
The Contribution of Psychological Factors to Inter-Individual Variability in Conditioned Pain Modulation Is Limited in Young Healthy Subjects


Abstract
:1. Introduction
2. Materials and Methods
2.1. Pooled Data
2.2. Statistical Models
3. Results
3.1. Main Effects and Interactions
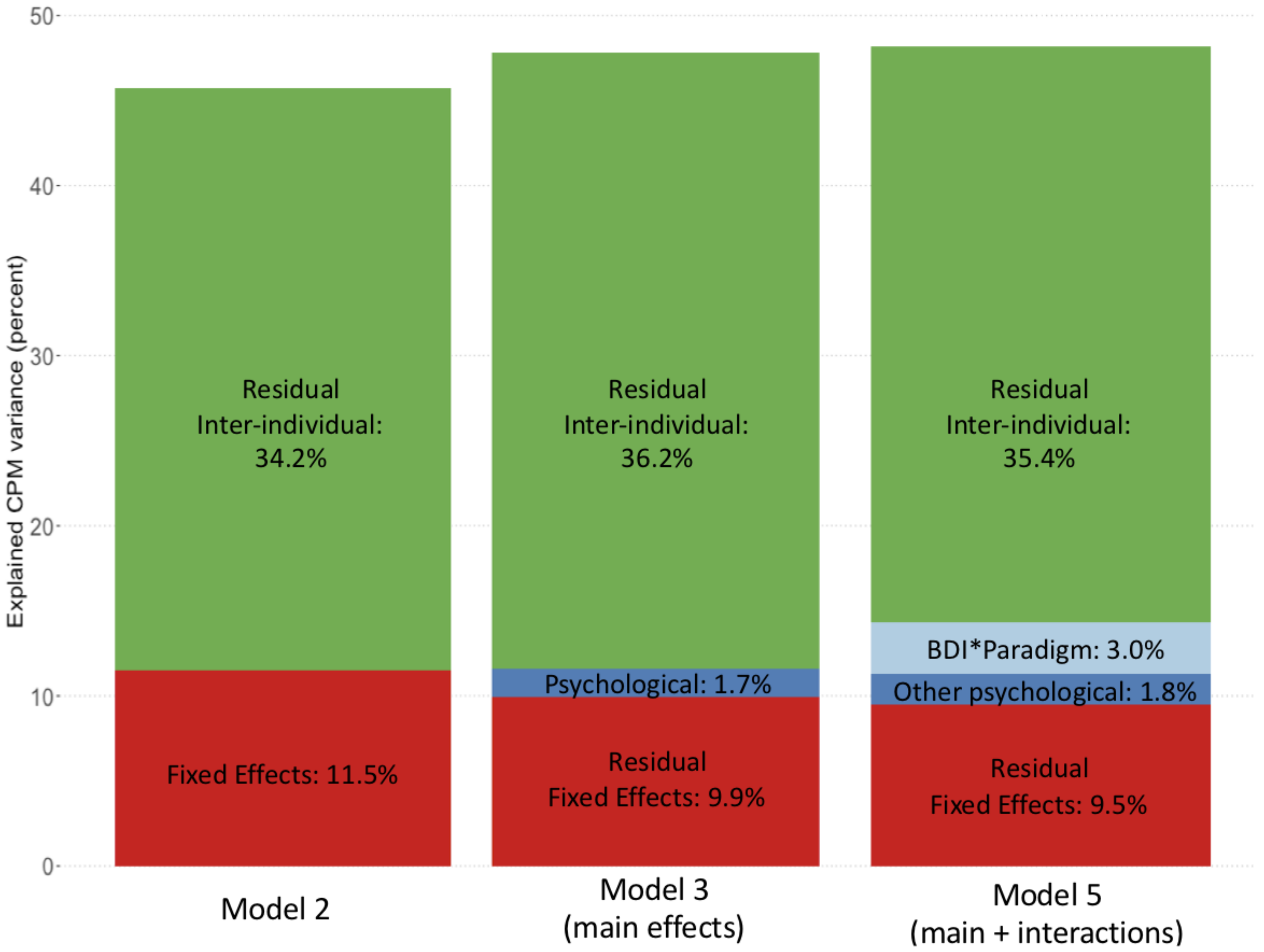
3.2. Analysis of Explained Variance
4. Discussion
- (i)
- Psychological factors, such as depression, anxiety or pain catastrophizing, do not significantly predict the CPM effect when different CPM paradigms are pooled.
