
Neuronal Dynamics of Pain in Parkinson’s Disease


Department of Neurology, Nara Medical University, Kashihara, Nara 634-8521, Japan
*
Author to whom correspondence should be addressed.
Brain Sci. 2021, 11(9), 1224; https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091224
Submission received: 12 July 2021
/
Revised: 5 September 2021
/
Accepted: 14 September 2021
/
Published: 16 September 2021
(This article belongs to the Section Behavioral Neuroscience)
Abstract
:Pain is an important non-motor symptom of Parkinson’s disease (PD). It negatively impacts the quality of life. However, the pathophysiological mechanisms underlying pain in PD remain to be elucidated. This study sought to use electroencephalographic (EEG) coherence analysis to compare neuronal synchronization in neuronal networks between patients with PD, with and without pain. Twenty-four patients with sporadic PD were evaluated for the presence of pain. Time-frequency and coherence analyses were performed on their EEG data. Whole-brain and regional coherence were calculated and compared between pain-positive and pain-negative patients. There was no significant difference in the whole-brain coherence between the pain-positive and pain-negative groups. However, temporal–temporal coherence differed significantly between the two groups (p = 0.031). Our findings indicate that aberrant synchronization of inter-temporal regions is involved in PD-related pain. This will further our understanding of the mechanisms underlying pain in PD.
1. Introduction
Parkinson’s disease (PD) is a well-known neurodegenerative disease. It is characterized by motor and non-motor symptoms (NMSs) [1,2]. Dopaminergic medications and deep brain stimulation therapy improve the motor symptoms and quality of life of patients with PD. However, NMSs are frequently difficult to treat. Many patients with PD experience pain as an NMS, which negatively impacts their quality of life [3]. PD-related pain never responds to analgesic medications, although it sometimes responds to dopaminergic medications [4]. Moreover, the mechanisms underlying pain in PD have not been sufficiently studied [5].
Pain in patients with PD may result from altered sensory processing [6]. Previous studies found that, as seen in central sensitization, abnormal neuronal synchronization occurs in the brain networks of patients with PD with pain [7]. Electroencephalography (EEG) is a simple method for measuring brain neuronal activity and synchronization [8]. Quantitative EEG analysis provides information about whole-brain and regional connectivity [8]. EEG coherence has been used as a biomarker for the clinical severity of PD [9].
Previous studies on neuronal synchronization have compared patients with PD with healthy controls. However, a comparison between patients with PD with and without pain has not yet been performed. Thus, our study aimed to elucidate the association between neuronal synchronization in neuronal networks and PD-related pain, using EEG coherence analysis. To this end, we investigated the difference in coherence between patients with PD, with and without pain.
2. Materials and Methods
2.1. Patients and Clinical Data
We included patients with continuous sporadic PD who visited Nara Medical University Hospital, Nara, Japan. The inclusion criteria were (1) Japanese patients with confirmed PD who met the U.K. PD Society Brain Bank clinical diagnostic criteria [10], (2) patients aged 40–90 years, and (3) patients with no significant brain lesions on magnetic resonance imaging. The exclusion criteria were (1) patients receiving medications that could influence the EEG findings (e.g., antianxiety medication, antidepressant medication, such as serotonin–noradrenaline reuptake inhibitors and selective serotonin reuptake inhibitors, antiepileptic medication, and opioids), (2) patients who had undergone operations, such as deep brain stimulation, (3) patients with severe cognitive impairment (Mini-Mental State Examination score < 10), and (4) patients with other known causes of pain (e.g., orthopedic disease, peripheral neuropathy, spinal cord disease). Pain was assessed using the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part I (MDS-UPDRS-I) scores for the item of pain and other sensations (Q 1.9) [11]. This item was rated on a scale of 0–4: (0—normal: no uncomfortable feelings such as pain, aches, tingling, or cramps. 1—slight: I have these feelings. However, I can do things and be with other people without difficulty. 2—mild: These feelings cause some problems when I do things or am with other people. 3—moderate: These feelings cause a lot of problems, but they do not stop me from doing things or being with other people. 4—severe: These feelings stop me from doing things or being with other people.). EEG (Neurofax EEG-1224, Nihon Kohden, Tokyo, Japan) was performed, using the international 10–20 electrode placement system and a sampling rate of 200 Hz. The electrodes were referenced to linked earlobes (A1 + A2). During EEG recordings, patients were instructed to relax in a supine position and avoid blinking as much as possible. The EEG examinations and clinical assessment were carried out at the same time of day on separate days within one month with the patients in the “on” phase after 1 to 2 h, while on their usual medications. As such, we sought to exclude the cases of dystonia-related pain in the “off” phase. This study was approved by the Clinical Research Ethics Board of Nara Medical University. Informed consent was obtained from all patients.
