Effects of Methylphenidate on Cognitive Function in Adults with Traumatic Brain Injury: A Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Risk of Bias in Individual Studies
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
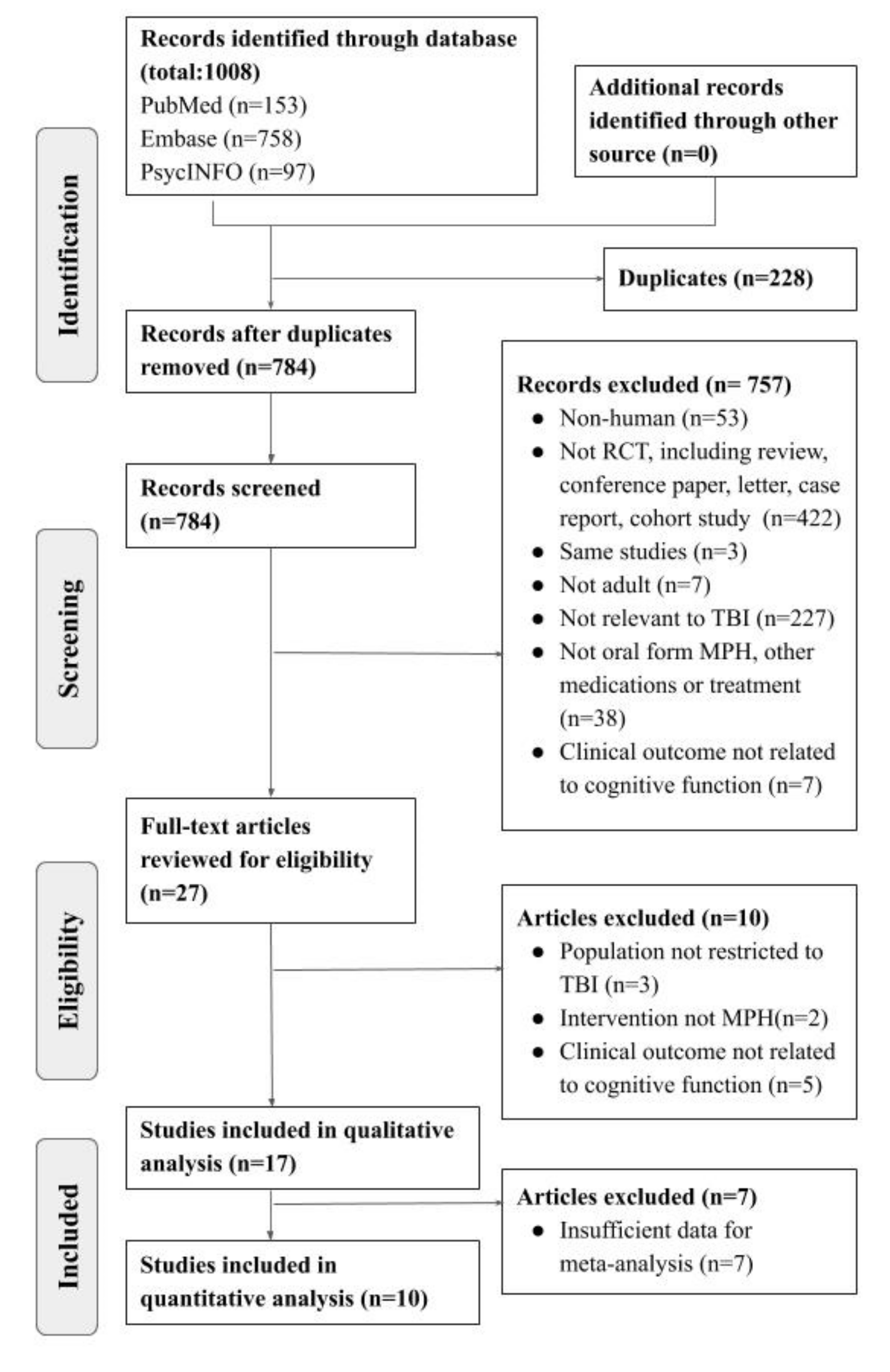
3.1. Study Identification and Selection
3.2. Study Characteristics
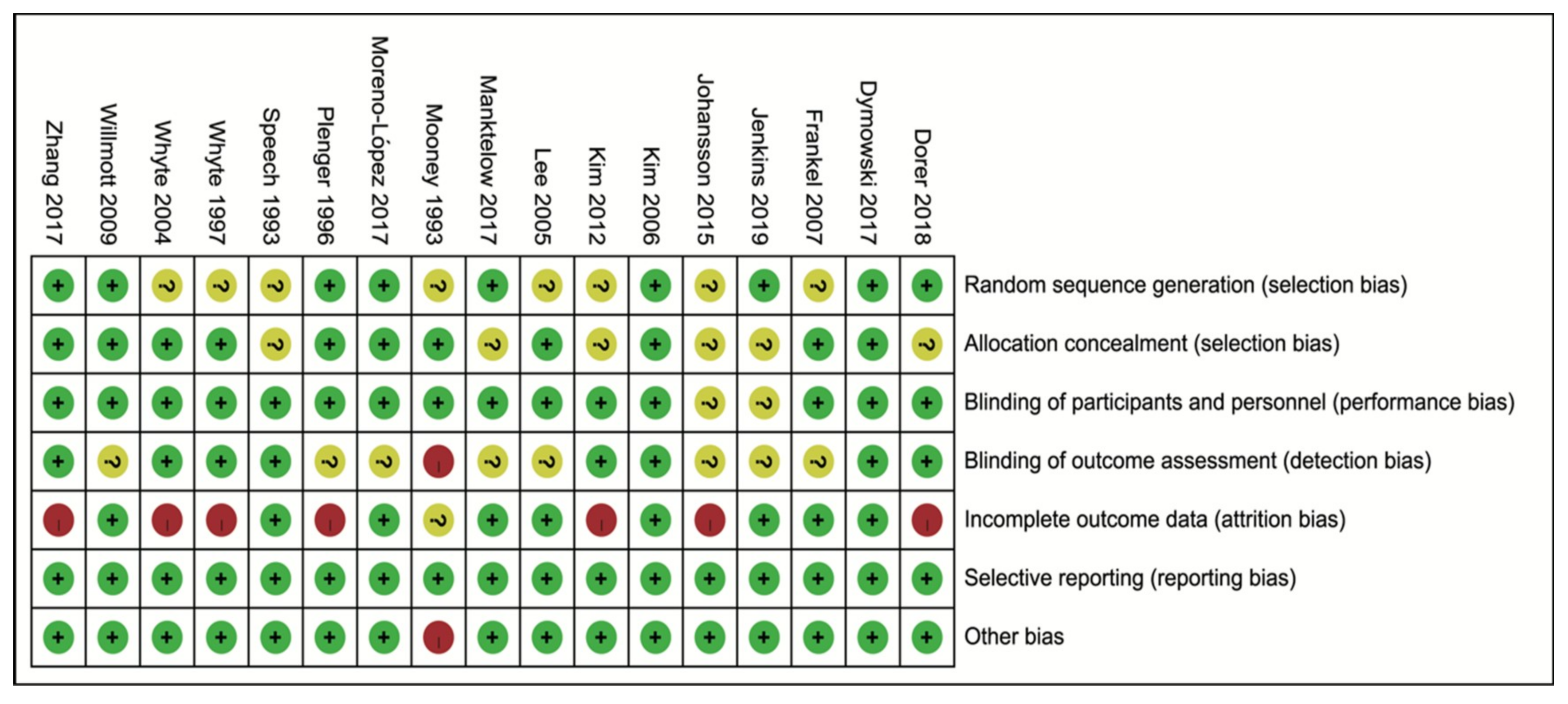
3.3. Quality and Risk of Bias Assessment
3.4. Effects of Methylphenidate on Cognitive Function Improvement
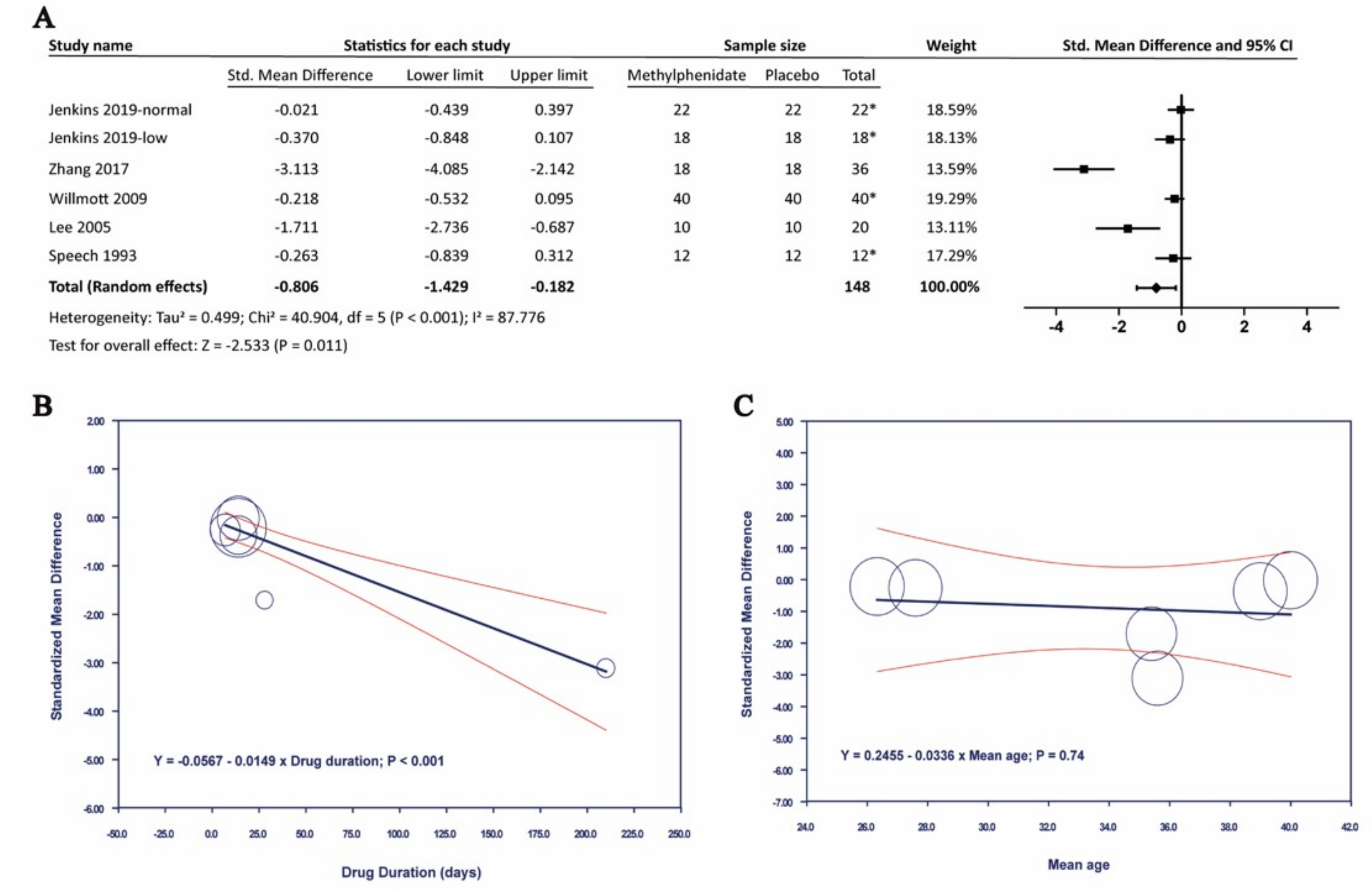
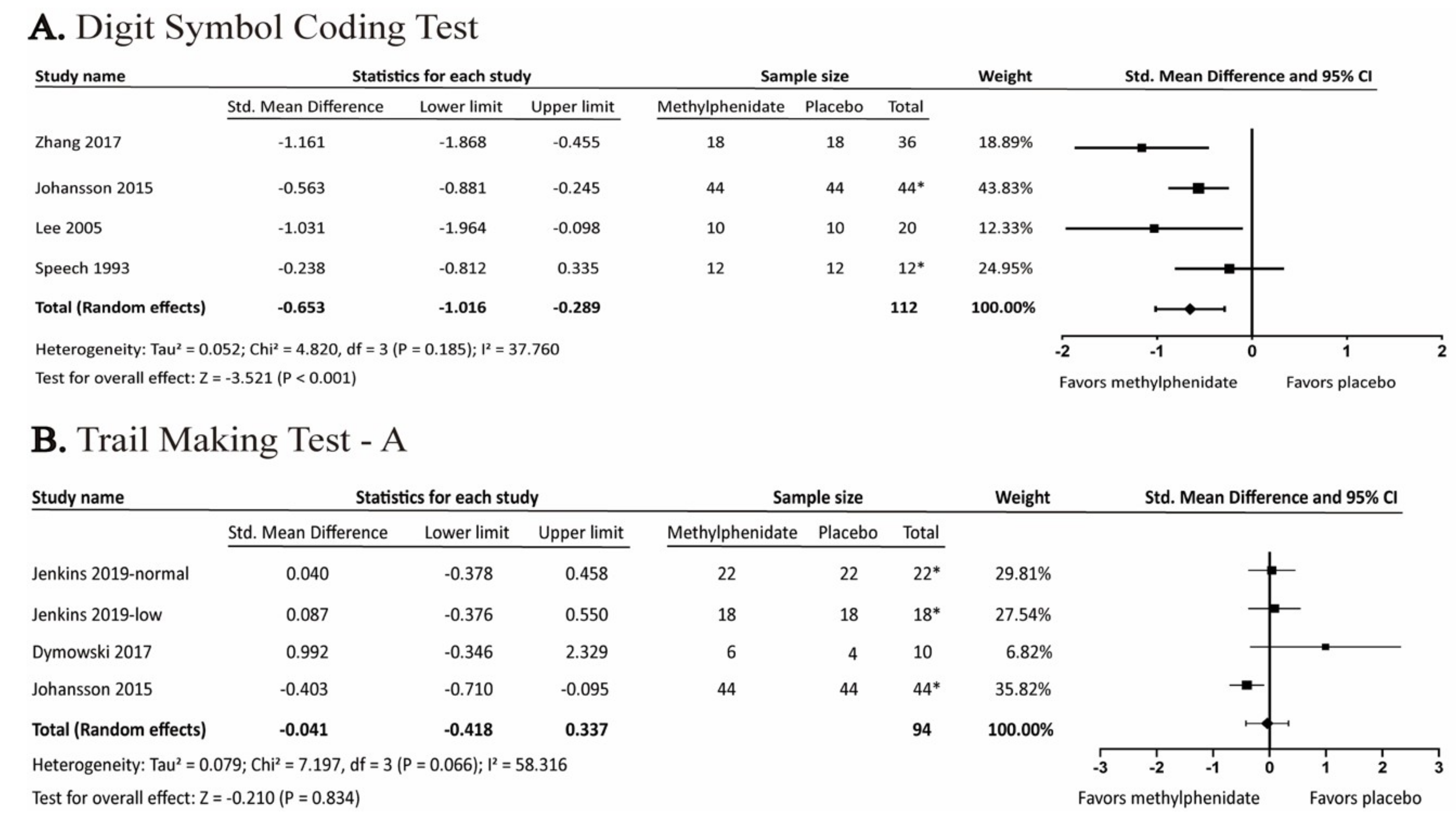
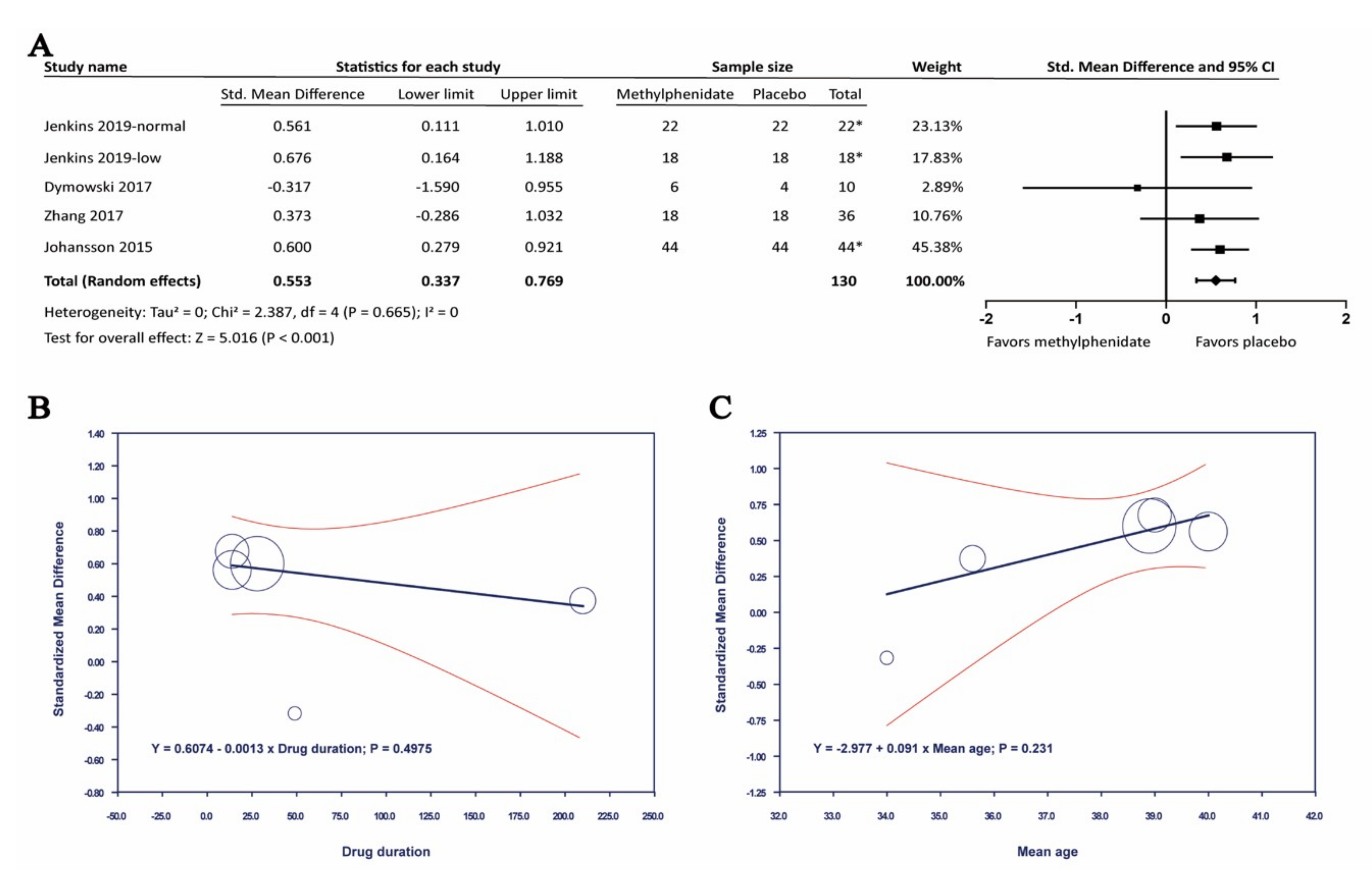
3.4.1. Effects of Methylphenidate on Processing Speed
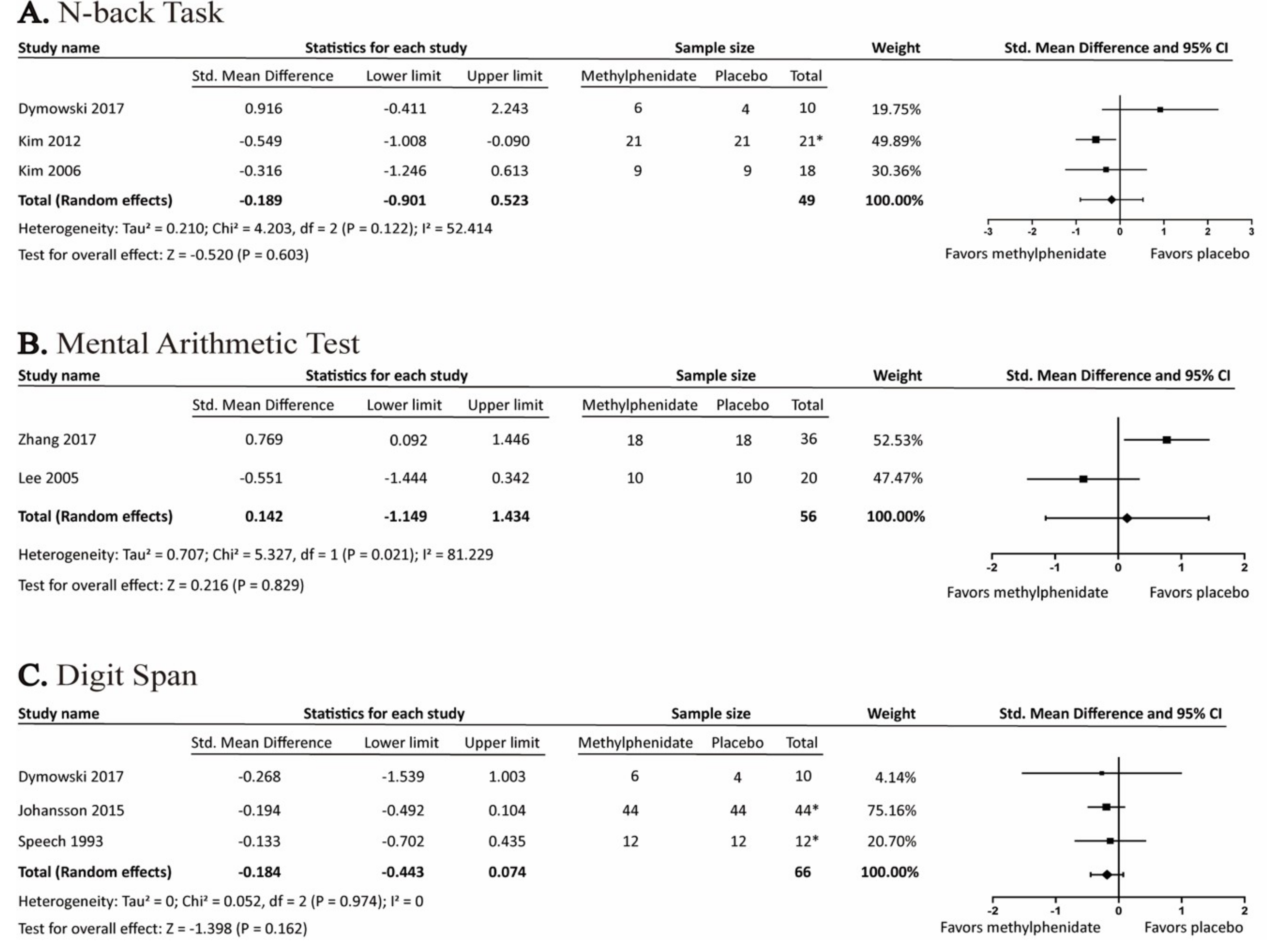
3.4.2. Effects of Methylphenidate on Working Memory
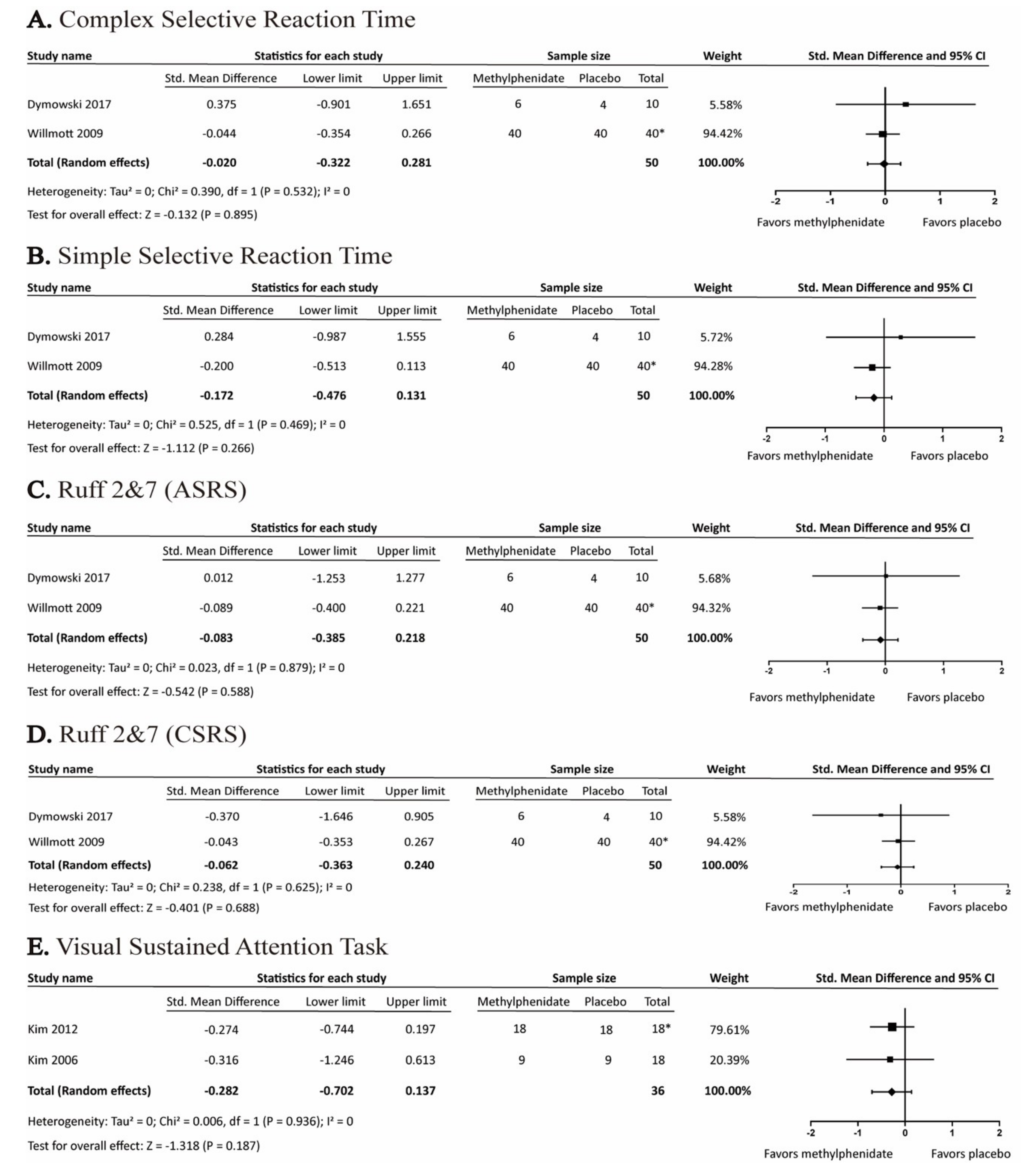
3.4.3. Effects of Methylphenidate on Attention
3.5. Adverse Events of Methylphenidate in Adult Patients with Traumatic Brain Injury
4. Discussion
4.1. Principle Finding
4.2. Comparison with Other Studies
4.3. Mechanism of TBI-Related Cognitive Deficits and MPH Effect
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Frost, R.B.; Farrer, T.J.; Primosch, M.; Hedges, D.W. Prevalence of Traumatic Brain Injury in the General Adult Population: A Meta-Analysis. Neuroepidemiology 2013, 40, 154–159. [Google Scholar] [CrossRef]
