
Differentiating Functional Cognitive Disorder from Early Neurodegeneration: A Clinic-Based Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Questionnaires
- vascular risk factors (hypertension, diabetes mellitus, hypercholesterolaemia, atrial fibrillation, coronary or cerebral or peripheral vascular disease), or use of medications unequivocally for these conditions;
- functional conditions excluding FCD (irritable bowel syndrome, non-epileptic attack disorder, chronic fatigue syndrome/myalgic encephalomyelitis, fibromyalgia);
- depression or anxiety, or use of medications unequivocally for this indication (e.g., including SSRIs but excluding amitriptyline and St John’s Wort);
- medications were listed and screened to identify those that can potentially impair cognition (this comprised patients on low levels of opiates, tramadol, pregabalin, gabapentin, lamotrigine, sleeping tablets, or amitriptyline).
2.3. Cognitive and Mood Assessments, and Analysis
2.4. Performance Validity, Personality Assessment, and Analysis
- higher levels of emotional/internalising dysfunction (“EID”)
- higher somatic complaints (excluding cognitive complaints) (“RC1”)
- higher cognitive complaints (“COG”)
- fewer positive emotional experiences, and avoid social situations and interactions (“INTr”)
- higher scores on scale “NEGE-r” (indicating those prone to experiencing a wide range of negative emotional experiences, which is associated with neuroticism in the 5-factor model of personality)
3. Results
3.1. Demographics and Background
3.2. Depression, Anxiety and Stress
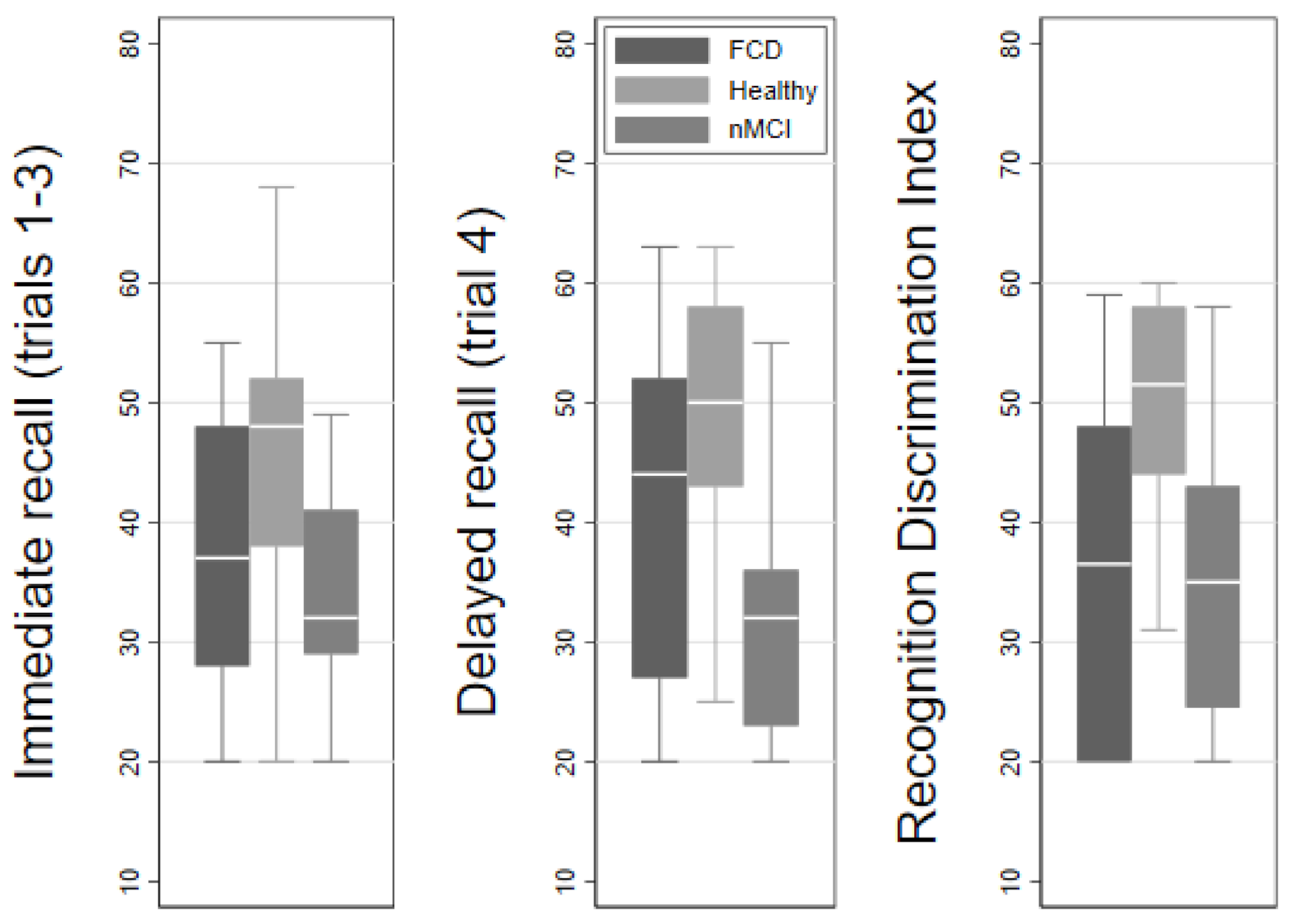
3.3. Cognitive Testing
3.4. Personality Data
3.4.1. Embedded Performance Validity Measures
3.4.2. Personality Content
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bharambe, V.; Larner, A.J. Functional cognitive disorders: Memory clinic study. Prog. Neurol. Psychiatry 2018, 22, 19–22. [Google Scholar] [CrossRef] [Green Version]
- Elsey, C.; Drew, P.; Jones, D.; Blackburn, D.; Wakefield, S.; Harkness, K.; Venneri, A.; Reuber, M. Towards diagnostic conversational profiles of patients presenting with dementia or functional memory disorders to memory clinics. Patient Educ. Couns. 2015, 98, 1071–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennington, C.; Hayre, A.; Newson, M.; Coulthard, E. Functional Cognitive Disorder: A Common Cause of Subjective Cognitive Symptoms. J. Alzheimers Dis. 2015, 48, S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.; Edwards, M. Trick or treat? Showing patients with functional (psychogenic) motor symptoms their physical signs. Neurology 2012, 79, 282–284. [Google Scholar] [CrossRef]
- McWhirter, L.; Ritchie, C.; Stone, J.; Carson, A. Functional cognitive disorders: A systematic review. Lancet Psychiatry 2020, 7, 191–207. [Google Scholar] [CrossRef]
- Schmidtke, K.; Pohlmann, S.; Metternich, B. The syndrome of functional memory disorder: Definition, etiology, and natural course. Off. J. Am. Assoc. Geriatr. Psychiatry 2008, 16, 981–988. [Google Scholar] [CrossRef]
