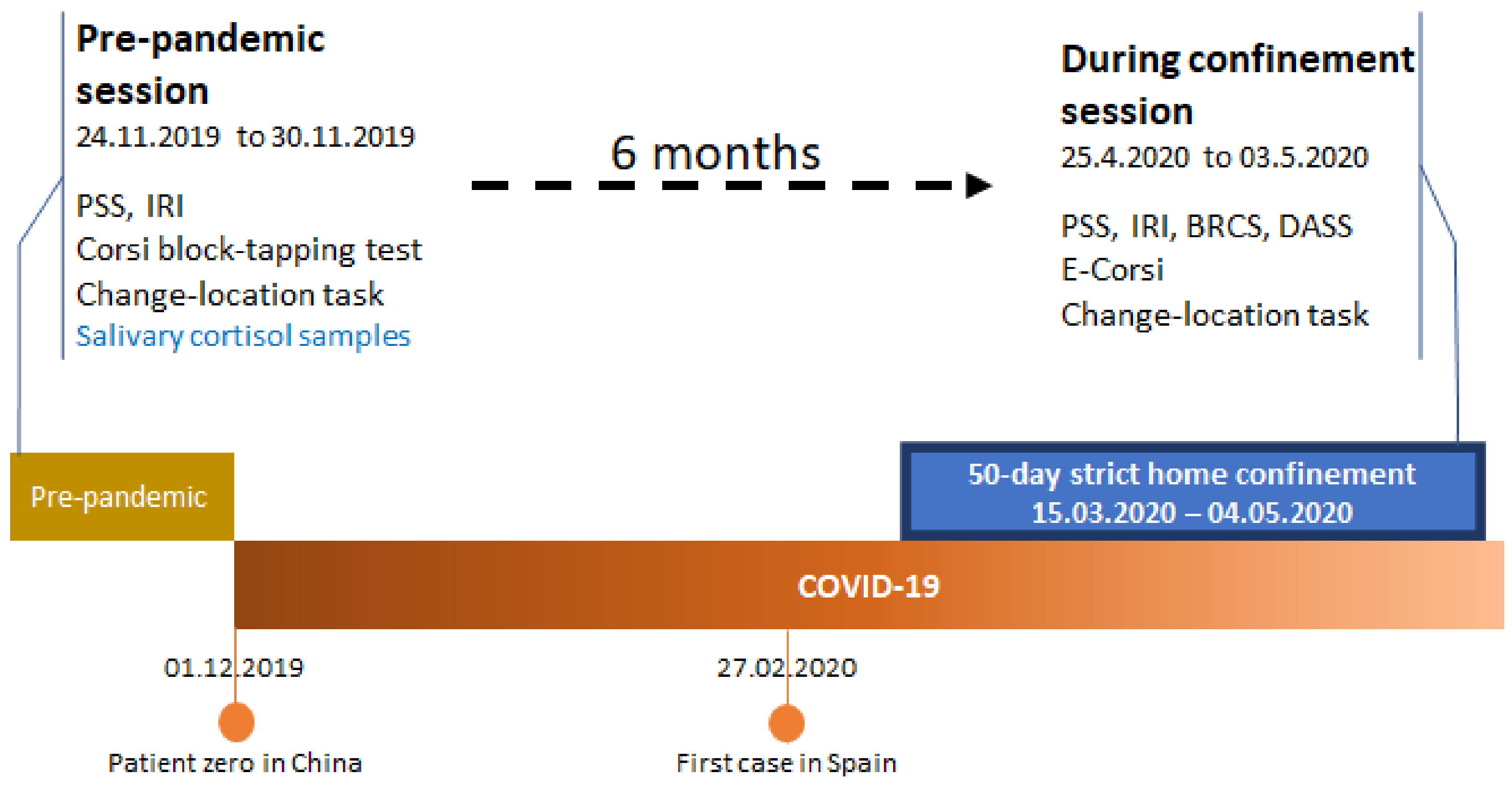
2.2. Procedure and Study Timeline
2.3. Saliva Sample Collection
2.4. Cognitive Tests
2.4.1. Corsi Block-Tapping Test
2.4.2. Change-Location Task
2.4.3. Electronic Corsi Block-Tapping Test (e-Corsi)
2.5. Questionnaire Measures
2.5.1. Perceived Stress Scale (PSS)
2.5.2. Interpersonal Reactivity Index (IRI)
2.5.3. Brief Resilient Coping Scale (BRCS)
2.5.4. Depression Anxiety and Stress Scales (DASS)
2.6. Data Management and Statistical Analyses
3. Results
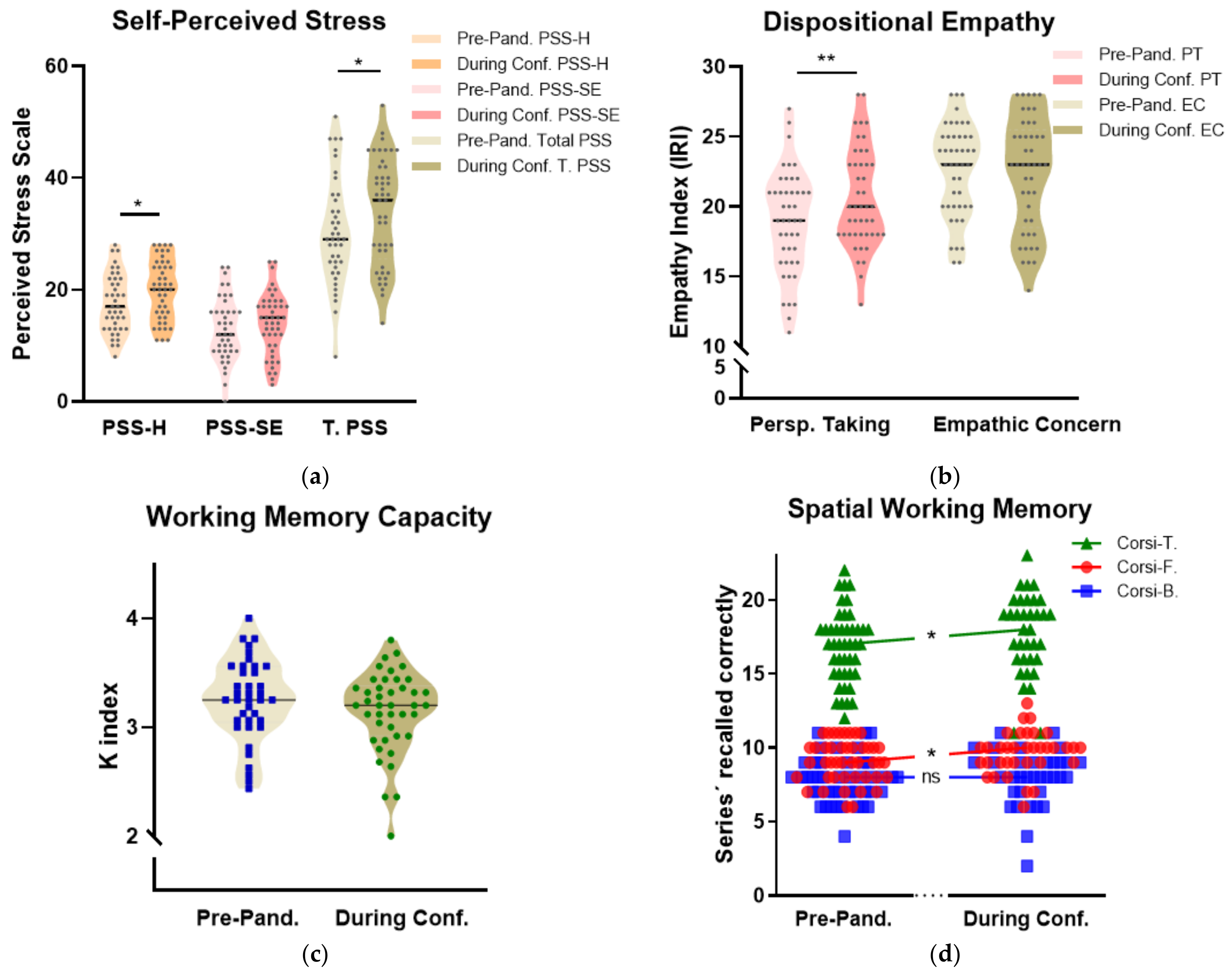
3.1. Changes Across Pre-Pandemic and During-Confinement Scores
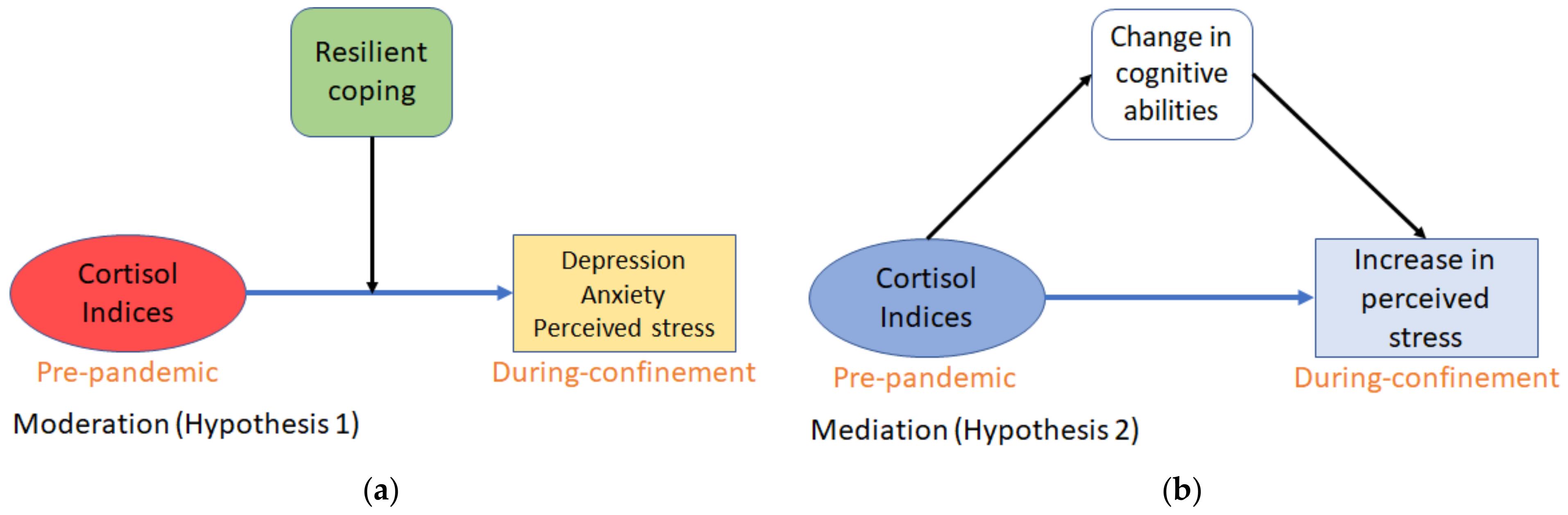
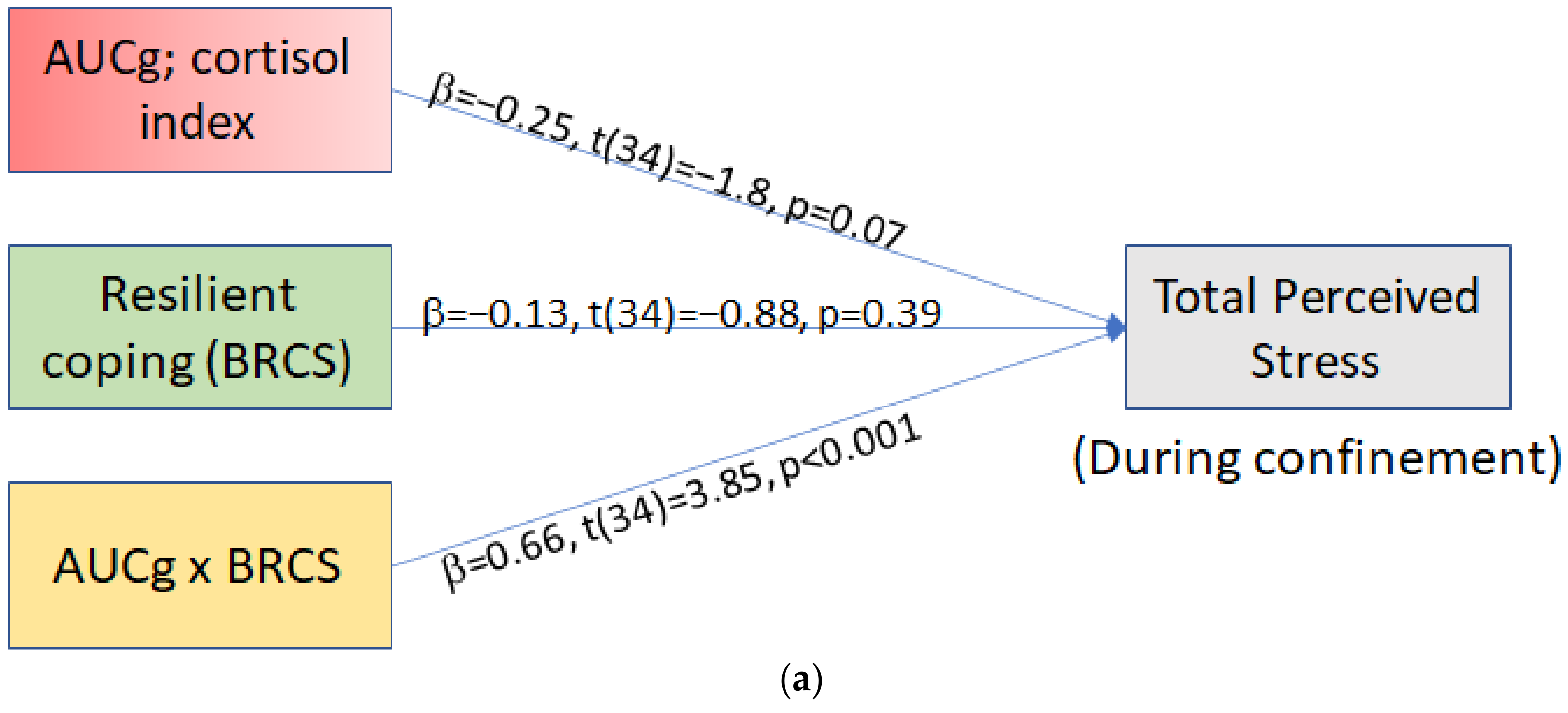
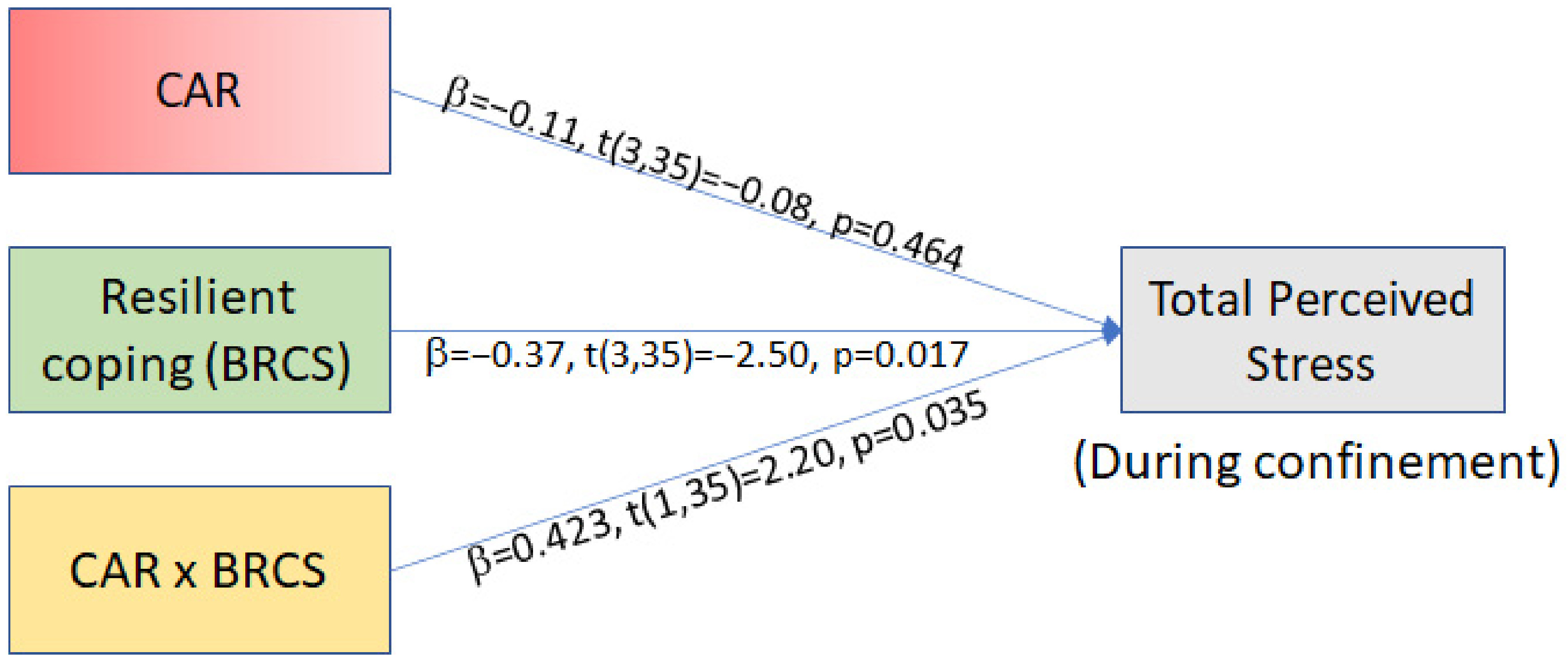
3.2. Moderation Analyses
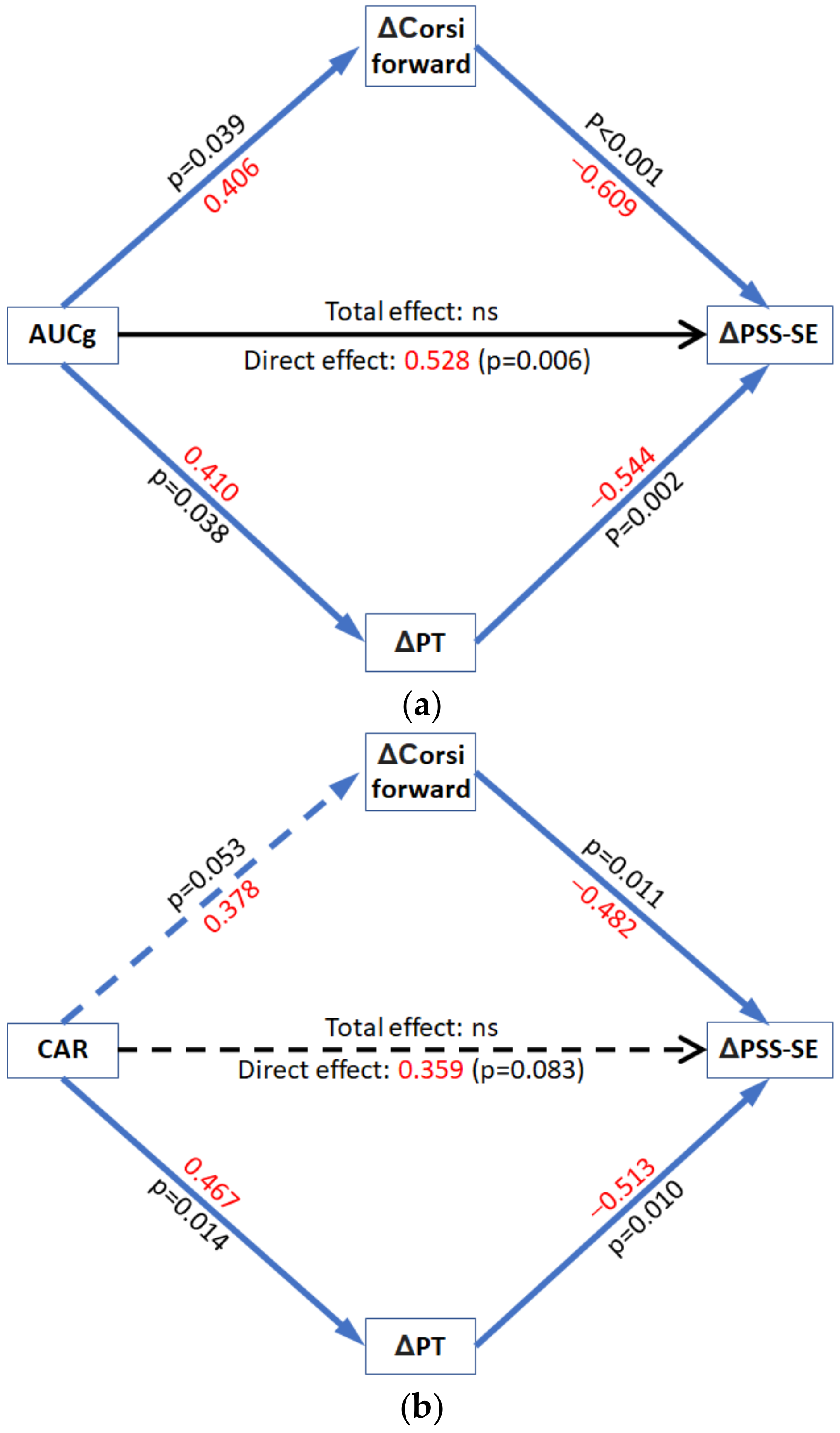
3.3. Mediation Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newby, J.M.; O’Moore, K.; Tang, S.; Christensen, H.; Faasse, K. Acute mental health responses during the COVID-19 pandemic in Australia. PLoS ONE 2020, 15, 1–21. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; Kontopantelis, E.; John, A.; Webb, R.T.; Wessely, S.; McManus, S.; et al. Mental Health Before and During the COVID-19 Pandemic: A Longitudinal Probability Sample Survey of the UK Population. SSRN Electron. J. 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Sandi, C. Stress, cognitive impairment and cell adhesion molecules. Nat. Rev. Neurosci. 2004, 5, 917–930. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; Juster, R.; Raymond, C.; Marin, M. The effects of chronic stress on the human brain: From neurotoxicity, to vulnerability, to opportunity. Front. Neuroendocrinol. 2018, 49, 91–105. [Google Scholar] [CrossRef]
- Belleau, E.L.; Treadway, M.T.; Pizzagalli, D.A. The Impact of Stress and Major Depressive Disorder on Hippocampal and Medial Prefrontal Cortex Morphology. Biol. Psychiatry 2019, 85, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Von Dawans, B.; Ditzen, B.; Trueg, A.; Fischbacher, U.; Heinrichs, M. Effects of acute stress on social behavior in women. Psychoneuroendocrinology 2019, 99, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Tomova, L.; Majdandžić, J.; Hummer, A.; Windischberger, C.; Heinrichs, M.; Lamm, C. Increased neural responses to empathy for pain might explain how acute stress increases prosociality. Soc. Cogn. Affect. Neurosci. 2017, 12, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Wolf, O.T.; Schulte, J.M.; Drimalla, H.; Hamacher-Dang, T.C.; Knoch, D.; Dziobek, I. Enhanced emotional empathy after psychosocial stress in young healthy men. Stress 2015, 18, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Starcke, K.; Brand, M. Decision making under stress: A selective review. Neurosci. Biobehav. Rev. 2012, 36, 1228–1248. [Google Scholar] [CrossRef] [PubMed]
- Luethi, M.; Meier, B.; Sandi, C. Stress effects on working memory, explicit memory, and implicit memory for neutral and emotional stimuli in healthy men. Front. Behav. Neurosci. 2009, 2, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, S.; Hermans, E.J.; van Marle, H.J.F.; Luo, J.; Fernández, G. Acute Psychological Stress Reduces Working Memory-Related Activity in the Dorsolateral Prefrontal Cortex. Biol. Psychiatry 2009, 66, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.E.; Diessler, S.; Varea, E.; Márquez, C.; Larsen, M.H.; Cordero, M.I.; Sandi, C. Personality traits in rats predict vulnerability and resilience to developing stress-induced depression-like behaviors, HPA axis hyper-reactivity and brain changes in pERK1/2 activity. Psychoneuroendocrinology 2012, 37, 1209–1223. [Google Scholar] [CrossRef]
