
Non-Invasive Transcutaneous Vagus Nerve Stimulation for the Treatment of Fibromyalgia Symptoms: A Study Protocol

 ,
,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
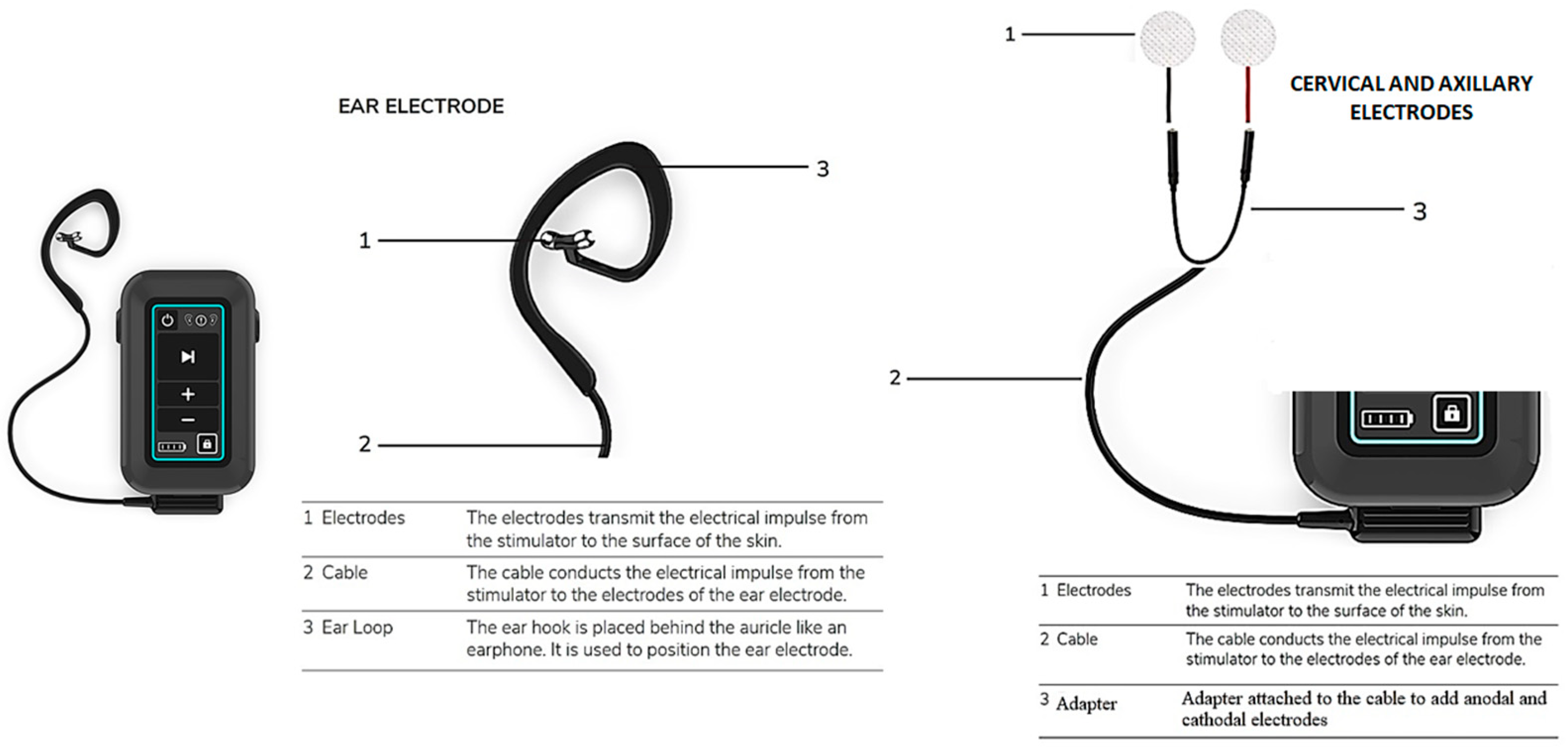
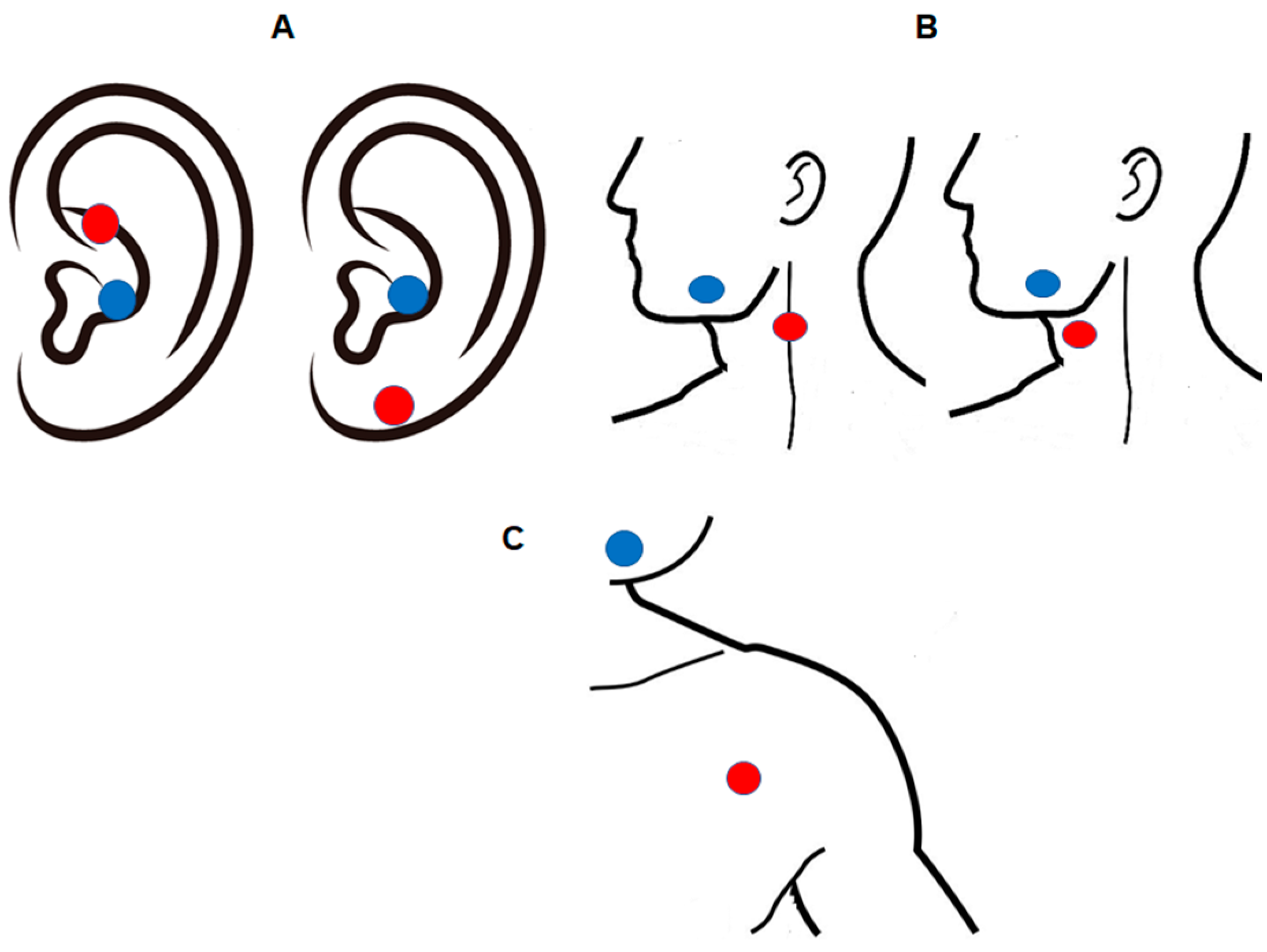
2.2. tVNS
2.3. Outcome Measures
2.4. Randomization Method
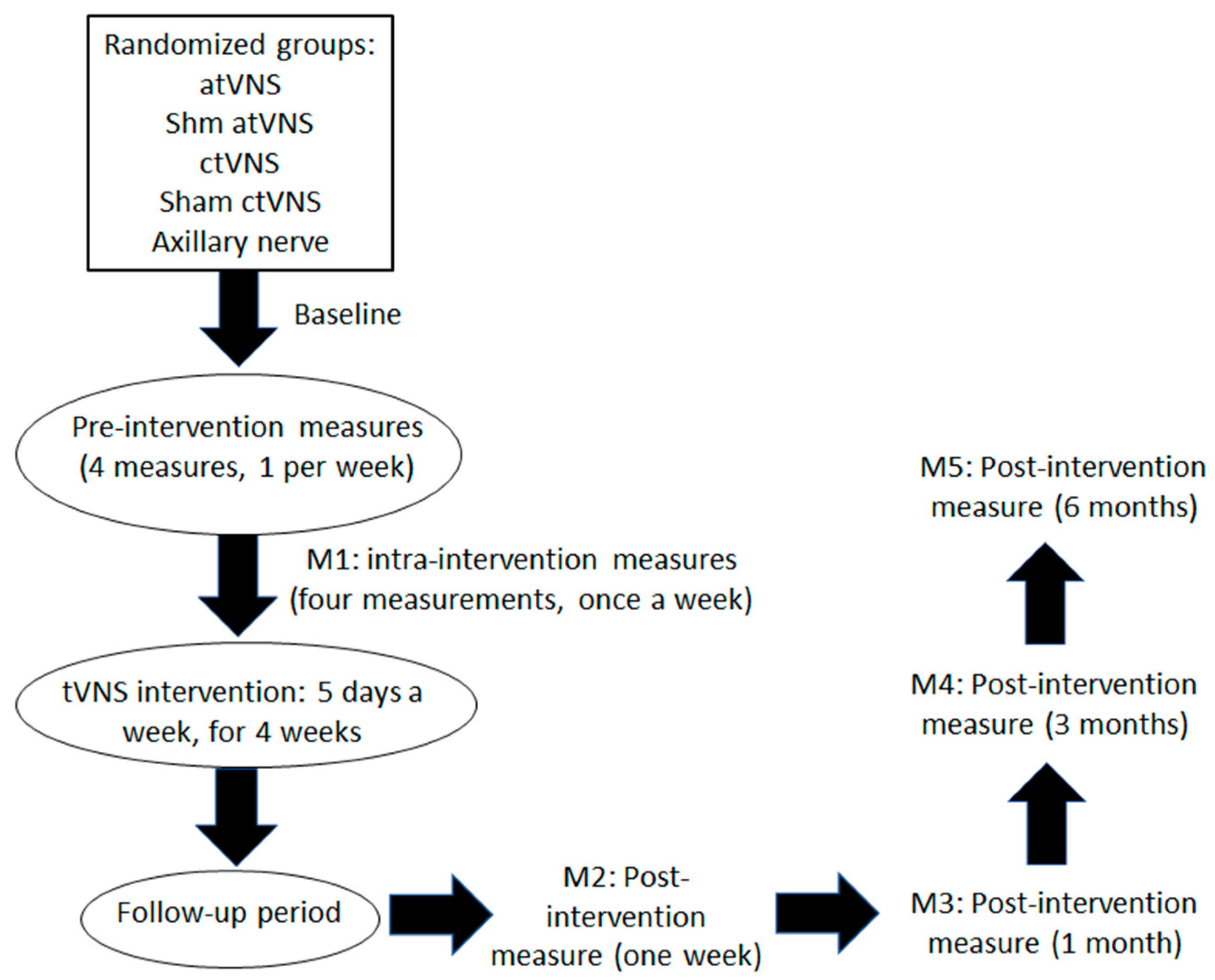
2.5. Procedure
2.6. Statistical Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borchers, A.T.; Gershwin, M.E. Fibromyalgia: A Critical and Comprehensive Review. Clin. Rev. Allerg. Immunol. 2015, 49, 100–151. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An Update on Clinical Characteristics, Aetiopathogenesis and Treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia Pathogenesis and Treatment Options Update. Curr. Pain. Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Maffei, M.E. Fibromyalgia: Recent Advances in Diagnosis, Classification, Pharmacotherapy and Alternative Remedies. IJMS 2020, 21, 7877. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.I.; Claydon, L.S.; Herbison, G.P.; Paley, C.A.; Jones, G. Transcutaneous Electrical Nerve Stimulation (TENS) for Fibromyalgia in Adults. In Cochrane Database of Systematic Reviews; The Cochrane Collaboration, Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2016; p. CD012172. [Google Scholar]
- Hammer, N.; Glätzner, J.; Feja, C.; Kühne, C.; Meixensberger, J.; Planitzer, U.; Schleifenbaum, S.; Tillmann, B.N.; Winkler, D. Human Vagus Nerve Branching in the Cervical Region. PLoS ONE 2015, 10, e0118006. [Google Scholar] [CrossRef] [PubMed]
- Lerman, I.; Davis, B.; Huang, M.; Huang, C.; Sorkin, L.; Proudfoot, J.; Zhong, E.; Kimball, D.; Rao, R.; Simon, B.; et al. Noninvasive Vagus Nerve Stimulation Alters Neural Response and Physiological Autonomic Tone to Noxious Thermal Challenge. PLoS ONE 2019, 14, e0201212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kox, M.; Pickkers, P. Modulation of the Innate Immune Response through the Vagus Nerve. Nephron 2015, 131, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Colzato, L.S.; Sellaro, R.; Beste, C. Darwin Revisited: The Vagus Nerve Is a Causal Element in Controlling Recognition of other’s Emotions. Cortex 2017, 92, 95–102. [Google Scholar] [CrossRef]