- Coronado, V.G.; Xu, L.; Basavaraju, S.V.; McGuire, L.C.; Wald, M.M.; Faul, M.; Hemphill, J.D. Hemphill, Control Centers for Disease, and Prevention. Surveillance for Traumatic Brain Injury-Related Deaths—United States, 1997–2007. MMWR Surveill. Summ. 2011, 60, 1–32. [Google Scholar]
- Peeters, W.; Brande, R.V.D.; Polinder, S.; Brazinova, A.; Steyerberg, E.W.; Lingsma, H.F.; Maas, A.I.R. Epidemiology of traumatic brain injury in Europe. Acta Neurochir. 2015, 157, 1683–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleminger, S.; Ponsford, J. Long term outcome after traumatic brain injury. BMJ 2005, 331, 1419–1420. [Google Scholar] [CrossRef] [PubMed]
- Busardò, F.P.; Kyriakou, C.; Cipolloni, L.; Zaami, S.; Frati, P. From Clinical Application to Cognitive Enhancement: The Example of Methylphenidate. Curr. Neuropharmacol. 2016, 14, 17–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warden, D.L.; Gordon, B.; McAllister, T.W.; Silver, J.M.; Barth, J.T.; Bruns, J.; Drake, A.; Gentry, T.; Jagoda, A.; Katz, D.I.; et al. Guidelines for the Pharmacologic Treatment of Neurobehavioral Sequelae of Traumatic Brain Injury. J. Neurotrauma 2006, 23, 1468–1501. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-H.; Huang, C.-C.; Sun, C.-K.; Lin, G.-H.; Hou, W.-H. Methylphenidate on Cognitive Improvement in Patients with Traumatic Brain Injury: A Meta-Analysis. Curr. Neuropharmacol. 2016, 14, 272–281. [Google Scholar] [CrossRef]