- (ii)
- Depression can explain some amount of inter-individual CPM variance dependent on the CPM paradigm. However, this contribution remains small (3.0%) when compared to the residual inter-individual variance (35.4%).
4.1. Future Directions
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yarnitsky, D. Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): Its relevance for acute and chronic pain states. Curr. Opin. Anaesthesiol. 2010, 23, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.L.; Kemp, H.I.; Ridout, D.; Yarnitsky, D.; Rice, A.S.C. Reliability of conditioned pain modulation: A systematic review. Pain 2016, 157, 2410–2419. [Google Scholar] [CrossRef] [PubMed]
- Nir, R.-R.; Yarnitsky, D. Conditioned Pain Modulation. Curr. Opin. Support. Palliat. Care 2015, 9, 131–137. [Google Scholar] [CrossRef]
- Yarnitsky, D.; Crispel, Y.; Eisenberg, E.; Granovsky, Y.; Ben-Nun, A.; Sprecher, E.; Best, L.-A.; Granot, M. Prediction of chronic post-operative pain: Pre-operative DNIC testing identifies patients at risk. Pain 2008, 138, 22–28. [Google Scholar] [CrossRef]
- Staud, R.; Robinson, M.E.; Vierck, C.J.; Price, D.D. Diffuse noxious inhibitory controls (DNIC) attenuate temporal summation of second pain in normal males but not in normal females or fibromyalgia patients. Pain 2003, 101, 167–174. [Google Scholar] [CrossRef]
- Riley, L.; King, C.D.; Wong, F.; Fillingim, R.B.; Mauderli, A.P. Lack of endogenous modulation and reduced decay of prolonged heat pain in older adults. Pain 2010, 150, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Graven-Nielsen, T.; Izumi, M.; Petersen, K.K.; Arendt-Nielsen, L. User-independent assessment of conditioning pain modulation by cuff pressure algometry. Eur. J. Pain 2017, 21, 552–561. [Google Scholar] [CrossRef]
- Oono, Y.; Wang, K.; Svensson, P.; Arendt-Nielsen, L. Conditioned Pain Modulation Evoked by Different Intensities of Mechanical Stimuli Applied to the Craniofacial Region in Healthy Men and Women. J. Orofac. Pain 2011, 25, 364–375. [Google Scholar]
- Graeff, P.; Itter, A.; Wach, K.; Ruscheweyh, R. Inter-individual differences explain more variance in conditioned pain modulation than age, sex and conditioning stimulus intensity combined. Brain Sci. 2021, 11, 1186. [Google Scholar] [CrossRef]
- Defrin, R.; Schreiber, S.; Ginzburg, K. Paradoxical Pain Perception in Posttraumatic Stress Disorder: The Unique Role of Anxiety and Dissociation. J. Pain 2015, 16, 961–970. [Google Scholar] [CrossRef]
- Klauenberg, S.; Maier, C.; Assion, H.-J.; Hoffmann, A.; Krumova, E.K.; Magerl, W.; Scherens, A.; Treede, R.-D.; Juckel, G. Depression and changed pain perception: Hints for a central disinhibition mechanism. Pain 2008, 140, 332–343. [Google Scholar] [CrossRef]
- Campbell, C.M.; Kronfli, T.; Buenaver, L.F.; Smith, M.T.; Haythornthwaite, J.A.; Edwards, R.R. Situational vs. dispositional measurement of catastrophizing: Associations. J. Pain 2011, 11, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Iliffe, S.; Swift, C.; Carmaciu, C.E.; Stuck, A.; Harari, D.; Kharicha, K.; Gillman, G. The relationship between pain intensity and severity and depression in older people: Exploratory study. BMC Fam. Pract. 2009, 10, 54. [Google Scholar] [CrossRef] [Green Version]
- Horn-Hofmann, C.; Priebe, J.A.; Schaller, J.; Görlitz, R.; Lautenbacher, S. Lack of predictive power of trait fear and anxiety for conditioned pain modulation (CPM). Exp. Brain Res. 2016, 234, 3649–3658. [Google Scholar] [CrossRef]
- Varallo, G.; Giusti, E.M.; Scarpina, F.; Cattivelli, R.; Capodaglio, P.; Castelnuovo, G. The association of kinesiophobia and pain catastrophizing with pain-related disability and pain intensity in obesity and chronic lower-back pain. Brain Sci. 2021, 11, 11. [Google Scholar] [CrossRef]
- Lewis, G.N.; Rice, D.A.; McNair, P.J. Conditioned Pain Modulation in Populations with Chronic Pain: A Systematic Review and Meta-Analysis. J. Pain 2012, 13, 936–944. [Google Scholar] [CrossRef]
- Nahman-Averbuch, H.; Nir, R.R.; Sprecher, E.; Yarnitsky, D. Psychological factors and conditioned pain modulation: A meta-analysis. Clin. J. Pain 2016, 32, 541–554. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C. Manual for the State-Trait Anxiety Inventory (STAI); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Michael, J.L.S.; Scott, R.B.; Jayne, P. The Pain Catastrophizing Scale_Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Fox, J.; Weisberg, S. An {R} Companion to Applied Regression, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Bartón, K. MuMIn: Multi-Model Inference. 2020. Available online: https://cran.r-project.org/web/packages/MuMIn/index.html (accessed on 1 January 2020).
