1. Introduction
The general confinement from the COVID-19 pandemic and the consequent school closure, interruption of contacts with family members and friends, as well as reduced social and leisure activities, has brought unparalleled modifications to the lifestyle of children and adolescents, with important repercussions on their mental state and behaviors [
1].
In particular, COVID-19 lockdown resulted in important changes in sleep habits and sleep disorders in a large portion of the world’s population of all ages [
2,
3,
4,
5,
6]. The increase in sleep difficulties was often associated with higher levels of psychopathological symptoms or decreased quality of life [
3,
7,
8].
In face of a great amount of literature on the young and adult general population, only a few studies were conducted on sleep patterns or disturbances of the clinical population, especially children and adolescents with autism spectrum disorder (ASD) [
9] and attention-deficit/hyperactivity and impulsive disorders (ADHD) [
10], despite their frequent sleep disturbances and altered sleep patterns, independently by COVID-19 [
11]. Since sleep patterns significantly changed during the lockdown in typically developing children and adolescents [
2,
5,
6,
12], similar or even worse changes in subjects with ADHD and ASD could be expected. Several studies [
9,
10,
13,
14,
15,
16,
17] reported a high percentage of patients with ASD or ADHD that changed their sleep with a significant worsening of sleep quality and disturbances during the lockdown. Specifically, ASD children showed significant worsening of sleep disturbances, sleep duration, and sleep quality [
14,
15] and an increase in bedtime resistance, delay in falling asleep, and night awakenings [
17]. Children with ADHD showed an alteration of sleep patterns in 85% of cases [
16] and, unlike their healthy peers in the control group that experienced an increase in school night sleep duration, they did not benefit from the COVID-19 lockdown [
13].
Significant changes in sleep habits and disturbances in children with ADHD or ASD and adolescents during the lockdown have been reported by other studies. Since ADHD and ASD are two neurodevelopmental disorders with different symptoms, we could have expected that sleep changes would reflect specific clinical traits characterizing these two populations. To the best of our knowledge, no study has compared these two disorders for their sleep patterns and disturbances during the COVID-19 lockdown, thus, the aim of this study was to evaluate the different responses of these two clinical conditions in terms of sleep patterns and sleep disturbances.
2. Materials and Methods
2.1. Participants
Parents of Italian children and adolescents completed an online survey, advertised via social media, for a limited time window (from 7th May to 15th June 2020), targeting children aged 4 to 18 years. ASD and ADHD children and adolescents had been diagnosed by a child and adolescent psychiatrist of the Child and Adolescent Mental Health Services, before the survey, and were being followed at the same center. The survey was developed and conducted following the guidelines set by the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) [
18]. From a total of 5825 respondents, we identified ADHD and ASD patients and selected randomly a sample of typically developing subjects matched for age and sex with the clinical groups.
In total, 100 ASD (16 females, 16% and 84 males, 84%), 236 ADHD patients (44 females, 18.6% and 192 males, 81.4%), and 340 controls (58 female, 17.1% and 282 males, 82.9%) were enrolled in the analysis.
In Italy, the COVID-19 lockdown started on March 2020 with important restrictions that included school closure, limited activities for businesses and factories, and movement restrictions. The strict lockdown in Italy lasted for almost three months, with the progressive reopening of several activities in mid-June 2020. Italian schools reopened in September 2020, with some limitations.
There was no monetary or credit compensation for participating in the study. The study protocol was approved by the Ethics Committee of the Department of Developmental and Social Psychology of the Sapienza University of Rome and was conducted in accordance with the Declaration of Helsinki.
2.2. Measures
A specific questionnaire was arranged for the survey. The first section was devoted to the collection of demographic data (age, gender, caregiver education, region of Italy). A second section was organized to gather information on sleep arrangement and schedule during weekdays and during weekends (bedtime, risetime, sleep latency, sleep duration, co-sleeping). All these questions were asked in order to evaluate differences between before and during the lockdown period. A third section of the survey was related to family composition, work of parents during the lockdown, online lessons for children and adolescents, screen exposure time (excluding the hours for lessons), use of over-the-counter or prescription drugs for sleep. Caregivers completed a modified version of the Sleep Disturbance Scale for Children (SDSC) [
19].
