
The Effect of Depression on Health-Related Quality of Life Is Mediated by Fatigue in Persons with Multiple Sclerosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
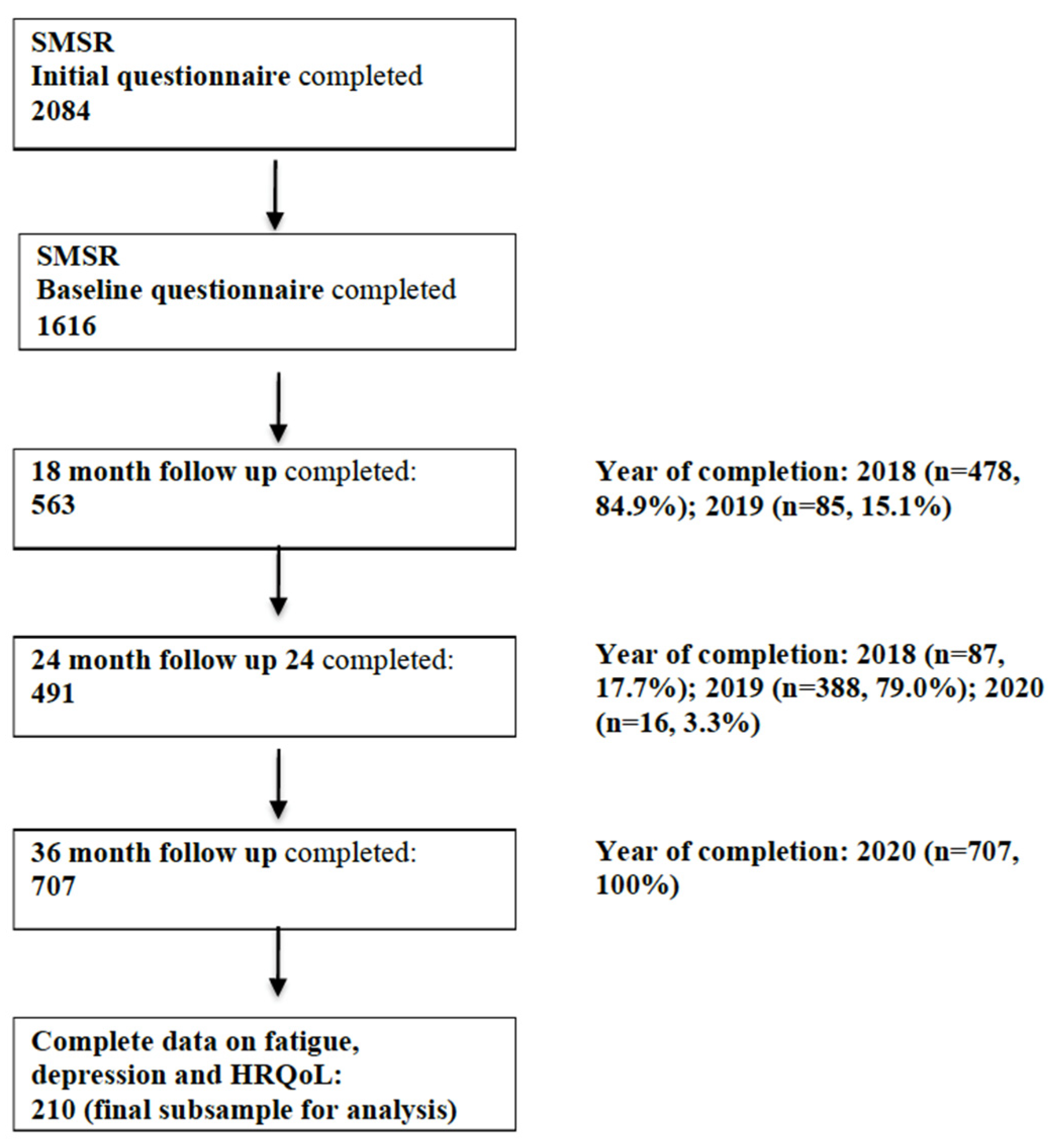
2.1. Study Sample and Data Collection
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis
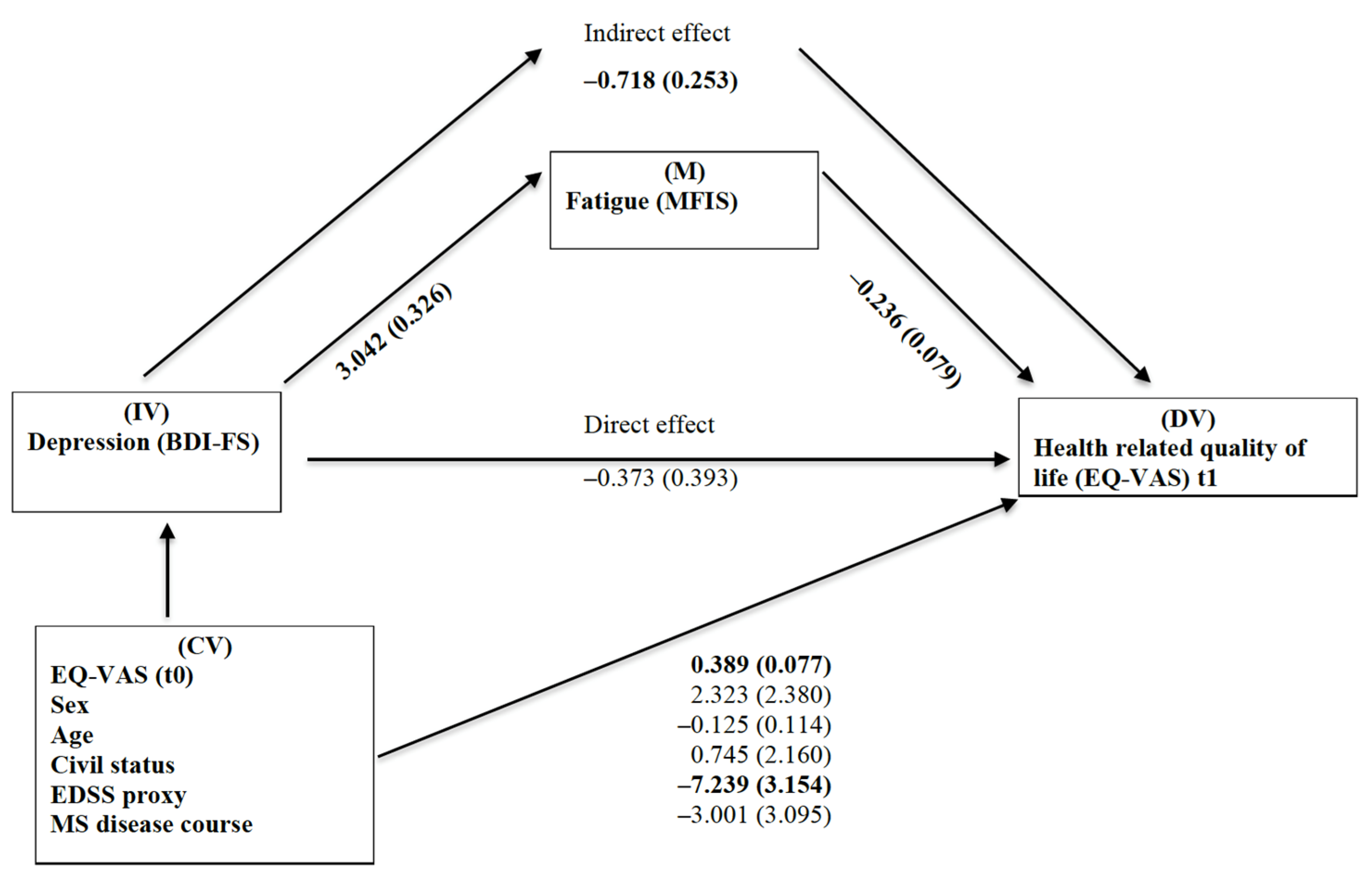
3.2. Regression and Path Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rudick, R.A.; Miller, D.; Clough, J.D.; Gragg, L.A.; Farmer, R.G. Quality of life in multiple sclerosis. Comparison with inflammatory bowel disease and rheumatoid arthritis. Arch. Neurol. 1992, 49, 1237–1242. [Google Scholar] [CrossRef]
- Berrigan, L.I.; Fisk, J.D.; Patten, S.B.; Tremlett, H.; Wolfson, C.; Warren, S.; Fiest, K.M.; McKay, K.A.; Marrie, R.A.; CIHR Team in the Epidemiology and Impact of Comorbidity on Multiple Sclerosis (ECoMS). Health-related quality of life in multiple sclerosis: Direct and indirect effects of comorbidity. Neurology 2016, 86, 1417–1424. [Google Scholar] [CrossRef] [Green Version]
- Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M. Ángeles Quality of life in adults with multiple sclerosis: A systematic review. BMJ Open 2020, 10, e041249. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.H.; Wahlig, E.; Bakshi, R.; Fishman, I.; Munschauer, F.; Zivadinov, R.; Weinstock-Guttman, B. Predicting quality of life in multiple sclerosis: Accounting for physical disability, fatigue, cognition, mood disorder, personality, and behavior change. J. Neurol. Sci. 2005, 231, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Biernacki, T.; Sandi, D.; Kincses, Z.T.; Füvesi, J.; Rózsa, C.; Mátyás, K.; Vécsei, L.; Bencsik, K. Contributing factors to health-related quality of life in multiple sclerosis. Brain Behav. 2019, 9, e01466. [Google Scholar] [CrossRef]
- Kesselring, J.; Beer, S. Symptomatic therapy and neurorehabilitation in multiple sclerosis. Lancet Neurol. 2005, 4, 643–652. [Google Scholar] [CrossRef]
- Wood, B.; Van Der Mei, I.A.F.; Ponsonby, A.-L.; Pittas, F.; Quinn, S.; Dwyer, T.; Lucas, R.M.; Taylor, B. Prevalence and concurrence of anxiety, depression and fatigue over time in multiple sclerosis. Mult. Scler. J. 2013, 19, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Manjaly, Z.-M.; A Harrison, N.; Critchley, H.; Do, C.T.; Stefanics, G.; Wenderoth, N.; Lutterotti, A.; Müller, A.; Stephan, K.E. Pathophysiological and cognitive mechanisms of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, P.; Kobelt, G.; Berg, J.; Capsa, D.; Eriksson, J.; The European Multiple Sclerosis Platform. New insights into the burden and costs of multiple sclerosis in Europe: Results for Switzerland. Mult. Scler. J. 2017, 23, 192–203. [Google Scholar] [CrossRef] [Green Version]
