Assessment and Management of HIV-Associated Cognitive Impairment: Experience from a Multidisciplinary Memory Service for People Living with HIV


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Setting
2.2. Neuropsychological Assessments
2.3. Psychological Assessment
2.4. Quality of Life Assessments
2.5. Diagnosis
3. Results
3.1. Mental Health and Quality of Life Assessments
3.2. Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- D’Arminio Monforte, A.; Cinque, P.; Mocroft, A.; Goebel, F.D.; Antunes, F.; Katlama, C.; Justesen, U.S.; Vella, S.; Kirk, O.; Lundgren, J.; et al. Changing incidence of central nervous system diseases in the EuroSIDA cohort. Ann. Neurol. 2004, 55, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.E.; Woods, S.P.; Grant, I.; Group HNRPH. Intra-individual neurocognitive variability confers risk of dependence in activities of daily living among HIV-seropositive individuals without HIV-associated neurocognitive disorders. Arch. Clin. Neuropsychol. 2012, 27, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.P.; Weber, E.; Weisz, B.M.; Twamley, E.W.; Grant, I.; Group HNRP. Prospective memory deficits are associated with unemployment in persons living with HIV infection. Rehabil. Psychol. 2011, 56, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Gorman, A.A.; Foley, J.M.; Ettenhofer, M.L.; Hinkin, C.H.; van Gorp, W.G. Functional consequences of HIV-associated neuropsychological impairment. Neuropsychol. Rev. 2009, 19, 186–203. [Google Scholar] [CrossRef] [PubMed]
- Heaton, R.K.; Clifford, D.B.; Franklin, D.R.; Woods, S.P.; Ake, C.; Vaida, F.; Ellis, R.J.; Letendre, S.L.; Marcotte, T.D.; Atkinson, J.H.; et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology 2010, 75, 2087–2096. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, D.; Underwood, J.; Post, F.A.; Vera, J.H.; Williams, I.; Boffito, M.; Sachikonye, M.; Anderson, J.; Mallon, P.W.; Winston, A.; et al. Defining cognitive impairment in people-living-with-HIV: The POPPY study. BMC Infect. Dis. 2016, 16, 617. [Google Scholar] [CrossRef] [PubMed]
- Antinori, A.; Arendt, G.; Becker, J.T.; Brew, B.J.; Byrd, D.A.; Cherner, M.; Clifford, D.B.; Cinque, P.; Epstein, L.G.; Goodkin, K.; et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology 2007, 69, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, S.; Winston, A.; Letendre, S.; Michael, B.D.; McArthur, J.C.; Khoo, S.; Solomon, T. Controversies in HIV-associated neurocognitive disorders. Lancet Neurol. 2014, 13, 1139–1151. [Google Scholar] [CrossRef]
- Gisslén, M.; Price, R.W.; Nilsson, S. The definition of HIV-associated neurocognitive disorders: Are we overestimating the real prevalence? BMC Infect. Dis. 2011, 11, 356. [Google Scholar] [CrossRef]
- Alford, K.; Vera, J.H. Cognitive Impairment in people living with HIV in the ART era: A Review. Br. Med. Bull. 2018, 127, 56–68. [Google Scholar] [CrossRef]
- Chesney, M.A.; Smith, A.W. Critical Delays in HIV Testing and Care: The Potential Role of Stigma; The American Behavioural Scientist: Thousand Oaks, CA, USA, 1999; pp. 1162–1174. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Wechsler, D. Test of Premorbid Functioning; UK Version (TOPF UK); Pearson Assessment: London, UK, 2011. [Google Scholar]