- Narad, M.E.; Kennelly, M.; Zhang, N.; Wade, S.L.; Yeates, K.O.; Taylor, H.G.; Epstein, J.N.; Kurowski, B.G. Secondary Attention-Deficit/Hyperactivity Disorder in Children and Adolescents 5 to 10 Years After Traumatic Brain Injury. JAMA Pediatr. 2018, 172, 437. [Google Scholar] [CrossRef]
- Adeyemo, B.O.; Biederman, J.; Zafonte, R.; Kagan, E.; Spencer, T.J.; Uchida, M.; Kenworthy, T.; Spencer, A.E.; Faraone, S.V. Mild Traumatic Brain Injury and ADHD. J. Atten. Disord. 2014, 18, 576–584. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Dorer, C.L.; Manktelow, A.E.; Allanson, J.; Sahakian, B.J.; Pickard, J.D.; Bateman, A.; Menon, D.K.; Stamatakis, E.A. Methylphenidate-mediated motor control network enhancement in patients with traumatic brain injury. Brain Inj. 2018, 32, 1040–1049. [Google Scholar] [CrossRef] [PubMed]
- Dymowski, A.R.; Ponsford, J.L.; Owens, J.A.; Olver, J.H.; Ponsford, M.; Willmott, C. The Efficacy and Safety of Extended-Release Methylphenidate Following Traumatic Brain Injury: A Randomised Controlled Pilot Study. Clin. Rehabil. 2017, 31, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Frankel, T.; Penn, C. Perseveration and conversation in TBI: Response to pharmacological intervention. Aphasiology 2007, 21, 1039–1078. [Google Scholar] [CrossRef]