- Larrieu, T.; Cherix, A.; Duque, A.; Rodrigues, J.; Lei, H.; Gruetter, R.; Sandi, C. Hierarchical Status Predicts Behavioral Vulnerability and Nucleus Accumbens Metabolic Profile Following Chronic Social Defeat Stress. Curr. Biol. 2017, 27, 2202–2210. [Google Scholar] [CrossRef] [Green Version]
- Weger, M.; Sandi, C. High anxiety trait: A vulnerable phenotype for stress-induced depression. Neurosci. Biobehav. Rev. 2018, 87, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.E.; Zanoletti, O.; Guillot de Suduiraut, I.; Sandi, C. Constitutive differences in glucocorticoid responsiveness to stress are related to variation in aggression and anxiety-related behaviors. Psychoneuroendocrinology 2017, 84, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Papilloud, A.; Veenit, V.; Tzanoulinou, S.; Riccio, O.; Zanoletti, O.; Guillot de Suduiraut, I.; Grosse, J.; Sandi, C. Peripubertal stress-induced heightened aggression: Modulation of the glucocorticoid receptor in the central amygdala and normalization by mifepristone treatment. Neuropsychopharmacology 2019, 44, 674–682. [Google Scholar] [CrossRef] [Green Version]
- Huzard, D.; Mumby, D.G.; Sandi, C.; Poirier, G.L.; van der Kooij, M.A. The effects of extrinsic stress on somatic markers and behavior are dependent on animal housing conditions. Physiol. Behav. 2015, 151, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Tzanoulinou, S.; Gantelet, E.; Sandi, C.; Márquez, C. Programming effects of peripubertal stress on spatial learning. Neurobiol. Stress 2020, 13, 100282. [Google Scholar] [CrossRef] [PubMed]
- Adam, E.K.; Kumari, M. Assessing salivary cortisol in large-scale, epidemiological research. Psychoneuroendocrinology 2009, 34, 1423–1436. [Google Scholar] [CrossRef]
- Buchanan, T.W.; Tranel, D.; Adolphs, R. Impaired memory retrieval correlates with individual differences in cortisol response but not autonomic response. Learn. Mem. 2006, 382–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, A.A.; Schwartz, J.E.; Smyth, J.; Kirschbaum, C.; Cohen, S.; Hellhammer, D.; Grossman, S. Individual differences in the diurnal cycle of salivary free cortisol: A replication of flattened cycles for some individuals. Psychoneuroendocrinology 2001, 26, 295–306. [Google Scholar] [CrossRef]
- Ulrich-Lai, Y.M.; Herman, J.P. Neural regulation of endocrine and autonomic stress responses. Nat. Rev. Neurosci. 2009, 10, 397–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruessner, J.C.; Wolf, O.T.; Hellhammer, D.H.; Buske-Kirschbaum, A.; Von Auer, K.; Jobst, S.; Kaspers, F.; Kirschbaum, C. Free cortisol levels after awakening: A reliable biological marker for the assessment of adrenocortical activity. Life Sci. 1997, 61, 2539–2549. [Google Scholar] [CrossRef]
- Wust, S.; Federenko, I.; Hellhammer, D.H.; Kirschbaum, C. Genetic factors, perceived chronic stress, and the free cortisol response to awakening. Psychoneuroendocrinology 2000, 25, 707–720. [Google Scholar] [CrossRef]
- Golden, S.H.; Sánchez, B.N.; Wu, M.; Champaneri, S.; Diez Roux, A.V.; Seeman, T.; Wand, G.S. Relationship between the cortisol awakening response and other features of the diurnal cortisol rhythm: The Multi-Ethnic Study of Atherosclerosis. Psychoneuroendocrinology 2013, 38, 2720–2728. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Reinwald, A.; Pruessner, J.C.; Hellhammer, D.H.; Federenko, I.; Rohleder, N.; Schürmeyer, T.H.; Kirschbaum, C. The cortisol response to awakening in relation to different challenge tests and a 12-hour cortisol rhythm. Life Sci. 1999, 64, 1653–1660. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Hellhammer, D.H.; Kirschbaum, C. Burnout, perceived stress, and cortisol responses to awakening. Psychosom. Med. 1999, 61, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.; Kirschbaum, C.; Prüßner, J.; Hellhammer, D. Increased free cortisol secretion after awakening in chronically stressed individuals due to work overload. Stress Med. 1998, 14, 91–97. [Google Scholar] [CrossRef]
