
Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Literature Volume
3.2. Operative Technique
3.2.1. Skull Clamp Placement and Positioning
3.2.2. Skin Incision and Soft-Tissue Dissection
3.2.3. Identification of Bony Landmarks
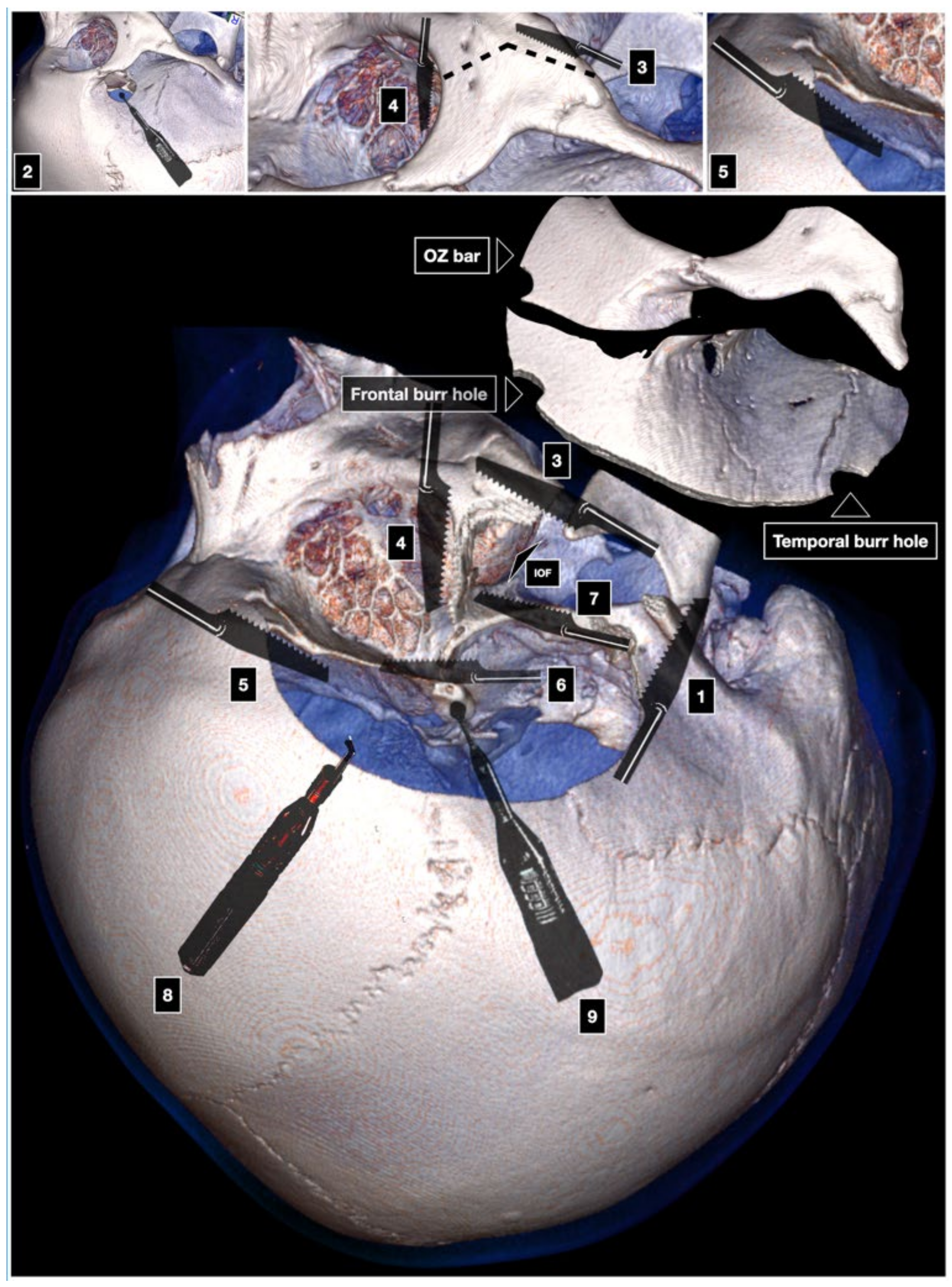
3.2.4. Craniotomy
One-Piece Orbitozygomatic Craniotomy
Two-Piece Cranio-Orbito-Zygomatic Craniotomy
- Orbitozygomatic Craniotomy (Zabramski Technique)
- 2.