- Jenkins, P.O.; De Simoni, S.; Bourke, N.J.; Fleminger, J.; Scott, G.; Towey, D.J.; Svensson, W.; Khan, S.; Patel, M.C.; Greenwood, R.; Friedland, D. Stratifying Drug Treatment of Cognitive Impairments after Traumatic Brain Injury Using Neuroimaging. Brain 2019, 142, 2367–2379. [Google Scholar] [CrossRef]
- Johansson, B.; Wentzel, A.-P.; Andréll, P.; Mannheimer, C.; Rönnbäck, L. Methylphenidate reduces mental fatigue and improves processing speed in persons suffered a traumatic brain injury. Brain Inj. 2015, 29, 758–765. [Google Scholar] [CrossRef]
- Kim, J.; Whyte, J.; Patel, S.; Europa, E.; Wang, J.; Coslett, H.B.; Detre, J.A. Methylphenidate Modulates Sustained Attention and Cortical Activation in Survivors of Traumatic Brain Injury: A Perfusion Fmri Study. Psychopharmacology 2012, 222, 47–57. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Ko, M.-H.; Na, S.-Y.; Park, S.-H.; Kim, K.-W. Effects of single-dose methylphenidate on cognitive performance in patients with traumatic brain injury: A double-blind placebo-controlled study. Clin. Rehabil. 2006, 20, 24–30. [Google Scholar] [CrossRef]
- Lee, H.; Kim, S.-W.; Kim, J.-M.; Shin, I.-S.; Yang, S.-J.; Yoon, J.-S. Comparing effects of methylphenidate, sertraline and placebo on neuropsychiatric sequelae in patients with traumatic brain injury. Hum. Psychopharmacol. Clin. Exp. 2005, 20, 97–104. [Google Scholar] [CrossRef]