- Reynolds, C.R.; Kamphaus, R.W. Reynolds Intellectual Assessment Scales; PAR, Inc.: Odessa, FL, USA, 2003. [Google Scholar]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, preliminary clinical validity). J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Efendov, A.; Joshi, R.; Lancee, W.; Saunders, D.; Rourke, S.B. Neurocognitive correlates of medication management in HIV/AIDS. J. Int. Neuropsychol. Soc. 2002, 8, 159. [Google Scholar]
- Duff, K.; Humphreys Clark, J.D.; O’Bryant, S.E.; Mold, J.W.; Schiffer, R.B.; Sutker, P.B. Utility of the RBANS in detecting cognitive impairment associated with Alzheimer’s disease: Sensitivity, specificity, and positive and negative predictive powers. Arch. Clin. Neuropsychol. 2008, 23, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Heyanka, D.J.; Scott, J.G.; Adams, R.L. Improving the diagnostic accuracy of the RBANS in mild cognitive impairment with construct-consistent measures. Appl. Neuropsychol. Adult 2015, 22, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Kortte, K.B.; Horner, M.D.; Windham, W.K. The trail making test, part B: Cognitive flexibility or ability to maintain set? Appl. Neuropsychol. 2002, 9, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Delis, D.C.; Kaplan, E.; Kramer, J.H. Delis-Kaplan Executive Function System: Technical Manual; Harcourt Assessment Company: San Antonio, TX, USA, 2001. [Google Scholar]
- Stern, A.R.; White, T. Neuropsychological Assessment Battery: Administration, Scoring, and Interpretation Manual; Psychological Assessment Resources: Luiz, FL, USA, 2003. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Dyer, M.T.; Goldsmith, K.A.; Sharples, L.S.; Buxton, M.J. A review of health utilities using the EQ-5D in studies of cardiovascular disease. Health Qual. Life Outcomes 2010, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A.; Pickard, A.S. Comparison of the EQ-5D and SF-12 health surveys in a general population survey in Alberta, Canada. Med. Care 2000, 38, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Lamping, D.L.; Banerjee, S.; Harwood, R.H.; Foley, B.; Smith, P.; Cook, J.C.; Murray, J.; Prince, M.; Levin, E.; et al. Development of a new measure of health-related quality of life for people with dementia: DEMQOL. Psychol. Med. 2007, 37, 737–746. [Google Scholar] [CrossRef]
- Park, M.H.; Smith, S.C.; Neuburger, J.; Chrysanthaki, T.; Hendriks, A.A.J.; Black, N. Sociodemographic Characteristics; Cognitive Function, and Health-related Quality of Life of Patients Referred to Memory Assessment Services in England. Alzheimer Dis. Assoc. Disord. 2017, 31, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.L.; Livingston, R.B.; Smernoff, E.N.; Reese, E.M.; Hafer, D.G.; Harris, J.B. Factor analysis of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) in a large sample of patients suspected of dementia. Appl. Neuropsychol. 2010, 17, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Karantzoulis, S.; Novitski, J.; Gold, M.; Randolph, C. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Utility in detection and characterization of mild cognitive impairment due to Alzheimer’s disease. Arch. Clin. Neuropsychol. 2013, 28, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Willis, R.; Matthews, D.; Contell, F.; Chan, J.; Murray, J. Improving the quality of care for mild to moderate dementia: An evaluation of the Croydon Memory Service Model. Int. J. Geriatr. Psychiatry 2007, 22, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Preventing HIV in the UK Heterosexual Population–National AIDS Trust. Available online: https://www.nat.org.uk/sites/default/files/publications/Het_HIV_prevention_July2015.pdf (accessed on 7 February 2019).