Retrospective questions were used to estimate perceived changes across two time periods: from “before the lockdown” (i.e., in the last month before the outbreak) to “during the lockdown” (i.e., in the seven days prior to filling out the survey).
The SDSC was originally validated on a sample of 6- to 16-year-old healthy children from the general population [
19] but was also used for younger children [
20,
21]. We grouped questions related to sleep-disordered breathing into one question and selected, in total, 13 items in order to facilitate the compilation by parents.
2.3. Data Analysis
Descriptive statistics were applied to characterize sociodemographic variables, sleep patterns, and sleep disturbances. Data were reported as frequencies and percentages for comparisons between the groups. The McNemar’s test was performed to compare sleep patterns and sleep disturbances before and during the lockdown. “Before-during” bedtime and risetime were recorded within three categories based if maintained, delayed, or anticipated and sleep duration if maintained, increased, or reduced. Chi-square tests were conducted to compare changes in sleep patterns, sleep schedule, and sleep disturbances before and during lockdown, within and between the groups. Fisher’s exact test was applied when appropriate.
For all comparisons, p-values less than 0.05 were considered to be statistically significant. Statistical analyses were performed using the SPSS software release 17.0 (SPSS INC, Chicago, IL, USA).
4. Discussion
The lockdown experience significantly impacted sleep patterns and disturbances of children and adolescents with ADHD and ASD, as well as of controls. As also indicated by other studies [
5,
6,
12], sleep is one of the more impaired domains during the COVID-19 lockdown, independently by mental health condition and age and it is known that sleep problems in ASD and ADHD patients may worsen daytime behavior and functioning, as well as increase parental distress [
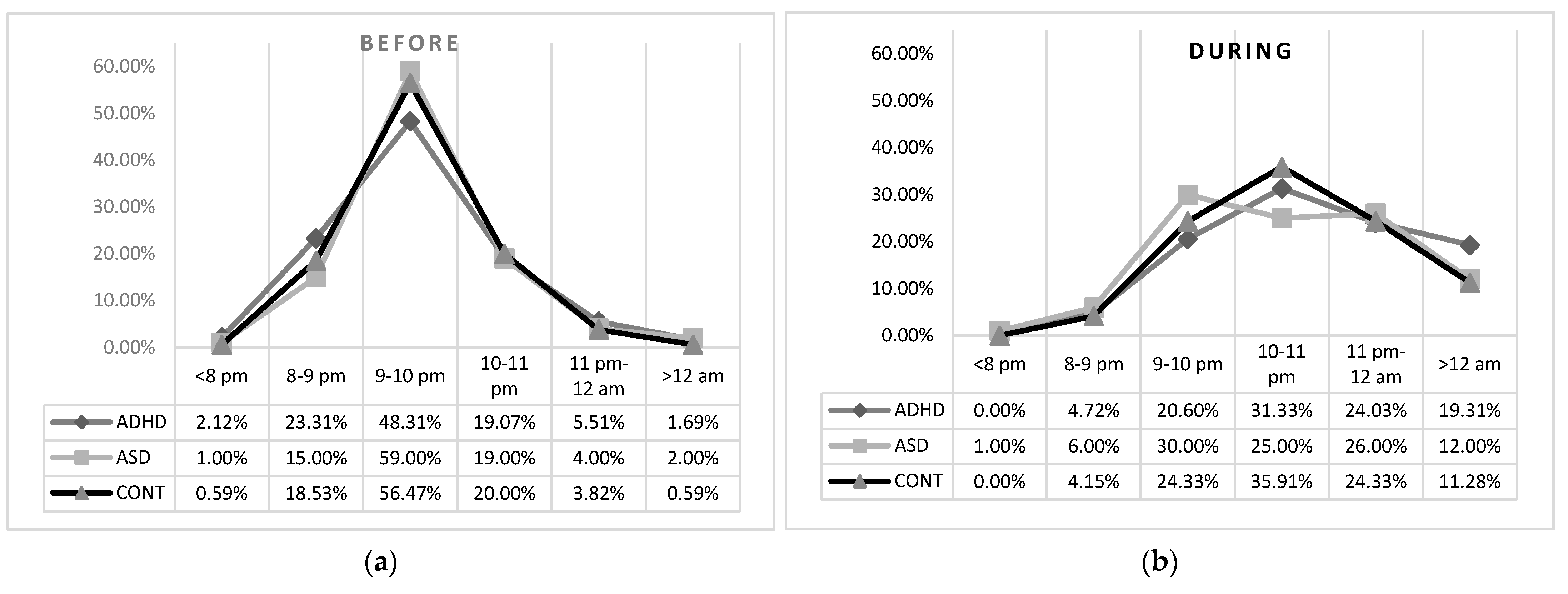
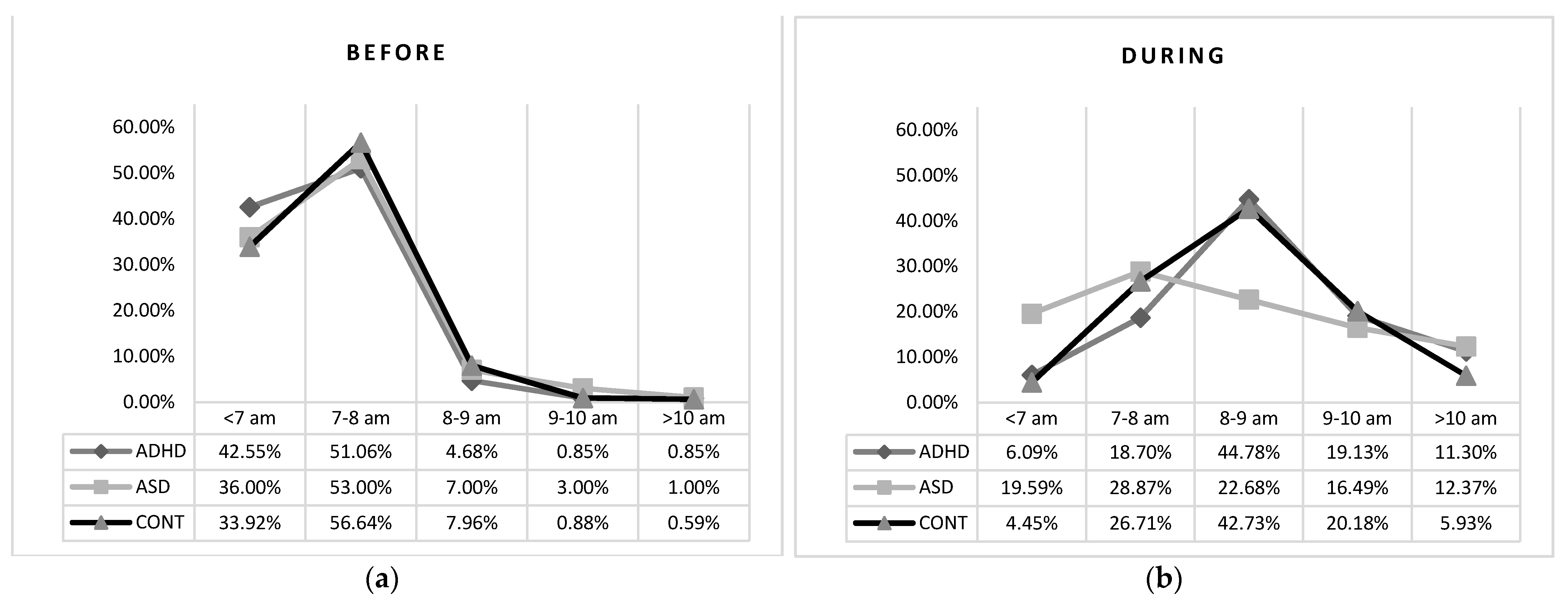
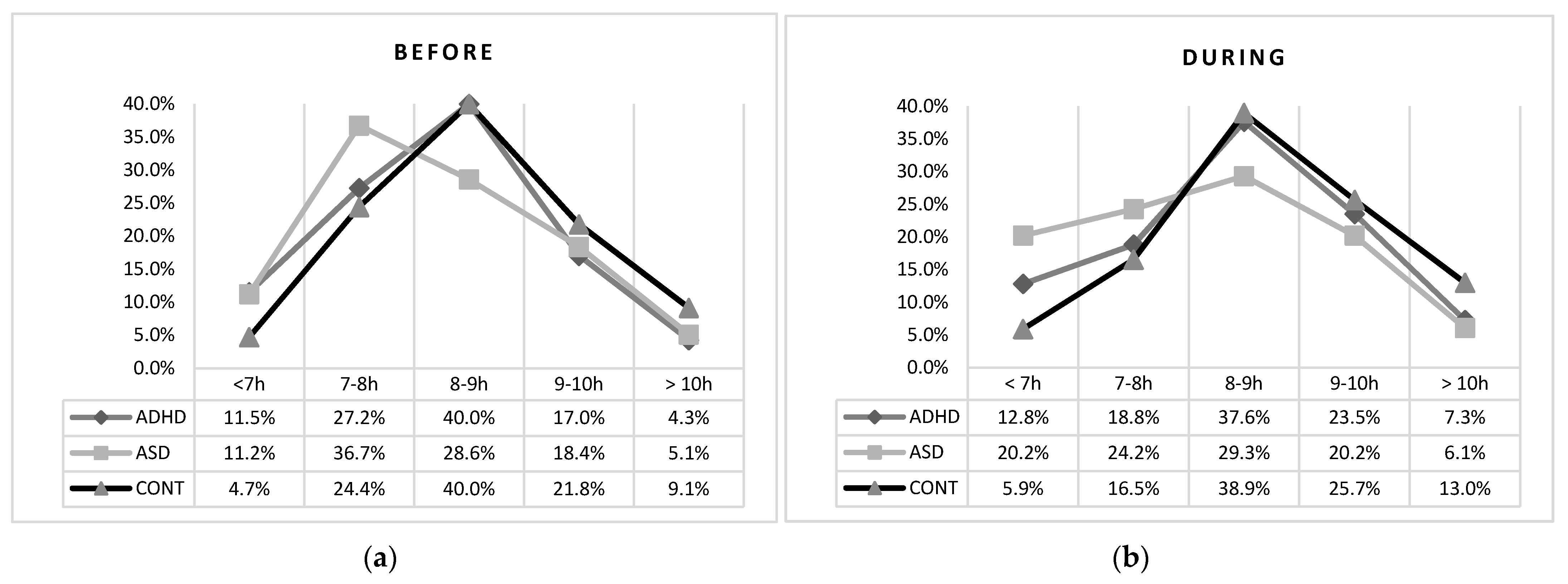
11]. We found, in both clinical groups, a higher percentage of subjects that reported a reduced sleep duration and an increased sleep latency than controls. ASD patients showed less changes in weekday-weekend risetime than both ADHD and controls, while children with ADHD reported higher delays in bedtime than the other groups. Our findings are supported by specific studies on these two clinical groups and controls [
2,
16], reporting delayed bedtime in children with ADHD [
10,
17] and a reduced sleep duration in both ADHD and ASD [
9,
10,
13,
15,
22].
Although changes of lifestyle caused by the lockdown affected both clinical groups and controls, generally children and adolescents with ADHD showed greater instability of their sleep schedule and increased delay in weekday sleep schedule, when compared to ASD and controls, during lockdown. This finding, according to the night-to-night variability in the sleep–wake patterns reported by several comparative studies in children with ADHD compared to typically developing children [
23,
24,
25], supports the consideration that the “variability” of sleep patterns, represents a distinctive marker of the ADHD condition.
Since ADHD patients’ functioning is strongly dependent on environmental changes, in agreement with other studies [
10,
26], our findings confirm that sudden lifestyle changes caused by the pandemic lockdown impacted the sleep and behavior of ADHD patients more than on those of ASD patients or controls. Conversely, children and adolescents with ASD seemed to be less vulnerable to the effects of prolonged isolation, showing a higher stability in bedtime and risetime than both ADHD and controls, probably linked to the stereotyped and fixed behavior of these children, since inflexibility and insistence on sameness are hallmark characteristics of ASD [
15].