- Manktelow, A.E.; Menon, D.K.; Sahakian, B.J.; Stamatakis, E.A. Working Memory after Traumatic Brain Injury: The Neural Basis of Improved Performance with Methylphenidate. Front. Behav. Neurosci. 2017, 11, 163. [Google Scholar] [CrossRef]
- Mooney, G.F.; Haas, L.J. Effect of methylphenidate on brain injury-related anger. Arch. Phys. Med. Rehabil. 1993, 74, 153–160. [Google Scholar]
- Moreno-López, L.; Manktelow, A.E.; Sahakian, B.J.; Menon, D.K.; Stamatakis, E.A. Anything goes? Regulation of the neural processes underlying response inhibition in TBI patients. Eur. Neuropsychopharmacol. 2017, 27, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Plenger, P.M.; Dixon, C.; Castillo, R.M.; Frankowski, R.F.; Yablon, S.A.; Levin, H.S. Subacute methylphenidate treatment for moderate to moderately severe traumatic brain injury: A preliminary double-blind placebo-controlled study. Arch. Phys. Med. Rehabil. 1996, 77, 536–540. [Google Scholar] [CrossRef]
- Speech, T.J.; Rao, S.M.; Osmon, D.C.; Sperry, L.T. A double-blind controlled study of methylphenidate treatment in closed head injury. Brain Inj. 1993, 7, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Whyte, J.; Hart, T.; Schuster, K.; Fleming, M.; Polansky, M.; Coslett, H.B. Effects of Methylphenidate on Attentional Function after Traumatic Brain Injury: A Randomized, Placebo-Controlled Trial. Am. J. Phys. Med. Rehabil. 