
Foam Rolling Elicits Neuronal Relaxation Patterns Distinct from Manual Massage: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
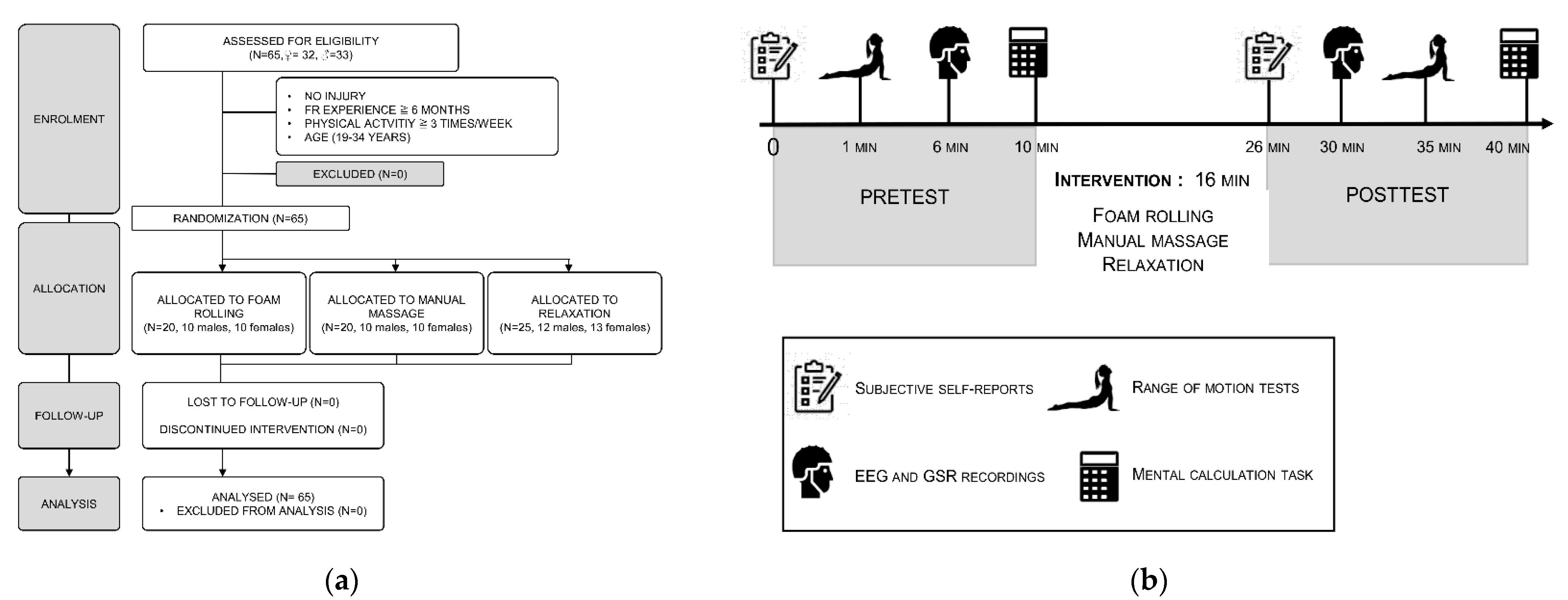
2.1. Participants
2.2. Experimental Design
2.2.1. Familiarization
2.2.2. Foam Rolling Intervention
2.2.3. Manual Massage Intervention
2.2.4. Relaxation Intervention
2.3. Dependent Variables
2.3.1. Self-Report Ratings on Likert-Type Scales
2.3.2. Motor and Cognitive Performances
2.3.3. Electroencephalography
2.3.4. Electrodermal Activity
3. Statistical Analysis
3.1. Power/Sample Size Considerations
3.2. Randomization
3.3. Data Analysis
4. Results
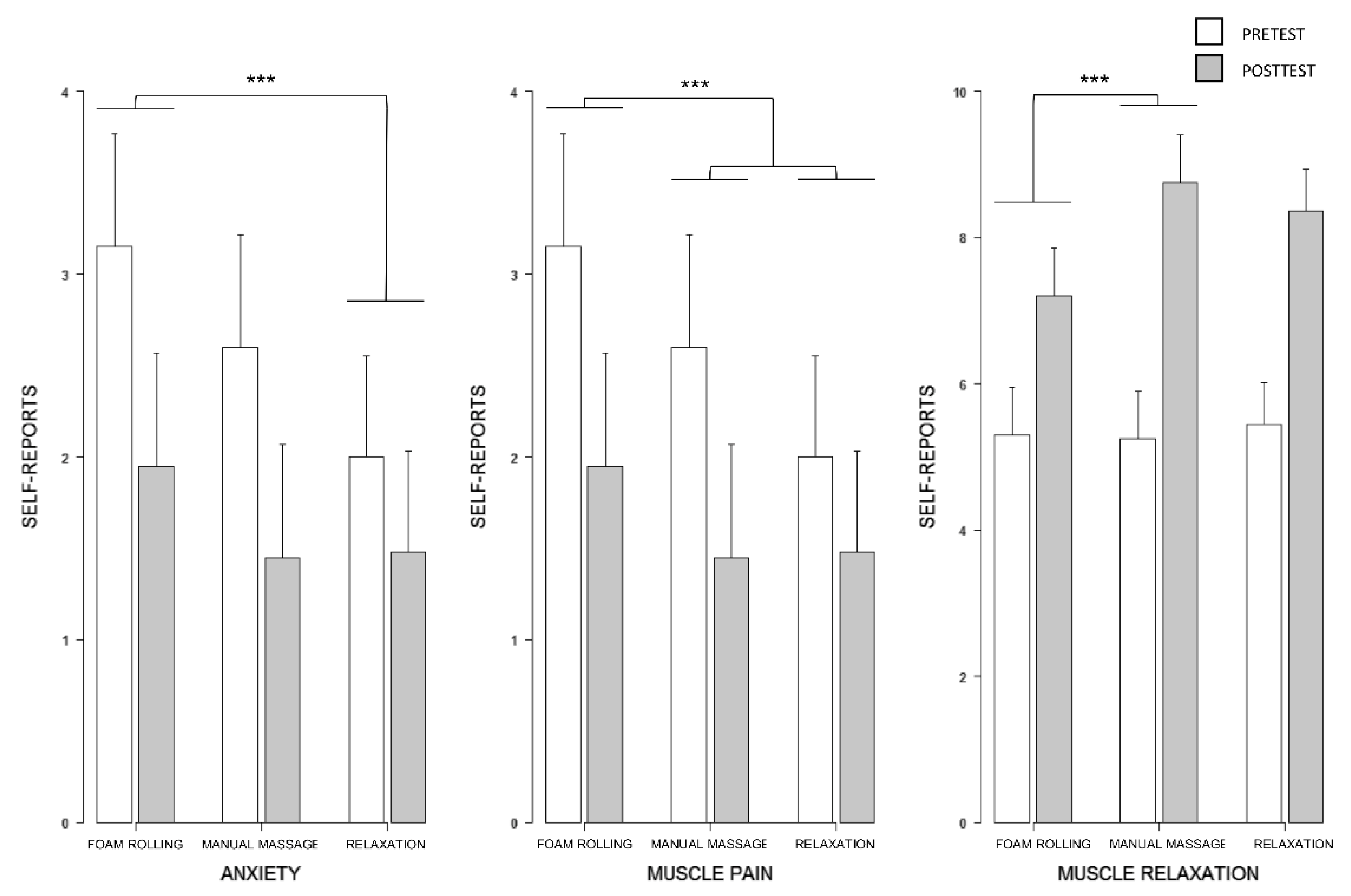
4.1. Change in Subjective Scores
4.1.1. Anxiety Ratings
4.1.2. Muscle Relaxation, Warmth, and Pain Ratings
4.2. Cognitive and Motor Performances
4.2.1. Mental Calculation
4.2.2. Sit-and-Reach Data
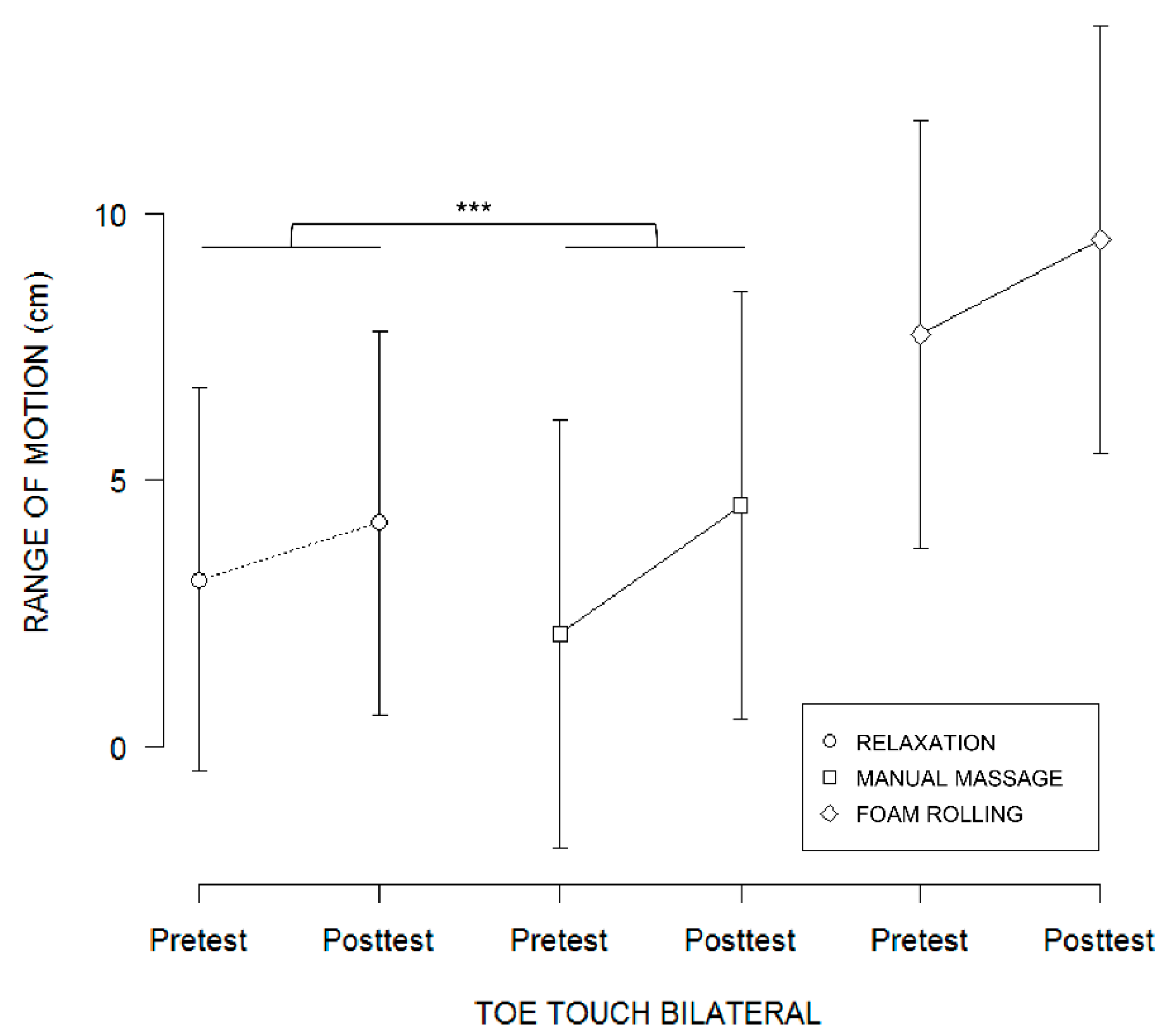
4.2.3. Toe-Touch Data
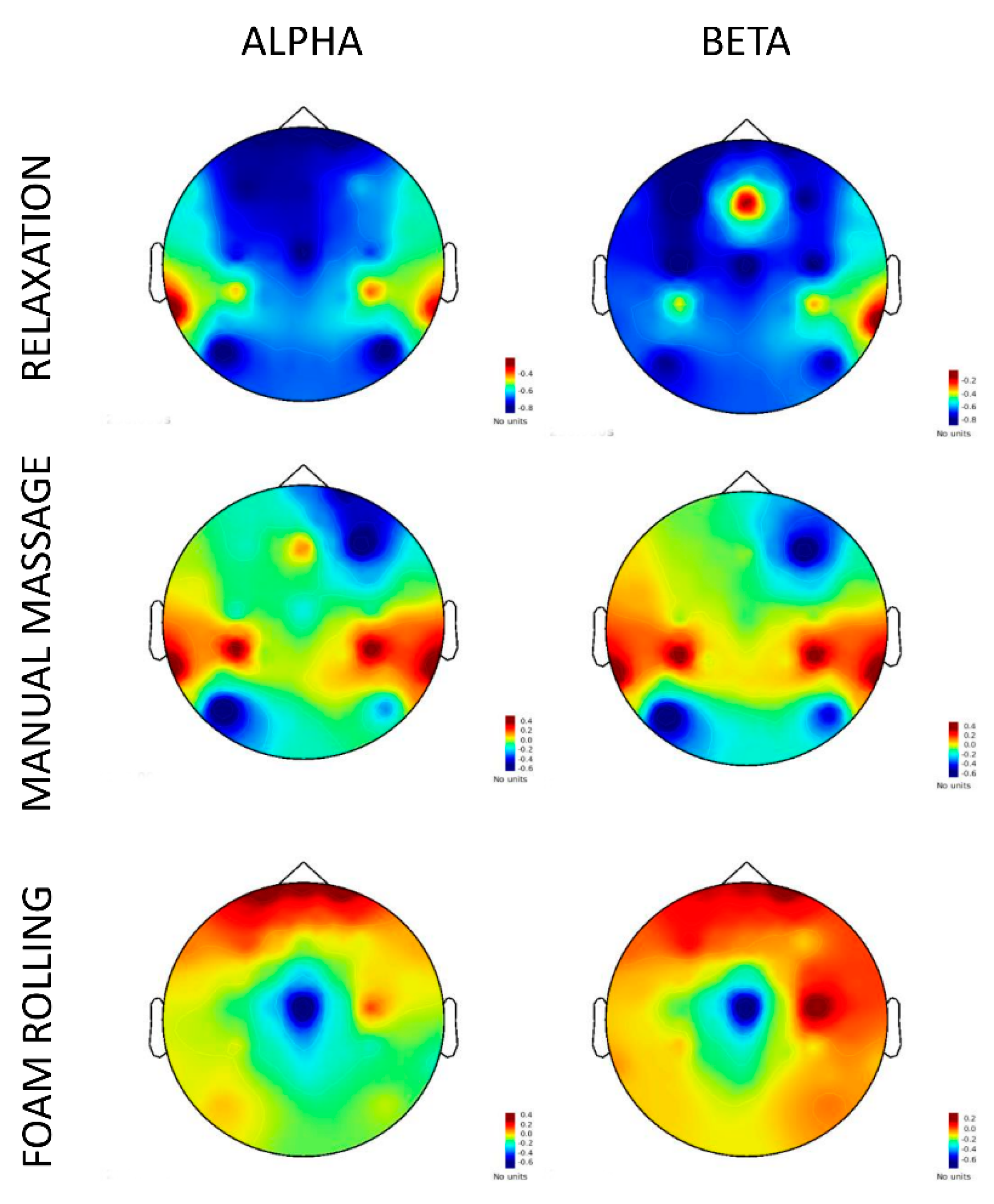
4.3. Neurophysiological Data
4.3.1. EEG Power Analysis
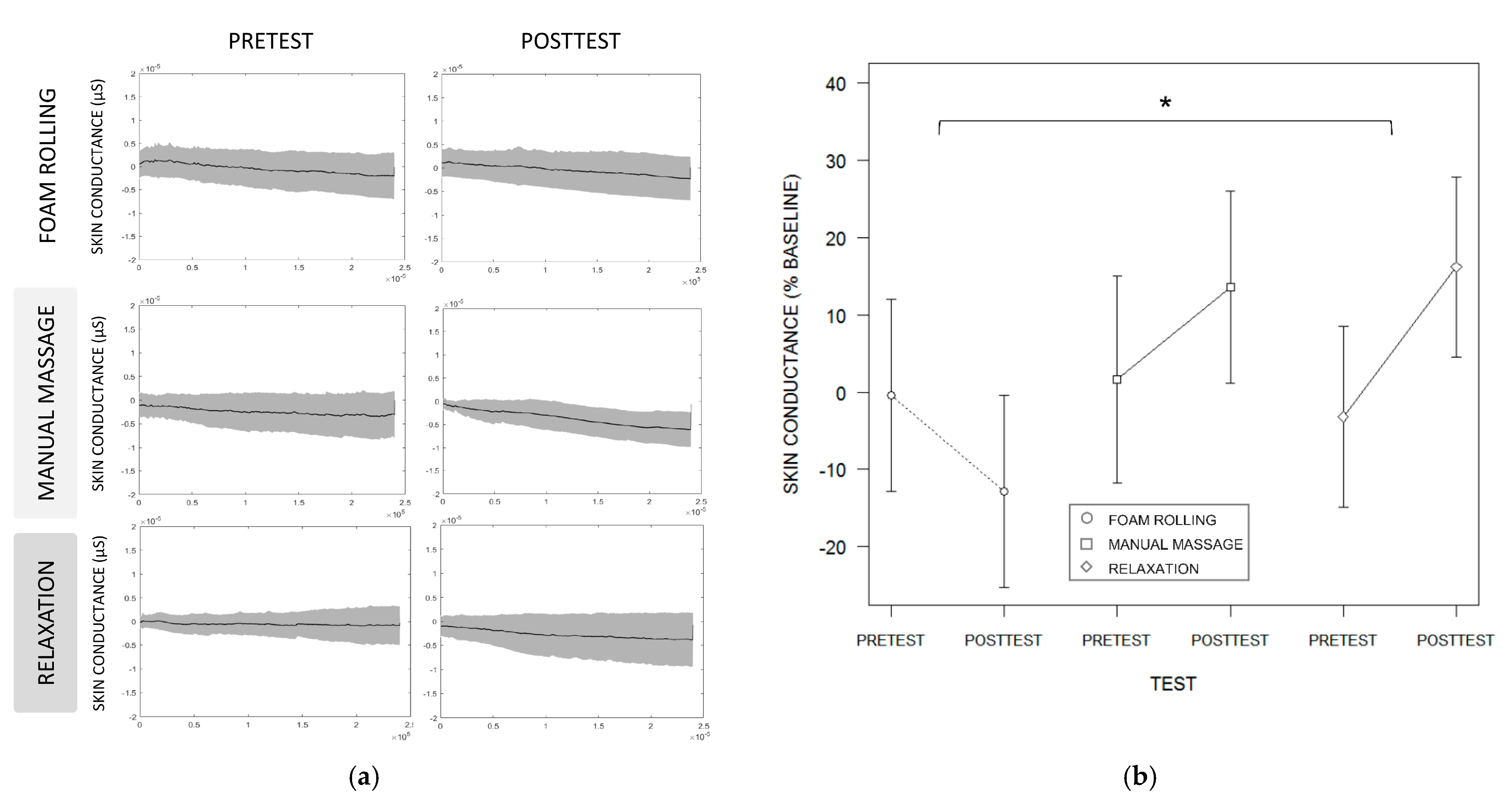
4.3.2. Skin Conductance
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guimberteau, J.C. Promenades Sous La Peau; Elsevier: Amsterdam, The Netherlands, 2004; ISBN 978–2-84299–649–9. [Google Scholar]
- Standley, R.A.; Miller, M.G.; Binkley, H. Massage’s Effect on Injury, Recovery, and Performance: A Review of Techniques and Treatment Parameters. Strength Cond. J. 2010, 32, 64–67. [Google Scholar] [CrossRef]
- Guimberteau, J.C.; Findley, T.W.; Kapandji, A.I.; Armstrong, C. L’architecture Du Corps Humain Vivant: Le Monde Extracellulaire, Les Cellules et Le Fascia Révélés Par l’endoscopie Intratissulaire; Ed Sully: Vannes, France, 2016; ISBN 978–2-35432–200–7. [Google Scholar]
- Estradère, J.D.J. Du Massage Son Historique, Ses Manipulations, Ses Effets Physiologiques et Thérapeutiques; Delahaye: Paris, France, 1863. [Google Scholar]
- Beck, M.F. Theory and Practice of Therapeutic Massage, 5th ed; Milady Publishing Compagny: Albany, NY, USA, 2010; ISBN 1–133–01086–5. [Google Scholar]
- Weerapong, P.; Hume, P.A.; Kolt, G.S. The Mechanisms of Massage and Effects on Performance, Muscle Recovery and Injury Prevention. Sports Med. 2005, 35, 235–256. [Google Scholar] [CrossRef] [PubMed]