- Huston, J.M. The Vagus Nerve and the Inflammatory Reflex: Wandering on a New Treatment Paradigm for Systemic Inflammation and Sepsis. Surg. Infect. 2012, 13, 187–193. [Google Scholar] [CrossRef]
- Komisaruk, B.R.; Frangos, E. Vagus Nerve Afferent Stimulation: Projection into the Brain, Reflexive Physiological, Perceptual, and Behavioral Responses, and Clinical Relevance. Auton. Neurosci. 2022, 237, 102908. [Google Scholar] [CrossRef]
- Dedoncker, J.; Vanderhasselt, M.-A.; Ottaviani, C.; Slavich, G.M. Mental Health during the COVID-19 Pandemic and beyond: The Importance of the Vagus Nerve for Biopsychosocial Resilience. Neurosci. Biobehav. Rev. 2021, 125, 1–10. [Google Scholar] [CrossRef]
- Attenello, F.; Amar, A.P.; Liu, C.; Apuzzo, M.L.J. Theoretical Basis of Vagus Nerve Stimulation. In Progress in Neurological Surgery; Slavin, K.V., Ed.; S. Karger AG: Berlin, Germany, 2015; Volume 29, pp. 20–28. ISBN 978-3-318-02808-9. [Google Scholar]
- Yuan, H.; Silberstein, S.D. Vagus Nerve and Vagus Nerve Stimulation, a Comprehensive Review: Part II. Headache J. Head Face Pain 2016, 56, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Lendvai, I.S.; Maier, A.; Scheele, D.; Hurlemann, R.; Kinfe, T.M. Spotlight on Cervical Vagus Nerve Stimulation for the Treatment of Primary Headache Disorders: A Review. J. Pain Res. 2018, 11, 1613–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rings, T.; von Wrede, R.; Bröhl, T.; Schach, S.; Helmstaedter, C.; Lehnertz, K. Impact of Transcutaneous Auricular Vagus Nerve Stimulation on Large-Scale Functional Brain Networks: From Local to Global. Front. Physiol. 2021, 12, 700261. [Google Scholar] [CrossRef] [PubMed]
- von Wrede, R.; Rings, T.; Schach, S.; Helmstaedter, C.; Lehnertz, K. Transcutaneous Auricular Vagus Nerve Stimulation Induces Stabilizing Modifications in Large-Scale Functional Brain Networks: Towards Understanding the Effects of TaVNS in Subjects with Epilepsy. Sci. Rep. 2021, 11, 7906. [Google Scholar] [CrossRef]
- Mirakaj, V.; Dalli, J.; Granja, T.; Rosenberger, P.; Serhan, C.N. Vagus Nerve Controls Resolution and Pro-Resolving Mediators of Inflammation. J. Exp. Med. 2014, 211, 1037–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, H.; Silberstein, S.D. Vagus Nerve and Vagus Nerve Stimulation, a Comprehensive Review: Part I: Headache. Headache J. Head Face Pain 2016, 56, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Silberstein, S.D. Vagus