- Grömping, U. Relative Importance for Linear Regression in R: The Package relaimpo. J. Stat. Softw. 2006, 17, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Thompson, T.; Correll, C.U.; Gallop, K.; Vancampfort, D.; Stubbs, B. Is Pain Perception Altered in People with Depression? A Systematic Review and Meta-Analysis of Experimental Pain Research. J. Pain 2016, 17, 1257–1272. [Google Scholar] [CrossRef] [Green Version]
- Ruscheweyh, R.; Albers, C.; Kreusch, A.; Sommer, J.; Marziniak, M. The effect of catastrophizing self-statements on pain perception and the nociceptive flexor reflex (RIII reflex). Clin. J. Pain 2013, 29, 725–732. [Google Scholar] [CrossRef]
- Rhudy, J.L.; Williams, A.E.; McCabe, K.M.; Nguyên, M.A.T.V.; Rambo, P. Affective modulation of nociception at spinal and supraspinal levels. Psychophysiology 2005, 42, 579–587. [Google Scholar] [CrossRef]
- Hubbard, C.S.; Ornitz, E.; Gaspar, J.X.; Smith, S.; Amin, J.; Labus, J.S.; Kilpatrick, L.A.; Rhudy, J.L.; Mayer, E.A.; Naliboff, B.D. Modulation of nociceptive and acoustic startle responses to an unpredictable threat in men and women. Pain 2011, 152, 1632–1640. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, S.; Schielzeth, H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Methods Ecol. E 2013, 4, 133–142. [Google Scholar] [CrossRef]
- Nakagawa, S.; Johnson, P.C.D.; Schielzeth, H. The coefficient of determination R2 and intra-class correlation coefficient from generalized linear mixed-effects models revisited and expanded. J. R. Soc. Interface 2017, 14, 20170213. [Google Scholar] [CrossRef] [Green Version]
- Ruscheweyh, R.; Weinges, F.; Schiffer, M.; Bäumler, M.; Feller, M.; Krafft, S.; Straube, A.; Sommer, J.; Marziniak, M. Control over spinal nociception as quantified by the nociceptive flexor reflex (RIII reflex) can be achieved under feedback of the RIII reflex. Eur. J. Pain 2015, 19, 480–489. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Bäumler, M.; Feller, M.; Krafft, S.; Sommer, J.; Straube, A. Learned control over spinal nociception reduces supraspinal nociception as quantified by late somatosensory evoked potentials. Pain 2015, 156, 2505–2513. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.; Harrison, R.; Gandhi, W.; van Reekum, C.M.; Salomons, T.V. Intrinsic attention to pain is associated with a pronociceptive phenotype. Pain Rep. 2021, 6, e934. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, K.B.; Christiansen, S.E.; Holmen, L.B.; Sand, T. The effect of a mental stressor on conditioned pain modulation in healthy subjects. Scand. J. Pain 2012, 3, 142–148. [Google Scholar] [CrossRef]
- Cormier, S.; Mathieu, P.; Rainville, P. Expectations Modulate Heterotopic Noxious Counter-Stimulation Analgesia. J. Pain 2013, 14, 114–125. [Google Scholar] [CrossRef]
- Lindstedt, F.; Berrebi, J.; Greayer, E.; Lonsdorf, T.B.; Schalling, M.; Ingvar, M.; Kosek, E. Conditioned pain modulation is associated with common Polymorphisms in the serotonin transporter gene. PLoS ONE 2011, 6, e18252. [Google Scholar] [CrossRef]