- Kerautret, Y.; Di Rienzo, F.; Eyssautier, C.; Guillot, A. Selective Effects of Manual Massage and Foam Rolling on Perceived Recovery and Performance: Current Knowledge and Future Directions toward Robotic Massages. Front. Physiol. 2020, 11, 1567. [Google Scholar] [CrossRef] [PubMed]
- Freiwald, J.; Baumgart, C.; Kühnemann, M.; Hoppe, M.W. Foam-Rolling in Sport and Therapy–Potential Benefits and Risks: Part 1–Definitions, Anatomy, Physiology, and Biomechanics. Thema Konserv. Ther. Sportorthopädie 2016, 32, 258–266. [Google Scholar] [CrossRef]
- Guillot, A.; Kerautret, Y.; Queyrel, F.; Schobb, W.; Di Rienzo, F. Foam Rolling and Joint Distraction with Elastic Band Training Performed for 5–7 Weeks Respectively Improve Lower Limb Flexibility. J. Sports Sci. Med. 2019, 18, 160–171. [Google Scholar]
- Kerautret, Y.; Guillot, A.; Di Rienzo, F. Evaluating the Effects of Embedded Self-Massage Practice on Strength Performance: A Randomized Crossover Pilot Trial. PLoS ONE 2021, 16, e0248031. [Google Scholar] [CrossRef]
- Kerautret, Y.; Guillot, A.; Eyssautier, C.; Gibert, G.; Di Rienzo, F. Effects of Self-Myofascial Release Interventions with or without Sliding Pressure on Skin Temperature, Range of Motion and Perceived Well-Being: A Randomized Control Pilot Trial. BMC Sports Sci Med Rehabil. 2021, 13, 43. [Google Scholar] [CrossRef]
- Schleip, R. Fascial Plasticity–A New Neurobiological Explanation: Part 1. J. Bodyw. Mov. Ther. 2003, 7, 11–19. [Google Scholar] [CrossRef]
- Schleip, R. Fascial Plasticity–A New Neurobiological Explanation Part 2. J. Bodyw. Mov. Ther. 2003, 7, 104–116. [Google Scholar] [CrossRef]
- Wilke, J.; Müller, A.-L.; Giesche, F.; Power, G.; Ahmedi, H.; Behm, D.G. Acute Effects of Foam Rolling on Range of Motion in Healthy Adults: A Systematic Review with Multilevel Meta-Analysis. Sports Med. 2020, 50, 387–402. [Google Scholar] [CrossRef]
- Schleip, R.; Müller, D.G. Training Principles for Fascial Connective Tissues: Scientific Foundation and Suggested Practical Applications. J. Bodyw. Mov. Ther. 2013, 17, 103–115. [Google Scholar] [CrossRef]