- Orbitopterional Craniotomy (Al-Mefty Technique)
Three-Piece Cranio-Orbito-Zygomatic Craniotomy
3.2.5. Dura Opening
3.2.6. Intradural Corridors
3.2.7. Reconstruction
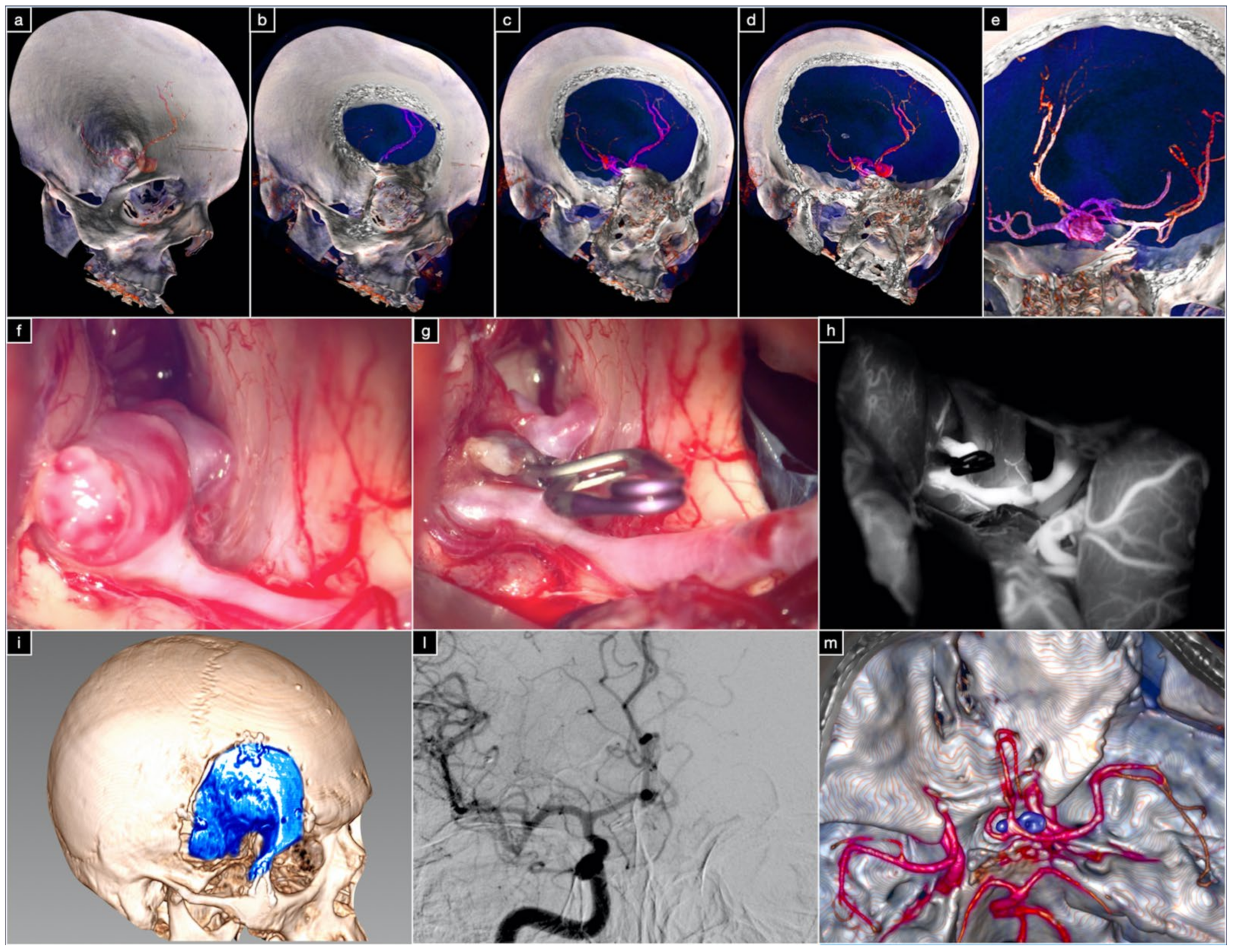
3.3. Illustrative Cases
3.3.1. Case 1: Complex Basilar Tip Aneurysm
3.3.2. Case 2: Large ACoA Aneurysm
4. Discussion
4.1. Complications Avoidance
4.2. Clinical Algorithm
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pellerin, P.; Lesoin, F.; Dhellemmes, P.; Donazzan, M.; Jomin, M. Usefulness of the Orbitofrontomalar Approach Associated with Bone Reconstruction for Frontotemporosphenoid Meningiomas. Neurosurgery 1984, 15, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Hakuba, A.; Liu, S.-S.; Shuro, N. The orbitozygomatic infratemporal approach: A new surgical technique. Surg. Neurol. 1986, 26, 271–276. [Google Scholar] [CrossRef]
- Al-Mefty, O. Supraorbital-Pterional Approach to Skull Base Lesions. Neurosurgery 1987, 21, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Aziz, K.M.A.; Froelich, S.C.; Cohen, P.L.; Sanan, A.; Keller, J.T.; Van Loveren, H.R. The One-Piece Orbitozygomatic Approach: The MacCarty Burr Hole and the Inferior Orbital Fissure as Keys to Technique and Application. Acta Neurochir. 2002, 144, 15–24. [Google Scholar] [CrossRef]
- Delashaw, J.B.; Tedeschi, H.; Rhoton, A.L. Modified Supraorbital Craniotomy. Neurosurgery 1992, 30, 954–956. [Google Scholar] [CrossRef]
- Lemole, G.M.; Henn, J.S.; Zabramski, J.M.; Spetzler, R.F. Modifications to the orbitozygomatic approach. J. Neurosurg. 2003, 99, 924–930. [Google Scholar] [CrossRef]
- Delashaw, J.B.; Jane, J.A.; Kassell, N.F.; Luce, C. Supraorbital craniotomy by fracture of the anterior orbital roof. J. Neurosurg. 1993, 79, 615–618. [Google Scholar] [CrossRef]
- Andaluz, N.; van Loveren, H.R.; Keller, J.T.; Zuccarello, M. The One-Piece Orbitopterional Approach. Skull Base 2003, 13, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Yaşargil, M.G.; Fox, J.L.; Ray, M.W. The Operative Approach to Aneurysms of the Anterior Communicating Artery. In Advances and Technical Standards in Neurosurgery; Al, K.H.E., Ed.; Springer: Vienna, Austria, 1975; Volume 2. [Google Scholar]
- Jane, J.A.; Park, T.S.; Pobereskin, L.H.; Winn, H.R.; Butler, A.B. The supraorbital approach: Technical note. Neurosurgery 1982, 11, 537–542. [Google Scholar] [CrossRef]
- Zabramski, J.M.; Kiriş, T.; Sankhla, S.K.; Cabiol, J.; Spetzler, R.F. Orbitozygomatic craniotomy. J. Neurosurg. 1998, 89, 336–341. [Google Scholar] [CrossRef] [Green Version]