- Guha, A.; Brier, M.R.; Ortega, M.; Westerhaus, E.; Nelson, B.; Ances, B.M. Topographies of Cortical and Subcortical Volume Loss in HIV and Aging in the cART Era. J. Acquir. Immune Defic. Syndr. 2016, 73, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Watkins, C.C.; Pieper, A.A.; Treisman, G.J. Safety considerations in drug treatment of depression in HIV-positive patients: An updated review. Drug Saf. 2011, 34, 623–639. [Google Scholar] [CrossRef]
- Ferrando, S.J.; Freyberg, Z. Treatment of depression in HIV positive individuals: A critical review. Int. Rev. Psychiatry 2008, 20, 61–71. [Google Scholar] [CrossRef]
- Rabkin, J.G.; Rabkin, R.; Harrison, W.; Wagner, G. Effect of imipramine on mood and enumerative measures of immune status in depressed patients with HIV illness. Am. J. Psychiatry 1994, 151, 516–523. [Google Scholar]
- Rabkin, J.G.; Rabkin, R.; Wagner, G. Effects of fluoxetine on mood and immune status in depressed patients with HIV illness. J. Clin. Psychiatry 1994, 55, 92–97. [Google Scholar]
- Sherr, L.; Clucas, C.; Harding, R.; Sibley, E.; Catalan, J. HIV and depression—A systematic review of interventions. Psychol. Health Med. 2011, 16, 493–527. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xu, C.; Zhang, A.; Zuo, X.N.; Gao, Q.; Li, X.; Liu, Z.; Cao, X.; Zhang, K. White matter abnormalities in medication-naïve adult patients with major depressive disorder: Tract-based spatial statistical analysis. Neuro. Endocrinol. Lett. 2014, 35, 697–702. [Google Scholar] [PubMed]
- Everall, I.P.; Salaria, S.; Atkinson, J.H.; Young, C.; Corbeil, J.; Grant, I.; Masliah, E.; HNRC (HIV Neurobehavioral Research Center). Diminished somatostatin gene expression in individuals with HIV and major depressive disorder. Neurology 2006, 67, 1867–1869. [Google Scholar] [CrossRef] [PubMed]
- Schroecksnadel, K.; Sarcletti, M.; Winkler, C.; Mumelter, B.; Weiss, G.; Fuchs, D.; Kemmler, G.; Zangerle, R. Quality of life and immune activation in patients with HIV-infection. Brain Behav. Immun. 2008, 22, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Grant, I.; Franklin, D.R.; Deutsch, R.; Woods, S.P.; Vaida, F.; Ellis, R.J.; Letendre, S.L.; Marcotte, T.D.; Atkinson, J.H.; Collier, A.C.; et al. Asymptomatic HIV-associated neurocognitive impairment increases risk for symptomatic decline. Neurology 2014, 82, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Cysique, L.A.; Brew, B.J. The effects of HIV and aging on brain functions: Proposing a research framework and update on last 3 years’ findings. Curr. Opin. HIV AIDS 2014, 9, 355–364. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, D.; Underwood, J.; Boffito, M.; Post, F.; Mallon, P.; Vera, J. Cognitive Function and Depression in HIV-Positive Individuals and Matched Controls; National AIDS Treatment Advocacy Project: Glasgow, UK, 23–26 October 2016. [Google Scholar]