- Stuke, K.; Flachenecker, P.; Zettl, U.K.; Elias, W.G.; Freidel, M.; Haas, J.; Pitschnau-Michel, D.; Schimrigk, S.; Rieckmann, P. Symptomatology of MS: Results from the German MS Registry. J. Neurol. 2009, 256, 1932–1935. [Google Scholar] [CrossRef]
- Jones, K.H.; Ford, D.; Jones, P.A.; John, A.; Middleton, R.M.; Lockhart-Jones, H.; Osborne, L.A.; Noble, J.G. A Large-Scale Study of Anxiety and Depression in People with Multiple Sclerosis: A Survey via the Web Portal of the UK MS Register. PLoS ONE 2012, 7, e41910. [Google Scholar] [CrossRef]
- Schippling, S.; O’Connor, P.; Knappertz, V.; Pohl, C.; Bogumil, T.; Suarez, G.; Cook, S.; Filippi, M.; Hartung, H.-P.; Comi, G.; et al. Incidence and course of depression in multiple sclerosis in the multinational BEYOND trial. J. Neurol. 2016, 263, 1418–1426. [Google Scholar] [CrossRef] [Green Version]
- Patten, S.B.; Fridhandler, S.; A Beck, C.; Metz, L.M. Depressive symptoms in a treated multiple sclerosis cohort. Mult. Scler. J. 2003, 9, 616–620. [Google Scholar] [CrossRef]
- Amtmann, D.; Kim, J.; Chung, H.; Bamer, A.M.; Askew, R.L.; Wu, S.; Cook, K.F.; Johnson, K.L. Comparing CESD-10, PHQ-9, and PROMIS depression instruments in individuals with multiple sclerosis. Rehabil. Psychol. 2014, 59, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Sadovnick, A.D.; Remick, R.A.; Allen, J.; Swartz, E.; Yee, I.; Eisen, K.; Farquhar, R.; Hashimoto, S.A.; Hooge, J.; Kastrukoff, L.F.; et al. Depression and multiple sclerosis. Neurology 1996, 46, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Barin, L.; Salmen, A.; Disanto, G.; Babačić, H.; Calabrese, P.; Chan, A.; Kamm, C.P.; Kesselring, J.; Kuhle, J.; Gobbi, C.; et al. The disease burden of Multiple Sclerosis from the individual and population perspective: Which symptoms matter most? Mult. Scler. Relat. Disord. 2018, 25, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Janssens, A.C.; van Doorn, P.A.; de Boer, J.B.; Kalkers, N.F.; van der Meche, F.G.; Passchier, J.; Hintzen, R.Q. Anxiety and depression influence the relation between disability status and quality of life in multiple sclerosis. Mult. Scler. 2003, 9, 397–403. [Google Scholar] [CrossRef]
- Marrie, R.A.; Horwitz, R.; Cutter, G.; Tyry, T. Cumulative impact of comorbidity on quality of life in MS. Acta Neurol. Scand. 2011, 125, 180–186. [Google Scholar] [CrossRef]
- Kargarfard, M.; Eetemadifar, M.; Mehrabi, M.; Maghzi, A.H.; Hayatbakhsh, M.R. Fatigue, depression, and health-related quality of life in patients with multiple sclerosis in Isfahan, Iran. Eur. J. Neurol. 2011, 19, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, A.M.; Schiavolin, S.; Brenna, G.; Brambilla, L.; Confalonieri, P.; Cortese, F.; Covelli, V.; Frangiamore, R.; Leonardi, M.; Mantegazza, R.; et al. Cognitive function alone is a poor predictor of health-related quality of life in employed patients with MS: Results from a cross-sectional study. Clin. Neuropsychol. 2016, 30, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Janardhan, V.; Bakshi, R. Quality of life in patients with multiple sclerosis: The impact of fatigue and depression. J. Neurol. Sci. 2002, 205, 51–58. [Google Scholar] [CrossRef]