Nerve and Vagus Nerve Stimulation, a Comprehensive Review: Part III. Headache J. Head Face Pain 2016, 56, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Kulshreshtha, P.; Deepak, K.K. Autonomic Nervous System Profile in Fibromyalgia Patients and Its Modulation by Exercise: A Mini Review. Clin. Physiol. Funct. Imaging 2013, 33, 83–91. [Google Scholar] [CrossRef]
- Cohen, H.; Neumann, L.; Kotler, M.; Buskila, D. Autonomic Nervous System Derangement in Fibromyalgia Syndrome and Related Disorders. Israel Med. Assoc. J. 2001, 3, 755–760. [Google Scholar]
- Martínez-Lavín, M. Fibromyalgia and Small Fiber Neuropathy: The Plot Thickens! Clin. Rheumatol 2018, 37, 3167–3171. [Google Scholar] [CrossRef]
- Adler, G.K.; Geenen, R. Hypothalamic–Pituitary–Adrenal and Autonomic Nervous System Functioning in Fibromyalgia. Rheum. Dis. Clin. N. Am. 2005, 31, 187–202. [Google Scholar] [CrossRef]
- Martínez-Martínez, L.-A.; Mora, T.; Vargas, A.; Fuentes-Iniestra, M.; Martínez-Lavín, M. Sympathetic Nervous System Dysfunction in Fibromyalgia, Chronic Fatigue Syndrome, Irritable Bowel Syndrome, and Interstitial Cystitis: A Review of Case-Control Studies. J. Clin. Rheumatol. 2014, 20, 146–150. [Google Scholar] [CrossRef]
- Hazra, S.; Venkataraman, S.; Handa, G.; Yadav, S.L.; Wadhwa, S.; Singh, U.; Kochhar, K.P.; Deepak, K.K.; Sarkar, K. A Cross-Sectional Study on Central Sensitization and Autonomic Changes in Fibromyalgia. Front. Neurosci. 2020, 14, 788. [Google Scholar] [CrossRef] [PubMed]
- Kulshreshtha, P.; Gupta, R.; Yadav, R.K.; Bijlani, R.L.; Deepak, K.K. A Comprehensive Study of Autonomic Dysfunction in the Fibromyalgia Patients. Clin. Auton. Res. 2012, 22, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Coskun Benlidayi, I. Role of Inflammation in the Pathogenesis and Treatment of Fibromyalgia. Rheumatol. Int. 2019, 39, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Littlejohn, G.; Guymer, E. Neurogenic Inflammation in Fibromyalgia. Semin. Immunopathol. 2018, 40, 291–300. [Google Scholar] [CrossRef]
- Metyas, S.; Rezk, T.; Arkfeld, D.; Leptich, T. Autoinflammation and Immunomodulation in Inflammatory Fibromyalgia Syndrome—A Review. Curr. Rheumatol. Rev. 2017, 13, 98–102. [Google Scholar] [CrossRef]