1997, 76, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Whyte, J.; Hart, T.; Vaccaro, M.; Grieb-Neff, P.; Risser, A.; Polansky, M.; Coslett, H.B. Effects of methylphenidate on attention deficits after traumatic brain injury: A multidimensional, randomized, controlled trial. Am. J. Phys. Med. Rehabil. 2004, 83, 401–420. [Google Scholar] [CrossRef] [PubMed]
- Willmott, C.; Ponsford, J. Efficacy of Methylphenidate in the Rehabilitation of Attention Following Traumatic Brain Injury: A Randomised, Crossover, Double Blind, Placebo Controlled Inpatient Trial. J. Neurol. Neurosurg. Psychiatry 2009, 80, 552–557. [Google Scholar] [CrossRef]
- Zhang, W.-T.; Wang, Y.-F. Efficacy of methylphenidate for the treatment of mental sequelae after traumatic brain injury. Medicine 2017, 96, e6960. [Google Scholar] [CrossRef]
- O Jenkins, P.; De Simoni, S.; Bourke, N.J.; Fleminger, J.; Scott, G.; Towey, D.J.; Svensson, W.; Khan, S.; Patel, M.; Greenwood, R.; et al. Dopaminergic abnormalities following traumatic brain injury. Brain 2018, 141, 797–810. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Comprehensive Meta-Analysis Version 3; Biostat: Englewood, NJ, USA, 2013.