- Ball, H.A.; McWhirter, L.; Ballard, C.; Bhome, R.; Blackburn, D.J.; Edwards, M.J.; Fleming, S.M.; Fox, N.C.; Howard, R.; Huntley, J.; et al. Functional cognitive disorder: Dementia’s blind spot. Brain 2020, 143, 2895–2903. [Google Scholar] [CrossRef]
- Stone, J. Functional neurological disorders: The neurological assessment as treatment. Pract. Neurol. 2016, 16, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Blackburn, D.; Reuber, M. Patients’ accounts of memory lapses in interactions between neurologists and patients with functional memory disorders. Sociol. Health Illn. 2019, 41, 249–265. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, F.C.; Loring, D.W.; Thomas, T.; Saleh, S.; Hajjar, I. Recognition Memory Performance as a Cognitive Marker of Prodromal Alzheimer’s Disease. J. Alzheimer’s Dis. JAD 2019, 72, 507–514. [Google Scholar] [CrossRef]
- Russo, M.J.; Campos, J.; Vazquez, S.; Sevlever, G.; Allegri, R.F. Adding Recognition Discriminability Index to the Delayed Recall Is Useful to Predict Conversion from Mild Cognitive Impairment to Alzheimer’s Disease in the Alzheimer’s Disease Neuroimaging Initiative. Front. Aging Neurosci. 2017, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Squire, L.R.; Wixted, J.T.; Clark, R.E. Recognition memory and the medial temporal lobe: A new perspective. Nat. Rev. Neurosci. 2007, 8, 872–883. [Google Scholar] [CrossRef] [Green Version]
- Teodoro, T.; Edwards, M.J.; Isaacs, J.D. A unifying theory for cognitive abnormalities in functional neurological disorders, fibromyalgia and chronic fatigue syndrome: Systematic review. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1308–1319. [Google Scholar] [CrossRef] [Green Version]
- McWhirter, L.; Ritchie, C.W.; Stone, J.; Carson, A. Performance validity test failure in clinical populations—A systematic review. J. Neurol. Neurosurg. Psychiatry 2020, 91, 945–952. [Google Scholar] [CrossRef]
- Rossetti, M.A.; Collins, R.L.; York, M.K. Performance Validity in Deep Brain Stimulation Candidates. Arch. Clin. Neuropsychol. 2017, 33, 508–514. [Google Scholar] [CrossRef]
- Jalilianhasanpour, R.; Williams, B.; Gilman, I.; Burke, M.J.; Glass, S.; Fricchione, G.L.; Keshavan, M.S.; LaFrance, W.C., Jr.; Perez, D.L. Resilience linked to personality dimensions, alexithymia and affective symptoms in motor functional neurological disorders. J. Psychosom. Res. 2018, 107, 55–61. [Google Scholar] [CrossRef]
- Cragar, D.E.; Berry, D.T.; Schmitt, F.A.; Fakhoury, T.A. Cluster analysis of normal personality traits in patients with psychogenic nonepileptic seizures. Epilepsy Behav. 2005, 6, 593–600. [Google Scholar] [CrossRef]
- Stone, J.; Warlow, C.; Deary, I.; Sharpe, M. Predisposing Risk Factors for Functional Limb Weakness: A Case-Control Study. J. Neuropsychiatry Clin. Neurosci. 2020, 32, 50–57. [Google Scholar] [CrossRef]