- Lange, G.; Janal, M.N.; Maniker, A.; FitzGibbons, J.; Fobler, M.; Cook, D.; Natelson, B.H. Safety and Efficacy of Vagus Nerve Stimulation in Fibromyalgia: A Phase I/II Proof of Concept Trial. Pain Med. 2011, 12, 1406–1413. [Google Scholar] [CrossRef] [Green Version]
- Antal, A.; Alekseichuk, I.; Bikson, M.; Brockmöller, J.; Brunoni, A.R.; Chen, R.; Cohen, L.G.; Dowthwaite, G.; Ellrich, J.; Flöel, A.; et al. Low Intensity Transcranial Electric Stimulation: Safety, Ethical, Legal Regulatory and Application Guidelines. Clin. Neurophysiol. 2017, 128, 1774–1809. [Google Scholar] [CrossRef] [Green Version]
- Yavari, F.; Jamil, A.; Mosayebi Samani, M.; Vidor, L.P.; Nitsche, M.A. Basic and Functional Effects of Transcranial Electrical Stimulation (TES)—An Introduction. Neurosci. Biobehav. Rev. 2018, 85, 81–92. [Google Scholar] [CrossRef]
- Butt, M.F.; Albusoda, A.; Farmer, A.D.; Aziz, Q. The Anatomical Basis for Transcutaneous Auricular Vagus Nerve Stimulation. J. Anat. 2020, 236, 588–611. [Google Scholar] [CrossRef] [Green Version]
- Deuchars, S.A.; Lall, V.K.; Clancy, J.; Mahadi, M.; Murray, A.; Peers, L.; Deuchars, J. Mechanisms Underpinning Sympathetic Nervous Activity and Its Modulation Using Transcutaneous Vagus Nerve Stimulation. Exp. Physiol. 2018, 103, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frangos, E.; Komisaruk, B.R. Access to Vagal Projections via Cutaneous Electrical Stimulation of the Neck: FMRI Evidence in Healthy Humans. Brain Stimul. 2017, 10, 19–27. [Google Scholar] [CrossRef]
- Yakunina, N.; Kim, S.S.; Nam, E.-C. Optimization of Transcutaneous Vagus Nerve Stimulation Using Functional MRI: TRANSCUTANEOUS VNS OPTIMIZATION USING FMRI. Neuromodul. Technol. Neural Interface 2017, 20, 290–300. [Google Scholar] [CrossRef]
- Verma, N.; Mudge, J.D.; Kasole, M.; Chen, R.C.; Blanz, S.L.; Trevathan, J.K.; Lovett, E.G.; Williams, J.C.; Ludwig, K.A. Auricular Vagus Neuromodulation—A Systematic Review on Quality of Evidence and Clinical Effects. Front. Neurosci. 2021, 15, 664740. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.L.; O’Leary, G.H.; Austelle, C.W.; Gruber, E.; Kahn, A.T.; Manett, A.J.; Short, B.; Badran, B.W. A Review of Parameter Settings for Invasive and Non-Invasive Vagus Nerve Stimulation (VNS) Applied in Neurological and Psychiatric Disorders. Front. Neurosci. 2021, 15, 709436. [Google Scholar] [CrossRef] [PubMed]