- Gravesande, K.S.V.; Blaschek, A.; Calabrese, P.; Rostásy, K.; Huppke, P.; Kessler, J.J.; Kalbe, E.; Mall, V. Fatigue and depression predict health-related quality of life in patients with pediatric-onset multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 36, 101368. [Google Scholar] [CrossRef]
- Nourbakhsh, B.; Julian, L.; Waubant, E. Fatigue and depression predict quality of life in patients with early multiple sclerosis: A longitudinal study. Eur. J. Neurol. 2016, 23, 1482–1486. [Google Scholar] [CrossRef]
- Chruzander, C.; Ytterberg, C.; Gottberg, K.; Einarsson, U.; Holmqvist, L.W.; Johansson, S. A 10-year follow-up of a population-based study of people with multiple sclerosis in Stockholm, Sweden: Changes in health-related quality of life and the value of different factors in predicting health-related quality of life. J. Neurol. Sci. 2014, 339, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Mohr, D.C.; Hart, S.L.; Goldberg, A. Effects of Treatment for Depression on Fatigue in Multiple Sclerosis. Psychosom. Med. 2003, 65, 542–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Muñoz, J.J.; Cigarán-Méndez, M.; Navarro-Pardo, E.; Pérez-De-Heredia-Torres, M.; Parás-Bravo, P.; Fernández-De-Las-Peñas, C. Is the association between health-related quality of life and fatigue mediated by depression in patients with multiple sclerosis? A Spanish cross-sectional study. BMJ Open 2018, 8, e016297. [Google Scholar] [CrossRef]
- Ford, H.; Trigwell, P.; Johnson, M. The nature of fatigue in multiple sclerosis. J. Psychosom. Res. 1998, 45, 33–38. [Google Scholar] [CrossRef]
- Gold, S.M.; Irwin, M.R. Depression and Immunity: Inflammation and Depressive Symptoms in Multiple Sclerosis. Immunol. Allergy Clin. N. Am. 2009, 29, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Gunzler, D.D.; Perzynski, A.; Morris, N.; Bermel, R.; Lewis, S.; Miller, D. Disentangling multiple sclerosis and de-pression: An adjusted depression screening score for patient-centered care. J. Behav. Med. 2015, 38, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, R.; Shaikh, Z.A.; Miletich, R.S.; Czarnecki, D.; Dmochowski, J.; Henschel, K.; Janardhan, V.; Dubey, N.; Kinkel, P.R. Fatigue in multiple sclerosis and its relationship to depression and neurologic disability. Mult. Scler. 2000, 6, 181–185. [Google Scholar] [CrossRef]