2.2. EEG Analysis
EEG data were analyzed, using MATLAB (version R2020a; Math Works) and EEGLAB toolbox (version 14.1.2) [12]. The EEG data were band-pass filtered, using finite-impulse response filtering. A low-pass filter of 45 Hz and high-pass filter of 1 Hz were applied. Since EEG data are often contaminated with artifacts at the beginning of a recording, we manually selected 60 s of resting-state eyes-closed EEG data 5 min after recording began. These data were segmented into 2 s epochs, and artifact-contaminated epochs were removed. Time-frequency analysis was performed across all 16 electrodes, using fast Fourier transformation with a wavelet transform and a frequency resolution of 1 Hz (Figure S1). The EEG data of the following four frequency bands were separately analyzed and compared between the groups: theta (4–7 Hz), alpha (8–12 Hz), beta (13–30 Hz), and gamma (31–45 Hz) [13]. The EEG data underwent notch filtering at 50 Hz and were decomposed, using wavelet transformation with two cycles per frequency band. A coherence analysis was performed between all electrode pairs [12]. All 16 electrodes were assigned to four brain regions (frontal—Fp1, Fp2, F3, F4, F7, and F8; parietal—C3, C4, P3, and P4; temporal—T3, T4, T5, and T6; and occipital—O1 and O2), and electrode pairs were categorized into 10 groups representing brain regions (frontal–frontal (FF); frontal–parietal (FP); frontal–temporal (FT); frontal–occipital (FO); parietal–parietal (PP); parietal–temporal (PT); parietal–occipital (PO); temporal–temporal (TT); temporal–occipital (TO); occipital–occipital (OO)). Whole-brain coherence was assessed by averaging the coherence values of all the electrode pairs, and regional coherence was assessed by averaging the coherence values of electrode pairs based on the region for each frequency band [14,15]. For example, the value of TT coherence was assessed by averaging the values of T3-T4, T3-T5, T3-T6, T4-T5, T4-T6, and T5-T6 [14]. The inter-regional coherence indicated FP, FT, FO, PT, PO, and TO coherence, and the intra-regional coherence indicated FF, PP, TT, and OO coherence. To evaluate inter-and intra-regional connectivity, regional coherence was compared between the pain-positive and pain-negative groups. We also probed the relationship between regional coherence and clinical characteristics in both groups.
2.3. Statistical Analyses
The means of variables were compared between pain-positive and pain-negative patients with PD, using an independent two-sample t-test and chi-square test. A Shapiro–Wilk test was used to assess the distribution of the data. Statistical significance was set at p < 0.05. A correlation was considered strong if the correlation coefficient (r) was >0.40. Analyses were performed in SPSS 22.0 J (IBM Japan, Tokyo, Japan).