- von Wrede, R.; Surges, R. Transcutaneous Vagus Nerve Stimulation in the Treatment of Drug-Resistant Epilepsy. Auton. Neurosci. 2021, 235, 102840. [Google Scholar] [CrossRef]
- Bazzichi, L.; Giacomelli, C.; Consensi, A.; Atzeni, F.; Batticciotto, A.; Di Franco, M.; Casale, R.; Sarzi-Puttini, P. One Year in Review 2016: Fibromyalgia. Clin. Exp. Rheumatol. 2016, 34, S145–S149. [Google Scholar]
- Johnson, R.L.; Wilson, C.G. A Review of Vagus Nerve Stimulation as a Therapeutic Intervention. J. Inflamm. Res. 2018, 11, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Kutlu, N.; Özden, A.V.; Alptekin, H.K.; Alptekin, J.Ö. The Impact of Auricular Vagus Nerve Stimulation on Pain and Life Quality in Patients with Fibromyalgia Syndrome. BioMed Res. Int. 2020, 2020, 8656218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clancy, J.A.; Mary, D.A.; Witte, K.K.; Greenwood, J.P.; Deuchars, S.A.; Deuchars, J. Non-Invasive Vagus Nerve Stimulation in Healthy Humans Reduces Sympathetic Nerve Activity. Brain Stimul. 2014, 7, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Ellrich, J. Transcutaneous Auricular Vagus Nerve Stimulation. J. Clin. Neurophysiol. 2019, 36, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, S.-Y.; Wang, D.; Wu, M.-Z.; He, J.-K.; Zhang, J.-L.; Zhao, B.; Hou, L.-W.; Wang, J.-Y.; Wang, L.; et al. Transcutaneous Auricular Vagus Nerve Stimulation: From Concept to Application. Neurosci. Bull. 2021, 37, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Yap, J.Y.Y.; Keatch, C.; Lambert, E.; Woods, W.; Stoddart, P.R.; Kameneva, T. Critical Review of Transcutaneous Vagus Nerve Stimulation: Challenges for Translation to Clinical Practice. Front. Neurosci. 2020, 14, 284. [Google Scholar] [CrossRef]
- Zaehle, T.; Krauel, K. Transcutaneous Vagus Nerve Stimulation in Patients with Attention-Deficit/Hyperactivity Disorder: A Viable Option? In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2021; Volume 264, pp. 171–190. ISBN 978-0-12-822344-4. [Google Scholar]
- Farmer, A.D.; Strzelczyk, A.; Finisguerra, A.; Gourine, A.V.; Gharabaghi, A.; Hasan, A.; Burger, A.M.; Jaramillo, A.M.; Mertens, A.; Majid, A.; et al. International Consensus Based Review and Recommendations for Minimum Reporting Standards in Research on Transcutaneous Vagus Nerve Stimulation (Version 2020). Front. Hum. Neurosci. 2021, 14, 568051. [Google Scholar] [CrossRef]