- Kaur, P. Comparative Study of Myofascial Release Technique and Transverse Friction Massage with Thermotherapy in Cervical Trigger Points. Int. J. Sci. Res. 2019, 8, 75–76. [Google Scholar]
- Leivadi, S.; Hernandez-Reif, M.; Field, T.; O’Rourke, M.; D’Arienzo, S.; Lewis, D.; del Pino, N.; Schanberg, S.; Kuhn, C. Massage Therapy and Relaxation Effects on University Dance Students. J. Dance Med. Sci. 1999, 3, 108–112. [Google Scholar]
- Behm, D.G.; Wilke, J. Do Self-Myofascial Release Devices Release Myofascia? Rolling Mechanisms: A Narrative Review. Sports Med. 2019, 49, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Field, T.; Ironson, G.; Scafidi, F.; Nawrocki, T.; Goncalves, A.; Burman, I.; Pickens, J.; Fox, N.; Schanberg, S.; Kuhn, C. Massage Therapy Reduces Anxiety and Enhances Eeg Pattern of Alertness and Math Computations. Int. J. Neurosci. 1996, 86, 197–205. [Google Scholar] [CrossRef]
- Field, T.; Hernande-Reif, M.; Diego, M.; Schanberg, S.; Kuhn, C. Cortisol Decreases and Serotonin and Dopamine Increase Following Massage Therapy. Int. J. Neurosci. 2005, 115, 1397–1413. [Google Scholar] [CrossRef]
- Wu, J.-J.; Cui, Y.; Yang, Y.-S.; Kang, M.-S.; Jung, S.-C.; Park, H.K.; Yeun, H.-Y.; Jang, W.J.; Lee, S.; Kwak, Y.S.; et al. Modulatory Effects of Aromatherapy Massage Intervention on Electroencephalogram, Psychological Assessments, Salivary Cortisol and Plasma Brain-Derived Neurotrophic Factor. Complement. Ther. Med. 2014, 22, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diego, M.A.; Field, T. Moderate Pressure Massage Elicits a Parasympathetic Nervous System Response. Int. J. Neurosci. 2009, 119, 630–638. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Park, B.N.R.; Kim, S.H. The Effects of Heat and Massage Application on Autonomic Nervous System. Yonsei Med. J. 2011, 52, 982–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, T. Massage Therapy Research Review. Complement. Ther. Clin. Pract. 2014, 20, 224–229. [Google Scholar] [CrossRef] [Green Version]
- Lastova, K.; Nordvall, M.; Walters-Edwards, M.; Allnutt, A.; Wong, A. Cardiac Autonomic and Blood Pressure Responses to an Acute Foam Rolling Session. J. Strength Cond. Res. 2018, 32, 2825–2830. [Google Scholar] [CrossRef]