- Marra, C.M.; Zhao, Y.; Clifford, D.B.; Letendre, S.; Evans, S.; Henry, K.; Ellis, R.J.; Rodriguez, B.; Coombs, R.W.; Schifitto, G.; et al. Impact of combination antiretroviral therapy on cerebrospinal fluid HIV RNA and neurocognitive performance. AIDS 2009, 23, 1359–1366. [Google Scholar] [CrossRef]
- Cross, H.M.; Combrinck, M.I.; Joska, J.A. HIV-associated neurocognitive disorders: Antiretroviral regimen, central nervous system penetration effectiveness, and cognitive outcomes. S. Afr. Med. J. 2013, 103, 758–762. [Google Scholar] [CrossRef]
- Calcagno, A.; Barco, A.; Trunfio, M.; Bonora, S. CNS-Targeted Antiretroviral Strategies: When Are They Needed and What to Choose. Curr. HIV/AIDS Rep. 2018, 15, 84. [Google Scholar] [CrossRef]
- Gisslén, M.; Price, R.W.; Andreasson, U.; Norgren, N.; Nilsson, S.; Hagberg, L.; Fuchs, D.; Spudich, S.; Blennow, K.; Zetterberg, H. Plasma Concentration of the Neurofilament Light Protein (NFL) is a Biomarker of CNS Injury in HIV Infection: A Cross-Sectional Study. EBioMedicine 2016, 3, 135–140. [Google Scholar] [CrossRef]
- Valcour, V.; Shikuma, C.; Shiramizu, B.; Watters, M.; Poff, P.; Selnes, O.A.; Grove, J.; Liu, Y.; Abdul-Majid, K.B.; Gartner, S.; et al. Age, apolipoprotein E4, and the risk of HIV dementia: The Hawaii Aging with HIV Cohort. J. Neuroimmunol. 2004, 157, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Burt, T.D.; Agan, B.K.; Marconi, V.C.; He, W.; Kulkarni, H.; Mold, J.E.; Cavrois, M.; Huang, Y.; Mahley, R.W.; Dolan, M.J.; et al. Apolipoprotein (apo) E4 enhances HIV-1 cell entry in vitro, and the APOE epsilon4/epsilon4 genotype accelerates HIV disease progression. Proc. Natl. Acad. Sci. USA 2008, 105, 8718–8723. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.E.; Woods, S.P.; Letendre, S.L.; Franklin, D.R.; Bloss, C.; Goate, A.; Heaton, R.K.; Collier, A.C.; Marra, C.M.; Gelman, B.B.; et al. Apolipoprotein E4 genotype does not increase risk of HIV-associated neurocognitive disorders. J. Neurovirol. 2013, 19, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Smit, M.; Brinkman, K.; Geerlings, S.; Smit, C.; Thyagarajan, K.; Sighem, A.; de Wolf, F.; Hallett, T.B.; ATHENA observational cohort. Future challenges for clinical care of an ageing population infected with HIV: A modelling study. Lancet Infect. Dis. 2015, 15, 810–818. [Google Scholar] [CrossRef]


{kind=link}