- Pruessner, M.; Hellhammer, D.H.; Pruessner, J.C.; Lupien, S.J. Self-reported depressive symptoms and stress levels in healthy young men: Associations with the cortisol response to awakening. Psychosom. Med. 2003, 65, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Adam, E.K.; Doane, L.D.; Zinbarg, R.E.; Mineka, S.; Craske, M.G.; Griffith, J.W. Prospective prediction of major depressive disorder from cortisol awakening responses in adolescence. Psychoneuroendocrinology 2010, 35, 921–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrshek-Schallhorn, S.; Doane, L.D.; Mineka, S.; Zinbarg, R.E.; Craske, M.G.; Adam, E.K. The cortisol awakening response predicts major depression: Predictive stability over a 4-year follow-up and effect of depression history. Psychol. Med. 2013, 43, 483–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stalder, T.; Evans, P.; Hucklebridge, F.; Clow, A. Associations between the cortisol awakening response and heart rate variability. Psychoneuroendocrinology 2011, 36, 454–462. [Google Scholar] [CrossRef]
- Perna, G.; Riva, A.; Defillo, A.; Sangiorgio, E.; Nobile, M.; Caldirola, D. Heart rate variability: Can it serve as a marker of mental health resilience? J. Affect. Disord. 2020, 263, 754–761. [Google Scholar] [CrossRef] [PubMed]
- LeMoult, J.; Ordaz, S.J.; Kircanski, K.; Singh, M.K.; Gotlib, I.H. Predicting first onset of depression in young girls: Interaction of diurnal cortisol and negative life events. J. Abnorm. Psychol. 2015, 124, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Sephton, S.E.; Sapolsky, R.M.; Kraemer, H.C.; Spiegel, D. Diurnal cortisol rhythm as a predictor of breast cancer survival. J. Natl. Cancer Inst. 2000, 92, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Sephton, S.E.; Lush, E.; Dedert, E.A.; Floyd, A.R.; Rebholz, W.N.; Dhabhar, F.S.; Spiegel, D.; Salmon, P. Diurnal cortisol rhythm as a predictor of lung cancer survival. Brain. Behav. Immun. 2013, 30, S163–S170. [Google Scholar] [CrossRef] [PubMed]
- Pineles, S.L.; Rasmusson, A.M.; Yehuda, R.; Lasko, N.B.; Macklin, M.L.; Pitman, R.K.; Orr, S.P. Predicting emotional responses to potentially traumatic events from pre-exposure waking cortisol levels: A longitudinal study of police and firefighters. Anxiety Stress Coping 2013, 26, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Pervanidou, P.; Kolaitis, G.; Charitaki, S.; Margeli, A.; Ferentinos, S.; Bakoula, C.; Lazaropoulou, C.; Papassotiriou, I.; Tsiantis, J.; Chrousos, G.P. Elevated morning serum interleukin (IL)-6 or evening salivary cortisol concentrations predict posttraumatic stress disorder in children and adolescents six months after a motor vehicle accident. Psychoneuroendocrinology 2007, 32, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Smider, N.A.; Essex, M.J.; Kalin, N.H.; Buss, K.A.; Klein, M.H.; Davidson, R.J.; Goldsmith, H.H. Salivary cortisol as a predictor of socioemotional adjustment during kindergarten: A prospective study. Child Dev. 2002, 73, 75–92. [Google Scholar] [CrossRef]
