
Association between Previous Statin Use and Alzheimer’s Disease: A Nested Case-Control Study Using a National Health Screening Cohort

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
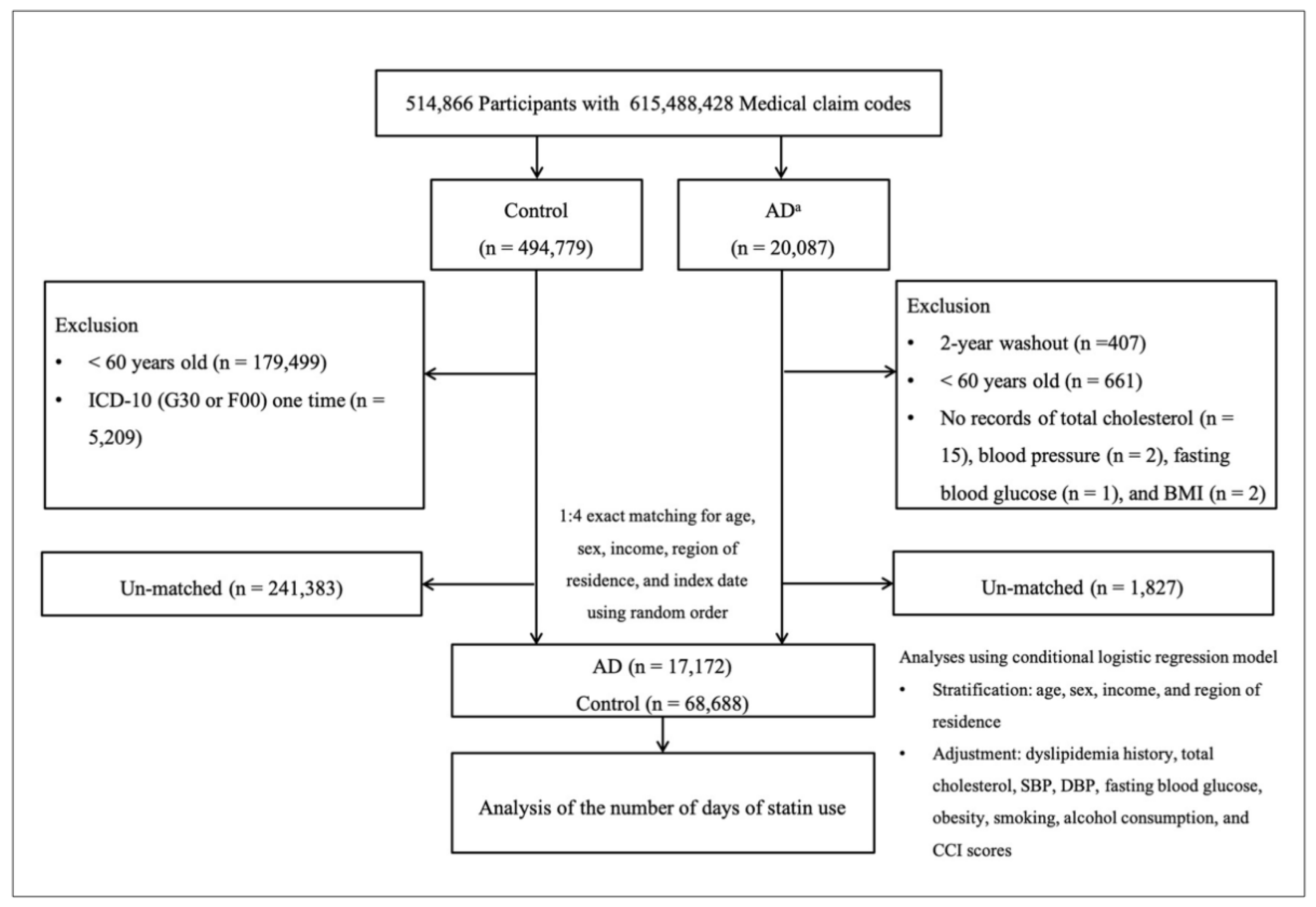
2.1. Study Population
2.2. Patient Selection
2.3. The Number of Days of Statin Use (Exposure)
2.4. Alzheimer’s Disease (Outcome)
2.5. Covariates
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gorelick, P.B. Stroke prevention. An opportunity for efficient utilization of health care resources during the coming decade. Stroke 1994, 25, 220–224. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer’s Disease International. Available online: https://www.alzint.org/about/dementia-facts-figures/ (accessed on 25 February 2021).
