Effect of Hand and Foot Massage Therapy on Psychological Factors and EEG Activity in Elderly People Requiring Long-Term Care: A Randomized Cross-Over Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Protocol
2.3. Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Williamson, A.T.; Fletcher, P.C.; Dawson, K.A. Complementary and alternative medicine. Use in an older population. J. Gerontol. Nurs. 2003, 29, 20–28. [Google Scholar] [CrossRef]
- Zhang, A.L.; Xue, C.C.; Lin, V.; Story, D.F. Complementary and alternative medicine use by older Australians. Ann. N. Y. Acad. Sci. 2007, 1114, 204–215. [Google Scholar] [CrossRef]
- Grief, C.J.; Grossman, D.; Rootenberg, M.; Mah, L. Attitudes of terminally ill older adults toward complementary and alternative medicine therapies. J. Palliat. Care 2013, 29, 205–209. [Google Scholar] [CrossRef]
- Beider, S.; Moyer, C.A. Randomized controlled trials of pediatric massage: A review. Evid. Based Complement. Alternat. Med. 2007, 4, 23–34. [Google Scholar] [CrossRef]
- McFeeters, S.; Pront, L.; Cuthbertson, L.; King, L. Massage, a complementary therapy effectively promoting the health and well-being of older people in residential care settings: A review of the literature. Int. J. Older People Nurs. 2016, 11, 266–283. [Google Scholar] [CrossRef]
- Sharpe, P.A.; Williams, H.G.; Granner, M.L.; Hussey, J.R. A randomised study of the effects of massage therapy compared to guided relaxation on well-being and stress perception among older adults. Complement. Ther. Med. 2007, 15, 157–163. [Google Scholar] [CrossRef]
- Munk, N.; Zanjani, F. Relationship between massage therapy usage and health outcomes in older adults. J. Bodyw. Mov. Ther. 2011, 15, 177–185. [Google Scholar] [CrossRef]
- Sefton, J.M.; Yarar, C.; Berry, J.W. Massage Therapy Produces Short-term Improvements in Balance, Neurological, and Cardiovascular Measures in Older Persons. Int. J. Ther. Massage Bodywork 2012, 5, 16–27. [Google Scholar]
- Sefton, J.M.; Yarar, C.; Berry, J.W. Six weeks of massage therapy produces changes in balance, neurological and cardiovascular measures in older persons. Int. J. Ther. Massage Bodywork 2012, 5, 28–40. [Google Scholar]
- Field, T.; Ironson, G.; Scafidi, F.; Nawrocki, T.; Goncalves, A.; Burman, I.; Pickens, J.; Fox, N.; Schanberg, S.; Kuhn, C. Massage therapy reduces anxiety and enhances EEG pattern of alertness and math computations. Int. J. Neurosci. 1996, 86, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.A.; Field, T. Massage and music therapies attenuate frontal EEG asymmetry in depressed adolescents. Adolescence 1999, 34, 529–534. [Google Scholar] [PubMed]
- Diego, M.A.; Field, T.; Sanders, C.; Hernandez-Reif, M. Massage therapy of moderate and light pressure and vibrator effects on EEG and heart rate. Int. J. Neurosci. 2004, 114, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Nakano, H.; Kodama, T.; Sakamoto, M.; Ueda, T.; Tani, T.; Mori, I.; Murata, S. Effect of Hand Massage on Occupational Leg Swelling and Resting-state Electroencephalographic Activity: A Randomized Cross-over Study. Int. J. Clin. Res. Trials 2018, 3, 125. [Google Scholar] [CrossRef]
- Snyder, M.; Egan, E.C.; Burns, K.R. Efficacy of hand massage in decreasing agitation behaviors associated with care activities in persons with dementia. Geriatr. Nurs. 1995, 16, 60–63. [Google Scholar] [CrossRef]
- Sansone, P.; Schmitt, L. Providing tender touch massage to elderly nursing home residents: A demonstration project. Geriatr. Nurs. 2000, 21, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Remington, R. Calming music and hand massage with agitated elderly. Nurs. Res. 2002, 51, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Kolcaba, K.; Schirm, V.; Steiner, R. Effects of hand massage on comfort of nursing home residents. Geriatr. Nurs. 2006, 27, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Hicks-Moore, S.L.; Robinson, B.A. Favorite music and hand massage: Two interventions to decrease agitation in residents with dementia. Dementia 2008, 7, 95–108. [Google Scholar] [CrossRef]
- Holliday-Welsh, D.M.; Gessert, C.E.; Renier, C.M. Massage in the management of agitation in nursing home residents with cognitive impairment. Geriatr. Nurs. 2009, 30, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Tatsumi, A.; Otsuka, T.; Kikuchi, K.; Mizuta, A.; Makino, K.; Kimoto, A.; Fujiwara, K.; Abe, T.; Nakagomi, T.; et al. Physical and psychological effects of 6-week tactile massage on elderly patients with severe dementia. Am. J. Alzheimers Dis. Other Demen. 2010, 25, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Moyle, W.; Johnston, A.N.; O’Dwyer, S.T. Exploring the effect of foot massage on agitated behaviours in older people with dementia: A pilot study. Australas J. Ageing 2011, 30, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Moyle, W.; Cooke, M.; O’Dwyer, S.T.; Murfield, J.; Johnston, A.; Sung, B. The effect of foot massage on long-term care staff working with older people with dementia: A pilot, parallel group, randomized controlled trial. BMC Nurs. 2013, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.; Kerr, J.R. Psychophysiological effects of back massage on elderly institutionalized patients. J. Adv. Nurs. 1993, 18, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Mok, E.; Woo, C.P. The effects of slow-stroke back massage on anxiety and shoulder pain in elderly stroke patients. Complement. Ther. Nurs. Midwifery 2004, 10, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Health and Welfare Services for the Elderly. Available online: http://www.mhlw.go.jp/english/wp/wp-hw6/dl/10e.pdf (accessed on 8 January 2019).