- Benedict, R.H.; Fishman, I.; McClellan, M.M.; Bakshi, R.; Weinstock-Guttman, B. Validity of the beck depression in-ventory-fast screen in multiple sclerosis. Mult. Scler. 2003, 9, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.; Magalhaes, S.; Richard, J.-F.; Audet, B.; Moore, C.S. The link between multiple sclerosis and depression. Nat. Rev. Neurol. 2014, 10, 507–517. [Google Scholar] [CrossRef]
- Thombs, B.D.; Ziegelstein, R.C.; Pilote, L.; Dozois, D.J.A.; Beck, A.T.; Dobson, K.S.; Fuss, S.; De Jonge, P.; Grace, S.L.; Stewart, D.E.; et al. Somatic symptom overlap in Beck Depression Inventory–II scores following myocardial infarction. Br. J. Psychiatry 2010, 197, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Steinemann, N.; Kuhle, J.; Calabrese, P.; Kesselring, J.; Disanto, G.; Merkler, D.; Pot, C.; Ajdacic-Gross, V.; Rodgers, S.; Puhan, M.A.; et al. The Swiss Multiple Sclerosis Registry (SMSR): Study protocol of a participatory, nationwide registry to promote epidemiological and patient-centered MS research. BMC Neurol. 2018, 18, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puhan, M.A.; Steinemann, N.; Kamm, C.P.; Müller, S.; Kuhle, J.; Kurmann, R.; Calabrese, P.; Kesselring, J.; Von Wyl, V.; Swiss Multiple Sclerosis Registry, SMSR. A digitally facilitated citizen-science driven approach accelerates participant recruitment and increases study population diversity. Swiss Med. Wkly. 2018, 148, w14623. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Matter-Walstra, K.; Klingbiel, D.; Szucs, T.; Pestalozzi, B.C.; Schwenkglenks, M. Using the EuroQol EQ-5D in Swiss Cancer Patients, Which Value Set Should be Applied? Pharmacoeconomics 2014, 32, 591–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perneger, T.V.; Combescure, C.; Courvoisier, D.S. General Population Reference Values for the French Version of the EuroQol EQ-5D Health Utility Instrument. Value Health 2010, 13, 631–635. [Google Scholar] [CrossRef]
- Barin, L.; Kaufmann, M.; Salmen, A.; Kamm, C.P.; Gobbi, C.; Kuhle, J.; Pot, C.; Chan, A.; Czaplinski, A.; Ajdacic-Gross, V.; et al. Patterns of care for Multiple Sclerosis in a setting of universal care access: A cross-sectional study. Mult. Scler. Relat. Disord. 2019, 28, 17–25. [Google Scholar] [CrossRef]
- Fisk, J.D.; Ritvo, P.G.; Ross, L.; Haase, D.A.; Marrie, T.J.; Schlech, W.F. Measuring the Functional Impact of Fatigue: Initial Validation of the Fatigue Impact Scale. Clin. Infect. Dis. 1994, 18, S79–S83. [Google Scholar] [CrossRef]