- Kang, H. Sample Size Determination and Power Analysis Using the G*Power Software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef]
- Nemeroff, C.B.; Mayberg, H.S.; Krahl, S.E.; McNamara, J.; Frazer, A.; Henry, T.R.; George, M.S.; Charney, D.S.; Brannan, S.K. VNS Therapy in Treatment-Resistant Depression: Clinical Evidence and Putative Neurobiological Mechanisms. Neuropsychopharmacology 2006, 31, 1345–1355. [Google Scholar] [CrossRef] [Green Version]
- Kreuzer, P.M.; Landgrebe, M.; Husser, O.; Resch, M.; Schecklmann, M.; Geisreiter, F.; Poeppl, T.B.; Prasser, S.J.; Hajak, G.; Langguth, B. Transcutaneous Vagus Nerve Stimulation: Retrospective Assessment of Cardiac Safety in a Pilot Study. Front. Psychiatry 2012, 3, 00070. [Google Scholar] [CrossRef] [Green Version]
- Kraus, T.; Hösl, K.; Kiess, O.; Schanze, A.; Kornhuber, J.; Forster, C. BOLD FMRI Deactivation of Limbic and Temporal Brain Structures and Mood Enhancing Effect by Transcutaneous Vagus Nerve Stimulation. J. Neural Transm. 2007, 114, 1485–1493. [Google Scholar] [CrossRef]
- Peuker, E.T.; Filler, T.J. The Nerve Supply of the Human Auricle. Clin. Anat. 2002, 15, 35–37. [Google Scholar] [CrossRef]
- Kraus, T.; Kiess, O.; Hösl, K.; Terekhin, P.; Kornhuber, J.; Forster, C. CNS BOLD FMRI Effects of Sham-Controlled Transcutaneous Electrical Nerve Stimulation in the Left Outer Auditory Canal—A Pilot Study. Brain Stimul. 2013, 6, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Straube, A.; Ellrich, J.; Eren, O.; Blum, B.; Ruscheweyh, R. Treatment of Chronic Migraine with Transcutaneous Stimulation of the Auricular Branch of the Vagal Nerve (Auricular t-VNS): A Randomized, Monocentric Clinical Trial. J. Headache Pain 2015, 16, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badia, X.; Muriel, C.; Gracia, A.; Manuel Núñez-Olarte, J.; Perulero, N.; Gálvez, R.; Carulla, J.; Cleeland, C.S. Validación española del cuestionario Brief Pain Inventory en pacientes con dolor de causa neoplásica. Med. Clínica 2003, 120, 52–59. [Google Scholar] [CrossRef]
- Perrot, S.; Lantéri-Minet, M. Patients’ Global Impression of Change in the Management of Peripheral Neuropathic Pain: Clinical Relevance and Correlations in Daily Practice. Eur. J. Pain 2019, 23, 1117–1128. [Google Scholar] [CrossRef] [PubMed]