- Hung, S.Y.; Fu, W.M. Drug candidates in clinical trials for Alzheimer’s disease. J. Biomed. Sci. 2017, 24, 47. [Google Scholar] [CrossRef] [PubMed]
- Paul, V.F.; David, S.; Elliott, D.B.; Paul, W. New approaches for the treatment of Alzheimer’s disease. Bioorg. Med. Chem. Lett. 2019, 29, 125–133. [Google Scholar]
- Cummings, J.L.; Morstorf, T.; Zhong, K. Alzheimer’s disease drug-development pipeline: Few candidates, frequent failures. Alzheimers Res. Ther. 2014, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Daneschvar, H.L.; Aronson, M.D.; Smetana, G.W. Do statins prevent Alzheimer’s disease? A narrative review. Eur. J. Intern. Med. 2015, 26, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Zhuang, Q.; Yang, J.; Zhang, Y. Statins excert neuroprotection on cerebral ischemia independent of their lipid-lowering action: The potential molecular mechanisms. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 1113–1126. [Google Scholar]
- Power, M.C.; Weuve, J.; Sharrett, A.R.; Blacker, D.; Gottesman, R.F. Statins, cognition, and dementia—Systematic review and methodological commentary. Nat. Rev. Neurol. 2015, 11, 220. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, B.; Craig, D.; Bullock, R.; Passmore, P. Statins for the prevention of dementia. Cochrane Database Syst. Rev. 2009, 2, CD003160, updated in 2016, 1, CD003160. [Google Scholar] [CrossRef]
- Saravi, S.S.S.; Saravi, S.S.S.; Arefidoust, A.; Dehpour, A.R. The beneficial effects of HMG-CoA reductase inhibitors in the processes of neurodegeneration. Metab. Brain. Dis. 2017, 32, 949–965. [Google Scholar] [CrossRef]
- Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet 2002, 360, 7–22. [Google Scholar] [CrossRef]
- Shepherd, J.; Blauw, G.J.; Murphy, M.B.; Bollen, E.; Buckley, B.M.; Cobbe, S.M.; Ford, I.; Gaw, A.; Hyland, M.; Jukema, J.W.; et al. PrOSPer study group. PrOspective Study of Pravastatin in the elderly at risk. Pravastatin in elderly individuals at risk of vascular disease (PrOSPer): A randomised controlled trial. Lancet 2002, 360, 1623–1630. [Google Scholar] [CrossRef]
- Levine, D.A.; Langa, K.M. Vascular cognitive impairment: Disease mechanisms and therapeutic implications. Neurotherapeutics 2011, 8, 361. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Tobacco Smoking and Alcohol Consumption Are Related to Benign Parotid Tumor: A Nested Case-Control Study Using a National Health Screening Cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Risk of neurodegenerative dementia in asthma patients: A nested case–control study using a national sample cohort. BMJ Open 2019, 9, e030227. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lim, J.-S.; Kong, I.G.; Choi, H.G. Hearing impairment and the risk of neurodegenerative dementia: A longitudinal follow-up study using a national sample cohort. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional association between GERD and asthma: Two longitudinal follow-up studies using a national sample cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e1009. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.; Choi, H.G. Practice of epidemiology: Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Beydoun, M.A.; Beason-Held, L.L.; Kitner-Triolo, M.H.; Beydoun, H.A.; Ferrucci, L.; Resnick, S.M.; Zonderman, A.B. Statins and serum cholesterol’s associations with incident dementia and mild cognitive impairment. J. Epidemiol. Community Health 2011, 65, 949–957. [Google Scholar] [CrossRef] [Green Version]