- McDermott, M.W.; Durity, F.A.; Rootman, J.; Woodhurst, W.B. Combined Frontotemporal-Orbitozygomatic Approach for Tumors of the Sphenoid Wing and Orbit. Neurosurgery 1990, 26, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Komune, N.; Hayashi, D.; Amano, T.; Nakamizo, A. Three-piece orbitozygomatic craniotomy: Anatomical and clinical findings. World Neurosurg. 2019, 128, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Campero, A.; Martins, C.; Socolovsky, M.; Torino, R.; Yasuda, A.; Domitrovic, L.; Rhoton, A. Three-Piece Orbitozygomatic Approach. Oper. Neurosurg. 2010, 66, ons-E119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luzzi, S.; Gallieni, M.; Del Maestro, M.; Trovarelli, D.; Ricci, A.; Galzio, R. Giant and Very Large Intracranial Aneurysms: Surgical Strategies and Special Issues. Acta Neurochir. Suppl. 2018, 129, 25–31. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Yaşargil, M. Interfascial Pterional (Frontotemporosphenoidal) Craniotomy; Georg Thieme Verlag: New York, NY, USA, 1984; Volume 1, pp. 217–220. [Google Scholar]
- Yaşargil, M.G.; Reichman, M.V.; Kubik, S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. J. Neurosurg. 1987, 67, 463–466. [Google Scholar] [CrossRef] [Green Version]
- Oikawa, S.; Mizuno, M.; Muraoka, S.; Kobayashi, S. Retrograde dissection of the temporalis muscle preventing muscle atrophy for pterional craniotomy. J. Neurosurg. 1996, 84, 297–299. [Google Scholar] [CrossRef] [Green Version]
- Kadri, P.A.S.; Al-Mefty, O. The anatomical basis for surgical preservation of temporal muscle. J. Neurosurg. 2004, 100, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Coscarella, E.; Vishteh, A.G.; Spetzler, R.F.; Seoane, E.; Zabramski, J.M. Subfascial and submuscular methods of temporal muscle dissection and their relationship to the frontalis branch of the facial nerve. J. Neurosurg. 2000, 92, 877–880. [Google Scholar] [CrossRef]
- Al-Mefty, O.; Anand, V.K. Zygomatic approach to skull-base lesions. J. Neurosurg. 1990, 73, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Al-Mefty, O. Skull base. Neurosurgery 1986, 19, 674–675. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-T.; Robinson, J.B.; Rohrich, R.J.; Ansari, M. The Blood Supply of the Reverse Temporalis Muscle Flap: Anatomic Study and Clinical Implications. Plast. Reconstr. Surg. 1999, 103, 1181–1188. [Google Scholar] [CrossRef]
- Cheung, L.K. The blood supply of the human temporalis muscle: A vascular corrosion cast study. J. Anat. 1996, 189, 431–438. [Google Scholar] [PubMed]
- Spetzler, R.F.; Lee, K.S. Reconstruction of the temporalis muscle for the pterional craniotomy. J. Neurosurg. 1990, 73, 636–637. [Google Scholar] [CrossRef] [PubMed]
- Baldoncini, M.; Saenz, A.; Villalonga, J.F.; Campero, A.; Fernandez, J.; Sánchez-Gonzalez, F.; Kadri, P.; Vasudevan, K.; Al-Mefty, O. Safe Zones for Temporal Muscle Hook Retraction: A Technical Note. World Neurosurg. 2020, 142, 63–67. [Google Scholar] [CrossRef]