3. Results
Twenty-four patients with PD (14 men and 10 women) fulfilled the selection criteria and were enrolled in this study. The pain-positive and pain-negative groups comprised 12 patients (7 men and 5 women) each. The demographic characteristics, levodopa-equivalent daily dose, and clinical features of the 24 patients with PD are summarized in Table 1. There was no statistically significant difference between the two groups in these variables, which included key variables, such as age, disease duration, MDS-UPDRS-III score, levodopa-equivalent daily dose [16], and Hoehn–Yahr scores. The mean score of MDS-UPDRS-I for pain and other sensations was 2.25 ± 0.75. One patient (8.3%) had a score of 1 (slight), eight (55.7%) patients had a score of 2 (mild), two (16.7%) patients had a score of 3 (moderate) and one (8.3%) patient had a score of 4 (severe; Table 1). Four of the patients (33%) had continuous pain, and eight (67%) patients had discontinuous pain.
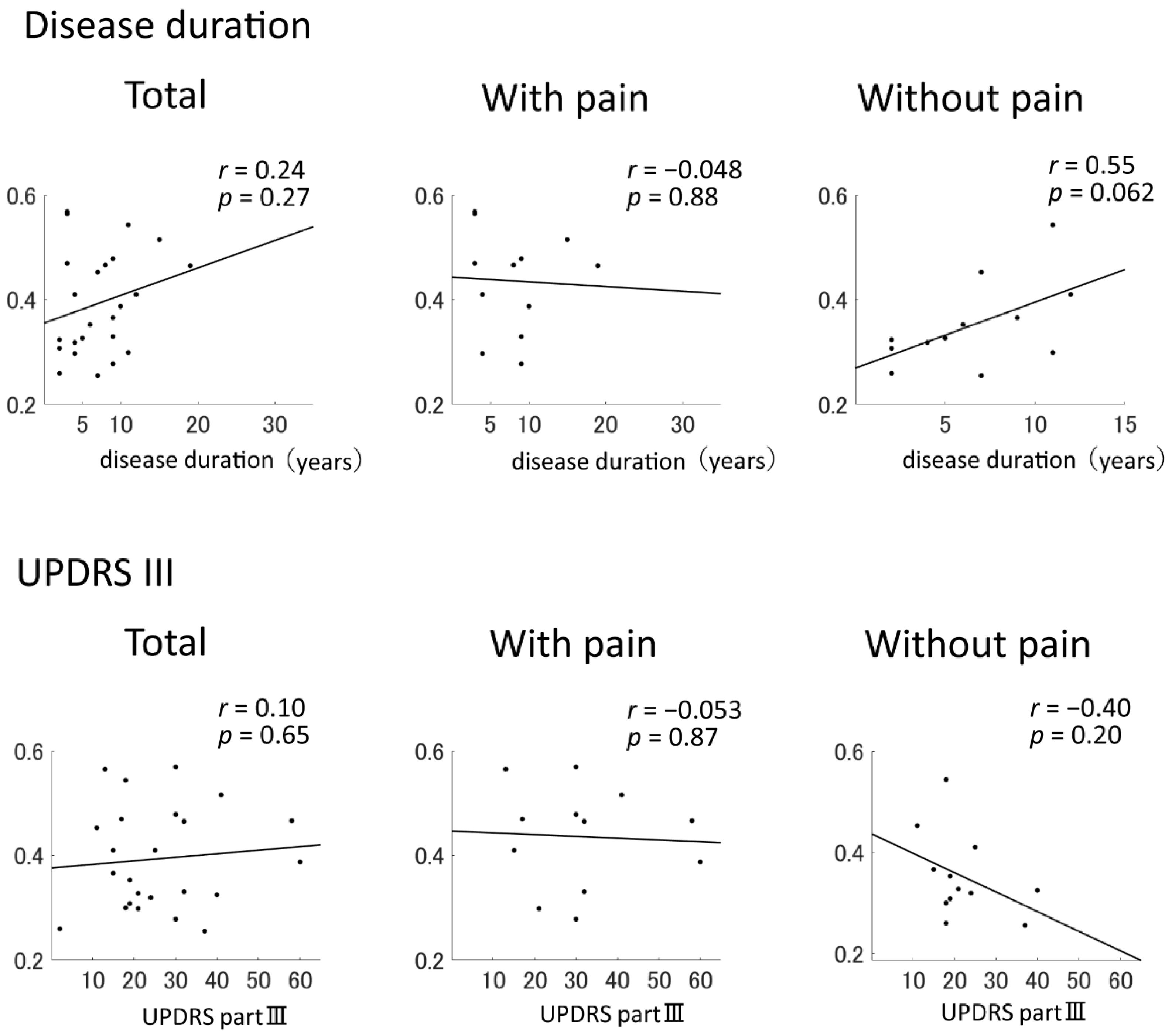
No significant differences were identified in whole-brain coherence in the alpha band between the pain-positive and pain-negative groups (p = 0.39). The coherence of the TT region in the alpha band significantly differed between the two groups (p = 0.031; Table 2) and was not correlated with the MDS-UPDRS-III score or disease duration in the pain-positive group (r = −0.053 and −0.048, respectively). However, these variables were correlated in the pain-negative group (r = −0.40 and 0.55, respectively; Figure 1). The pain-positive group was further divided into limb-pain (n = 5) and trunk-pain (n = 7) groups, and the whole-brain coherence, regional coherence, MDS-UPDRS-III score, and disease duration were compared between these two groups. The coherence of the TT region was higher in the trunk-pain group than in the limb-pain group (p = 0.034). There were no significant differences between the limb-pain and trunk-pain groups in the MDS-UPDRS-III score (p = 1.00) or disease duration (p = 0.40).
4. Discussion
Here, EEG coherence in the alpha frequency band, used to evaluate neuronal synchronization in brain networks, was associated with pain modulation. Functional abnormalities can result in the reorganization of the sensory system [17]. This can lead to central sensitization, defined as an increased responsiveness of nociceptive neurons in the central nervous system to normal or subthreshold afferent input [18]. Pain hypersensitivity is elicited by neural signal amplification. Central sensitization has been