- Munoz, E.; Sliwinski, M.J.; Scott, S.B.; Hofer, S. Global perceived stress predicts cognitive change among older adults. Psychol. Aging 2015, 30, 487–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vignemont, F.; Singer, T. The empathic brain: How, when and why? Trends Cogn. Sci. 2006, 10, 435–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamay-Tsoory, S.G.; Aharon-Peretz, J.; Perry, D. Two systems for empathy: A double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 2009, 132, 617–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, Z.; Hong, S.; Liu, F.; Su, Y. A meta-analysis of the relationship between empathy and executive function. PsyCh J. 2020, 9, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Allott, K.A.; Rapado-Castro, M.; Proffitt, T.M.; Bendall, S.; Garner, B.; Butselaar, F.; Markulev, C.; Phassouliotis, C.; McGorry, P.D.; Wood, S.J.; et al. The impact of neuropsychological functioning and coping style on perceived stress in individuals with first-episode psychosis and healthy controls. Psychiatry Res. 2015, 226, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Riglin, L.; Collishaw, S.; Shelton, K.H.; McManus, I.C.; Ng-Knight, T.; Sellers, R.; Thapar, A.K.; Frederickson, N.; Rice, F. Higher cognitive ability buffers stress-related depressive symptoms in adolescent girls. Dev. Psychopathol. 2015, 28, 97–109. [Google Scholar] [CrossRef] [PubMed]
- D’Zurilla, T.J.; Sheedy, C.F. Relation between Social Problem-Solving Ability and Subsequent Level of Psychological Stress in College Students. J. Pers. Soc. Psychol. 1991, 61, 841–846. [Google Scholar] [CrossRef]
- Cox, C.L.; Uddin, L.Q.; di Martino, A.; Castellanos, F.X.; Milham, M.P.; Kelly, C. The balance between feeling and knowing: Affective and cognitive empathy are reflected in the brain’s intrinsic functional dynamics. Soc. Cogn. Affect. Neurosci. 2012, 7, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Almela, M.; van der Meij, L.; Hidalgo, V.; Villada, C.; Salvador, A. The cortisol awakening response and memory performance in older men and women. Psychoneuroendocrinology 2012, 37, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Evans, P.D.; Fredhoi, C.; Loveday, C.; Hucklebridge, F.; Aitchison, E.; Forte, D.; Clow, A. The diurnal cortisol cycle and cognitive performance in the healthy old. Int. J. Psychophysiol. 2011, 79, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, A.S.; Bradley, A.J.; Anderson, K.N.; Watson, S.; Gallagher, P.; McAllister-Williams, R.H. Cortisol awakening response and spatial working memory in man: A U-shaped relationship. Hum. Psychopharmacol. 2014, 29, 295–298. [Google Scholar] [CrossRef]
- Franz, C.E.; O’Brien, R.C.; Hauger, R.L.; Mendoza, S.P.; Panizzon, M.S.; Prom-Wormley, E.; Eaves, L.J.; Jacobson, K.; Lyons, M.J.; Lupien, S.; et al. Cross-sectional and 35-year longitudinal assessment of salivary cortisol and cognitive functioning: The Vietnam Era Twin Study of Aging. Psychoneuroendocrinology 2011, 36, 1040–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Corsi, P.M. Memory and the Medial Temporal Region of the Brain. Ph.D. Thesis, McGill University, Montreal, QC, Canada, 1972. Unpublished. [Google Scholar]
- Shipstead, Z.; Redick, T.S.; Hicks, K.L.; Engle, R.W. The scope and control of attention as separate aspects of working memory. Memory 2012, 20, 608–628. [Google Scholar] [CrossRef]
- Cowan, N.; Elliott, E.M.; Saults, S.J.; Morey, C.C.; Mattox, S.; Hismjatullina, A.; Conway, A.R.A. On the capacity of attention: Its estimation and its role in working memory and cognitive aptitudes. Cogn. Psychol. 2005, 51, 42–100. [Google Scholar] [CrossRef] [Green Version]
- Remor, E. Psychometric Properties of a European Spanish Version of the Perceived Stress Scale (PSS). J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewitt, P.L.; Flett, G.L.; Mosher, S.W. The Perceived Stress Scale: Factor structure and relation to depression symptoms in a psychiatric sample. J. Psychopathol. Behav. Assess. 1992, 14, 247–257. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy mechanism in human agency. Am. Psychol. 1982, 37, 122–147. [Google Scholar] [CrossRef]