- Shimizu, S.; Tanriover, N.; Rhoton, A.L.; Yoshioka, N.; Fujii, K. MacCarty Keyhole and Inferior Orbital Fissure in Orbitozygomatic Craniotomy. Oper. Neurosurg. 2005, 57, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Tanriover, N.; Ulm, A.J.; Rhoton, A.L.; Kawashima, M.; Yoshioka, N.; Lewis, S.B. One-Piece Versus Two-Piece Orbitozygomatic Craniotomy: Quantitative And Qualitative Considerations. Oper. Neurosurg. 2006, 58, 229–237. [Google Scholar] [CrossRef]
- Andaluz, N.; Van Loveren, H.R.; Keller, J.T.; Zuccarello, M. Anatomic and clinical study of the orbitopterional approach to anterior communicating artery aneurysms. Neurosurgery 2003, 52, 1140–1148, discussion 1148–1149. [Google Scholar] [PubMed]
- Chanda, A.; Nanda, A. Anatomical study of the orbitozygomatic transsellar—transcavernous—transclinoidal approach to the basilar artery bifurcation. J. Neurosurg. 2002, 97, 151–160. [Google Scholar] [CrossRef]
- Schwartz, M.S.; Anderson, G.J.; Horgan, M.A.; Kellogg, J.X.; McMenomey, S.O.; Delashaw, J.B. Quantification of increased exposure resulting from orbital rim and orbitozygomatic osteotomy via the frontotemporal transsylvian approach. J. Neurosurg. 1999, 91, 1020–1026. [Google Scholar] [CrossRef] [Green Version]
- Meybodi, A.T.; Benet, A.; Rubio, R.R.; Yousef, S.; Mokhtari, P.; Preul, M.C.; Lawton, M.T. Comparative Analysis of Orbitozygomatic and Subtemporal Approaches to the Basilar Apex: A Cadaveric Study. World Neurosurg. 2018, 119, e607–e616. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, D.D.; Morais, B.A.; Figueiredo, E.G.; Spetzler, R.F.; Preul, M.C. Accessing the Anterior Mesencephalic Zone: Orbitozygomatic Versus Subtemporal Approach. World Neurosurg. 2018, 119, e818–e824. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, S.A.; Yamaki, V.N.; Solla, D.J.F.; de Andrade, A.F.; Teixeira, M.J.; Spetzler, R.F.; Preul, M.C.; Figueiredo, E.G. Pterional, Pretemporal, and Orbitozygomatic Approaches: Anatomic and Comparative Study. World Neurosurg. 2019, 121, e398–e403. [Google Scholar] [CrossRef] [PubMed]
- Alaywan, M.; Sindou, M. Fronto-temporal approach with orbito-zygomatic removal surgical anatomy. Acta Neurochir. 1990, 104, 79–83. [Google Scholar] [CrossRef]
- Figueiredo, E.G.; Tavares, W.M.; Rhoton, A.L., Jr.; De Oliveira, E. Nuances and technique of the pretemporal transcavernous approach to treat low-lying basilar artery aneurysms. Neurosurg. Rev. 2009, 33, 129–135. [Google Scholar] [CrossRef]
- Gonzalez, L.F.; Crawford, N.R.; Horgan, M.A.; Deshmukh, P.; Zabramski, J.M.; Spetzler, R.F. Working area and angle of attack in three cranial base approaches: Pterional, orbitozygomatic, and maxillary extension of the orbitozygomatic approach. Neurosurgery 2002, 50, 550–555. [Google Scholar]
- Lee, J.-S.; Scerrati, A.; Zhang, J.; Ammirati, M. Quantitative analysis of surgical exposure and surgical freedom to the anterosuperior pons: Comparison of pterional transtentorial, orbitozygomatic, and anterior petrosal approaches. Neurosurg. Rev. 2016, 39, 599–605. [Google Scholar] [CrossRef]