thought to play a role in unexplained pain in several disorders, such as fibromyalgia, epilepsy, Alzheimer’s disease, and PD [19,20]. Alongside limb pain, patients with PD commonly experience trunk pain, including abdominal pain [21]. Various factors, such as altered posture, muscle tone abnormalities, and truncal dystonia, contribute to trunk pain in patients with PD. However, trunk pain is frequently neglected and insufficiently treated in patients with PD [22].
An EEG coherence analysis revealed that patients with PD with pain showed higher regional coherence, representing increased functional connectivity, in the temporal regions. The temporal lobe is generally responsible for establishing long-term memory, cognitive and emotional functions, and auditory processing [23]. However, several neuroimaging studies have reported altered activation within this region [24,25,26]. In patients with chronic low back pain, the anterior hippocampus, a part of the medial temporal lobe, showed significantly lower levels of activity and functional connectivity than the medial prefrontal cortex [26]. The anterior hippocampus is involved in mood-related functions and psychological modulation, likely through interactions with the amygdala. The amygdala regulates psychological responses and has been thought to play a role in pain-related negative affect processing. The amygdala may induce hypoalgesia to modulate pain in individuals with psychological stress. Anterior hippocampus–amygdala interactions are known to be involved in both the encoding and retrieval of affective information, and this has been observed in individuals with experimental pain. Thus, pain-related abnormal anterior hippocampal activity may be related to psychological dysregulation. Pain may be considered a stressor, and it elicits a prolonged stress response; this implies that pain poses an allostatic load on the neuronal networks. The hippocampus is particularly sensitive to the neurotoxic effects of prolonged exposure to psychological stress, which affects its structure and function [26]. Our results are consistent with the previous findings, demonstrating that aberrant connectivity in the temporal lobe could result in pain. Moreover, we found that temporal lobe connectivity was not correlated with the MDS-UPDRS-III score or disease duration in patients with PD with pain, which is consistent with the findings of a previous study [27]. These results suggest that higher temporal lobe inter-regional connectivity is related to pain in patients with PD.