- Schmaling, K.B.; Jones, J.F. MMPI profiles of patients with chronic fatigue syndrome. J. Psychosom. Res. 1996, 40, 67–74. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Duncan, C.J.; Roberts, N.A.; Kirlin, K.A.; Parkhurst, D.; Burleson, M.H.; Drazkowski, J.F.; Sirven, J.I.; Noe, K.H.; Crepeau, A.Z.; Hoerth, M.T.; et al. Diagnostic utility of the Minnesota Multiphasic Personality Inventory-2 Restructured Form in the epilepsy monitoring unit: Considering sex differences. Epilepsy Behav. 2018, 88, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Mousavinasab, S.M.; Gorganinezhad-Moshiri, M.; Saberifirouzi, M.; Dehbozorgi, G.; Mehrabani, D. Personality characteristics and irritable bowel syndrome in Shiraz, southern Iran. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2007, 13, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Alluri, P.R.; Solit, J.; Leveroni, C.L.; Goldberg, K.; Vehar, J.V.; Pollak, L.E.; Colvin, M.K.; Perez, D.L. Cognitive Complaints in Motor Functional Neurological (Conversion) Disorders: A Focused Review and Clinical Perspective. Cogn. Behav. Neurol. 2020, 33, 77–89. [Google Scholar] [CrossRef] [PubMed]
- van der Hoeven, R.M.; Broersma, M.; Pijnenborg, G.H.; Koops, E.A.; van Laar, T.; Stone, J.; van Beilen, M. Functional (psychogenic) movement disorders associated with normal scores in psychological questionnaires: A case control study. J. Psychosom. Res. 2015, 79, 190–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conversano, C.; Marchi, L.; Ciacchini, R.; Carmassi, C.; Contena, B.; Bazzichi, L.M.; Gemignani, A. Personality Traits in Fibromyalgia (FM): Does FM Personality Exists? A Systematic Review. Clin. Pract. Epidemiol. Ment. Health 2018, 14, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Pennington, C.; Ball, H.; Swirski, M. Functional Cognitive Disorder: Diagnostic Challenges and Future Directions. Diagnostics 2019, 9, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Shapiro, A.M.; Benedict, R.H.B.; Schretlen, D.; Brandt, J. Construct and Concurrent Validity of the Hopkins Verbal Learning Test—Revised. Clin. Neuropsychol. 1999, 13, 348–358. [Google Scholar] [CrossRef]
- Crawford, J.R.; Henry, J.D. The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample. Br. J. Clin. Psychol. 2003, 42 (Pt 2), 111–131. [Google Scholar] [CrossRef] [Green Version]
- Macmillan, N.A.; Creelman, C.D. Detection Theory: A User’s Guide; Psychology Press: New York, NY, USA, 2004. [Google Scholar]
- Ben-Porath, Y.S.; Tellegen, A. The Minnesota Multiphasic Personality Inventory-2 Restructured Form: Manual for Administration, Scoring, and Interpretation; University of Minnesota Press: Minneapolis, MN, USA, 2008. [Google Scholar]
- Sharf, A.J.; Rogers, R.; Williams, M.M.; Henry, S.A. The Effectiveness of the MMPI-2-RF in Detecting Feigned Mental Disorders and Cognitive Deficits: A Meta-Analysis. J. Psychopathol. Behav. Assess. 2017, 39, 441–455. [Google Scholar] [CrossRef]