- Meybodi, A.T.; Benet, A.; Rubio, R.R.; Yousef, S.; Lawton, M.T. Comprehensive Anatomic Assessment of the Pterional, Orbitopterional, and Orbitozygomatic Approaches for Basilar Apex Aneurysm Clipping. Oper. Neurosurg. 2017, 15, 538–550. [Google Scholar] [CrossRef]
- Luzzi, S.A.G.L.; Del Maestro, M.; Galzio, R. Cranio-Orbito-Zygomatic Approach. In Neurovascular Surgical Diseases: A Case-based Approach; Galzio, S.L.R., Ed.; Nova Science Publishers, Inc: Hauppauge, NY, USA, 2020. [Google Scholar]
- Luzzi, S.; Del Maestro, M.; Galzio, R. Microneurosurgery for Paraclinoid Aneurysms in the Context of Flow Diverters. Acta Neurochir. Suppl. 2021, 47–53. [Google Scholar] [CrossRef]
- Luzzi, S.; Del Maestro, M.; Galzio, R. Posterior Circulation Aneurysms: A Critical Appraisal of a Surgical Series in Endovascular Era. Acta Neurochir. Suppl. 2021, 132, 39–45. [Google Scholar] [CrossRef]
- Luzzi, S.; Gragnaniello, C.; Lucifero, A.G.; Del Maestro, M.; Galzio, R. Microneurosurgical management of giant intracranial aneurysms: Datasets of a twenty-year experience. Data Brief 2020, 33, 106537. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, S.; Gragnaniello, C.; Lucifero, A.G.; Del Maestro, M.; Galzio, R. Surgical Management of Giant Intracranial Aneurysms: Overall Results of a Large Series. World Neurosurg. 2020, 144, e119–e137. [Google Scholar] [CrossRef] [PubMed]
- Giotta Lucifero, A.; Fernandez-Miranda, J.C.; Nunez, M.; Bruno, N.; Tartaglia, N.; Ambrosi, A.; Marseglia, G.L.; Galzio, R.; Luzzi, S. The Modular Concept in Skull Base Surgery: Anatomical Basis of the Median, Paramedian and Lateral Corridors. Acta Biomed. 2021, 92, e2021411. [Google Scholar] [CrossRef] [PubMed]
- Mascitelli, J.R.; Gandhi, S.; Meybodi, A.T.; Lawton, M.T. The oculomotor-tentorial triangle. Part 2: A microsurgical workspace for vascular lesions in the crural and ambient cisterns. J. Neurosurg. 2019, 130, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Meybodi, A.T.; Gandhi, S.; Mascitelli, J.; Bozkurt, B.; Bot, G.; Preul, M.C.; Lawton, M.T. The oculomotor-tentorial triangle. Part 1: Microsurgical anatomy and techniques to enhance exposure. J. Neurosurg. 2019, 130, 1426–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.-D.; Elhadi, A.M.; Mendes, G.A.; Maramreddy, N.; Agrawal, A.; Kalb, S.; Nakaji, P.; Spetzler, R.F.; Preul, M.C. Quantitative Study of the Opticocarotid and Carotid-Oculomotor Windows for the Interpeduncular Fossa, Before and After Internal Carotid Artery Mobilization and Posterior Communicating Division. Oper. Neurosurg. 2015, 11, 162–180. [Google Scholar] [CrossRef]
- Youssef, A.S.; Aziz, K.M.A.; Kim, E.-Y.; Keller, J.T.; Zuccarello, M.; van Loveren, H.R. The Carotid-oculomotor Window in Exposure of Upper Basilar Artery Aneurysms: A Cadaveric Morphometric Study. Neurosurgery 2004, 54, 1181–1189. [Google Scholar] [CrossRef]