Our study sheds light on the possible mechanisms underlying PD-related pain; however, several limitations should be considered. First, we presented a novel approach to evaluate PD-related pain, using EEG coherence analysis. It may be key in elucidating the mechanism of pain in PD cases. This clinical study was a pilot study with a limited sample size [9]. Based on the obtained results, a large clinical trial should be performed to validate our findings in the appropriate populations. Second, our study focused on the difference in neuronal synchronization between patients with and without pain and did not consider other clinical factors that might influence pain, such as depression [28], which has been associated with abnormal connectivity in the default mode network in patients with PD [29]. Many other factors, such as age, sex, and medical history, may also contribute to the reorganization of functional connectivity in neuronal networks [30]. Third, we did not assess pain intensity, because the intensity of PD-related pain fluctuates throughout the day [31]. Additionally, to evaluate cortical–subcortical synchronization with pain, further studies, such as stereo-EEG and functional MRI studies, are needed [7,32].
5. Conclusions
In conclusion, we performed an EEG coherence analysis in patients with PD, with and without pain. Aberrant neuronal synchronization and abnormal inter-temporal lobe connectivity may be involved in PD-related pain. By performing the EEG analysis, we examined the mechanisms of abnormal connectivity underpinning pain in PD. There have been numerous basic and clinical research studies on pain in patients with PD; however, the mechanism remains unclear. Therefore, it may be useful to evaluate pain from a new perspective by performing a non-invasive neurophysiological technique.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/brainsci11091224/s1, Figure S1: Time frequency and coherence analysis on EEG data.
Author Contributions
Conceptualization, K.K. and T.M.; formal analysis, K.K. and T.M.; writing—original draft preparation, K.K. and T.M.; supervision, K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by grants from Grants-in-Aid (KAKENHI No. 20K19453 and 17K17843) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Clinical Research Ethics Board of Nara Medical University (Approval Number: 2670).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lim, S.Y.; Lang, A.E. The nonmotor symptoms of Parkinson’s disease--an overview. Mov. Disord. 2010, 25 (Suppl. 1), S123–S130. [Google Scholar] [CrossRef]
- Dickson, D.W. Neuropathology of Parkinson disease. Parkinsonism Relat. Disord. 2018, 46 (Suppl. 1), S30–S33. [Google Scholar] [CrossRef] [PubMed]
- Ford, B. Pain in Parkinson’s disease. Mov. Disord. 2010, 25 (Suppl. 1), S98–S103. [Google Scholar] [CrossRef]
- Kass-Iliyya, L.; Kobylecki, C.; McDonald, K.R.; Gerhard, A.; Silverdale, M.A. Pain in multiple system atrophy and progressive supranuclear palsy compared to Parkinson’s disease. Brain Behav. 2015, 5, e00320. [Google Scholar] [CrossRef] [PubMed]
- Polli, A.; Weis, L.; Biundo, R.; Thacker, M.; Turolla, A.; Koutsikos, K.; Chaudhuri, K.R.; Antonini, A. Anatomical and functional correlates of persistent pain in Parkinson’s disease. Mov. Disord. 2016, 31, 1854–1864. [Google Scholar] [CrossRef]