- Flachenecker, P.; Kümpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P.; Trenkwalder, C.; Toyka, K.V. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. J. 2002, 8, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Kos, D.; Kerckhofs, E.; Carrea, I.; Verza, R.; Ramos, M.; Jansa, J. Evaluation of the Modified Fatigue Impact Scale in four different European countries. Mult. Scler. J. 2005, 11, 76–80. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. BDI—Fast Screen for Medical Patients Manual; The Psychological Corporation: San Antonio, TX, USA, 2000. [Google Scholar]
- A Steer, R.; A Cavalieri, T.; Leonard, D.M.; Beck, A.T. Use of the Beck depression inventory for primary care to screen for major depression disorders. Gen. Hosp. Psychiatry 1999, 21, 106–111. [Google Scholar] [CrossRef]
- Strober, L.B.; Arnett, P.A. Depression in multiple sclerosis: The utility of common self-report instruments and de-velopment of a disease-specific measure. J. Clin. Exp. Neuropsychol. 2015, 37, 722–732. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, M.; Salmen, A.; Barin, L.; Puhan, M.A.; Calabrese, P.; Kamm, C.P.; Gobbi, C.; Kuhle, J.; Manjaly, Z.-M.; Ajdacic-Gross, V.; et al. Development and validation of the self-reported disability status scale (SRDSS) to estimate EDSS-categories. Mult. Scler. Relat. Disord. 2020, 42, 102148. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator mediator variable distinction in social psychological-research—Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivar. Behav Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [Green Version]
- Sobel, M.E. Asymptotic Confidence Intervals for Indirect Effects in Structural Equation Models. Sociol. Methodol. 1982, 13, 290. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- IBM Corp. IBM Spss Statistics for Macintosh, Version 25.0; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Nunnari, D.; De Cola, M.C.; D’Aleo, G.; Rifici, C.; Russo, M.; Sessa, E.; Bramanti, P.; Marino, S. Impact of Depression, Fatigue, and Global Measure of Cortical Volume on Cognitive Impairment in Multiple Sclerosis. Biomed Res. Int. 2015, 2015, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kroencke, D.C.; Lynch, S.G.; Denney, D.R. Fatigue in multiple sclerosis: Relationship to depression, disability, and disease pattern. Mult. Scler. 2000, 6, 131–136. [Google Scholar] [CrossRef]
- Strober, L.B.; Arnett, P.A. An examination of four models predicting fatigue in multiple sclerosis. Arch. Clin. Neuropsychol. 2005, 20, 631–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Multiple Sclerosis Council for Clinical Practice Guidelines. Fatigue and Multiple Sclerosis: Evidence-based Management Strategies for Fatigue in Multiple Sclerosis; Paralyzed Veterans of America: Washington, DC, USA, 1998. [Google Scholar]
- Miller, J.; Calabrese, P. The role of inflammation in depression. Curr. Neurobiol. 2021, in press. [Google Scholar]
- Brenner, P.; Piehl, F. Fatigue and depression in multiple sclerosis: Pharmacological and non-pharmacological interventions. Acta Neurologica Scandinavica 2016, 134, 47–54. [Google Scholar] [CrossRef]