- Rahme, R.; Kurbanov, A.; Keller, J.T.; Abruzzo, T.A.; Jimenez, L.; Ringer, A.J.; Choutka, O.; Zuccarello, M. The Interlenticulostriate Approach to Very High-Riding Distal Basilar Trunk Aneurysms. Oper. Neurosurg. 2017, 13, 338–344. [Google Scholar] [CrossRef]
- Waldron, J.S.; Lawton, M.T. The Supracarotid-infrafrontal Approach: Surgical Technique and Clinical Application to Cavernous Malformations in the Anteroinferior Basal Ganglia. Oper. Neurosurg. 2009, 64, ONS86–ONS95. [Google Scholar] [CrossRef]
- Kinoshita, M.; Tanaka, S.; Nakada, M.; Ozaki, N.; Hamada, J.-I.; Hayashi, Y. What Bone Part Is Important to Remove in Accessing the Suprachiasmatic Region with Less Frontal Lobe Retraction in Frontotemporal Craniotomies. World Neurosurg. 2012, 77, 342–348. [Google Scholar] [CrossRef]
- Campero, A.; Campero, A.A.; Socolovsky, M.; Martins, C.; Yasuda, A.; Basso, A.; Rhoton, A. The transzygomatic approach. J. Clin. Neurosci. 2010, 17, 1428–1433. [Google Scholar] [CrossRef] [PubMed]
- Seçkin, H.; Avci, E.; Uluç, K.; Niemann, D.; Başkaya, M.K. The work horse of skull base surgery: Orbitozygomatic approach. Technique, modifications, and applications. Neurosurg. Focus 2008, 25, E4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Mefty, O.; Smith, R.R. Tailoring the cranio-orbital approach. Keio J. Med. 1990, 39, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, E.G.; Deshmukh, P.; Zabramski, J.M.; Preul, M.C.; Crawford, N.R.; Siwanuwatn, R.; Spetzler, R.F. Quantitative Anatomic Study of Three Surgical Approaches to the Anterior Communicating Artery Complex. Oper. Neurosurg. 2005, 56, ONS-397. [Google Scholar] [CrossRef] [PubMed]
- Sergio, D.P.; Gilberto, G.M.A.; Edison, J.N.; Antonio, J.T.M.; Nilton, D.C. Basilar Aneurysm Surgery: The Subtemporal Approach with Section of the Zygomatic Arch. Neurosurgery 1986, 18, 125–128. [Google Scholar] [CrossRef]
- Ammirati, M.; Ma, J.; Becker, D.; Black, K.; Cheatham, M.; Bloch, J. Transzygomatic Approach to the Tentorial Incisura: Surgical Anatomy. Skull Base 1992, 2, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Arnaout, M.M.; Luzzi, S.; Galzio, R.; Aziz, K. Supraorbital keyhole approach: Pure endoscopic and endoscope-assisted perspective. Clin. Neurol. Neurosurg. 2019, 189, 105623. [Google Scholar] [CrossRef]
- Flores-Justa, A.; Luzzi, S.; Lucifero, A.G.; Villalonga, J.; Saenz, A.; Santin-Amo, J.; Baldoncini, M.; Campero, A. Use of Neuroanatomic Knowledge and Neuronavigation System for a Safe Anterior Petrosectomy. Brain Sci. 2021, 11, 488. [Google Scholar] [CrossRef]