- Potvin, S.; Larouche, A.; Normand, E.; De Souza, J.B.; Gaumond, I.; Grignon, S.; Marchand, S. DRD3 Ser9Gly Polymorphism Is Related to Thermal Pain Perception and Modulation in Chronic Widespread Pain Patients and Healthy Controls. J. Pain 2009, 10, 969–975. [Google Scholar] [CrossRef]
- Ibancos-Losada, M.D.R.; Osuna-Pérez, M.C.; Castellote-Caballero, M.Y.; Díaz-Fernández, Á. Conditioned pain modulation effectiveness: An experimental study comparing test paradigms and analyzing potential predictors in a healthy population. Brain Sci. 2020, 10, 599. [Google Scholar] [CrossRef]
- Chalaye, P.; Devoize, L.; Lafrenaye, S.; Dallel, R.; Marchand, S. Cardiovascular influences on conditioned pain modulation. Pain 2013, 154, 1377–1382. [Google Scholar] [CrossRef]
- Giusti, E.M.; Manna, C.; Varallo, G.; Cattivelli, R.; Manzoni, G.M.; Gabrielli, S.; D’amario, F.; Lacerenza, M.; Castelnuovo, G. The predictive role of executive functions and psychological factors on chronic pain after orthopaedic surgery: A longitudinal cohort study. Brain Sci. 2020, 10, 685. [Google Scholar] [CrossRef]
- Glombiewski, J.A.; Hartwich-Tersek, J.; Rief, W. Depression in Chronic Back Pain Patients: Prediction of Pain Intensity and Pain Disability in Cognitive-Behavioral Treatment. Psychosomatics 2010, 51, 130–136. [Google Scholar] [CrossRef]
- Edwards, R.R.; Bingham, C.O.; Bathon, J.; Haythornthwaite, J.A. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Care Res. 2006, 55, 325–332. [Google Scholar] [CrossRef]


{kind=link}
| Predictor | Estimate | p-Value |
|---|---|---|
| CSTEMP | 1.35 | 0.085 |
| AGE | −0.07 | 0.840 |
| SEX | 1.35 | 0.817 |
| BDI | −0.14 | 0.861 |
| STAI TRAIT | −0.08 | 0.821 |
| PCS | −0.30 | 0.289 |
| PARADIGM 1 | 3.43 | 0.753 |
| PARADIGM 2 | 5.05 | 0.442 |
| Model | Predictor | Estimate | p-Value |
|---|---|---|---|
| MODEL 2 | CSTemp | 1.54 | 0.001 |
| Age | 0.26 | 0.546 | |
| Sex | −1.86 | 0.700 | |
| Paradigm | −8.47 | 0.085 | |
| Repeat | −3.07 | 0.190 | |
| MODEL 3 | CSTemp | 1.55 | 0.002 |
| Age | 0.19 | 0.679 | |
| Sex | −1.57 | 0.755 | |
| BDI | −0.48 | 0.599 | |
| STAI Trait | 0.02 | 0.965 | |
| PCS | 0.00 | 0.999 | |
| Paradigm | −7.60 | 0.197 | |
| Repeat | −3.04 | 0.195 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graeff, P.; Stacheneder, R.; Alt, L.; Ruscheweyh, R. The Contribution of Psychological Factors to Inter-Individual Variability in Conditioned Pain Modulation Is Limited in Young Healthy Subjects. Brain Sci. 2022, 12, 623. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050623
Graeff P, Stacheneder R, Alt L, Ruscheweyh R. The Contribution of Psychological Factors to Inter-Individual Variability in Conditioned Pain Modulation Is Limited in Young Healthy Subjects. Brain Sciences. 2022; 12(5):623. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050623
Chicago/Turabian StyleGraeff, Philipp, Regina Stacheneder, Laura Alt, and Ruth Ruscheweyh. 2022. "The Contribution of Psychological Factors to Inter-Individual Variability in Conditioned Pain Modulation Is Limited in Young Healthy Subjects" Brain Sciences 12, no. 5: 623. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050623