- Grossman, P.; Kappos, L.; Gensicke, H.; D’Souza, M.; Mohr, D.C.; Penner, I.-K.; Steiner, C. MS quality of life, depression, and fatigue improve after mindfulness training: A randomized trial. Neurology 2010, 75, 1141–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, R.; Simpson, S.; Ramparsad, N.; Lawrence, M.; Booth, J.; Mercer, S.W. Effects of mindfulness-based inter-ventions on physical symptoms in people with multiple sclerosis—A systematic review and meta-analysis. Mult. Scler. Relat. Dis. 2020, 38. [Google Scholar]
- Han, A. Mindfulness-and acceptance-based interventions for symptom reduction of people with multiple sclerosis: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2021. [Google Scholar] [CrossRef] [PubMed]
- Segal, Z.V.; Williams, M.; Teasdale, J. Mindfulness-Based Cognitive Therapy for Depression; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sample Characteristic | n = 210 |
|---|---|
| Sociodemographics | |
| Sex | |
| Women | 150 (71.4%) |
| Men | 60 (28.6%) |
| Age (median (IQR)) | 50.5 (44.0; 58.0) |
| Education 1, a | |
| Low | 78 (38.2%) |
| High | 126 (61.8%) |
| Occupational status b | |
| Working | 141 (67.5%) |
| Not working | 68 (32.5%) |
| Urbanicity 2 | |
| Urban | 192 (91.4%) |
| Urban to rural | 3 (1.4%) |
| Rural | 15 (7.1%) |
| Civil status | |
| Married or registered partnership | 121 (57.6%) |
| Other | 89 (42.4%) |
| Clinical MS-related MS Disease Course c | |
| CIS | 2 (1.0%) |
| RRMS | 146 (69.9%) |
| PPMS | 17 (8.1%) |
| SPMS | 36 (17.2%) |
| Transition or other type | 8 (3.8%) |
| Dichotomized MS Disease Course (Excluding CIS) c | |
| RRMS | 146 (70.5%) |
| Progressive MS (PPMS, SPMS, Transition) | 61 (29.5%) |
| Time since MS Diagnosis d (median (IQR)) | 11.0 (6.0; 17.0) |
| Disease Modifying Treatment e (current, past 6 months) | |
| Yes | 146 (71.2%) |
| No | 59 (28.8%) |
| Bouts f (current, past 6 months) | |
| Yes | 15 (7.8%) |
| No | 177 (92.2%) |
| Proxy Measure to Estimate EDSS g | |
| EDSS 0–3.5 | 147 (70.3%) |
| EDSS 4–6.5 | 45 (21.5%) |
| EDSS ≥ 7 | 17 (8.1%) |
| Fatigue Sum Scores (MFIS) | |
| Clinically relevant fatigue | 71 (33.8%) |
| No clinically relevant fatigue | 139 (66.2%) |
| Overall sum score (median (IQR)) | 30.0 (13.8; 42.0) |
| Cognitive subscale (median (IQR)) | 11.0 (5.0; 18.0) |
| Physical subscale (median (IQR)) | 15.0 (5.8; 20.0) |
| Psychosocial subscale (median (IQR)) | 3.0 (1.0; 4.3) |
| Health-Related Quality of Life | |
| EQ-VAS (18-month follow-up survey) (median (IQR)) | 80.0 (65.0; 90.3) |
| EQ-5D-index (18-month follow-up survey) h (median (IQR)) | 71.1 (50.5; 92.9) |
| EQ-VAS (36-month follow-up survey) (median (IQR)) | 80.0 (60.0; 90.0) |