- Jodo, E.; Yamada, Y.; Hatayama, T.; Abe, T.; Kinya, M. Effects of Facial Massage on the Spontaneous EEG. Tohoku Psychol. Folia 1988, 47, 8–15. [Google Scholar]
- Nakano, H.; Kodama, T.; Ueda, T.; Mori, I.; Tani, T.; Murata, S. Effect of Hand and Foot Massage Therapy on Psychological Factors and EEG Activity in Elderly People Requiring Long-Term Care: A Randomized Cross-over Study. Brain Sci. 2019, 9, 54. [Google Scholar] [CrossRef] [Green Version]
- Diego, M.A.; Field, T.; Sanders, C.; Hernandez-Reif, M. Massage therapy of moderate and light pressure and vibrator effects on eeg and heart rate. Int. J. Neurosci. 2004, 114, 31–44. [Google Scholar] [CrossRef]
- Kaewcum, N.; Siripornpanich, V. The Effects of Unilateral Swedish Massage on the Neural Activities Measured by Quantitative Electroencephalography (EEG). J. Health Res. 2018, 32, 36–46. [Google Scholar] [CrossRef]
- Krause, F.; Wilke, J.; Niederer, D.; Vogt, L.; Banzer, W. Acute Effects of Foam Rolling on Passive Stiffness, Stretch Sensation and Fascial Sliding: A Randomized Controlled Trial. Hum. Mov. Sci. 2019, 67, 102514. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomized Trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cometta, M.; Falquet, B. L’efficacité de l’utilisation Du Foam Roller Sur l’extensibilité Musculaire Des. Ischio-Jambiers; Haute Ecole de Santé Valais: Leukerbad, Switzerland, 2018. [Google Scholar]
- Cheatham, S.W.; Baker, R. Differences in Pressure Pain Threshold among Men and Women after Foam Rolling. J. Bodyw. Mov. Ther. 2017, 21, 978–982. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kolber, M.J. Does Roller Massage with a Foam Roll Change Pressure Pain Threshold of the Ipsilateral Lower Extremity Antagonist and Contralateral Muscle Groups? An Exploratory Study. J. Sport Rehabil. 2018, 27, 165–169. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Stull, K.R. Comparison of Three Different Density Type Foam Rollers on Knee Range of Motion and Pressure Pain Threshold: A Randomized Controlled Trial. Int. J. Sports Phys. Ther. 2018, 13, 474–482. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Stull, K.R. Comparison of a Foam Rolling Session with Active Joint Motion and without Joint Motion: A Randomized Controlled Trial. J. Bodyw. Mov. Ther. 2018, 22, 707–712. [Google Scholar] [CrossRef]