- Saito, T.; Izawa, K.P.; Watanabe, S. The relative and absolute reliability of the Functional Independence and Difficulty Scale in community-dwelling frail elderly Japanese people using long-term care insurance services. Aging Clin. Exp. Res. 2017, 29, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.Y.; Tsai, P.S.; Lee, P.H.; Chang, W.Y.; Yang, C.M. The efficacy of reflexology: Systematic review. J. Adv. Nurs. 2008, 62, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 1–55. [Google Scholar]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Marqui, R.D. Discrete, 3D distributed, linear imaging methods of electric neuronal activity. Part 1: Exact, zero error localization. arXiv, 2017; arXiv:0710.3341. [Google Scholar]
- Fuchs, M.; Kastner, J.; Wagner, M.; Hawes, S.; Ebersole, J.S. A standardized boundary element method volume conductor model. Clin. Neurophysiol. 2002, 113, 702–712. [Google Scholar] [CrossRef] [Green Version]
- Mazziotta, J.; Toga, A.; Evans, A.; Fox, P.; Lancaster, J.; Zilles, K.; Woods, R.; Paus, T.; Simpson, G.; Pike, B.; et al. A probabilistic atlas and reference system for the human brain: International Consortium for Brain Mapping (ICBM). Philos. Trans. R. Soc. Lond. B Biol. Sci. 2001, 356, 1293–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crabbe, J.B.; Dishman, R.K. Brain electrocortical activity during and after exercise: A quantitative synthesis. Psychophysiology 2004, 41, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Gogolla, N. The insular cortex. Curr. Biol. 2017, 27, R580–R586. [Google Scholar] [CrossRef] [PubMed]
- Duerden, E.G.; Arsalidou, M.; Lee, M.; Taylor, M.J. Lateralization of affective processing in the insula. Neuroimage 2013, 78, 159–175. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, K.A.; Wager, T.D.; Kober, H.; Bliss-Moreau, E.; Barrett, L.F. The brain basis of emotion: A meta-analytic review. Behav. Brain Sci. 2012, 35, 121–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewer, J.A.; Garrison, K.A.; Whitfield-Gabrieli, S. What about the “Self” is Processed in the Posterior Cingulate Cortex? Front. Hum. Neurosci. 2013, 7, 647. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.; Sharp, D.J. The role of the posterior cingulate cortex in cognition and disease. Brain 2014, 137, 12–32. [Google Scholar] [CrossRef] [PubMed]