| Neuropsychological Test | Test Description |
|---|---|
| Montreal Cognitive Assessment (MoCA) [12] | Completed prior to clinic attendance, this screening test is designed to detect Mild Cognitive Impairment (MCI) and Alzheimer’s disease across five domains. Scored out of 30, ≥26 is considered normal, ≤23 indicative of MCI and >17 of AD [12]. |
| Test of premorbid functioning UK version (TOPF) [13] | The TOPF is a word reading task designed to assess estimated premorbid functioning [13]. |
| Reynolds Intellectual Screening Test (RIST) [14] | The RIST provides a measure of general intelligence (14). An index score is calculated based on its two subtests which examine vocabulary knowledge and nonverbal reasoning. |
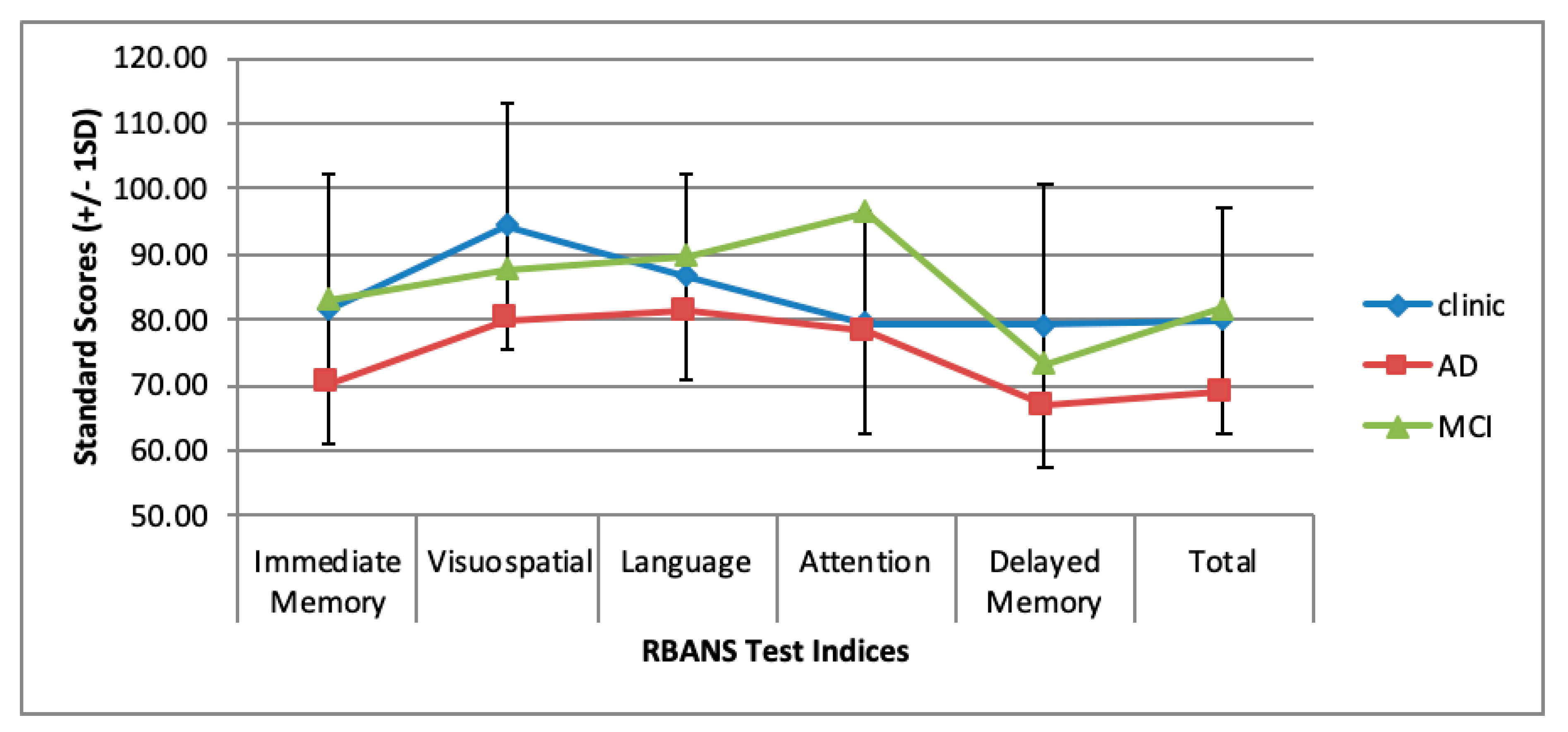
| Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) [15,16] | The RBANS is a brief assessment battery from which five index scores can be derived from each of its subtests: memory, language, visuospatial processing and attention. It has demonstrated strong diagnostic accuracy for Alzheimer’s disease and MCI [17,18]. |
| Trail Making Test [19] | The Tombaugh (2004) version of the Trail Making Test was employed as a measure of executive functioning [19], with Part B noted to measure cognitive flexibility along with set shifting [20]. |
| Delis Kaplan Executive Function Scale (DKEFS) colour word interference test [21] | This subtest from the DKEFS [21] is a version of the classic ‘stroop’ colour-word interference task, which was employed as a test of executive functioning to measure inhibitory control. |
| Neuropsychological Assessment Battery—Screening Module (NAB-SM) mazes task [22] | One subtest from the screening module of the NAB-SM [22] is included in this battery to provide a basic test of planning. |
| Variable | Total |
|---|---|
| Demographic Data | |
| Median age in years (range) ** | 55 (36–84) |
| Male (%) | 41 (79) |
| White (%) | 43 (83) |
| Black British/African (%) Asian MSM (%) Heterosexual (%) Other (%) | 7 (13) 2 (4) 38 (73) 13 (25) 1 (2) |
| Referral source: | |
| HIV Physician (%) | 33 (63) |
| Memory Assessment Service (%) | 4 (8) |
| Neurology Service (%) | 3 (6) |
| Community HIV specialists (%) | 3 (6) |
| Mental Health Services (%) | 1 (2) |
| Other (%) | 8 (15) |
| HIV Clinical Data | |
| Time since HIV diagnosis (years) ** | 17 (1–34) |
| Duration of cART (years) ** | 13 (1–22) |
| Nadir CD4 count (cells/μL) * | 312.27 (207.48) |
| Current CD4 count (cells/μL) * | 689.37 (279.45) |
| Current CD8 count (cells/μL) * | 920.98 (410.06) |
| CD4:CD8 ratio | 0.87 (.47) |
| VL >40 (%) | 4 (8) |
| On cART (%) | 51 (98) |