- Bettermann, K.; Arnold, A.M.; Williamson, J.; Rapp, S.; Sink, K.; Toole, J.F.; Carlson, M.C.; Yasar, S.; Dekosky, S.; Burke, G.L. Statins, risk of dementia, and cognitive function: Secondary analysis of the ginkgo evaluation of memory study. J. Stroke Cerebrovasc. Dis. 2012, 21, 436–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haag, M.D.; Hofman, A.; Koudstaal, P.J.; Stricker, B.H.; Breteler, M.M. Statins are associated with a reduced risk of Alzheimer disease regardless of lipophilicity. The Rotterdam Study. J. Neurol. Neurosurg. Psychiatry 2009, 80, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Cramer, C.; Haan, M.; Galea, S.; Langa, K.; Kalbfleisch, J. Use of statins and incidence of dementia and cognitive impairment without dementia in a cohort study. Neurology 2008, 71, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Sparks, D.L.; Kryscio, R.J.; Sabbagh, M.N.; Connor, D.J.; Sparks, L.M.; Liebsack, C. Reduced risk of incident AD with elective statin use in a clinical trial cohort. Curr. Alzheimer Res. 2008, 5, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Swiger, K.J.; Manalac, R.J.; Blumenthal, R.S.; Blaha, M.J.; Martin, S.S. Statins and cognition: A systematic review and meta-analysis of short-and long-term cognitive effects. Mayo Clin. Proc. 2013, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Ott, B.R.; Daiello, L.A.; Dahabreh, I.J.; Springate, B.A.; Bixby, K.; Murali, M.; Trikalinos, T.A. Do statins impair cognition? A systematic review and meta-analysis of randomized controlled trials. J. Gen. Intern. Med. 2015, 30, 348–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reitz, C.; Tang, M.-X.; Luchsinger, J.; Mayeux, R. Relation of plasma lipids to Alzheimer disease and vascular dementia. Arch Neurol. 2004, 61, 705–714. [Google Scholar] [CrossRef] [Green Version]
- Akiyama, H.; Barger, S.; Barnum, S.; Bradt, B.; Bauer, J.; Cole, G.M.; Cooper, N.R.; Eikelenboom, P.; Emmerling, M.; Fiebich, B.L. Inflammation and Alzheimer’s disease. Neurobiol. Aging 2000, 21, 383–421. [Google Scholar] [CrossRef]
- Wanamaker, B.L.; Swiger, K.J.; Blumenthal, R.S.; Martin, S.S. Cholesterol, statins, and dementia: What the cardiologist should know. Clin. Cardiol. 2015, 38, 243–250. [Google Scholar] [CrossRef]
- Wang, Q.; Yan, J.; Chen, X.; Li, J.; Yang, Y.; Weng, J.P.; Deng, C.; Yenari, M.A. Statins: Multiple neuroprotective mechanisms in neurodegenerative diseases. Exp. Neurol. 2011, 230, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Tamboli, I.Y.; Barth, E.; Christian, L.; Siepmann, M.; Kumar, S.; Singh, S.; Tolksdorf, K.; Heneka, M.T.; Lütjohann, D.; Wunderlich, P. Statins promote the degradation of extracellular amyloid β-peptide by microglia via stimulation of exosome-associated insulin-degrading enzyme (IDE) secretion. J. Biol. Chem. 2010, 285, 37405–37414. [Google Scholar] [CrossRef] [Green Version]
- Refolo, L.M.; Pappolla, M.A.; LaFrancois, J.; Malester, B.; Schmidt, S.D.; Thomas-Bryant, T.; Tint, G.S.; Wang, R.; Mercken, M.; Petanceska, S.S.; et al. A cholesterol-lowering drug reduces β-amyloid pathology in a transgenic mouse model of Alzheimer’s disease. Neurobiol. Dis. 2001, 8, 890–899. [Google Scholar] [CrossRef] [Green Version]