The significantly decreased sleep duration in the ADHD group, compared to controls, is supported by the study by Becker et al. [
13], suggesting that ADHD patients did not benefit from the COVID-19 lockdown, unlike their healthy peers of the control group that experienced an increase in school days night sleep duration and were more likely to obtain recommended sleep duration during COVID-19. Similarly, Mutluer et al. [
15] reported a decrease in the number of hours ASD children slept from before to during COVID-19. Finally, our findings agree with those by Bruni et al. [
2] who reported a general stable sleep duration among healthy children, with only a small but significant increase during lockdown.
We found an increase in several sleep disorders during the lockdown: some disorders increased in all the three groups, such as anxiety at bedtime and daytime sleepiness while difficulties in falling asleep hypnic jerks, rhythmic movement disorder, night awakenings, restless sleep, sleepwalking, and daytime sleepiness increased especially in patients with ASD and ADHD. Interestingly, at baseline, ADHD children resulted to have increased bruxism, nightmares, and daytime sleepiness than their ASD peers, while during the lockdown ASD and ADHD children and adolescents had a similar prevalence of all sleep disturbances, with the exception of nightmares that were more frequent in ADHD children.
Very few studies have been published on the impact of the COVID-19 lockdown on sleep disorders of patients with ASD and ADHD. Regarding the sleep disorders of ASD patients during the pandemic, our results are in agreement with those by Türkoğlu et al. [
17] that reported an increase in difficulties (and delay) in falling asleep, and anxiety at bedtime; in contrast, we did not find an increase in night awakenings, but we observed an increase in daytime sleepiness. Similarly, Lugo-Marin et al. [
14] reported a deterioration in sleep quality in 56% of 100 ASD patients (children and adults). Very few studies have examined sleep disorders of ADHD youths during COVID-19. In a sample of 241 youth (aged 6–15 years) with ADHD in China, 48% of parents indicated that COVID-19 had not changed their child’s sleep, with 20% indicating that sleep had worsened, and 32% indicating that sleep had improved. Becker et al. [
13] reported less improvement of daytime sleepiness in ADHD adolescents compared to their healthy peers of the control group.
Several sleep symptoms that we found increased in our ASD and ADHD children have been recognized to be an expression of a psychological distress condition [
27,
28] strictly related to the pandemic.
Altogether, our findings confirm a great distress susceptibility in both clinical children due to the sudden changes of lifestyle imposed by the lockdown experience that determined a vulnerability of their sleep–wake patterns. The different sleep pattern alterations in the two clinical groups might be linked to their core traits defining two distinct disorders: children with ASD, that tended to maintain their sleep–wake schedule, were less vulnerable due to the stereotyped behavior and insistence on sameness while children with ADHD, that showed greater changes in sleep–wake patterns, were more vulnerable, due to their innate behavior instability, swift changes in mood, and low frustration tolerance.
We have to consider that the interruption of social relationships, the reduction in physical activities as well as the academic and normal working activities, had an impact on sleep. In parallel, other studies showed a strong impact of lockdown on affective domains, highlighting mainly an increase in depression symptoms (for ADHD see Melegari et al., 2021) [
26]. Further studies focused on the lockdown impact on both sleep patterns and affective states in these clinical populations should contribute to explain their reciprocal interaction. Some limitations of this study need to be considered, such as the sample size (although relatively large for this condition) and sampling only respondents from a single country; thus, results may not be fully generalizable to other countries. In addition, the predetermined sample size to adequately reduce the risk of type II error was not achieved. Furthermore, most subjectively reported elements of the SDSC should be interpreted with caution due to potential parental misinterpretation in ASD subjects that are often non-verbal. Although the survey was conducted after only a few days from the end of the strict lockdown and in the presence of lighter restrictions, we cannot exclude a memory bias of the parents. Finally, we should consider that self-selection bias is inherent with the online survey methodology employing nonprobability sampling. On the other hand, a strength of the study is that examined similarity or differences in sleep pattern changes using the same instruments and the same temporal window of investigation.







{kind=link}
{kind=link}
{kind=link}