- Schultz, J.H.; Luthe, W. Autogenic Training: A Psychophysiologic Approach to Psychotherapy; Autogenic Training: A Psychophysiologic Approach to Psychotherapy; Grune & Stratton: Oxford, UK, 1959; p. 289. [Google Scholar]
- Ayala, F.; Sainz de Baranda, P.; De Ste Croix, M.; Santonja, F. Reproducibility and Criterion-Related Validity of the Sit and Reach Test and Toe Touch Test for Estimating Hamstring Flexibility in Recreationally Active Young Adults. Phys. Ther. Sport 2012, 13, 219–226. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Merino-Marban, R.; Viciana, J. Criterion-Related Validity of Sit-and-Reach Tests for Estimating Hamstring and Lumbar Extensibility: A Meta-Analysis. J. Sports Sci. Med. 2014, 13, 1–14. [Google Scholar] [PubMed]
- Chung, P.-K.; Yuen, C.-K. Criterion-Related Validity of Sit-and-Reach Tests in University Men in Hong Kong. Percept. Mot. Skills 1999, 88, 304–316. [Google Scholar] [CrossRef] [PubMed]
- Diego, M.A.; Jones, N.A.; Field, T.; Hernandez-reif, M.; Schanberg, S.; Kuhn, C.; Galamaga, M.; McAdam, V.; Galamaga, R. Aromatherapy Positively Affects Mood, EEG Patterns of Alertness and Math Computations. Int. J. Neurosci. 1998, 96, 217–224. [Google Scholar] [CrossRef]
- Field, T.; Diego, M.; Hernandez-Reif, M. Tai Chi/Yoga Effects on Anxiety, Heartrate, EEG and Math Computations. Complement. Ther. Clin. Pract. 2010, 16, 235–238. [Google Scholar] [CrossRef] [Green Version]
- Caviola, S.; Carey, E.; Mammarella, I.C.; Szucs, D. Stress, Time Pressure, Strategy Selection and Math Anxiety in Mathematics: A Review of the Literature. Front. Psychol. 2017, 8, 1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadel, F.; Baillet, S.; Mosher, J.C.; Pantazis, D.; Leahy, R.M. Brainstorm: A User-Friendly Application for MEG/EEG Analysis. Comput. Intell. Neurosci. 2011, 2011, 879716. [Google Scholar] [CrossRef]