- Pérez-Albéniz, A.; De Paúl, J.; Etxeberría, J.; Montes, M.P.; Torres, E. Adaptación de Interpersonal Reactivity Index (IRI) al español. Psicothema 2003, 15, 267–272. [Google Scholar]
- Limonero, J.T.; Tomás-Sábado, J.; Gómez-Romero, M.J.; Maté-Méndez, J.; Sinclair, V.G.; Wallston, K.A.; Gómez-Benito, J. Evidence for validity of the brief resilient coping scale in a young spanish sample. Span. J. Psychol. 2014, 17, e34. [Google Scholar] [CrossRef]
- Ruiz, F.J.; Martín, M.B.G.; Falcón, J.C.S.; González, P.O. The hierarchical factor structure of the spanish version of depression anxiety and stress scale-21. Int. J. Psychol. Psychol. Ther. 2017, 17, 97–105. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Process Analysis-Appendices A & B (V3); The Guilford Press: New York, NY, USA, 2017; ISBN 9788578110796. [Google Scholar]
- Larsson, C.A.; Gullberg, B.; Råstam, L.; Lindblad, U. Salivary cortisol differs with age and sex and shows inverse associations with WHR in Swedish women: A cross-sectional study. BMC Endocr. Disord. 2009, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, R.; Stalder, T.; Jarczok, M.; Almeida, D.M.; Badrick, E.; Bartels, M.; Boomsma, D.I.; Coe, C.L.; Dekker, M.J.H.J.; Donzella, B.; et al. The CIRCORT database: Reference ranges and seasonal changes in diurnal salivary cortisol derived from a meta-dataset comprised of 15 field studies. Psychoneuroendocrinology 2017, 76, 226–227. [Google Scholar] [CrossRef] [PubMed]
- Andrews, B.; Wilding, J.M. The relation of depression and anxiety to life-stress and achievement in students. Br. J. Psychol. 2004, 95, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Melchior, M.; Caspi, A.; Milne, B.J.; Danese, A.; Poulton, R.; Moffitt, T.E. Work stress precipitates depression and anxiety in young, working women and men. Psychol. Med. 2007, 37, 1119–1129. [Google Scholar] [CrossRef] [Green Version]
- Hammen, C. Stress and depression. Annu. Rev. Clin. Psychol. 2005, 1, 293–319. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.H.; Sarason, I.G. Life stress, depression and anxiety: Internal- external control as a moderator variable. J. Psychosom. Res. 1978, 22, 205–208. [Google Scholar] [CrossRef]
- Beasley, M.; Thompson, T.; Davidson, J. Risilience in response to life stress: The effects of coping style and cognitive hardiness. Pers. Individ. Dif. 2003, 34, 77–95. [Google Scholar] [CrossRef]
- Bitsika, V.; Sharpley, C.F.; Bell, R. The Buffering Effect of Resilience upon Stress, Anxiety and Depression in Parents of a Child with an Autism Spectrum Disorder. J. Dev. Phys. Disabil. 2013, 25, 533–543. [Google Scholar] [CrossRef]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef]
- Vythilingam, M.; Vermetten, E.; Anderson, G.M.; Luckenbaugh, D.; Anderson, E.R.; Snow, J.; Staib, L.H.; Charney, D.S.; Bremner, J.D. Hippocampal volume, memory, and cortisol status in major depressive disorder: Effects of treatment. Biol. Psychiatry 2004, 56, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Olff, M.; de Vries, G.J.; Güzelcan, Y.; Assies, J.; Gersons, B.P.R. Changes in cortisol and DHEA plasma levels after psychotherapy for PTSD. Psychoneuroendocrinology 2007, 32, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Fava, M.; Rosenbaum, J.F.; McCarthy, M.; Pava, J.A.; Steingard, R.; Fox, R. Correlations between perceived stress and depressive symptoms among depressive outpatients. Stress Med. 1992, 8, 73–76. [Google Scholar] [CrossRef]