- Berardelli, A.; Conte, A.; Fabbrini, G.; Bologna, M.; Latorre, A.; Rocchi, L.; Suppa, A. Pathophysiology of pain and fatigue in Parkinson’s disease. Parkinsonism Relat. Disord. 2012, 18 (Suppl. 1), S226–S228. [Google Scholar] [CrossRef]
- Engels, G.; McCoy, B.; Vlaar, A.; Theeuwes, J.; Weinstein, H.; Scherder, E.; Douw, L. Clinical pain and functional network topology in Parkinson’s disease: A resting-state fMRI study. J. Neural Transm. (Vienna) 2018, 125, 1449–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, R.; Winter, W.R.; Ding, J.; Nunez, P.L. EEG and MEG coherence: Measures of functional connectivity at distinct spatial scales of neocortical dynamics. J. Neurosci. Methods 2007, 166, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Yuvaraj, R.; Murugappan, M.; Ibrahim, N.M.; Sundaraj, K.; Omar, M.I.; Mohamad, K.; Palaniappan, R.; Satiyan, M. Inter-hemispheric EEG coherence analysis in Parkinson’s disease: Assessing brain activity during emotion processing. J. Neural Transm. (Vienna) 2015, 122, 237–252. [Google Scholar] [CrossRef]
- Daniel, S.E.; Lees, A.J. Parkinson’s Disease Society Brain Bank, London: Overview and research. J. Neural Transm. Suppl. 1993, 39, 165–172. [Google Scholar]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, W.; Jin, S.H.; Kim, M.; Kim, J.S.; Chung, C.K. Abnormal functional brain network in epilepsy patients with focal cortical dysplasia. Epilepsy Res. 2014, 108, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Leon-Carrion, J.; Leon-Dominguez, U.; Pollonini, L.; Wu, M.H.; Frye, R.E.; Dominguez-Morales, M.R.; Zouridakis, G. Synchronization between the anterior and posterior cortex determines consciousness level in patients with traumatic brain injury (TBI). Brain Res. 2012, 1476, 22–30. [Google Scholar] [CrossRef]
- Laptinskaya, D.; Fissler, P.; Kuster, O.C.; Wischniowski, J.; Thurm, F.; Elbert, T.; von Arnim, C.A.F.; Kolassa, I.T. Global EEG coherence as a marker for cognition in older adults at risk for dementia. Psychophysiology 2020, 57, e13515. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Cauda, F.; Palermo, S.; Costa, T.; Torta, R.; Duca, S.; Vercelli, U.; Geminiani, G.; Torta, D.M. Gray matter alterations in chronic pain: A network-oriented meta-analytic approach. Neuroimage Clin. 2014, 4, 676–686. [Google Scholar] [CrossRef] [Green Version]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Tommaso, M.; Kunz, M.; Valeriani, M. Therapeutic approach to pain in neurodegenerative diseases: Current evidence and perspectives. Expert Rev. Neurother 2017, 17, 143–153. [Google Scholar] [CrossRef]
- Abuhasira, R.; Zlotnik, Y.; Horev, A.; Ifergane, G. Fibromyalgia-Like Syndrome Associated with Parkinson’s Disease-A Cohort Study. J. Clin. Med. 2019, 8, 1118. [Google Scholar] [CrossRef] [Green Version]
- Barone, P.; Antonini, A.; Colosimo, C.; Marconi, R.; Morgante, L.; Avarello, T.P.; Bottacchi, E.; Cannas, A.; Ceravolo, G.; Ceravolo, R.; et al. The PRIAMO study: A multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Mov. Disord. 2009, 24, 1641–1649. [Google Scholar] [CrossRef]
- Broetz, D.; Eichner, M.; Gasser, T.; Weller, M.; Steinbach, J.P. Radicular and nonradicular back pain in Parkinson’s disease: A controlled study. Mov. Disord. 2007, 22, 853–856. [Google Scholar] [CrossRef]
- Chauviere, L. Update on temporal lobe-dependent information processing, in health and disease. Eur. J. Neurosci. 2020, 51, 2159–2204. [Google Scholar] [CrossRef] [PubMed]