- Nummenmaa, L.; Glerean, E.; Hari, R.; Hietanen, J.K. Bodily maps of emotions. Proc. Natl. Acad. Sci. USA 2014, 111, 646–651. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group A | Group B | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Age (years) | 80.33 | ± | 3.98 | 83.00 | ± | 2.97 | 0.22 |
| Height (cm) | 152.67 | ± | 8.10 | 147.77 | ± | 5.99 | 0.26 |
| Body weight (kg) | 53.35 | ± | 12.53 | 56.88 | ± | 4.70 | 0.53 |
| MMSE (scores) | 27.67 | ± | 2.42 | 26.50 | ± | 2.43 | 0.42 |
| Hand Massage | Foot Massage | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Pleasant (scores) | 4.17 | ± | 0.72 | 4.08 | ± | 0.67 | 0.78 |
| Relaxed (scores) | 3.92 | ± | 1.00 | 4.17 | ± | 0.83 | 0.56 |
| Fresh (scores) | 4.00 | ± | 0.74 | 3.92 | ± | 0.79 | 0.71 |
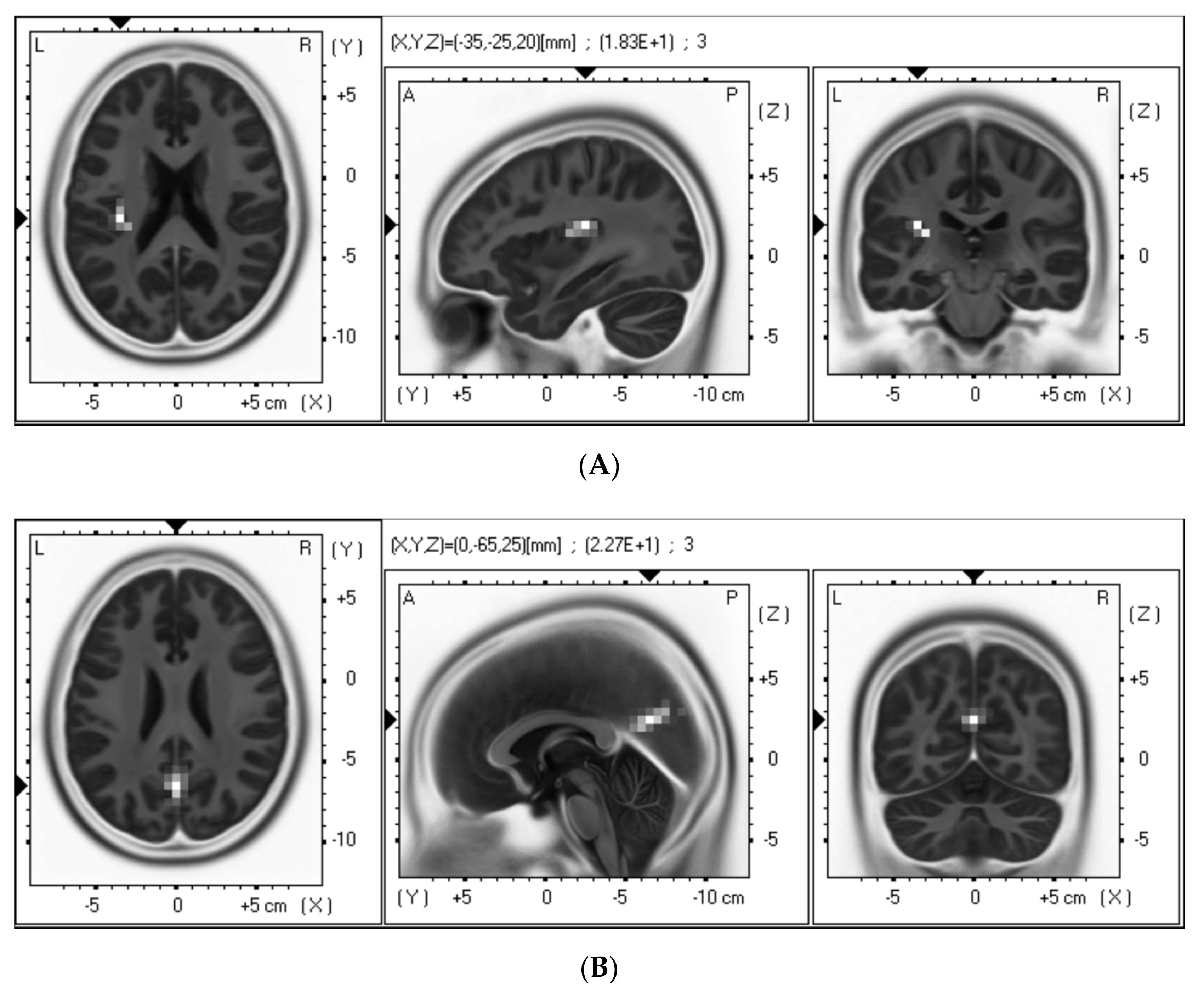
| Type of Massage | Brain Region | BA | MNI Coordinates | p-Value |
|---|---|---|---|---|
| (x, y, z) | ||||
| Hand | Insular cortex | 13 | 35, 0, 15 | <0.05 |
| Foot | Left posterior cingulate cortex | 31 | 10, −70, 15 | <0.05 |
| Right posterior cingulate cortex | 31 | −10, −75, 20 | <0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, H.; Kodama, T.; Ueda, T.; Mori, I.; Tani, T.; Murata, S. Effect of Hand and Foot Massage Therapy on Psychological Factors and EEG Activity in Elderly People Requiring Long-Term Care: A Randomized Cross-Over Study. Brain Sci. 2019, 9, 54. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9030054
Nakano H, Kodama T, Ueda T, Mori I, Tani T, Murata S. Effect of Hand and Foot Massage Therapy on Psychological Factors and EEG Activity in Elderly People Requiring Long-Term Care: A Randomized Cross-Over Study. Brain Sciences. 2019; 9(3):54. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9030054
Chicago/Turabian StyleNakano, Hideki, Takayuki Kodama, Tomohiro Ueda, Ikuko Mori, Tomiko Tani, and Shin Murata. 2019. "Effect of Hand and Foot Massage Therapy on Psychological Factors and EEG Activity in Elderly People Requiring Long-Term Care: A Randomized Cross-Over Study" Brain Sciences 9, no. 3: 54. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9030054