- Ruiz-Robledillo, N.; De Andrés-García, S.; Pérez-Blasco, J.; González-Bono, E.; Moya-Albiol, L. Highly resilient coping entails better perceived health, high social support and low morning cortisol levels in parents of children with autism spectrum disorder. Res. Dev. Disabil. 2014, 35, 686–695. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Hendrickx, H.; Dadd, T.; Elliman, T.D.; Willis, T.A.; Talbot, D.; Mayes, A.E.; Thethi, K.; Powell, J.; Dye, L. Cortisol awakening rise in middle-aged women in relation to psychological stress. Psychoneuroendocrinology 2009, 34, 1486–1489. [Google Scholar] [CrossRef] [PubMed]
- Carnegie, R.; Araya, R.; Ben-Shlomo, Y.; Glover, V.; O’Connor, T.G.; O’Donnell, K.J.; Pearson, R.; Lewis, G. Cortisol awakening response and subsequent depression: Prospective longitudinal study. Br. J. Psychiatry 2014, 204, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardeveld, F.; Spijker, J.; Vreeburg, S.A.; De Graaf, R.; Hendriks, S.M.; Licht, C.M.M.; Nolen, W.A.; Penninx, B.W.J.H.; Beekman, A.T.F. Increased cortisol awakening response was associated with time to recurrence of major depressive disorder. Psychoneuroendocrinology 2014, 50, 62–71. [Google Scholar] [CrossRef]
- Stroud, C.B.; Vrshek-Shallhorn, S.; Norkett, E.M.; Doane, L.D. The cortisol awakening response (CAR) interacts with acute interpersonal stress to prospectively predict depressive symptoms among early adolescent girls. Psychoneuroendocrinology 2019, 107, 9–18. [Google Scholar] [CrossRef]
- Schuler, K.L.; Ruggero, C.J.; Goldstein, B.L.; Perlman, G.; Klein, D.N.; Kotov, R. Diurnal Cortisol Interacts With Stressful Events to Prospectively Predict Depressive Symptoms in Adolescent Girls. J. Adolesc. Health 2017, 61, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Monroe, S.M.; Simons, A.D. Diathesis-stress theories in the context of life stress research: Implications for the depressive disorders. Psychol. Bull. 1991, 110, 406–425. [Google Scholar] [CrossRef]
- Kudielka, B.M.; Bellingrath, S.; Hellhammer, D.H. Cortisol in burnout and vital exhaustion: An overview. G. Ital. di Med. del Lav. Ed Ergon. 2006, 28, 34–42. [Google Scholar]
- Holsboer, F. The corticosteroid receptor hypothesis of depression. Neuropsychopharmacology 2000, 23, 477–501. [Google Scholar] [CrossRef] [Green Version]
- Schuhmacher, A.; Mössner, R.; Jessen, F.; Scheef, L.; Block, W.; Belloche, A.C.; Lennertz, L.; Welper, H.; Höfels, S.; Pfeiffer, U.; et al. Association of amygdala volumes with cortisol secretion in unipolar depressed patients. Psychiatry Res. Neuroimaging 2012, 202, 96–103. [Google Scholar] [CrossRef]
- Faresjö, Å.; Theodorsson, E.; Chatziarzenis, M.; Sapouna, V.; Claesson, H.P.; Koppner, J.; Faresjö, T. Higher Perceived Stress but Lower Cortisol Levels Found among Young Greek Adults Living in a Stressful Social Environment in Comparison with Swedish Young Adults. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Koh, D.M.M.; Ng, V.; Chun Yue Lee, F.; Gregory Chan, M.; Dong, F.M.M.; Eng Chia, S. Salivary Cortisol Levels and Work-Related Stress Among Emergency Department Nurses. J. Occup. Environ. Med. 2001, 43, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Hjortskov, N.; Rissén, D.; Blangsted, A.K.; Fallentin, N.; Lundberg, U.; Søgaard, K. The effect of mental stress on heart rate variability and blood pressure during computer work. Eur. J. Appl. Physiol. 2004, 92, 84–89. [Google Scholar] [CrossRef]
- Weibel, L.; Gabrion, I.; Aussedat, M.; Kreutz, G. Work-related stress in an emergency medical dispatch center. Ann. Emerg. Med. 2003, 43, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- González-Cabrera, J.; Calvete, E.; León-Mejía, A.; Pérez-Sancho, C.; Peinado, J.M. Relationship between cyberbullying roles, cortisol secretion and psychological stress. Comput. Hum. Behav. 2017, 70, 153–160. [Google Scholar] [CrossRef]