- Baldoncini, M.; Luzzi, S.; Giotta Lucifero, A.; Flores-Justa, A.; González-López, P.; Campero, A.; Villalonga, J.F.; Lawton, M.T. Optic Foraminotomy for Clipping of Superior Carotid-Ophthalmic Aneurysms. Front Surg. 2021, 8, 681115. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Baldoncini, M.; Tataryn, Z.; Demichelis, M.; Conde, A.; Purves, C.; Lucifero, A.G.; Hernesniemi, J.; Luzzi, S. Microsurgical Clipping of Carotid-Ophthalmic Tandem Aneurysms: Case Report and Surgical Nuances. Medicina 2021, 57, 731. [Google Scholar] [CrossRef]
- Saeki, N.; Rhoton, A.L. Microsurgical anatomy of the upper basilar artery and the posterior circle of Willis. J. Neurosurg. 1977, 46, 563–578. [Google Scholar] [CrossRef] [PubMed]
- Newton, T.H.; Potts, D.G. (Eds.) Angiography. In Radiology of the Skull and Brain; Mosby Company: St. Louis, MO, USA, 1974; Volume 2. [Google Scholar]
- Lucifero, G.A.; Baldoncini, M.; Bruno, N.; Tartaglia, N.; Ambrosi, A.; Marseglia, G.L.; Galzio, R.; Campero, A.; Hernesniemi, J.; Luzzi, S. Microsurgical Neurovascular Anatomy of the Brain: The Anterior Circulation (Part I). Acta Biomed. 2021, 92, e2021412. [Google Scholar] [CrossRef]
- Lucifero, G.A.; Baldoncini, M.; Bruno, N.; Tartaglia, N.; Ambrosi, A.; Marseglia, G.L.; Galzio, R.; Campero, A.; Hernesniemi, J.; Luzzi, S. Microsurgical Neurovascular Anatomy of the Brain: The Posterior Circulation (Part II). Acta Biomed. 2021, 92, e2021413. [Google Scholar] [CrossRef]
- Ammirati, M.; Spallone, A.; Ma, J.; Cheatham, M.; Becker, D. An Anatomicosurgical Study of the Temporal Branch of the Facial Nerve. Neurosurgery 1993, 33, 1038–1044. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approach | Area of Exposure (mm2 ± SD) | ||
|---|---|---|---|
| Posterior Clinoid | Tentorial Edge | Basilar Tip | |
| Pterional | 2915 ± 585 | 2521 ± 301 | 1639 ± 244 |
| Orbitopterional | 3702 ± 943 | 3536 ± 539 | 2020 ± 350 |
| COZ | 4170 ± 1053 | 4249 ± 1186 | 2400 ± 386 |
| Approach | Surgical Target (% Increase in Exposure) | ||
|---|---|---|---|
| Posterior Clinoid | Tentorial Edge | Basilar Tip | |
| Orbitopterional | 26 * | 39 * | 28 * |
| Pterional + Zygomatic Osteotomy | 13 | 17 | 22 |
| COZ | 43 * | 64 * | 51 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luzzi, S.; Giotta Lucifero, A.; Spina, A.; Baldoncini, M.; Campero, A.; Elbabaa, S.K.; Galzio, R. Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom. Brain Sci. 2022, 12, 405. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12030405
Luzzi S, Giotta Lucifero A, Spina A, Baldoncini M, Campero A, Elbabaa SK, Galzio R. Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom. Brain Sciences. 2022; 12(3):405. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12030405
Chicago/Turabian StyleLuzzi, Sabino, Alice Giotta Lucifero, Alfio Spina, Matías Baldoncini, Alvaro Campero, Samer K. Elbabaa, and Renato Galzio. 2022. "Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom" Brain Sciences 12, no. 3: 405. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12030405