- Beaudoin, M.; Desrichard, O. Are memory self-efficacy and memory performance related? A meta-analysis. Psychol. Bull. 2011, 137, 211–241. [Google Scholar] [CrossRef]
- Bhome, R.; McWilliams, A.; Huntley, J.D.; Fleming, S.M.; Howard, R.J. Metacognition in functional cognitive disorder-a potential mechanism and treatment target. Cogn. Neuropsychiatry 2019, 24, 311–321. [Google Scholar] [CrossRef]
- Camos, V.; Portrat, S. The impact of cognitive load on delayed recall. Psychon. Bull. Rev. 2015, 22, 1029–1034. [Google Scholar] [CrossRef] [Green Version]
- Tran, T.; Milanovic, M.; Holshausen, K.; Bowie, C.R. What is normal cognition in depression? Prevalence and functional correlates of normative versus idiographic cognitive impairment. Neuropsychology 2021, 35, 33–41. [Google Scholar] [CrossRef]
- Sawyer, R.J.; Testa, S.M.; Dux, M. Embedded performance validity tests within the Hopkins Verbal Learning Test—Revised and the Brief Visuospatial Memory Test—Revised. Clin. Neuropsychol. 2017, 31, 207–218. [Google Scholar] [CrossRef]
- Smith, K.; Boone, K.; Victor, T.; Miora, D.; Cottingham, M.; Ziegler, E.; Zeller, M.; Wright, M. Comparison of Credible Patients of Very Low Intelligence and Non-Credible Patients on Neurocognitive Performance Validity Indicators. Clin. Neuropsychol. 2014, 28, 1048–1070. [Google Scholar] [CrossRef]
- Boone, K.B.; Lu, P.; Wen, J. Comparison of various RAVLT scores in the detection of noncredible memory performance. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2005, 20, 301–319. [Google Scholar] [CrossRef] [Green Version]
- Paula, J.J.; Miranda, D.M.; Nicolato, R.; Moraes, E.N.; Bicalho, M.A.; Malloy-Diniz, L.F. Verbal learning on depressive pseudodementia: Accentuate impairment of free recall, moderate on learning processes, and spared short-term and recognition memory. Arq. Neuropsiquiatr. 2013, 71, 596–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| FCD | Healthy | nMCI | ||
|---|---|---|---|---|
| Mean (SD) | ANOVA F (p) | |||
| Age | 58.3 (12.6) | 60.8 (5.8) | 72.1 (11.7) | 9.59 (<0.01) |
| Years of education | 13.8 (2.8) | 14.7 (3.7) | 14.4 (3.0) | 0.50 (0.61) |
| n (%) per group | Chi2 (p) | |||
| Sex (female) | 10 (48) | 18 (72) | 8 (47) | 3.73 (0.15) |
| Vascular risk factors | 8 (40) | 7 (28) | 14 (82) | 12.55 (<0.01) |
| Other functional disorder (excluding FCD) | 4 ^ (20) | 4 ^^ (16) | 0 (0) | 3.63 (0.16) |
| Depression or anxiety | 5 (24) | 3 (12) | 3 (18) | 1.19 (0.55) |
| Medication with potential cognitive side effects | 9 (43) | 8 (32) | 5 (29) | 1.20 (0.55) |
| Depression Anxiety and Stress Scale | Mean (SD) | Regression 1: Coefficient (p) | |||
|---|---|---|---|---|---|
| FCD | Healthy | nMCI | FCD vs. Healthy | FCD vs. nMCI | |
| Depression | 11.1 (11.4) | 3.4 (4.8) | 8.6 (8.3) | −1.13 (<0.01) | −0.38 (0.30) |
| Anxiety | 9.9 (10.5) | 3.1 (4.3) | 8 (6.7) | −1.11 (<0.01) | −0.14 (0.71) |