| On PI based regimen (%) | 12 (24) |
| On PI based and NRTIs regimen (%) | 13 (25) |
| On NRTI and NNRTI regimen (%) | 18 (35) |
| On another combination of regiment (%) | 9 (17) |
| Health Data | |
| Smoking (% smokers) | 12 (23) |
| Alcohol intake (units/week) ** | 2 (0–90) |
| Recreational drugs (% use) Cannabis (%) Methedrone GHB Other | 16 (31) 10 (16) 4 (25) 3 (19) 5 (31) |
| CVD Risk (RISK2) * | 10.34 (9.45) |
| Mean number (range) non-HIV medications Antidepressants (%) | 4.6 (0–20) 24 (46) |
| Statins (%) | 14 (27) |
| Antiplatelets (%) | 8 (15) |
| Analgesia (%) | 12 (23) |
| PPI (%) | 12 (23) |
| Other (%) | 33 (63) |
| Polypharmacy (≥3 non-HIV medications, %) | 26 (50) |
| Management Type | N |
|---|---|
| MRI | 20 |
| LP | 22 |
| Request Blood Tests | 6 |
| CT/ PET Scan | 2 |
| Neurology advice | 5 |
| Request genotyping of CSF virus | 2 |
| Switch/review/intensify cART | 14 |
| Request other health investigation | 9 |
| Review/modify co-medication | 11 |
| Refer to generic Mental Health Services | 16 |
| Refer to HIV Mental Health Specialist Services | 8 |
| Refer to community HIV Specialist nursing team | 12 |
| Refer to Other Health Services | 5 |
| Signpost to a non-HIV community service | 6 |
| Control CVD risk factors | 11 |
| In clinic advice: Cognitive strategies/remediation | 10 |
| In clinic advice: Lifestyle | 14 |
| In clinic advice: Mental health management | 7 |
| In clinic advice: cART adherence | 5 |
| Total | 185 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alford, K.; Banerjee, S.; Nixon, E.; O’Brien, C.; Pounds, O.; Butler, A.; Elphick, C.; Henshaw, P.; Anderson, S.; Vera, J.H. Assessment and Management of HIV-Associated Cognitive Impairment: Experience from a Multidisciplinary Memory Service for People Living with HIV. Brain Sci. 2019, 9, 37. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9020037
Alford K, Banerjee S, Nixon E, O’Brien C, Pounds O, Butler A, Elphick C, Henshaw P, Anderson S, Vera JH. Assessment and Management of HIV-Associated Cognitive Impairment: Experience from a Multidisciplinary Memory Service for People Living with HIV. Brain Sciences. 2019; 9(2):37. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9020037
Chicago/Turabian StyleAlford, Kate, Sube Banerjee, Eileen Nixon, Clara O’Brien, Olivia Pounds, Andrew Butler, Claire Elphick, Phillip Henshaw, Stuart Anderson, and Jaime H. Vera. 2019. "Assessment and Management of HIV-Associated Cognitive Impairment: Experience from a Multidisciplinary Memory Service for People Living with HIV" Brain Sciences 9, no. 2: 37. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9020037