- Salgueiro, M.; García-Leiva, J.M.; Ballesteros, J.; Hidalgo, J.; Molina, R.; Calandre, E.P. Validation of a Spanish Version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual. Life Outcomes 2013, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and Validity of the Spanish Version of the Pittsburgh Sleep Quality Index (PSQI) in Patients with Fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Richter, P.; Werner, J.; Heerlein, A.; Kraus, A.; Sauer, H. On the Validity of the Beck Depression Inventory. Psychopathology 1998, 31, 160–168. [Google Scholar] [CrossRef]
- De la Rosa-Cáceres, A.; Stasik-O’Brien, S.; Rojas, A.J.; Sanchez-Garcia, M.; Lozano, O.M.; Díaz-Batanero, C. Spanish Adaptation of the Inventory of Depression and Anxiety Symptoms (IDAS-II) and a Study of Its Psychometric Properties. J. Affect. Disord. 2020, 271, 81–90. [Google Scholar] [CrossRef]
- Penley, J.A.; Wiebe, J.S.; Nwosu, A. Psychometric Properties of the Spanish Beck Depression Inventory-II in a Medical Sample. Psychol. Assess. 2003, 15, 569–577. [Google Scholar] [CrossRef]
- Arnau, R.C.; Meagher, M.W.; Norris, M.P.; Bramson, R. Psychometric Evaluation of the Beck Depression Inventory-II with Primary Care Medical Patients. Health Psychol. 2001, 20, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.-Y.; In, J. Randomization in Clinical Studies. Korean J. Anesth. 2019, 72, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Hey, S.P.; Kimmelman, J. The Questionable Use of Unequal Allocation in Confirmatory Trials. Neurology 2014, 82, 77–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, V.W.; Bour, L.J.; Carter, K.; Chipman, J.J.; Everett, C.C.; Heussen, N.; Hewitt, C.; Hilgers, R.-D.; Luo, Y.A.; Renteria, J.; et al. A Roadmap to Using Randomization in Clinical Trials. BMC Med. Res. Methodol. 2021, 21, 168. [Google Scholar] [CrossRef]
- Wolf, V.; Kühnel, A.; Teckentrup, V.; Koenig, J.; Kroemer, N.B. Does Transcutaneous Auricular Vagus Nerve Stimulation Affect Vagally Mediated Heart Rate Variability? A Living and Interactive Bayesian Meta-analysis. Psychophysiology 2021, 58, e13933. [Google Scholar] [CrossRef]
- Brock, C.; Brock, B.; Aziz, Q.; Møller, H.J.; Pfeiffer Jensen, M.; Drewes, A.M.; Farmer, A.D. Transcutaneous Cervical Vagal Nerve Stimulation Modulates Cardiac Vagal Tone and Tumor Necrosis Factor-Alpha. Neurogastroenterol. Motil. 2017, 29, e12999. [Google Scholar] [CrossRef]