- Rabinowitz, A.R.; Levin, H.S. Cognitive sequelae of traumatic brain injury. Psychiatr. Clin. North Am. 2014, 37, 1–11. [Google Scholar] [CrossRef]
- Valentine, J.; Pigott, T.D.; Rothstein, H. How Many Studies Do You Need?: A Primer on Statistical Power for Meta-Analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Hindmarch, I.; Parrott, A. Repeated dose comparison of nomifensine, imipramine and placebo on subjective assessments of sleep and objective measures of psychomotor performance. Br. J. Clin. Pharmacol. 1977, 4, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Bowie, C.R.; Harvey, P.D. Administration and interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, P.; Fleminger, J.; De-Simoni, S.; Jolly, A.; Gorgoraptis, N.; Hampshire, A.; Sharp, D. Home computerised cognitive testing for Tbi is feasible and popular. J. Neurol. Neurosurg. Psychiatry 2015, 86, e4. [Google Scholar] [CrossRef]
- Ponsford, J.; Draper, K.; Schönberger, M. Functional outcome 10 years after traumatic brain injury: Its relationship with demographic, injury severity, and cognitive and emotional status. J. Int. Neuropsychol. Soc. 2008, 14, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Bonnelle, V.; Leech, R.; Kinnunen, K.M.; Ham, T.E.; Beckmann, C.F.; De Boissezon, X.; Greenwood, R.J.; Sharp, D.J. Default Mode Network Connectivity Predicts Sustained Attention Deficits after Traumatic Brain Injury. J. Neurosci. 2011, 31, 13442–13451. [Google Scholar] [CrossRef]
- Jaeger, J. Digit Symbol Substitution Test: The Case for Sensitivity over Specificity in Neuropsychological Testing. J. Clin. Psychopharmacol. 2018, 38, 513–519. [Google Scholar] [CrossRef]
- De Monte, V.E.; Geffen, G.M.; May, C.R.; McFarland, K. Improved sensitivity of the rapid screen of mild traumatic brain injury. J. Clin. Exp. Neuropsychol. 2010, 32, 28–37. [Google Scholar] [CrossRef]
- Narayan, R.K.; Michel, M.E.; Ansell, B.; Baethmann, A.; Biegon, A.; Bracken, M.B.; Bullock, M.R.; Choi, S.C.; Clifton, G.L.; Contant, C.F.; et al. Clinical Trials in Head Injury. J. Neurotrauma 2002, 19, 503–557. [Google Scholar] [CrossRef]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.G.; Wade, D.T. The Rivermead Post Concussion Symptoms Questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef]
- Hammerness, P.; Fried, R.; Petty, C.; Meller, B.; Biederman, J. Assessment of Cognitive Domains durzing Treatment with Oros Methylphenidate in Adolescents with Adhd. Child Neuropsychol. 2014, 20, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Storebø, O.J.; Simonsen, E.; Gluud, C. Methylphenidate for Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. JAMA 2016, 315, 2009–2010. [Google Scholar] [CrossRef] [PubMed]
- Eme, R. ADHD: An integration with pediatric traumatic brain injury. Expert Rev. Neurother. 2012, 12, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Backeljauw, B.; Kurowski, B.G. Interventions for attention problems after pediatric traumatic brain injury: What is the evidence? PM&R 2014, 6, 814–824. [Google Scholar]
- Johansson, B.; Wentzel, A.P.; Andrell, P.; Ronnback, L.; Mannheimer, C. Long-Term Treatment with Methylphenidate for Fatigue after Traumatic Brain Injury. Acta Neurol. Scand. 2017, 135, 100–107. [Google Scholar] [CrossRef]
- Motaghinejad, M.; Motevalian, M.; Shabab, B. Effects of chronic treatment with methylphenidate on oxidative stress and inflammation in hippocampus of adult rats. Neurosci. Lett. 2016, 619, 106–113. [Google Scholar] [CrossRef]
- A Maxwell, R.; Plummer, A.J.; Ross, S.D.; I Daniel, A. Studies concerning the cardiovascular actions of the central nervous stimulant, methylphenidate. J. Pharmacol. Exp. Ther. 1958, 123, 22–27. [Google Scholar]
- Lamberti, M.; Italiano, D.; Guerriero, L.; D’Amico, G.; Siracusano, R.; Ingrassia, M.; Germanò, E.; Calabrò, M.; Gagliano, A.; Spina, E. Evaluation of acute Cardiovascular effects of immediate-release Methylphenidate in children and adolescents with attention deficit Hyperactivity disorder. Clin. Ther. 2015, 37, e47. [Google Scholar] [CrossRef] [Green Version]
- Lonn, E.M.; Rambihar, S.; Gao, P.; Custodis, F.F.; Sliwa, K.; Teo, K.K.; Yusuf, S.; Bohm, M. Heart Rate Is Associated with Increased Risk of Major Cardiovascular Events, Cardiovascular and All-Cause Death in Patients with Stable Chronic Cardiovascular Disease: An Analysis of Ontarget/Transcend. Clin. Res. Cardiol. 2014, 103, 149–159. [Google Scholar] [CrossRef]
- Liang, E.F.; Lim, S.Z.; Tam, W.W.; Ho, C.S.; Zhang, M.W.; McIntyre, R.S.; Ho, R.C. The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Heal. 2018, 15, 1789. [Google Scholar] [CrossRef]
- Gennarelli, T.A.; Thibault, L.E.; Adams, J.H.; Graham, D.I.; Thompson, C.J.; Marcincin, R.P. Diffuse axonal injury and traumatic coma in the primate. Ann. Neurol. 1982, 12, 564–574. [Google Scholar] [CrossRef] [PubMed]
- McHugh, G.S.; Engel, D.C.; Butcher, I.; Steyerberg, E.W.; Lu, J.; Mushkudiani, N.; Hernandez, A.V.; Marmarou, A.; Maas, A.I.; Murray, G.D. Prognostic Value of Secondary Insults in Traumatic Brain Injury: Results from The IMPACT Study. J. Neurotrauma 2007, 24, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.R.; Tesco, G. Molecular mechanisms of cognitive dysfunction following traumatic brain injury. Front. Aging Neurosci. 2013, 5, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, P.O.; Mehta, M.A.; Sharp, D.J. Catecholamines and cognition after traumatic brain injury. Brain 2016, 139, 2345–2371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, G.D.; Lavin, A. Methylphenidate increases cortical excitability via activation of alpha-2 noradrenergic receptors. Neuropsychopharmacol. 2006, 31, 594–601. [Google Scholar] [CrossRef]
- Cools, R.; D’Esposito, M. Inverted-U-shaped dopamine actions on human working memory and cognitive control. Boil. Psychiatry 2011, 69, e113–e125. [Google Scholar] [CrossRef]
- Andersen, S.L.; Navalta, C.P. Altering the course of neurodevelopment: A framework for understanding the enduring effects of psychotropic drugs. Int. J. Dev. Neurosci. 2004, 22, 423–440. [Google Scholar] [CrossRef]