- Simons, M.; Keller, P.; Dichgans, J.; Schulz, J.B. Cholesterol and Alzheimer’s disease: Is there a link? Neurology 2001, 57, 1089–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayorh, M.A.; Ganafa, A.A.; Eatman, D.; Walton, M. Simvastatin and losartan enhance nitric oxide and reduce oxidative stress in salt-induced hypertension. Am. J. Hypertens. 2005, 18, 1496–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laufs, U.; La Fata, V.; Plutzky, J.; Liao, J.K. Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation 1998, 97, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Erdös, B.; Snipes, J.A.; Tulbert, C.D.; Katakam, P.; Miller, A.W.; Busija, D.W. Rosuvastatin improves cerebrovascular function in Zucker obese rats by inhibiting NAD (P) H oxidase-dependent superoxide production. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H1264–H1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, M.V.F.; Loures, C.D.M.G.; Alves, L.C.V.; de Souza, L.C.; Borges, K.B.G.; Carvalho, M.D.G. Alzheimer’s disease: Risk factors and potentially protective measures. J. Biomed. Sci. 2019, 26, 33. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, R.A. Risk factors for Alzheimer’s disease. Folia Neuropathol. 2019, 57, 87–105. [Google Scholar] [CrossRef] [Green Version]
- Knopman, D.S.; Parisi, J.E.; Boeve, B.F.; Cha, R.H.; Apaydin, H.; Salviati, A.; Edland, S.D.; Rocca, W.A. Vascular dementia in a population-based autopsy study. Arch Neurol. 2003, 60, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K.A. The enigma of vascular cognitive disorder and vascular dementia. Acta Neuropathol. 2007, 113, 349–388. [Google Scholar] [CrossRef] [PubMed]
- Korczyn, A.D. Mixed dementia—The most common cause of dementia. Ann. N. Y. Acad. Sci. 2002, 977, 129–134. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total Participants | |||
|---|---|---|---|---|
| AD | Control | p Value | ||
| Age (years, n, %) | 1.000 | |||
| 60–64 | 951 (5.5) | 3804 (5.5) | ||
| 65–69 | 2212 (12.9) | 8848 (12.9) | ||
| 70–74 | 4237 (24.7) | 16,948 (24.7) | ||
| 75–79 | 5311 (30.9) | 21,244 (30.9) | ||
| 80–84 | 3826 (22.3) | 15,304 (22.3) | ||
| 85+ | 635 (3.7) | 2540 (3.7) | ||
| Gender (n, %) | 1.000 | |||
| Male | 6742 (39.3) | 26,968 (39.3) | ||
| Female | 10,430 (60.7) | 41,720 (60.7) | ||
| Income (n, %) | 1.000 | |||
| 1 (lowest) | 3519 (20.5) | 14,076 (20.5) | ||
| 2 | 1937 (11.3) | 7748 (11.3) | ||
| 3 | 2324 (13.5) | 9296 (13.5) | ||
| 4 | 3067 (17.9) | 12,268 (17.9) | ||
| 5 (highest) | 6325 (36.8) | 25,300 (36.8) | ||
| Region of residence (n, %) | 1.000 | |||
| Urban | 5986 (34.9) | 23,944 (34.9) | ||
| Rural | 11,186 (65.1) | 44,744 (65.1) | ||
| Total cholesterol (mg/dL, mean, SD) | 197.7 (41.5) | 197.3 (39.5) | 0.284 | |
| SBP (mmHg, mean, SD) | 131.1 (18.0) | 131.4 (17.2) | 0.022 b | |
| DBP (mmHg, mean, SD) | 78.7 (11.1) | 78.7 (10.7) | 1.000 | |
| Fasting blood glucose (mg/dL, mean, SD) | 107.5 (38.6) | 103.1 (29.7) | <0.001 b | |
| Obesity (n, %) c | <0.001 a | |||
| Underweight | 942 (5.5) | 2935 (4.3) | ||
| Normal | 6898 (40.2) | 24,979 (36.4) | ||
| Overweight | 4053 (23.6) | 17,587 (25.6) | ||
| Obese I | 4785 (27.9) | 20,969 (30.5) | ||
| Obese II | 494 (2.9) | 2218 (3.2) | ||