| Stress | 12.2 (9.9) | 5.2 (5.1) | 11 (8.0) | −0.88 (<0.01) | −0.0.17 (0.62) |
| Scale | Regression: Coefficient (p) | ||||
|---|---|---|---|---|---|
| FCD | H | nMCI | FCD vs. H | FCD vs. nMCI | |
| TMT-B 1 | Mean (SD) | ||||
| Time in seconds | 105 (74) | 75 (38) | 134 (82) | −0.40 (0.02) | −0.02 (0.92) |
| HVLT-R 2 | Raw score mean; t-score mean (SD) | ||||
| Total recall (trials 1-3) | 20.9; 37.3 (12.3) | 24.4; 45.7 (10.6) | 16.1; 33.7 (8.8) | 9.13 (<0.01) | −3.60 (0.31) |
| Trial 4 recall (delayed recall) | 7.4; 40.3 (14.0) | 9.5; 49.2 (10.0) | 3.8; 31.8 (10.1) | 8.86 (0.02) | −8.52 (0.03) |
| Retention (trial 4/best of trial 2 and trial 3) | 0.79; 43.1 (14.1) | 0.92; 50.0 (9.9) | 0.48; 32.8 (12.1) | 6.99 (0.07) | −10.34 (0.01) |
| Recognition discrimination index (recognition hits minus false positives) | 7.2; 36.4 (14.0) | 10.8; 50.5 (8.3) | 7.6; 34.9 (11.5) | 14.12 (<0.01) | −1.45 (0.71) |
| Mean (SD) | |||||
| D-prime 1 | 2.22 (1.58) | 3.68 (0.84) | 2.18 (1.12) | 12.62 (<0.01) | −0.30 (0.94) |
| Performance Validity Failure: n (Percent) | Personality Content Scales 5: t-Scores (SD) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| >15/338 items unscorable 1 | >1 scale >10% items unscorable 2 | Potentially random or fixed responding 3 | Over-report 1+ scale 4 | EID | RC1 | COG | INTRr | NEGEr | |
| FCD (n = 20) | 5 (25) | 8 (40) | 2 (10) | 11 (52) | 59.6 (13.4) | 70.6 (18.5) | 75.4 (15.2) | 61.2 (18.0) | 57.6 (15.4) |
| nMCI (n = 15) | 9 (60) | 9 (60) | 4 (27) | 6 (35) | 58.0 (8.6) | 66.6 (12.6) | 70.7 (12.8) | 60.2 (11.5) | 55.5 (13.2) |
| Healthy (n = 25) | 0 (0) | 1 (4) | 0 (0) | 4 (16) | 50.1 (11.7) | 57.2 (10.3) | 55.7 (13.7) | 55.8 (13.5) | 48.4 (9.91) |
| Group comparison: Chi 2 (p) | Group comparison: coefficient (p) | ||||||||
| FCD vs. nMCI | 4.4 (0.04) | 1.4 (0.24) | 1.7 (0.20) | 0.12 (0.73) | 1.67 (0.73) | 0.68 (0.91) | −3.30 (0.59) | 2.34 (0.71) | 1.57 (0.76) |
| FCD vs. Healthy | 7.0 (0.01) | 9.00 (<0.01) | 2.6 (0.11) | 9.4 (<0.01) | −10.16 (0.01) | −12.35 (0.01) | −21.08 (<0.01) | −3.98 (0.42) | −9.40 (0.03) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ball, H.A.; Swirski, M.; Newson, M.; Coulthard, E.J.; Pennington, C.M. Differentiating Functional Cognitive Disorder from Early Neurodegeneration: A Clinic-Based Study. Brain Sci. 2021, 11, 800. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060800
Ball HA, Swirski M, Newson M, Coulthard EJ, Pennington CM. Differentiating Functional Cognitive Disorder from Early Neurodegeneration: A Clinic-Based Study. Brain Sciences. 2021; 11(6):800. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060800
Chicago/Turabian StyleBall, Harriet A., Marta Swirski, Margaret Newson, Elizabeth J. Coulthard, and Catherine M. Pennington. 2021. "Differentiating Functional Cognitive Disorder from Early Neurodegeneration: A Clinic-Based Study" Brain Sciences 11, no. 6: 800. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060800