- Niddam, D.M.; Chan, R.C.; Lee, S.H.; Yeh, T.C.; Hsieh, J.C. Central representation of hyperalgesia from myofascial trigger point. Neuroimage 2008, 39, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Oathes, D.; Hush, J.; Darnall, B.; Charvat, M.; Mackey, S.; Etkin, A. Perturbed connectivity of the amygdala and its subregions with the central executive and default mode networks in chronic pain. Pain 2016, 157, 1970–1978. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, L.J.; Barnett, A.; Leboucher, A.; Golosky, M.; McAndrews, M.P.; Seminowicz, D.A.; Moayedi, M. The medial temporal lobe in nociception: A meta-analytic and functional connectivity study. Pain 2019, 160, 1245–1260. [Google Scholar] [CrossRef]
- Beiske, A.G.; Loge, J.H.; Ronningen, A.; Svensson, E. Pain in Parkinson’s disease: Prevalence and characteristics. Pain 2009, 141, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.Q.; Qureshi, A.R.M.; Rahman, N.; Mohammed, A.; Sarfraz, Z.; Rana, R. Disability from pain directly correlated with depression in Parkinson’s disease. Clin. Neurol. Neurosurg. 2017, 160, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Brakowski, J.; Spinelli, S.; Dorig, N.; Bosch, O.G.; Manoliu, A.; Holtforth, M.G.; Seifritz, E. Resting state brain network function in major depression—Depression symptomatology, antidepressant treatment effects, future research. J. Psychiatr. Res. 2017, 92, 147–159. [Google Scholar] [CrossRef]
- Gao, L.L.; Wu, T. The study of brain functional connectivity in Parkinson’s disease. Transl. Neurodegener. 2016, 5, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franke, C.; Storch, A. Nonmotor Fluctuations in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 134, 947–971. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, A.A.; Kupsch, A.; Schneider, G.H.; Brown, P. Reduction in subthalamic 8-35 Hz oscillatory activity correlates with clinical improvement in Parkinson’s disease. Eur. J. Neurosci. 2006, 23, 1956–1960. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pearson correlation coefficients and graphs for the correlation of temporal–temporal coherence in the alpha range with disease duration and MDS-UPDRS-III score. The lines indicate the approximate line using the least squares method. MDS-UPDRS-III = Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III.
Figure 1.
Pearson correlation coefficients and graphs for the correlation of temporal–temporal coherence in the alpha range with disease duration and MDS-UPDRS-III score. The lines indicate the approximate line using the least squares method. MDS-UPDRS-III = Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III.


{kind=link}
Table 1.
Demographic and clinical characteristics of the participants.
| PD | PD with Pain | PD without Pain | p Value | |
|---|---|---|---|---|
| Number | 24 | 12 | 12 | |
| Age | 72.29 ± 8.70 | 72.58 ± 10.80 | 72.0 ± 6.42 | 0.87 |
| Sex | 14 Male/10 Female | 7 Male/5 Female | 7 Male/5 Female | 1.00 |
| Disease Duration, years | 7.25 ± 4.40 | 8.08 ± 5.28 | 6.5 ± 3.66 | 0.40 |
| Pain Duration, years | 4.0 ± 2.61 | NA | NA | |
| H–Y stages | ||||
| H–Y II | 7 (29.2%) | 3 (25.0%) | 4 (33.3%) | 0.69 |
| H–Y III | 9 (37.5%) | 4 (33.3%) | 5 (41.7%) | |
| H–Y IV | 8 (33.3%) | 5 (41.7%) | 3 (25.0%) | |
| LEDD, mg | 598.86 ± 364.99 | 621.60 ± 368.89 | 576.13 ± 375.96 | 0.77 |