- González-Cabrera, J.; Fernández-Prada, M.; Iribar-Ibabe, C.; Peinado, J.M. Acute and chronic stress increase salivary cortisol: A study in the real-life setting of a national examination undertaken by medical graduates. Stress 2014, 17, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Lara, A.H.; Wallis, J.D. The role of prefrontal cortex in working memory: A mini review. Front. Syst. Neurosci. 2015, 9, 173. [Google Scholar] [CrossRef] [Green Version]
- Herman, J.P.; Ostrander, M.M.; Mueller, N.K.; Figueiredo, H. Limbic system mechanisms of stress regulation: Hypothalamo-pituitary- adrenocortical axis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 1201–1213. [Google Scholar] [CrossRef]
- Balkin, T.J.; Braun, A.R.; Wesensten, N.J.; Jeffries, K.; Varga, M.; Baldwin, P.; Belenky, G.; Herscovitch, P. The process of awakening: A PET study of regional brain activity patterns mediating the re-establishment of alertness and consciousness. Brain 2002, 125, 2308–2319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibb, B.E.; Beevers, C.G.; McGeary, J.E. Toward an integration of cognitive and genetic models of risk for depression. Cogn. Emot. 2013, 27, 193–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masten, A.S.; Hubbard, J.J.; Gest, S.D.; Tellegen, A.; Garmezy, N.; Ramirez, M. Competence in the context of adversity: Pathways to resilience and maladaptation from childhood to late adolescence. Dev. Psychopathol. 1999, 11, 143–169. [Google Scholar] [CrossRef] [Green Version]
- Otto, M.W. Life event, mood, and cognitive predictors of perceived stress before and after treatment for major depression. Cogn. Ther. Res. 1997, 21, 409–420. [Google Scholar] [CrossRef]
- Southwick, S.M.; Vythilingam, M.; Charney, D.S. The psychobiology of depression and resilience to stress: Implications for prevention and treatment. Annu. Rev. Clin. Psychol. 2005, 1, 255–291. [Google Scholar] [CrossRef] [PubMed]
- Gambin, M.; Sharp, C. Relations between empathy and anxiety dimensions in inpatient adolescents. Anxiety Stress Coping 2018, 31, 447–458. [Google Scholar] [CrossRef]
- Loeys, T.; Moerkerke, B.; Vansteelandt, S. A cautionary note on the power of the test for the indirect effect in mediation analysis. Front. Psychol. 2014, 5, 1549. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Schoofs, D.; Preuß, D.; Wolf, O.T. Psychosocial stress induces working memory impairments in an n-back paradigm. Psychoneuroendocrinology 2008, 33, 643–653. [Google Scholar] [CrossRef]
- Salehi, B.; Cordero, M.I.; Sandi, C. Learning under stress: The inverted-U-shape function revisited. Learn. Mem. 2010, 17, 522–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weerda, R.; Muehlhan, M.; Wolf, O.T.; Thiel, C.M. Effects of acute psychosocial stress on working memory related brain activity in men. Hum. Brain Mapp. 2010, 31, 1418–1429. [Google Scholar] [CrossRef]
- Brunetti, R.; Del Gatto, C.; Delogu, F. eCorsi: Implementation and testing of the Corsi block-tapping task for digital tablets. Front. Psychol. 2014, 5, 1–8. [Google Scholar] [CrossRef]
- Siddi, S.; Preti, A.; Lara, E.; Brébion, G.; Vila, R.; Iglesias, M.; Cuevas-Esteban, J.; López-Carrilero, R.; Butjosa, A.; Haro, J.M. Comparison of the touch-screen and traditional versions of the Corsi block-tapping test in patients with psychosis and healthy controls. BMC Psychiatry 2020, 20, 329. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.J.; Brewer, G. Performance on the traditional and the touch screen, tablet versions of the Corsi Block and the Tower of Hanoi tasks. Comput. Hum. Behav. 2016, 60, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Claessen, M.H.G.; Van Der Ham, I.J.M.; Van Zandvoort, M.J.E. Computerization of the standard corsi block-tapping task affects its underlying cognitive concepts: A pilot study. Appl. Neuropsychol. 2015, 22, 180–188. [Google Scholar] [CrossRef]