- Schrantee, A.; Tamminga, H.G.H.; Bouziane, C.; Bottelier, M.A.; Bron, E.E.; Mutsaerts, H.-J.M.M.; Zwinderman, A.H.; Groote, I.R.; Rombouts, S.A.R.B.; Lindauer, R.J.L.; et al. Age-Dependent Effects of Methylphenidate on the Human Dopaminergic System in Young vs. Adult Patients with Attention-Deficit/Hyperactivity Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2016, 73, 955–962. [Google Scholar] [CrossRef]
- Kolb, B.; Gibb, R. Brain Plasticity and Behaviour in the Developing Brain. J. Can. Acad. Child Adolesc. Psychiatry 2011, 20, 265–276. [Google Scholar]
- Laviola, G.; Adriani, W.; Terranova, M.; Gerra, G. Psychobiological risk factors for vulnerability to psychostimulants in human adolescents and animal models. Neurosci. Biobehav. Rev. 1999, 23, 993–1010. [Google Scholar] [CrossRef]
- Faraj, B.A.; Israili, Z.H.; Perel, J.M.; Jenkins, M.L.; Holtzman, S.G.; A Cucinell, S.; Dayton, P.G. Metabolism and disposition of methylphenidate-14C: Studies in man and animals. J. Pharmacol. Exp. Ther. 1974, 191, 535–547. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Severity | Age | Size | Study Design | Dose Regimen | Measurements Related to Cognitive Outcome | Adverse Events |
|---|---|---|---|---|---|---|---|
| Dorer 2018 [11] | Mild to severe TBI for more than 6 months | 19–58 | 28 | Double-blind, placebo-controlled, crossover study | 30 mg, one dose |
| No available data |
| Dymowski 2017 [12] | Mild to severe TBI at least 6 months | 16–65 | 11 | Randomized, placebo-controlled, double-blind trial | 0.6 mg/kg QD extended-release methylphenidate for 7 weeks |
| Trend to increase BP and anxiety |
| Frankel 2007 [13] | Severity not mentioned for 9 years and 10 years respectively | 40 and 49 | 2 | Randomized, placebo-controlled, double-blind trial | 25 mg QD for 2 weeks |
| No available data |
| Jenkins 2019 [14] | Moderate to severe TBI for at least 3 months | 20–65 | 40 | Randomized, double-blind, placebo-controlled, crossover study | 0.3 mg/kg BID for 2 weeks |
| Restlessness, increased heart rate |
| Johansson 2015 [15] | 40 mild TBI and 4 moderate TBI for more than 6 months | 18–65 | 44 | Randomized, crossover study | No medication 4 weeks, low dose (5 mg TID) 4 weeks, normal dose (20 mg TID) 4 weeks. |
| Increased BP, restlessness, depressive symptoms. No serious events. |
| Kim 2012 [16] | Moderate to severe TBI for at least 3 months | 16–60 | 23 | Randomized, double-blind, placebo-controlled crossover study | 0.3 mg/kg one dose |
| No available data |
| Kim 2006 [17] | Mild TBI for at least 6 months | 16–60 | 18 | Randomized, double-blind, placebo-controlled trial | 20 mg one dose |
| No patient complained about uncomfortable side effect |
| Lee 2005 [18] | Mild to moderate TBI for at least 2 months but no longer than 1 year | 18–55 | 30 | Randomized, double-blind, placebo-controlled trial | Methylphenidate starts at 5 mg/day to 20 mg/day in a week / sertraline starts 25 mg /day and increased to 100 mg/day in a week / placebo for 4 weeks. |
| Nausea/vomiting, diarrhea, constipation, palpitation, sweating |
| Manktelow 2017 [19] | Moderate to severe TBI for at least 6 months | 18–60 | 30 | Randomized, double-blinded, placebo-controlled, crossover study | Single dose of 30 mg |
| No available data |
| Mooney 1993 [20] | Severity not mentioned at least 6 months | 18–50 | 38 | Randomized, placebo-controlled group, single-blind trial | Gradually added to 30 mg per day for 6 weeks |
| No difference evaluated by The Recent Experience Checklist |
| Moreno-López 2017 [21] | Moderate to severe TBI for at least 7 months | 36.86 in average | 34 | Randomized, double-blinded, crossover study | 30 mg single dose |
| No available data |
| Plenger 1996 [22] | Moderate to severe TBI or complicated mild TBI, subacute stage | 16–64 | 23 | Randomized, double-blind, placebo-controlled trial | 0. 3 mg/kg BID for 30 days |
| insomnia, headache |
| Speech 1993 [23] | Moderate to severe TBI for 73 to 102 months | > 12 | 12 | Randomized, double-blind, placebo-controlled crossover study | 0.3 mg/kg BID for 1 week, then cross-over |
| No patients report side effect |
| Whyte 1997 [24] | Mild to severe TBI for 38 to 3245 days | 17–75 | 19 | Randomized, double-blind, placebo-controlled trial | 0.25 mg/kg BID for 2 days |
| No available data |
| Whyte 2004 [25] | Moderate to severe TBI for at least 3 months | 16–60 | 34 | Randomized, double-blind, placebo-controlled, crossover study | 0.3 mg/kg BID for 6 weeks |
| No available data |
| Wilmott 2009 [26] | Moderate to severe TBI for averaged 68 days | 16–60 | 40 | Randomized, double-blind, placebo-controlled, crossover study | 0.3 mg/kg BID for 2 weeks |
| Evaluated by Side Effects Questionnaire (The safety data was published in separate studies) |
| Zhang 2017 [27] | Mild to severe TBI for 2 weeks to 1 year | 18–65 | 36 | Randomized, double-blinded, placebo-controlled trial | Starting from 5 mg/day and gradually titrated to 20 mg/day for 30 weeks |
| No difference in heart rate, BP, body weight between groups |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, Y.-J.; Chien, Y.-C.; Liu, C.-T.; Wu, H.-C.; Chang, C.-Y.; Wu, M.-Y. Effects of Methylphenidate on Cognitive Function in Adults with Traumatic Brain Injury: A Meta-Analysis. Brain Sci. 2019, 9, 291. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9110291
Chien Y-J, Chien Y-C, Liu C-T, Wu H-C, Chang C-Y, Wu M-Y. Effects of Methylphenidate on Cognitive Function in Adults with Traumatic Brain Injury: A Meta-Analysis. Brain Sciences. 2019; 9(11):291. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9110291
Chicago/Turabian StyleChien, Yung-Jiun, Yung-Chen Chien, Chien-Ting Liu, Hsin-Chi Wu, Chun-Yu Chang, and Meng-Yu Wu. 2019. "Effects of Methylphenidate on Cognitive Function in Adults with Traumatic Brain Injury: A Meta-Analysis" Brain Sciences 9, no. 11: 291. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9110291