- Keustermans, G.C.E.; Hoeks, S.B.E.; Meerding, J.M.; Prakken, B.J.; de Jager, W. Cytokine Assays: An Assessment of the Preparation and Treatment of Blood and Tissue Samples. Methods 2013, 61, 10–17. [Google Scholar] [CrossRef]
- Numis, A.L.; Fox, C.H.; Lowenstein, D.J.; Norris, P.J.; Di Germanio, C. Comparison of Multiplex Cytokine Assays in a Pediatric Cohort with Epilepsy. Heliyon 2021, 7, e06445. [Google Scholar] [CrossRef]
- Reckow, J.; Rahman-Filipiak, A.; Garcia, S.; Schlaefflin, S.; Calhoun, O.; DaSilva, A.F.; Bikson, M.; Hampstead, B.M. Tolerability and Blinding of 4x1 High-Definition Transcranial Direct Current Stimulation (HD-TDCS) at Two and Three Milliamps. Brain Stimul. 2018, 11, 991–997. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A Systematic Review on Reporting and Assessment of Adverse Effects Associated with Transcranial Direct Current Stimulation. Int. J. Neuropsychopharmacol. 2011, 14, 1133–1145. [Google Scholar] [CrossRef]
- Mourdoukoutas, A.P.; Truong, D.Q.; Adair, D.K.; Simon, B.J.; Bikson, M. High-Resolution Multi-Scale Computational Model for Non-Invasive Cervical Vagus Nerve Stimulation: High-Resolution Multi-Scale Model For Nvns. Neuromodul. Technol. Neural Interface 2018, 21, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molero-Chamizo, A.; Nitsche, M.A.; Bolz, A.; Andújar Barroso, R.T.; Alameda Bailén, J.R.; García Palomeque, J.C.; Rivera-Urbina, G.N. Non-Invasive Transcutaneous Vagus Nerve Stimulation for the Treatment of Fibromyalgia Symptoms: A Study Protocol. Brain Sci. 2022, 12, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12010095
Molero-Chamizo A, Nitsche MA, Bolz A, Andújar Barroso RT, Alameda Bailén JR, García Palomeque JC, Rivera-Urbina GN. Non-Invasive Transcutaneous Vagus Nerve Stimulation for the Treatment of Fibromyalgia Symptoms: A Study Protocol. Brain Sciences. 2022; 12(1):95. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12010095
Chicago/Turabian StyleMolero-Chamizo, Andrés, Michael A. Nitsche, Armin Bolz, Rafael Tomás Andújar Barroso, José R. Alameda Bailén, Jesús Carlos García Palomeque, and Guadalupe Nathzidy Rivera-Urbina. 2022. "Non-Invasive Transcutaneous Vagus Nerve Stimulation for the Treatment of Fibromyalgia Symptoms: A Study Protocol" Brain Sciences 12, no. 1: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12010095