| L-dopa | 23 (95.8%) | 12 (100%) | 11 (91.7%) | 0.31 |
| D-Agonist | 12 (50%) | 7 (58.3%) | 5 (41.7%) | 0.41 |
| MAOBI | 3 (16.7%) | 1 (8.3%) | 2 (16.7%) | 0.54 |
| MDS-UPDRS | ||||
| Total | 61.13 ± 27.92 | 71.25 ± 34.21 | 51.0 ± 15.4 | 0.075 |
| Part I | 12.92 ± 6.95 | 13.92 ± 8.17 | 11.92 ± 5.66 | 0.49 |
| Pain and other sensations score | ||||
| 1 (Slight) | 1 (8.3%) | NA | NA | |
| 2 (Mild) | 8 (55.7%) | NA | NA | |
| 3 (Moderate) | 2 (16.7%) | NA | NA | |
| 4 (Severe) | 1 (8.3%) | NA | NA | |
| Part II | 16.13 ± 9.76 | 19.58 ± 11.57 | 12.67 ± 6.27 | 0.082 |
| Part III | 26.83 ± 13.00 | 31.58 ± 15.22 | 22.08 ± 8.5 | 0.072 |
| Part IV | 5.25 ± 3.71 | 6.17 ± 4.09 | 4.33 ± 3.20 | 0.23 |
| MMSE score | 24.58 ± 4.14 | 25.0 ± 3.95 | 24.17 ± 4.45 | 0.63 |
| FAB score | 12.96 ± 2.56 | 13.08 ± 3.06 | 12.83 ± 2.08 | 0.82 |
Note: Data are presented as mean ± SD. Disease duration was calculated as the number of years since PD diagnosis. Hoehn and Yahr stages were used to assess the severity of motor symptoms. The Movement Disorder Society Unified Parkinson’s Disease Rating Scale was administered to the patients in the “on” phase. The total dose of medication was converted to a levodopa-equivalent daily dose in mg [16]. PD = Parkinson’s disease; H–Y = Hoehn and Yahr; LEDD = levodopa-equivalent daily dose; L-dopa = L-3, 4-Dihydroxyphenylalanine; D-Agonist = dopamine agonist; MAOBI = monoamine oxidase-B inhibitors; MDS-UPDRS = Movement Disorder Society Unified Parkinson’s Disease Rating Scale; MMSE = Mini-Mental State Examination; FAB = frontal assessment battery; SD = standard deviation; NA = not available.
Table 2.
Comparison of the whole-brain and regional coherence values in the alpha band between patients with PD, with and without pain.
Table 2.
Comparison of the whole-brain and regional coherence values in the alpha band between patients with PD, with and without pain.
| PD with Pain | PD without Pain | p Value | |
|---|---|---|---|
| Whole brain | 0.46 ± 0.12 | 0.42 ± 0.07 | 0.39 |
| FF | 0.63 ± 0.11 | 0.59 ± 0.08 | 0.40 |
| FP | 0.45 ± 0.15 | 0.42 ± 0.07 | 0.49 |
| FT | 0.37 ± 0.12 | 0.32 ± 0.07 | 0.16 |
| FO | 0.31 ± 0.13 | 0.27 ± 0.12 | 0.35 |
| PP | 0.58 ± 0.13 | 0.58 ± 0.08 | 0.96 |
| PT | 0.46 ± 0.12 | 0.45 ± 0.08 | 0.77 |
| PO | 0.52 ± 0.11 | 0.52 ± 0.11 | 0.91 |
| TT | 0.44 ± 0.10 | 0.35 ± 0.08 | <0.05 |
| TO | 0.44 ± 0.11 | 0.44 ± 0.11 | 0.92 |
| OO | 0.64 ± 0.10 | 0.60 ± 0.10 | 0.35 |
Note: Data are presented as mean ± SD. FF = frontal–frontal; FP = frontal–parietal; FT = frontal–temporal; FO = frontal–occipital; PP = parietal–parietal; PT = parietal–temporal; PO = parietal–occipital; TT = temporal–temporal; TO = temporal–occipital; OO = occipital–occipital; SD = standard deviation.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kinugawa, K.; Mano, T.; Sugie, K. Neuronal Dynamics of Pain in Parkinson’s Disease. Brain Sci. 2021, 11, 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091224
AMA Style
Kinugawa K, Mano T, Sugie K. Neuronal Dynamics of Pain in Parkinson’s Disease. Brain Sciences. 2021; 11(9):1224. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091224
Chicago/Turabian StyleKinugawa, Kaoru, Tomoo Mano, and Kazuma Sugie. 2021. "Neuronal Dynamics of Pain in Parkinson’s Disease" Brain Sciences 11, no. 9: 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091224
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.