- Kilavik, B.E.; Zaepffel, M.; Brovelli, A.; MacKay, W.A.; Riehle, A. The Ups and Downs of Beta Oscillations in Sensorimotor Cortex. Spec. Issue Neuronal Oscil. Mov. Disord. 2013, 245, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Babiloni, C.; Del Percio, C.; Arendt-Nielsen, L.; Soricelli, A.; Romani, G.L.; Rossini, P.M.; Capotosto, P. Cortical EEG Alpha Rhythms Reflect Task-Specific Somatosensory and Motor Interactions in Humans. Clin. Neurophysiol. 2014, 125, 1936–1945. [Google Scholar] [CrossRef] [PubMed]
- Pfurtscheller, G. EEG Event-Related Desynchronization (ERD) and Synchronization (ERS). Electroencephalogr. Clin. Neurophysiol. 1997, 1, 26. [Google Scholar] [CrossRef]
- Pfurtscheller, G.; Lopes da Silva, F.H. Event-Related EEG/MEG Synchronization and Desynchronization: Basic Principles. Clin. Neurophysiol. 1999, 110, 1842–1857. [Google Scholar] [CrossRef]
- Collet, C.; Salvia, E.; Petit-Boulanger, C. Measuring Workload with Electrodermal Activity during Common Braking Actions. Ergonomics 2014, 57, 886–896. [Google Scholar] [CrossRef] [PubMed]
- Bellemare, C.; Bissonnette, L.; Kröger, S. Statistical Power of within and Between-Subjects Designs in Economic Experiments. SSRN Scholarly Paper. 2014. [Google Scholar] [CrossRef] [Green Version]
- Bradbury-Squires, D.J.; Noftall, J.C.; Sullivan, K.M.; Behm, D.G.; Power, K.E.; Button, D.C. Roller-Massager Application to the Quadriceps and Knee-Joint Range of Motion and Neuromuscular Efficiency during a Lunge. J. Athl. Train. 2015, 50, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Fairall, R.R.; Cabell, L.; Boergers, R.J.; Battaglia, F. Acute Effects of Self-Myofascial Release and Stretching in Overhead Athletes with GIRD. J. Bodyw. Mov. Ther. 2017, 21, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Grabow, L.; Young, J.D.; Byrne, J.M.; Granacher, U.; Behm, D.G. Unilateral Rolling of the Foot Did Not Affect Non-Local Range of Motion or Balance. J. Sports Sci. Med. 2017, 16, 209–218. [Google Scholar]
- Champely, S.; Ekstrom, C.; Dalgaard, P.; Gill, J.; Weibelzahl, S.; Anandkumar, A.; Ford, C.; Volcic, R.; De Rosario, H.; De Rosario, M.H. Package ‘Pwr.’ R Package Version 1.3-0. 2018. Available online: http://cran.r-project.org/package=pwr (accessed on 18 June 2021).