| Smoking status (n, %) | <0.001 a | |||
| Non-smoker | 13,587 (79.1) | 54,537 (79.4) | ||
| Past smoker | 1715 (10.0) | 7570 (11.0) | ||
| Current smoker | 1870 (10.9) | 6581 (9.6) | ||
| Alcohol consumption (n, %) | <0.001 a | |||
| <1 time a week | 13,339 (77.7) | 51,085 (74.4) | ||
| ≥1 time a week | 3833 (22.3) | 17,603 (25.6) | ||
| CCI score (score, n, %) d | <0.001 a | |||
| 0 | 6256 (36.4) | 38,044 (55.4) | ||
| 1 | 4068 (23.7) | 13,134 (19.1) | ||
| 2 | 2605 (15.2) | 7682 (11.2) | ||
| 3 | 1945 (11.3) | 4459 (6.5) | ||
| ≥4 | 2298 (13.4) | 5369 (7.8) | ||
| Dyslipidaemia (n, %) | 6485 (37.8) | 24,781 (36.1) | <0.001 a | |
| Number of days of statin use per year (days, mean, SD) | 114.4 (228.8) | 114.4 (234.2) | 0.997 | |
| Periods of statin prescription (n, %) | <0.001 a | |||
| 0 days | 118,86 (69.2) | 49,995 (72.8) | ||
| ≥1 day & <6 months | 1838 (18.7) | 5104 (7.4) | ||
| ≥6 months & <1 year | 877 (5.1) | 3175 (4.6) | ||
| ≥1 year & <1.5 years | 656 (3.8) | 2234 (3.3) | ||
| ≥1.5 years | 1915 (11.2) | 8180 (11.9) | ||
| Characteristics | Odds Ratios | p Value for Interaction | |||||
|---|---|---|---|---|---|---|---|
| Crude b | p Value | Model 1 bc | p Value | Model 2 bd | p Value | ||
| Total participants (n = 85,860) | 1.00 (0.97–1.03) | 0.997 | 0.96 (0.93–0.99) | 0.003 a | 0.95 (0.92–0.98) | 0.003 a | |
| Age <75 years old, men (n = 14,840) | 1.08 (1.01–1.16) | 0.019 a | 1.00 (0.92–1.08) | 0.918 | 1.00 (0.92–1.08) | 0.912 | 0.009 a |
| Age <75 years old, women (n = 22,160) | 1.08 (1.02–1.13) | 0.004 a | 0.98 (0.92–1.04) | 0.420 | 0.98 (0.92–1.04) | 0.487 | |
| Age ≥75 years old, men (n = 18,870) | 0.98 (0.9–1.04) | 0.581 | 0.96 (0.90–1.03) | 0.210 | 0.95 (0.89–1.02) | 0.150 | |
| Age ≥75 years old, women (n = 29,990) | 0.93 (0.89–0.97) | 0.001 a | 0.92 (0.88–0.97) | 0.002 a | 0.92 (0.88–0.97) | 0.002 a | |
| Low income (n = 38,900) | 1.01 (0.97–1.05) | 0.586 | 0.96 (0.92–1.01) | 0.090 | 0.96 (0.91–1.00) | 0.074 | 0.448 |
| High income (n = 46,960) | 0.99 (0.96–1.03) | 0.650 | 0.95 (0.91–0.99) | 0.014 a | 0.95 (0.91–0.99) | 0.013 a | |
| Urban (n = 29,930) | 0.99 (0.95–1.03) | 0.653 | 0.95 (0.90–0.99) | 0.028 a | 0.95 (0.90–0.99) | 0.029 a | 0.795 |
| Rural (n = 55,930) | 1.01 (0.97–1.04) | 0.717 | 0.96 (0.92–1.00) | 0.044 a | 0.96 (0.92–1.00) | 0.035 a | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Lee, H.S.; Wee, J.H.; Kim, Y.H.; Min, C.Y.; Yoo, D.M.; Choi, H.G. Association between Previous Statin Use and Alzheimer’s Disease: A Nested Case-Control Study Using a National Health Screening Cohort. Brain Sci. 2021, 11, 396. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11030396
Kim JH, Lee HS, Wee JH, Kim YH, Min CY, Yoo DM, Choi HG. Association between Previous Statin Use and Alzheimer’s Disease: A Nested Case-Control Study Using a National Health Screening Cohort. Brain Sciences. 2021; 11(3):396. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11030396
Chicago/Turabian StyleKim, Ji Hee, Heui Seung Lee, Jee Hye Wee, Yoo Hwan Kim, Chan Yang Min, Dae Myoung Yoo, and Hyo Geun Choi. 2021. "Association between Previous Statin Use and Alzheimer’s Disease: A Nested Case-Control Study Using a National Health Screening Cohort" Brain Sciences 11, no. 3: 396. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11030396