- Smyth, M.M.; Scholey, K.A. Determining Spatial Span: The Role of Movement Time and Articulation Rate. Q. J. Exp. Psychol. Sect. A 1992, 45, 479–501. [Google Scholar] [CrossRef]
- Smyth, M.M.; Scholey, K.A. Interference in immediate spatial memory. Mem. Cogn. 1994, 45, 479–501. [Google Scholar] [CrossRef]
- Escamilla, J.C.; Castro, J.J.F.; Baliyan, S.; Ortells-Pareja, J.J.; Rodríguez, J.J.O.; Cimadevilla, J.M. Allocentric spatial memory performance in a virtual reality-based task is conditioned by visuospatial working memory capacity. Brain Sci. 2020, 10, 552. [Google Scholar] [CrossRef] [PubMed]
- Bendall, R.C.A.; Thompson, C. Emotion has no impact on attention in a change detection flicker task. Front. Psychol. 2015, 6, 1592. [Google Scholar] [CrossRef] [Green Version]
- De Waal, F.B.M. Putting the altruism back into altruism: The evolution of empathy. Annu. Rev. Psychol. 2008, 59, 279–300. [Google Scholar] [CrossRef]
- Montag, C.; Schubert, F.; Heinz, A.; Gallinat, J. Prefrontal cortex glutamate correlates with mental perspective-taking. PLoS ONE 2008, 3, e3890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhardt, B.C.; Singer, T. The neural basis of empathy. Annu. Rev. Neurosci. 2012, 35, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soreni, N.; Cameron, D.H.; Streiner, D.L.; Rowa, K.; McCabe, R.E. Seasonality Patterns of Internet Searches on Mental Health: Exploratory Infodemiology Study. JMIR Ment. Health 2019, 6, 12974. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | |
|---|---|
| Gender | 80% female |
| Age | 21.09 (6.42) |
| Ethnicity | 93.6% Caucasian |
| AUCg | 3.880 (1.492) |
| CAR | 0.126 (0.115) |
| BRCS | 13.911 (3.636) |
| DASS (Anxiety) | 8.356 (6.079) |
| DASS (Depression) | 9.422 (5.864) |
| Pre-Pandemic | During-Confinement | |
|---|---|---|
| IRI: Perspective-Taking | 18.93(3.66) | 20.56(3.53) |
| IRI: Empathic Concern | 22.67(3.30) | 22.38(4.02) |
| PSS: Helplessness | 17.51(5.21) | 20.43 (5.30) |
| PSS: Self-Efficacy | 12.95(5.67) | 14.12(5.63) |
| PSS: Total | 30.46(9.45) | 30.46(9.70) |
| Corsi-Forward Score | 8.88 (1.45) | 9.66(1.45) |
| Corsi-Backward Score | 7.77(1.54) | 8.00(1.86) |
| Corsi-Total Score | 16.66(2.52) | 17.71(2.61) |
| Change-Location Score | 3.17(0.35) | 3.26(0.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baliyan, S.; Cimadevilla, J.M.; de Vidania, S.; Pulopulos, M.M.; Sandi, C.; Venero, C. Differential Susceptibility to the Impact of the COVID-19 Pandemic on Working Memory, Empathy, and Perceived Stress: The Role of Cortisol and Resilience. Brain Sci. 2021, 11, 348. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11030348
Baliyan S, Cimadevilla JM, de Vidania S, Pulopulos MM, Sandi C, Venero C. Differential Susceptibility to the Impact of the COVID-19 Pandemic on Working Memory, Empathy, and Perceived Stress: The Role of Cortisol and Resilience. Brain Sciences. 2021; 11(3):348. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11030348
Chicago/Turabian StyleBaliyan, Shishir, José Manuel Cimadevilla, Silvia de Vidania, Matías M. Pulopulos, Carmen Sandi, and César Venero. 2021. "Differential Susceptibility to the Impact of the COVID-19 Pandemic on Working Memory, Empathy, and Perceived Stress: The Role of Cortisol and Resilience" Brain Sciences 11, no. 3: 348. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11030348