- Suresh, K. An Overview of Randomization Techniques: An Unbiased Assessment of Outcome in Clinical Research. J. Hum. Reprod. Sci. 2011, 4, 8. [Google Scholar] [CrossRef]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D. Nlme: Linear and Nonlinear Mixed Effects Models, R Package Version 3; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Ben-Shachar, M.; Makowski, D.; Lüdecke, D. Compute and Interpret Indices of Effect Size. CRAN Online Ser. 2020. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Warrenburg, S.; Pagano, R.R.; Woods, M.; Hlastala, M. A Comparison of Somatic Relaxation and EEG Activity in Classical Progressive Relaxation and Transcendental Meditation. J. Behav. Med. 1980, 3, 73–93. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, G.D.; Benson, H.; Friedman, R. Topographic EEG Mapping of the Relaxation Response. Biofeedback Self-Regul. 1996, 21, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Rizzolatti, G.; Fogassi, L.; Gallese, V. Motor and Cognitive Functions of the Ventral Premotor Cortex. Curr. Opin. Neurobiol. 2002, 12, 149–154. [Google Scholar] [CrossRef]
- Ouchi, Y.; Kanno, T.; Okada, H.; Yoshikawa, E.; Shinke, T.; Nagasawa, S.; Minoda, K.; Doi, H. Changes in Cerebral Blood Flow under the Prone Condition with and without Massage. Neurosci. Lett. 2006, 407, 131–135. [Google Scholar] [CrossRef]
- Kodama, K.; Takamoto, K.; Nishimaru, H.; Matsumoto, J.; Takamura, Y.; Sakai, S.; Ono, T.; Nishijo, H. Analgesic Effects of Compression at Trigger Points Are Associated with Reduction of Frontal Polar Cortical Activity as Well as Functional Connectivity between the Frontal Polar Area and Insula in Patients with Chronic Low Back Pain: A Randomized Trial. Front. Syst. Neurosci. 2019, 13, 68. [Google Scholar] [CrossRef]
- Gómez-Ramírez, J.; Freedman, S.; Mateos, D.; Pérez Velázquez, J.L.; Valiante, T.A. Exploring the Alpha Desynchronization Hypothesis in Resting State Networks with Intracranial Electroencephalography and Wiring Cost Estimates. Sci. Rep. 2017, 7, 15670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehrer, P.M.; Carr, R.; Sargunaraj, D.; Woolfolk, R.L. Stress Management Techniques: Are They All Equivalent, or Do They Have Specific Effects? Biofeedback Self-Regul. 1994, 19, 353–401. [Google Scholar] [CrossRef]
- Blizard, D.A.; Cowings, P.; Miller, N.E. Visceral Responses to Opposite Types of Autogenic-Training Imagery. Biol. Psychol. 1975, 3, 49–55. [Google Scholar] [CrossRef]
- Mohammadi Ziabari, S.S.; Treur, J. Cognitive Modeling of Mindfulness Therapy by Autogenic Training. In Proceedings of the Information Systems Design and Intelligent Applications; Satapathy, S.C., Bhateja, V., Somanah, R., Yang, X.-S., Senkerik, R., Eds.; Springer: Singapore, 2019; pp. 53–66. [Google Scholar]
- Mulder, T.; de Vries, S.; Zijlstra, S. Observation, Imagination and Execution of an Effortful Movement: More Evidence for a Central Explanation of Motor Imagery. Exp. Brain Res. 2005, 163, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Ajimsha, M.S.; Majeed, N.A.; Chinnavan, E.; Thulasyammal, R.P. Effectiveness of Autogenic Training in Improving Motor Performances in Parkinson’s Disease. Complement. Ther. Med. 2014, 22, 419–425. [Google Scholar] [CrossRef]
- Lehrer, P.M.; Woolfolk, R.L.; Sime, W.E. Principles and Practice of Stress Management, Third Edition; Guilford Press: New York, NY, USA, 2007; ISBN 978-1-60623–828–8. [Google Scholar]
- Leonova, A.B.; Kuznetsova, A.S.; Barabanshchikova, V.V. Job Specificity in Human Functional State Optimization by Means of Self-Regulation Training. Procedia-Soc. Behav. Sci. 2013, 86, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Arabaci, R. Acute Effects of Pre-Event Lower Limb Massage on Explosive and High Speed Motor Capacities and Flexibility. J. Sports Sci. Med. 2008, 7, 549–555. [Google Scholar] [PubMed]
- Arazi, H.; Asadi, A.; Hoseini, K. Comparison of Two Different Warm-Ups (Static-Stretching and Massage): Effects on Flexibility and Explosive Power. Acta Kinesiol. 2012, 6, 55–59. [Google Scholar]
- Kanthack, T.F.D.; Guillot, A.; Papaxanthis, C.; Guizard, T.; Collet, C.; Di Rienzo, F. Neurophysiological Insights on Flexibility Improvements through Motor Imagery. Behav. Brain Res. 2017, 331, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Eriksson Crommert, M.; Lacourpaille, L.; Heales, L.J.; Tucker, K.; Hug, F. Massage Induces an Immediate, Albeit Short-Term, Reduction in Muscle Stiffness. Scand. J. Med. Sci. Sports 2015, 25, e490–e496. [Google Scholar] [CrossRef]