| EQ-5D-index (36-month follow-up survey) i (median (IQR)) | 71.4 (47.2; 91.0) |
| Clinical Depression-Related BDI-FS | |
| Clinically relevant depressive symptomatology | 53 (25.2%) |
| No clinically relevant depressive symptomatology | 157 (74.8%) |
| Overall sum score (median (IQR)) | 1.0 (0.0;4.0) |
| Antidepressants | |
| Yes | 16 (7.6%) |
| No | 197 (92.9%) |
| If yes (n = 16) | |
| Selective serotonin reuptake inhibitors (SSRIs) | 5 (31.2%) |
| Serotonin–norepinephrine reuptake inhibitors (SNRIs) | 5 (31.2%) |
| Serotonin antagonist and reuptake inhibitors (SARIs) | 1 (6.3%) |
| Tricyclic antidepressants (TCAs) | 1 (6.3%) |
| Herbal antidepressants (St. John’s wort) | 2 (12.5%) |
| Detailed information missing | 2 (12.5%) |
| Psychotherapy | |
| Yes | 32 (15.2%) |
| No | 178 (84.8%) |
| Consumption of Psychoactive Substances | |
| Smoking Status | |
| Still smoking | 35 (16.7%) |
| No | 175 (83.3%) |
| Effects on EQ-5D (DV) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IV | M | Effect of IV on M | Direct Effect of IV on DV | Effect of M on DV | Effect of IV on DV after Inclusion of M to the Model | ||||||||||||
| Estimate | Estimate | Estimate | Estimate | ||||||||||||||
| B | SE | β | p-Value | B | SE | β | p-Value | B | SE | β | p-Value | B | SE | β | p-Value | ||
| BDI- FS Sum Score | MFIS Sum Score | 1.926 | 0.326 | 0.345 | <0.001 | −0.828 | 0.378 | −0.125 | 0.030 | −0.265 | 0.075 | −0.224 | <0.001 | −0.373 | 0.402 | −0.056 | 0.355 |
| MFIS Subscale | B | SE |
|---|---|---|
| Physical subscale | −0.624 | 0.250 |
| Psychosocial subscale | −0.538 | 0.256 |
| Cognitive subscale | −0.485 | 0.192 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodgers, S.; Manjaly, Z.-M.; Calabrese, P.; Steinemann, N.; Kaufmann, M.; Salmen, A.; Chan, A.; Kesselring, J.; Kamm, C.P.; Kuhle, J.; et al. The Effect of Depression on Health-Related Quality of Life Is Mediated by Fatigue in Persons with Multiple Sclerosis. Brain Sci. 2021, 11, 751. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060751
Rodgers S, Manjaly Z-M, Calabrese P, Steinemann N, Kaufmann M, Salmen A, Chan A, Kesselring J, Kamm CP, Kuhle J, et al. The Effect of Depression on Health-Related Quality of Life Is Mediated by Fatigue in Persons with Multiple Sclerosis. Brain Sciences. 2021; 11(6):751. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060751
Chicago/Turabian StyleRodgers, Stephanie, Zina-Mary Manjaly, Pasquale Calabrese, Nina Steinemann, Marco Kaufmann, Anke Salmen, Andrew Chan, Jürg Kesselring, Christian P. Kamm, Jens Kuhle, and et al. 2021. "The Effect of Depression on Health-Related Quality of Life Is Mediated by Fatigue in Persons with Multiple Sclerosis" Brain Sciences 11, no. 6: 751. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060751