- Moraska, A. Therapist Education Impacts the Massage Effect on Postrace Muscle Recovery. Med. Sci. Sports Exerc. 2007, 39, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Sharp, C.; Coltharp, H.; Hurford, D.; Cole, A. Increasing Mathematical Problem-Solving Performance through Relaxation Training. Math. Educ. Res. J. 2000, 12, 53–61. [Google Scholar] [CrossRef]
- Mazzeo, C.A. Nurturing the Mind/Body Connection: A Phenomenological Analysis of Emotional Release in Massage Therapy; Proquest Umi Dissertation Publishing: Chicago, IL, USA, 2011; ISBN 978-1-243–45223–8. [Google Scholar]
- Eliska, O.; Eliskova, M. Are Peripheral Lymphatics Damaged by High Pressure Manual Massage? Lymphology 1995, 28, 21–30. [Google Scholar]
- Freiwald, J.; Baumgart, C.; Kühnemann, M.; Hoppe, M.W. Foam-Rolling in Sport and Therapy–Potential Benefits and Risks: Part 2–Positive and Adverse Effects on Athletic Performance. Thema Konserv. Ther. Sportorthopädie 2016, 32, 267–275. [Google Scholar] [CrossRef]
- Wiech, K.; Tracey, I. Pain, Decisions, and Actions: A Motivational Perspective. Front. Neurosci. 2013, 7, 46. [Google Scholar] [CrossRef] [Green Version]
- Bigliassi, M. Corollary Discharges and Fatigue-Related Symptoms: The Role of Attentional Focus. Front. Psychol. 2015, 6, 1002. [Google Scholar] [CrossRef] [Green Version]
- Kaada, B.; Torsteinb, O. Increase of Plasma β-Endorphins in Connective Tissue Massage. Gen. Pharmacol. Vasc. Syst. 1989, 20, 487–489. [Google Scholar] [CrossRef]
- Arroyo-Morales, M.; Olea, N.; Martínez, M.M.; Hidalgo-Lozano, A.; Ruiz-Rodríguez, C.; Díaz-Rodríguez, L. Psychophysiological Effects of Massage-Myofascial Release after Exercise: A Randomized Sham-Control Study. J. Altern. Complement. Med. 2008, 14, 1223–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalichman, L.; Ben David, C. Effect of Self-Myofascial Release on Myofascial Pain, Muscle Flexibility, and Strength: A Narrative Review. J. Bodyw. Mov. Ther. 2017, 21, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Field, T.; Diego, M.; Hernandez-Reif, M. Massage Therapy Research. Dev. Rev. 2007, 27, 75–89. [Google Scholar] [CrossRef]
- Buttagat, V.; Eungpinichpong, W.; Kaber, D.; Chatchawan, U.; Arayawichanon, P. Acute Effects of Traditional Thai Massage on Electroencephalogram in Patients with Scapulocostal Syndrome. Complement. Ther. Med. 2012, 20, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Von Mohr, M.; Crowley, M.J.; Walthall, J.; Mayes, L.C.; Pelphrey, K.A.; Rutherford, H.J.V. EEG Captures Affective Touch: CT-Optimal Touch and Neural Oscillations. Cogn. Affect. Behav. Neurosci. 2018, 18, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.N.; Best, T.M. Is Self Myofascial Release an Effective Preexercise and Recovery Strategy? A Literature Review. Curr. Sports Med. Rep. 2015, 14, 200–208. [Google Scholar] [CrossRef]
- Wiewelhove, T.; Döweling, A.; Schneider, C.; Hottenrott, L.; Meyer, T.; Kellmann, M.; Pfeiffer, M.; Ferrauti, A. A Meta-Analysis of the Effects of Foam Rolling on Performance and Recovery. Front. Physiol. 2019, 10, 376. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Age (years) | Height (m) | Mass (kg) | BMI (kg/m2) |
|---|---|---|---|---|
| Relaxation | 25.9 ± 3.2 | 1.71 ± 10.5 | 67.3 ± 11.1 | 23 ± 2.3 |
| (range 20–34) | (range 1.53–1.91) | (range 48–98) | (range 19.8–28.8) | |
| Foam Rolling | 26.1 ± 3.1 | 1.73 ± 7 | 70.9 ± 10.4 | 23.6 ± 2.4 |
| (range 19–31) | (range 1.62–1.83) | (range 53–90) | (range 19.5–30.1) | |
| Manual Massage | 24.8 ± 3 | 1.72 ± 12.3 | 70.3 ± 13.4 | 23.6 ± 2.6 |
| (range 20–32) | (range 1.53–1.97) | (range 51–95) | (range 19–27.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerautret, Y.; Guillot, A.; Daligault, S.; Di Rienzo, F. Foam Rolling Elicits Neuronal Relaxation Patterns Distinct from Manual Massage: A Randomized Controlled Trial. Brain Sci. 2021, 11, 818. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060818
Kerautret Y, Guillot A, Daligault S, Di Rienzo F. Foam Rolling Elicits Neuronal Relaxation Patterns Distinct from Manual Massage: A Randomized Controlled Trial. Brain Sciences. 2021; 11(6):818. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060818
Chicago/Turabian StyleKerautret, Yann, Aymeric Guillot, Sébastien Daligault, and Franck Di Rienzo. 2021. "Foam Rolling Elicits Neuronal Relaxation Patterns Distinct from Manual Massage: A Randomized Controlled Trial" Brain Sciences 11, no. 6: 818. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060818